
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 9 (2025), Article ID: JPHIP-250
https://doi.org/10.33790/jphip1100250Research Article
The Impact of State Economic Indicators on State Population Health Outcomes
David M. Remmert1*, M.P.H., Ph.D., and Thomas O'Rourke2, Ph.D., M.P.H.,
1Assistant Professor, School of Nursing and Health Sciences, Illinois Wesleyan University, 1312 Park Street, Bloomington, IL 61701, United States.
2Professor Emeritus, Department of Kinesiology and Community Health, University of Illinois at Urbana-Champaign, 906 S. Goodwin, Urbana, IL 61801, United States.
Corresponding Author Details: David Remmert, PhD., Assistant Professor, School of Nursing and Health Sciences, Illinois Wesleyan University, 1312 Park Street, Bloomington, IL 61701, United States.
Received date: 03rd November, 2025
Accepted date: 22nd December, 2025
Published date: 24th December, 2025
Citation: Remmert, D. M., & O'Rourke, T., (2025). The Impact of State Economic Indicators on State Population Health Outcomes. J Pub Health Issue Pract 9(2): 250.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: 35 years after the IOM report, The Future of Public Health (1988) [1], multiple authors [2,3] have reflected on key lessons in considering what needs to be achieved to build a robust public health system that improves health for all. A central theme is the renewed emphasis on the role of evidence-based policy. A prior study clearly evidenced the importance of policy to achieving better health outcomes [4]. How better health outcomes are influenced by policy within high and low-income states, however, remains elusive.
Purpose: The purpose of this study is to assess the validity of state economic indicators as predictors of well-established state health outcomes.
Methods: To assess relationships between a state’s economic status and health outcomes, we developed a ranking methodology relying on a matrix of three state economic variables: income inequality, percent of the population in poverty, and median household income. To assess validity of these measures, we calculated a composite Z-score to assess the impact on health outcomes. We ran correlations comparing the twenty-five highest and lowest Economic Index states on each of the health outcomes. Standardized mortality rates are calculated providing additional insight.
Results: Findings evidenced that state economic variables correlated highly with five of the six health outcomes. For each indicator, states with higher (better) Economic Index scores had better health outcomes (other than age-adjusted prevalence of any disability). The question of “What if we were equal?” asked in earlier research focused on race and health [5] also has relevance in terms of socioeconomic status on health.
Background
The tenets of the Socio-Ecological model help us to understand that health is influenced by multiple factors. For example, policy, influenced by politics, is an important determinant of health. Multiple examples of how policy has improved health range from maternal and child health policies [6], vaccination policy [7], policy oriented around traffic safety and injury prevention [8], policy oriented around controlling tobacco use [9], among many others. Beginning with the Whitehall studies initiated in 1967 though, we also came to understand the important contributions of socio-economic status to health. Household income, income inequality and poverty are contributing factors also influencing health and health outcomes. “In practice there is a strong relationship between economics and politics because the performance of the economy is one of the key political battlegrounds. Many economic issues are inherently political because they lend themselves to different opinions. Many economic issues are seen through the eyes of political beliefs. For example, some people are instinctively more suspicious of government intervention. Therefore, they prefer economic policies, which seek to reduce government interference in the economy. For example, supply side economics, which concentrates on deregulation, privatisation, and tax cuts [10].”
In an earlier study titled “Quantifying the Impact of State Health Policy on State Population Health Outcomes,”[4] the validity of state policy hazardous scores on state health outcomes was assessed. This analysis identified and enhanced understanding of the association between how robust state health policies matter to population health overall.
This research provided clear evidence that those states with supportive health policies typically ranked better in terms of the actual causes of death, and subsequently, population health outcomes. Consistent with the socio-cultural perspective of health, Galea et al., (2011) highlighted the fact that social influences can matter just as much to health status as other antecedent causes [11]. In their view, these authors noted how such factors as low education, racial segregation, low social support, individual level and area level poverty, and income inequality play a role in numbers of deaths each year. More focused research efforts are needed to deepen our understanding of those influences and quantify them. That is, in addition to health policy, how much do factors such as income inequality, median household income, and poverty status play a role in health outcomes, and how do these variables interact within low and high-income states?
In prior research [4], it was noted that the highest/best average rankings across all health outcomes belonged to New Hampshire, Massachusetts, Vermont, Connecticut, and Hawaii. Conversely, the lowest/worst average rankings across all outcomes belonged to Mississippi, Arkansas, Alabama, Kentucky, and Louisiana. While these earlier studies quantified the contribution of how health policy may influence health outcomes, a cursory examination of the data findings of the study noted that the states with the lowest ranking states for health outcomes also appeared among the lowest in terms of median household income and that the highest outcome states also appeared among the highest in terms of median household income. This calls into question the value of policy where poverty status may be an over-riding macro-level influence.
How economic conditions matter to the health status of populations received thorough analysis by Venkataramani et al. (2020). In this commentary, the authors noted that the trend in life expectancy, which began to decline in the United States beginning in 2014, appeared to be primarily driven by worsening health among working- age individuals of lower socioeconomic status. Worsening economic conditions were noted as a “primary causal driver of adverse health trends among low-income and less-educated working-age US residents [12].” This analysis reinforces the notion that health isn’t just about health policy, but also about economic policy, as bore out repeatedly in our lowest income states.
Worsening economic outcomes for less-educated and low-income individuals can influence health through several channels. Falling incomes can reduce access to basic material resources (e.g., stable housing, healthy foods, health insurance, and healthcare) needed to ensure good health. Worsening economic outcomes may also increase exposure to stressors such as poor environmental conditions (e.g., soil, air, and water pollution). Increasing economic insecurity may directly harm health through increasing biological and psychosocial stress, as well [12].
Several economic indicators have been seen in earlier research to matter considerably to health overall. Income inequality, for example, is strongly linked to health outcomes, with those in lower socioeconomic positions generally experiencing worse health and shorter lifespans. This disparity is not solely due to individual income and is also influenced by the distribution of income within a society. Income disparities can lead to increased stress, reduced social cohesion, and poorer health behaviors, impacting everyone, not just those with low incomes [13-15]. According to Khullar et al. (2018), income inequality in the United States (the difference between high- income and low-income earners) has increased dramatically in recent decades, while health indicators have plateaued, and life expectancy differences by income have grown [16].
Also, higher median household income is generally associated with better health outcomes. Conversely, lower median household income is often linked to poorer health, including shorter lifespans and higher rates of chronic diseases. This relationship is not just a correlation but shows a gradient effect, with health risks decreasing as income increases [17-19]. Not surprisingly, poverty and health are closely linked, with poverty significantly increasing the risk of various health problems. Individuals living in poverty often experience poorer health outcomes, including higher rates of chronic diseases, mental health issues, and premature mortality. This connection stems from multiple factors, including limited access to healthcare, healthy food, and safe housing, as well as increased exposure to environmental hazards and chronic stress [20-22].
Purpose
The purpose of this study is to, 1) assess the intercorrelations between the economic indicators of state income inequality, percent of population in poverty, and median household income, 2) assess the strength of relationship between state economic indicators and health outcomes, 3) compare the twenty-five highest and lowest states ranked by their average Economic Index (a composite of the 3 economic indicators above), and 4) compare the twenty-five highest and lowest ranked states by health outcomes and their Standardized Mortality Rate (SMR).
Rankings are frequently used as an evaluation tool to measure a plethora of different quality of life variables throughout our society. Typically, these rankings are often used for comparison purposes and directing resources, offering more or less check-off boxes evaluating the presence or absence of variables important to the subject of study. Much less frequently has the validity of rankings been assessed empirically. That is, how well do they correlate to well-established outcomes they purport to assess? Using a ranking methodology empirically to measure state health status remains a meaningful approach.
Significance
This study builds upon the established importance of economics and health status. By focusing on the state-level, it seeks to enhance our understanding of the importance of economics and its impact on health at the state level. States can play a key role. Unlike non governmental organizations and entities, states are legal entities empowered to pass legislation, taxation, enact rules and regulations, set standards accompanied by enforcement powers. As such, states are in a unique position to impact population health. The Tenth Amendment specifically reserves powers not delegated to the federal government, nor prohibited, to the states or the people. This ensures that states retain significant authority while remaining within the framework of the Constitution.
Understanding state economic variables and state health outcomes can provide valuable insight to state legislators, policy makers, planners, and administrators to develop, implement and evaluate programs and initiatives to improve health outcomes and overall population health. Knowing how states rank in terms of state economic variables and their relationship to state health outcomes may be informative to business, industry, and labor leaders. Those responsible for education and job training can find the results useful as well as health professionals in both the public and private sector. Advocacy groups can find the results helpful in their efforts to improve health of their constituencies. The media may use findings to enhance public awareness of how well their state ranks and promote efforts to enhance rankings. Individuals may find results informative in voting and location decisions.
Besides focusing on the state level, a unique aspect of this study is not only identifying the interrelationships between the state economic variables, but assessing validity through a composite Economic Index comprised of three key economic variables and then assessing the strength of the Economic Index to each of the state health outcomes. To provide further insight, the study then compares the average Economic Index score of the top and bottom twenty-five states on each outcome.
Methods
Since existing literature has noted that both policy and economics can impact health outcomes, it seemed appropriate and important to better understand the interaction of economics on health status, using each state as a focal point. In this study, we assess the impact of state economic variables on the same widely used health outcome measures used in a previous study [4]. To assess this relationship, three widely referenced economic variables used in prior research were selected as the independent variables after review of the literature [16,23-24].
State economic variables ranking used to assess validity as predictors of state health outcomes included median household income, percentage of the population in poverty, and income inequality (defined as the ratio of household income at the 80th percentile to income at the 20th percentile (https://www.countyhealthrankings. org/health-data/community-conditions/social-and-economic-factors/ income-employment-and-wealth/income-inequality?year=2025, accessed 5/11/2025). For each of these economic indicators, descriptive statistics were calculated that included the mean, standard deviation, and the Z-score using Microsoft Excel. The Z-score allowed us to compare each of the 50 states in terms of how far above or below the mean they ranked. Pearson product-moment correlation analyses were run to determine how correlated each of these economic indicators were to each other.
Additional Pearson product-moment correlation tests were run to determine how well a composite average Z-score of these state economic indicators (termed the “Economic Index”) correlated with each of the six health outcomes. The health outcomes serving as the dependent variable of study included indicators commonly used to measure health across populations, [25-26] including All-Cause Mortality, Life Expectancy, Infant Mortality Rate, Years of Potential Life Lost at age 75 (a measure of premature death), Percent of the Population Self-Reporting Fair or Poor Health, and Age-Adjusted Prevalence of Any Disability.
To assess the impact of economic variables with the dependent variables, we compared the twenty-five highest and lowest Economic Index states on each of the health outcomes noted above. A t-test of independent groups assuming equal variances was used to determine if the differences between states were statistically significant. Finally, to provide additional insight, the Standardized Mortality Rate (SMR) was calculated to determine the impact of state Economic Index on health status. All analyses were run using SPSS version [29].
Results
Results of the correlation analyses between state economic variables are shown in Table 1. Findings indicate significant inter-relationships between state economic variables. Median household income negatively correlated with both income inequality and percent of the population in poverty. Not surprisingly, as state median household increased both income inequality and percent of population in poverty decreased. Also, as income inequality increased so did the percent of population in poverty.
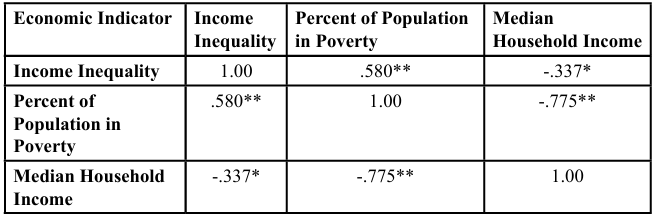
Table 1. Correlation between study variables
Since the three state economic variables appeared significantly correlated, we generated a composite state Economic Index Z-score by averaging the Z-scores of the three state economic variables. To assess validity, the state Economic Index Z-scores were correlated to six health outcomes using the Pearson product-moment correlation test. These correlations are noted in Table 2.
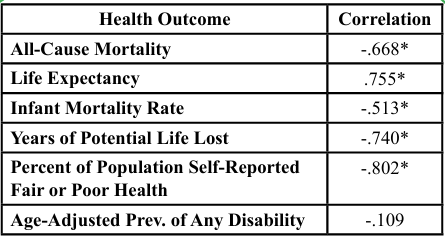
Table 2. Correlation of State Economic Index Z-Score and Health Outcomes
Significant correlations at the <.001 level were found between the state Economic Index Z-scores for all outcomes except age-adjusted prevalence of any disability. States with higher (more favorable) Economic Index Z-scores exhibited lower all-cause mortality, higher life expectancy, a lower infant mortality rate, less years of potential life lost, and lower percent of the population self-reporting being in fair or poor health. These results were consistent with an earlier study evidencing significant correlations between a state hazardous score (a measure of the strength of each state’s health policies) and state health outcomes [4].
Using the state composite Economic Index score, Table 3 compares the economic data for income inequality, percentage of the population in poverty, and median household income for the highest (best) twenty-five and lowest (worst) twenty-five states. T-test results indicated significant differences existed at the <.01 level between the highest and lowest states for each variable. The highest 25 states had less income inequality, 7.4 percent less poverty and a nearly twenty- thousand dollars ($19,876) higher median income.
Table 4 compares the twenty-five highest (best) Economic Index states and lowest (worst) Economic Index states on each of the health outcomes. Means and standard deviations for each of the health outcomes is provided. As shown in Table 4, significant differences at the <.001 level were found between the twenty-five highest (best) Economic Index states and the lowest (worst) Economic Index states on each health outcome, with the exception of the Age-Adjusted Prevalence of Any Disability.
Consistent with the previous correlation results, states with better Economic Index Z- scores had lower all-cause mortality rate, greater life expectancy, a lower infant mortality rate, less years of potential life lost, and a lower percent of the population self-reporting being in fair or poor health.
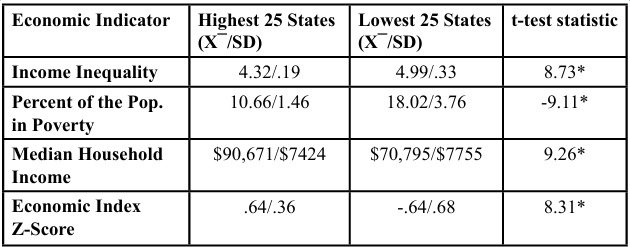
Table 3. Comparison of 25 Highest and Lowest States by Economic Indicator
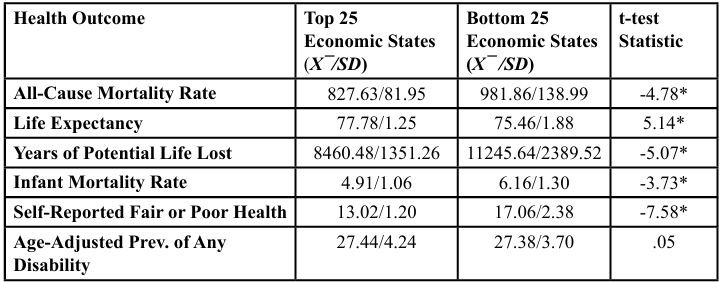
Table 4. State Health Outcomes by State Economic Index Score
Finally, calculations were performed to translate the data using the standardized mortality rate (SMR). From this calculation, we are able to compare observed vs expected numbers of deaths using a standard population. SMR calculations, and the related epidemiological calculation of Attributable Risk, provide additional important insight comparing high (best) Economic Index states with low (worst) Economic Index states. The SMR calculation noted that the lowest twenty-five Economic Index states had 24.3 percent more deaths observed than expected from the age-specific rates in the standard population (highest Economic Index states). The states with the lowest Economic Index had an observed death count of 2,356,349. Applying the mortality rate of the best Economic Index states to the worst would equate to an expected death count of 1,895,488. Economic status of the lowest economic states may account for 460,861 excess deaths.
Discussion
In a previous study, [4] it was found that state hazardous score (a measure of the strength of the state’s health policies) based on state rules, regulations and expenditures were highly correlated with widely referenced health outcomes including life expectancy, age- adjusted mortality rate, infant mortality rate, years of potential life lost (YPLL) and self-reported fair or poor health. In this study, we had similar findings based on state economic variables of median household income, percent poverty and income inequality as well as a composite Economic Index score combining those three variables. States with better scores had better health outcomes.
The body of evidence in academic literature confirms the importance of economic status as an independent variable impacting health status. For example, poverty and income inequality have a strong negative impact on health outcomes evidenced by higher rates of disease, increased mortality, shorter life expectancy, limited access to health care, nutritional deficiencies, greater exposure to environmental risks, inadequate housing, social isolation and stress. Reducing poverty and narrowing the gap between high-income earners and low-income earners will improve the health and wellbeing of populations [15]. This study supports that contention. Additional confirmatory evidence was noted when comparing each of the three economic variables and the composite Economic Index of the twenty- five highest (best) to the lowest (worse) twenty-five ranked states. Higher ranked states had significantly better outcomes for all but one outcome measure (Age-Adjusted Prevalence of any Disability). The calculation of a Standardized Mortality Rate (SMR) provided further confirmation.
The issue of policy, economics and health is complex. While there is no shortage of proposals to address poverty and income inequality there is an abundance of debate often without consensus on how these challenges should be met. It is not the intent of this article to advocate for specific proposals or programs, but to assess the importance of economic variables on health outcomes and, from the literature, suggest options and strategies for consideration by those in policy advocacy roles or in policy making positions at any level.
Hobbs and Wenzel (2020) suggest, “Reducing poverty and inequality requires a multi-pronged approach focusing on economic growth, social policies, and addressing systemic issues. Strategies include promoting education, increasing access to healthcare, boosting incomes for low-wage workers, expanding social safety nets, and combating discrimination [27].” Consistent with the above general strategies are programs to boost employment opportunities, job training and increase labor productivity leading to higher incomes. Strengthening social safety net programs like Earned Income Tax Credit, Child Tax Credit, the Supplemental Nutrition Assistance Program (SNAP) [28], expanding Medicaid and other public health insurance programs to increase healthcare access [29,30], investing in education to provide people with the skills and knowledge needed for economic success and greater participation in society, reducing income inequality by reversing recent tax policy to a more progressive income tax where higher earners pay a larger percentage of their income in taxes to help redistribute wealth and fund social programs [17,31] have all been suggested policy approaches found in the literature.
Our findings highlight the importance and vital role of health professionals as ‘policy advocates.’ The need for additional training of public health professionals toward developing proficiency in policy advocacy, both in terms of health and economic policy, is especially salient given these findings.
Several websites that provide evidence-based policy recommendations and training include https://cityhealthdashboard.com/, https://www. countyhealthrankings.org/strategies-and-solutions/what-works- for-health, https://amchp.org/, and https://www.changlabsolutions. org/phla. We look forward to continued research that focuses on the impact of health policy on health outcomes, as well as research that evaluates public health advocacy training and experience in undergraduate and graduate settings.
Limitations
The independent variables included three state economic variables used to assess the relationship with six widely referenced health outcomes. Similarly, given the significant interrelationships between the three state economic scores, we generated a composite Economic Index to represent a composite state economic score to rank states. We do not imply this is a definitive ranking. Clearly, there are other possible ways to rank states other than by economic indicators. Case in point, a previous study with similar findings to this study supported the use of state rankings based on state policies, expenditures, rules, and regulations as potential predictors of health outcomes [4].
The results of this study supported and confirmed the value of the socio-ecological model to understanding population health. Using other ways to rank states may result in different findings. However, state rankings using economic indicators which are well referenced in the literature, appear reasonable. Also, findings of this study rankings should be viewed as ephemeral and subject to change on an ongoing basis. For example, going forward, states that improve or worsen their economic standing may exhibit improved or poorer health outcomes.
To assess the validity of state rankings, we used multiple health outcome measures. We do not imply using these outcome measures are an inclusive definitive measure. There are other health outcome statistics that could have been used, either singly or as part of a larger composite which could have resulted in different findings. However, these particular outcome measures are frequently used, and several of these measures continue to be used by the Organization for Economic Cooperation and Development (OECD) [25], the World Health Organization (WHO) [26] and others who find these measures helpful in health policy discussions. As with any other statistical measures, these health statistics are subject to fluctuation over time. For this reason, we used the most recent available data for each source.
This study focused predominately on state economic indicators policies and their association to health outcomes overall. While states, as legal governing bodies have significant authority, a state with a low economic rank does not necessarily translate into poor population health throughout that state. Many towns and municipalities, for example, may or may not address economic challenges and have more or less favorable outcomes found in this study. Thus, we caution that the relationship between state economic variables and health outcomes cannot be generalized to specific areas within the state.
While this study assesses the relationship of state economics and health outcomes and suggests options and strategies for consideration by advocates and policy makers, it is not the intent, nor purpose, to promote, advance, nor dismiss or discredit the merits of any proposal. Such proposals need to be determined by informed study and involvement of many different stakeholders.
Conclusions
The purpose of this article was to assess the association between state economic status (using a composite Economic Index) and health outcomes. This investigation has offered a number of important considerations.
Economic policy matters: A plethora of research has noted that socio-economic status relates to health outcomes. The inter-related variables of income, employment status, and education are related to better health overall, but the evidence notes that they serve as a gradient that at each upward level, health outcomes become better [32]. How to improve economic outcomes, however, is a much debated and very complicated issue. A policy approach to improving economic status is an important consideration with many suggested strategies offered in the literature. This investigation, taking a state- by-state comparative analysis, offers additional consideration in terms of policy approaches at the geographical government level having significant influence over these decisions.
Geography matters: Curtis, et al., (1998) observed that while individual characteristics are very important for the health inequalities observed between people, their geographical setting also has some significance [33]. The work by Galea, et al., (2011) confirmed that area-level poverty plays a role in mortality overall [11]. This study supports this contention.
Ranking methodology provides a unique empirical perspective: Because of the influence each state government holds over policy, ranking methodology offers an important comparative analysis when considering the influence of economic policy on health outcomes.
Competing Interests:
The authors declare that they have no competing interests.
References
Institute of Medicine (US) Committee for the Study of the Future of Public Health. The Future of Public Health. Washington (DC): National Academies Press (US); 1988. View
Brownson, R. C., Erwin, P. C. (2024). Revisiting The Future of Public Health: The Good, the Bad, and the Ugly. Am J Public Health. May; 114(5):479-485. View
McGowan, A. K., Greeley, S., Griffis, R., Polan, S. L. (2024). Thirty-Six Years After the 1988 IOM Future of Public Health: Stop Ruminating and Start Taking Action. Am J Public Health. May; 114(5):486-488. View
Remmert, D. M., O’Rourke, T. (2025). Quantifying the Impact of State Health Policy on State Population Health Outcomes. Health Promotion Practice. 0(0). View
Satcher, D., Fryer, G. E. Jr, McCann, J., Troutman, A., Woolf, S. H., & Rust, G. (2005). What if we were equal? A comparison of the black-white mortality gap in 1960 and 2000. Health Aff (Millwood). 24(2):459-464. View
Anyanwu, E. C. (2024). Maternal and child health policy: A global review of current practices and future directions. World J Adv Res Rev. 21(2):1770-1781. View
Ogugua, J. O., Anyanwu, E. C., Olorunsogo, T., Maduka, C. P., & Ayo-Farai, O. (2024). Ethics and strategy in vaccination: A review of public health policies and practices. International Journal of Science and Research Archive. 11(1), 883-895. View
Ederer, D. J., Panik, R. T., Botchwey, N., & Watkins, K. (2023). The Safe Systems Pyramid: A new framework for traffic safety. Transportation Research Interdisciplinary Perspectives. Sep; 21:100905. View
Levy, D. T., Tam, J., Kuo, C., Fong, G. T., & Chaloupka, F. (2018). The impact of implementing tobacco control policies: the 2017 tobacco control policy scorecard. Journal of Public Health Management and Practice. 24(5), 448-457. View
Pettinger, T. (2020). The relationship between economics and politics. Economics Help Blog. [Accessed 6/20/2025]. View
Galea, S., Tracy, M., Hoggatt, K.J., DiMaggio, C., & Karpati, A. (2011). Estimated deaths attributable to social factors in the United States. American Journal of Public Health. 101(8), 1456-1465. View
Venkataramani, A. S., O’Brien, R., Whitehorn, G. L., & Tsai, A. C. (2020). Economic influences on population health in the United States: Toward policymaking driven by data and evidence. PLoS Med. 17(9): e1003319. View
Kawachi, I., Kennedy, B. P. (1999). Income inequality and health: pathways and mechanisms. Health Services Res. 34(1 Pt 2): 215-227. Accessed July 7, 2025. View
Avanceña, A. L. V., DeLuca, E. K., Iott, B., et al. (2021). Income and Income Inequality Are a Matter of Life and Death. What Can Policymakers Do About It? American Journal of Public Health. 111(8):1404-1408. View
Pickett, K. E., & Wilkinson, R. G. (2015). Income inequality and health: A causal review. Social Science and Medicine. 128:316-326. View
Khullar, D., & Chokshi, D. A. (2018). Health, income, & poverty: Where we are & what could help. Health Affairs. 10(10.1377), 10-1377. View
Finkelstein, D. M., Harding, J. F., Paulsell, D., English, B., Hijjawi, G. R., Ng’andu, J. (2022). Economic Well-Being And Health: The Role Of Income Support Programs In Promoting Health And Advancing Health Equity. Health Affairs. 41(12):1700-1706. View
Fang, W., Cao, Y., Chen, Y., Zhang, H., Ni, R., Hu, W., Pan, G. (2023). Associations of family income and healthy lifestyle with all-cause mortality. J Glob Health. Nov 15;13:04150. View
Zissimopoulou, O., Leontidou, E., Tsiptsios, D., Manolis, A., Ioannides, D., Trypsiani, I., Steiropoulos, P., Constantinidis, T. C., Tripsianis, G., Nena, E. (2020). Association of Family Income with Health Indices and Healthcare Utilization in a Large Sample of Residents in Northern Greece. Maedica (Bucur). Dec; 15(4):490-502. View
Office of Disease Prevention and Health Promotion, Office of the Assistant Secretary for Health, Office of the Secretary, U.S. Department of Health and Human Services. Healthy People 2030, 2020. View
Knifton, L., Inglis, G. (2020). Poverty and mental health: policy, practice and research implications. BJPsych Bulletin. 44(5):193 196. View
Siddiqui, F., Salam, R. A., Lassi, R. S. , Das, J. K. (2020). The Intertwined Relationship Between Malnutrition and Poverty. Frontiers in Public Health. Volume 8. View
Apenyo, T., Vera-Urbina, A. E., Ahmad, K., Taveira, T. H., Wu, W. C. (2022). Association between median household income, state Medicaid expansion status, and COVID-19 outcomes across US counties. PLoS ONE. 17(8 August). View
Parolin, Z., Lee, E. K. (2022). The Role of Poverty and Racial Discrimination in Exacerbating the Health Consequences of COVID-19. The Lancet Regional Health - Americas. 7. View
Organization for Economic Cooperation and Development. (2023). Health at a glance: 2023. View
World Health Organization. World health statistics 2023: A visual summary (2023). View
Hobbs, B. K., & Wenzel, N. G. (2020). Income Inequality and Poverty: Are We Asking the Right Questions? New Perspectives on Political Economy, 16(1-2), 17-38. View
Hamad, R., Gosliner, W., Brown, E. M., et al. (2022). Understanding Take-Up Of The Earned Income Tax Credit Among Californians With Low Income. Health Affairs. 41(12):1715-1724. View
Haeder, S. F., Moynihan, D. P. (2023). Most Americans support minimizing administrative burdens for Medicaid recipients as the public health emergency ends. Health Affairs Scholar. 1(1). View
Lax, Y., Bouchelle, Z., & Vasan, A. (2025). Financial Assistance and Access to Care. Social Drivers of Health. American Academy of Pediatrics. Itasca, IL. View
Himmelstein, K. E. W., Tsai, A. C., Venkataramani, A. S. (2024). Wealth Redistribution to Extend Longevity in the US. JAMA Internal Medicine. 184(3):311-320. View
Marmot, M. G., Rose, G., Shipley, M., et al. (1978). Employment grade and coronary heart disease in British civil servants. J Epidemiol Community Health. 32(4):244-249. View
Curtis, S. and Rees Jones, I. (1998). Is There a Place for Geography in the Analysis of Health Inequality? Sociology of Health & Illness. 20: 645-672. View