
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 10 (2026), Article ID: JPHIP-254
https://doi.org/10.33790/jphip1100254Research Article
Comparison of Barriers Against Utilization of Free or Reduced Cost Health Care in Urban and Rural Clinics in Southwest Missouri
Kip Thompson*, Robert Niezgoda, Nima K. Lal, Patricia J. Horton, and Sakinya Palakurthi
Missouri State University, 901 S. National, Springfield, MO 65897, United States.
Corresponding Author Details: Kip Thompson, Associate Professor, School of Health Sciences, Missouri State University, 901 S. National, Springfield, MO 65897, United States.
Received date: 09th January, 2026
Accepted date: 06th March, 2026
Published date: 09th March, 2026
Citation: Thompson, K., Niezgoda, R., Lal, N. K., Horton, P. J., & Palakurthi, S., (2026). Comparison of Barriers Against Utilization of Free or Reduced Cost Health Care in Urban and Rural Clinics in Southwest Missouri. J Pub Health Issue Pract 10(1): 254.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Barriers exist in the United States which potentially prevent 46 million Americans from having reliable access to healthcare. While the Affordable Care Act was implemented to address this issue, as recently as 2024, it was estimated that 27.2 million eligible Americans still did not possess insurance. Access is most often limited due to being under or uninsured, but can also occur on racial/ethnic lines, socioeconomic status, and proximity to health care providers. In response to discrepancies in access to care, programs at the state and federal level have been implemented including Medicare/Medicaid and federally qualified community health centers (FQHC’s). Even when controlling for factors related to access, many people who are eligible for federal support do not utilize free healthcare provided by community health centers. Little research exists on the effects of behavior on healthcare utilization, especially between rural and urban populations. This research was conducted to determine what barriers, if any, exist which prevent under or uninsured patients from utilizing free or reduced cost clinics in rural and urban settings in Southwest Missouri. Our findings indicate that primary factors affecting utilization differ significantly between rural and urban areas. Secondary factors in care choice were related to the perception of quality. Additionally, significantly more respondents in rural areas would continue to utilize free or reduced cost facilities if given the choice compared to respondents from the urban areas. Regardless, respondents from both locations indicated their preferred care would be with a private provider. The lack of consistent providers at FQHC’s was perceived as a barrier with many respondents indicating they were discriminated against in their health care because they do not have a single primary care provider. These results may imply that access to a consistent provider and location may play a role in perceived barriers to care.
Key words: Health Care, Barriers, Utilization, Perception, Quality, Uninsured, FQHC
Introduction
Access to healthcare has been a serious problem in the United States for several decades and continues to persist. Historically, access to care was limited by proximity to a provider, especially for rural populations. Care was based on a fee provided service, with each individual responsible for direct payment to the provider.In response to pay freezes and a poor economy during World War II, United States manufacturers began providing basic catastrophic health care as an incentive to prospective employees [1]. This system evolved into the current model where 64% of all Americans receive some form of universal health coverage through their employer [2]. This system of employer-provided insurance led to high utilization and subsequent increases in the cost of care. As a result, many Americans were left without access to health care because of prohibitive costs. By 2006, the number of uninsured individuals was estimated to be 46 million, with the number steadily increasing to a level of almost 50 million by 2009 [3,4]. To address this growing issue, the federal government initiated several programs specifically aimed at the under and uninsured. In 1965, the United States created Medicare and Medicaid under Titles XVIII and XIX respectively of the Social Security Act. This program provides health insurance to individuals over the age of 65 or those with low income (pegged against the Federal Poverty Level). The primary purpose was to reduce the level of health disparities in the United States by providing a low-cost alternative to the more standard system of employer-based insurance [5]. Additionally, in the 1960’s, efforts were undertaken through President Johnson’s War on Poverty, to reduce the number of uninsured through the creation of federally qualified health centers (FQHC’s) [6]. These centers provide a safety net to the under and uninsured by providing comprehensive care to those least able to afford it [7,8].
More recently, efforts have been expanded through passage of the Affordable Care Act, which looked to decrease the number of uninsured by up to 32 million [9]. Even with these efforts, the number of uninsured in the US as of 2024 is estimated at 27.2 million [10]. Even with expanded insurance coverage and coverage through FQHC’s, a large proportion of those eligible for free or reduced cost healthcare do not access this care, often delaying first treatment by a significant amount of time [11]. For example, as recently as 2011, only 15% of those eligible for utilization of a FQHC did so [8]. Individuals don’t use FQHC’s for various reasons including difficulties in applying for and using the health care system, limited hours of operation, long wait times and lack of services such as transportation and child care [8]. Lack of appointment flexibility and restricted hours were also reported as barriers to utilization. The most commonly reported reason for not seeking care was lack of insurance (50.8%). Even when told FQHC’s did not require insurance and charge based on income, respondents reported they could not afford the minimal fees [8]. While many reasons exist for lack of utilization, most research has focused on financial barriers to access [12]. Reducing barriers to healthcare is critical. Regular access to reliable health care, especially for groups which are typically categorized as underserved (those with low income, low socio-economic status, racial and ethnic minorities, etc.) has been shown to reduce disparities, especially in primary care [13,14].
While steps have been taken to increase access to healthcare, discrepancies still remain. Poor access to health care is influenced by a wide range of factors and the interaction between these factors [15,16]. Most studies have looked at financial barriers to health care access and utilization, especially the inability to afford insurance. While insurance is an important component in access to health care, even when free care is provided, many uninsured individuals delay seeking medical care. Nonfinancial barriers (accessibility, acceptability and accommodation) are common reasons why people delay or don’t use health care and may actually exceed financial barriers [17]. This implies that even when free care may be available, some people may not be able to or elect not to use community health care clinics [17]. A large amount of research has also been conducted on the effects of distance to providers on utilization of safety-net health care providers. As the distance to a safety net provider such as a community health clinic decrease, the access to health care increases for eligible participants. However, even when the uninsured live close to a safety net provider, the disparity in access to care compared to someone with insurance is still high [18]. One suggested reason for this is the impact of open access and walk in coverage to wait for times and misperceptions about the quality of care. Most community clinics operate on a walk-in basis and, at times, have long wait times to be seen by a provider. These long wait times may serve as a barrier to access of care for uninsured persons [18,19]. This may be especially important in Missouri where the health care safety net may be inadequate to meet the need [20]. While the quality of care is perceived to be lower, free or reduced fee community health clinics have been shown to reduce any disparities in the health of the uninsured compared to the insured, specifically in the areas of primary care, preventive services (such as prenatal care for expecting mothers) and access to medications [13].
Other studies have found similar benefits of these types of clinics in reaching an underserved population with most respondents satisfied with the care they receive, although for specialties (pharmacy, mental health), a high proportion of those utilizing community health clinics feel their needs are unmet [3]. Retention and long-term utilization of government subsidized programs appear to be related to the eligibility criteria of the program and the frequency of recertification. Age and sex appear to have an influence on the initial and continued utilization. Younger individuals were less likely to continue with use compared to older individuals and males were less likely to stay enrolled compared to females [3]. Additionally, while Medicare/ Medicaid was designed to reduce disparities in access to healthcare across all demographics, this has not been the case. Based on reported prostate screening episodes for Medicare recipients, white males were more likely to receive prostate exams compared to black males and high-income males were more likely to receive a prostate exam compared to low-income males. Additionally, men who receive a prostate exam through community health clinics are more likely to receive an influenza vaccination, regardless of the aforementioned barriers [21]. The same effects have been seen in the United Kingdom, where the National Health Service has provided equal access to primary care and services since 1948, but disparities continue to exist [5].
The results of previous research indicate other factors besides race and socioeconomic status influence the utilization of health care services, even when they are provided at no or reduced cost, causing utilization to remain low. This implies behavioral factors may play a major role in health care choices and utilization; however, little research has been done to tease out which behaviors may be the most important [13]. Determining which behaviors affect utilization is important in helping to guide future policy decisions regarding access to care. Reducing barriers to healthcare is critical. Regular access to primary care has been shown to reduce or mitigate the impacts of many socioeconomic factors related to health outcomes, including income and race [13]. Reducing poor health outcomes will become more and more important as health care costs continue to rise.
The aim of this research is to determine if factors other than cost are barriers to utilization, and if so, what these barriers might be. Specifically, little research has been conducted on behavioral issues or perceptions as barriers to utilization of federally funded community health centers. It is hoped that through this research, information can be gained regarding the effects of behavior and perception on health care utilization. New information gained from the research will assist policy planners to develop more tools when developing programs which will increase utilization by decreasing barriers. To that end, the primary research question is: What are the primary barriers against utilization of free community health care clinics by the uninsured?
Methods
Because there is a lack of knowledge in the effects of behavior in healthcare utilization, a quantitative research design using a self or researcher administered questionnaire was utilized [22]. Utilization of healthcare often involves several decision-making processes by the individual, and a firm understanding of those decision-making processes is needed to adequately address barriers regarding use of healthcare.
Data was collected using a self-completed, semi-structured individual questionnaire. Questions were derived from the Patient Satisfaction Questionnaire Short-Form (PSQ-18) [23]. Check-Box type questions regarding the decisions used in healthcare utilization were asked of all participants in the study. Potential participants were recruited from two local free health clinics, the original FQHC in Springfield, Missouri (urban) and a free or reduced cost clinic at the Polk County, Missouri (rural) Health Center. Springfield, Missouri, located in S.W. Missouri, is the third largest city in the state. As of 2024, the population of the city of Springfield is 170,596 with a metropolitan area population of 496,975. Springfield is mostly white (86%) with a mix of other racial/ethnic groups (2% African American, 2% Asian, 5% Hispanic, and 1% other) has a median household income of $67,219, with 11.2% of the population below the federal poverty level. Ninety-three percent of the residents have at least a high school diploma [24]. Polk County Missouri is also in S.W. Missouri and is located directly north of Greene County Missouri where Springfield is located. As of 2024, the population of Polk County is 32,444 with 11,900 living in the city of Bolivar, the county seat. Polk County is mostly white (91%) with a mix of other racial/ethnic groups (1% African American, 1% Asian, 3% Hispanic, and 4% other) has a median household income of $59,647, with 16.3% of the population below the federal poverty level. Eighty-eight percent of the residents have at least a high school diploma [24]. To ensure an adequate sample size, questionnaires were provided to all persons utilizing these clinics. However, priority was given to first time users. Minimum sample sizes for both locations were set at 25 new participants with questionnaires provided for approximately six months at both locations.
Because of the nature of data collection, the number of questions was kept to a minimum (28 questions total) to allow participants to rapidly complete the questionnaire related to the research topic. To minimize bias, the same questions were asked at all study locations regardless of the participants. The staff providing the questionnaire at all study locations were trained on the purpose of the study and the questions prior to providing the questionnaire to potential participants. Bilingual questionnaires in English and Spanish were utilized to reduce barriers related to the person’s primary language. All staff handing out the form used a prescribed script to describe the overall aims of the study to any potential participant and to acquire informed consent. All information collected was analyzed to produce descriptive information (mean, percentages, etc.) related to the participants. All facets of this research project were approved by the Missouri State University Institutional Review Board (IRB# IRB FY2016-196) prior to implementation of the study.
Data was analyzed using IBM SPSS 24 and Excel. Differences in means were tested using an Independent Sample t-test. A Chi-Square test was performed to test for differences in questionnaire responses between Springfield and Polk County. Correlations between factors were determined using a Spearman’s Correlation test. Significance for all tests was set at p< 0.05. This research followed all STROBE aims related to observational research studies [25].
Results
Demographics (Table 1):
There was a significant difference between average age, insurance status and the reasons for not having insurance between Springfield and Polk County (p < 0.0001). Patients in Polk County were more likely to be older and uninsured. Respondents at both locations indicated cost was the primary factor for not having insurance.
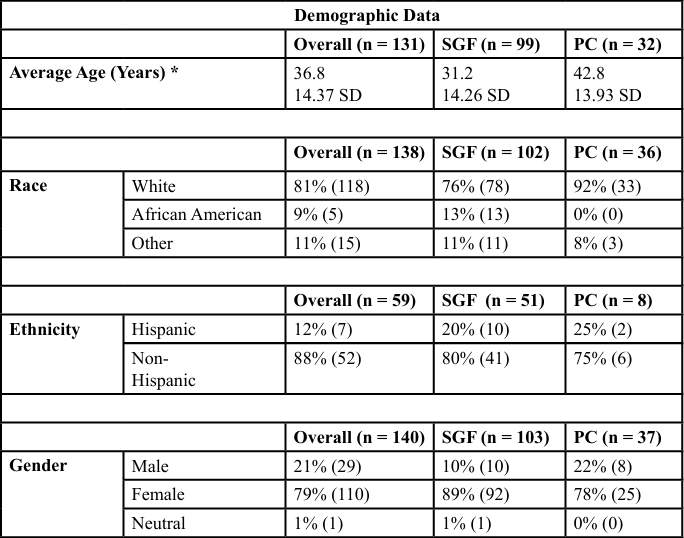
Table 1. Demographic results based on the questionnaire between the health center in Springfield (SGF), Missouri (Urban) and the Polk County (PC) Missouri (Rural). An independent samples t-test was used to compare the mean age between locations. A Chi-Square test was used to determine any significant differences in categorical responses between locations. The level of significance for all tests was α = 0.05. Note, due to rounding, values may not add to 100%.
Characteristics of Care (Table 2):
Respondents at Polk County were more likely to seek care for chronic or reoccurring health problems (41%) while those in Springfield sought care for pregnancy related issues (29%). For both locations, cost due to lack of income or insurance was the most reported reason they did not seek care. Respondents in Polk County (63%, p < 0.05) indicated they did not seek care due to cost compared to those in Springfield (29%, p < 0.05). Significantly more respondents sought care at a free or reduced cost clinic in Polk County (61%) compared to Springfield (24%) (p = 0.004). More people in Springfield (25%) indicated they usually receive care from a private doctor compared to Polk County (14%) (p = 0.004). The preferred location of service differed by location.
Significantly more respondents from Polk County (36%) would choose a free or reduced cost location if care were free while only 28% would do so from Springfield (p = 0.029). Additionally, more respondents from Springfield would choose an urgent care facility (8%) or emergency room (5%) if care were free compared to Polk County (0% for both). However, for both locations, respondents indicated their preferred location for care would be with a private provider (58% and 57% respectively).
Care Choice (Table 3):
Primary factors for the location where respondents seek care differed significantly by location (p = 0.001). For Polk County, 41% of all respondents indicated the primary factor on where to seek care was related to cost. Conversely, 25% of respondents from Springfield indicated cost was a primary factor. These numbers are similar for factors listed on where the patient sought care that day. For Polk County, 48% indicated the primary factor was cost while for Springfield, 24% indicated cost as a primary factor (p < 0.0001). It is important to note that for both locations, perception of quality was the primary or secondary factor which influenced where they sought care (Table 4).
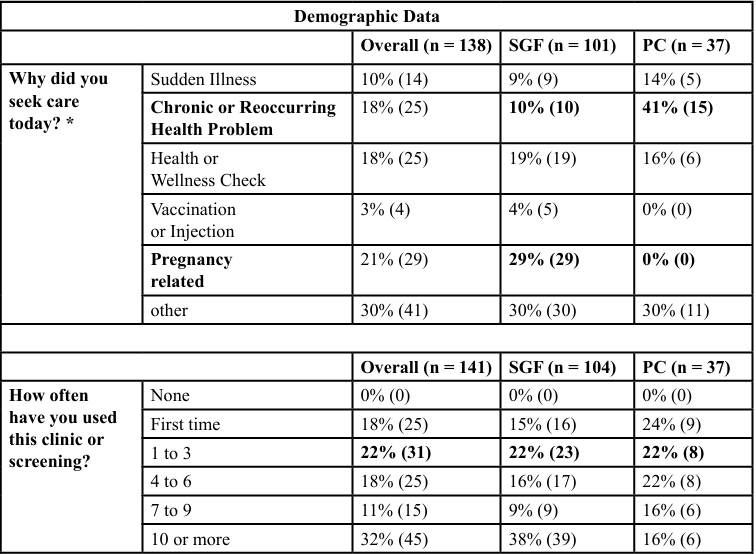
Table 2. Results of the questionnaire related to characteristics of care the health center in Springfield (SGF), Missouri (Urban) and the Polk County (PC) Missouri (Rural). Factors which were significantly different between the sites are denoted by an asterisk and bold font. Differences in responses between both locations were analyzed using a Chi-Square test with a level of significance of α = 0.05. While not significant, it is important to note that the majority of individuals at both locations have not felt unfairly treated. However, of those who did feel unfairly treated, the primary response was treated unfairly due to insurance status. Note, due to rounding, values may not add to 100%.
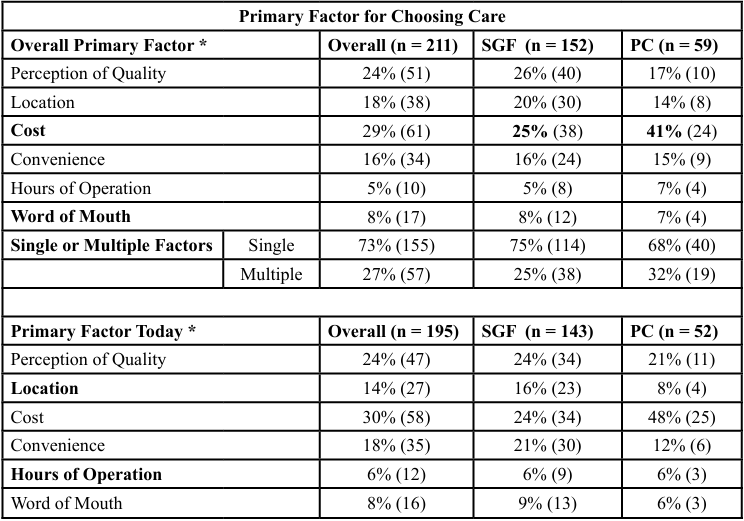
Table 3. Results of the questionnaire related to the primary factors influencing choice of care between the health center in Springfield (SGF), Missouri (Urban) and the Polk County (PC) Missouri (Rural). Factors which were significantly different between the sites are denoted by an asterisk and bold font. Differences in responses between both locations were analyzed using a Chi-Square test with a level of significance of α = 0.05. Note, due to rounding, values may not add to 100%.
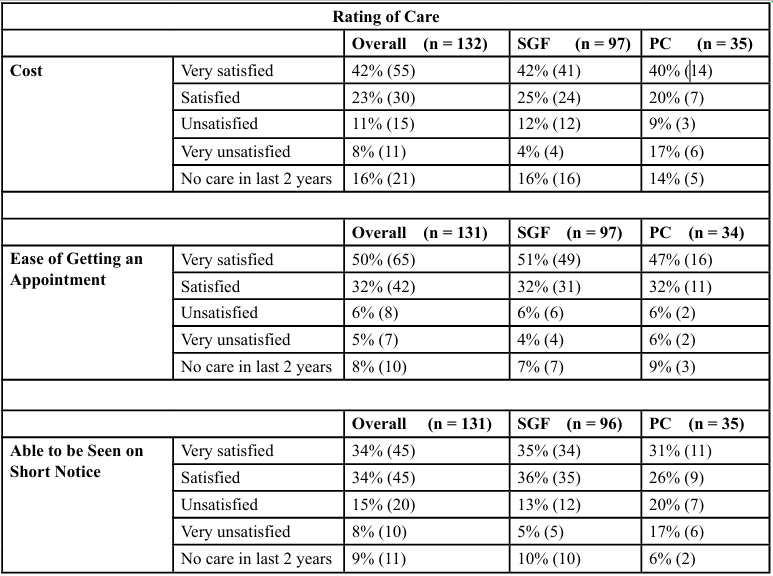
Table 4. Results of the questionnaire related to the rating of care between the health center in Springfield (SGF), Missouri (Urban) and the Polk County (PC) Missouri (Rural). No significant differences were found between care ratings for each factor between each location (α = 0.05). Note, due to rounding, values may not add to 100%.
Discussion
Based on the results of this study, several conclusions can be drawn. First, economies at both locations are depressed with a high proportion of users at or below the federal poverty level. As with other studies, cost seems to be the most important factor for utilizers of both clinics. Those utilizing the clinic in Polk County indicated cost as the most important factor. This is most likely related to the proportion (14.5%) of people with no insurance in Polk County [26]. These uninsured residents are most likely to utilize the clinic in Polk County. However, for individuals using the clinic in Springfield (an urban location), perception of the quality of care was the most important factor (although cost was a close second). This might be related to differences in location, age of the patients, and the reason why the clinics were used. The Springfield respondents were mostly younger females utilizing the clinic for pregnancy related issues. Polk County respondents were older and mostly used the clinic for chronic disease issues. For both locations, cost was also a factor in the inability to obtain insurance, although most were eligible for Medicaid/MO Health Net assistance (which was utilized more in Springfield). Most respondents at both locations indicated they were satisfied with the level of care provided at each location. However, given a choice, respondents at both locations indicated they would prefer to receive care from a private provider. Interestingly, significantly more respondents from Springfield indicated that if care were free, they would choose to receive their care from an emergency room. This may indicate a persistent belief that emergency rooms provide better quality of care for underinsured people in urban environments. Alternatively, individuals may prefer emergency rooms as their source of primary care because of accessibility (open 24 hours per day, 7 days per week) and access to a complete range of services where no referrals are needed. More research needs to be done to identify primary factors which cause individuals to prefer care in emergency rooms as well as the perception of quality in free clinics versus emergency rooms. This could potentially reduce the strain on emergency room use for non-emergency cases. Finally, for both locations, 12% to 15% of the respondents indicated they felt they were treated unfairly because of their insurance status (Medicaid/MO Health Net or no insurance at all). It is possible these respondents would use a private provider (as indicated above) but feel they are discriminated against because of their insurance status. This could discourage them from seeking care at a free or reduced cost clinic.More research needs to be conducted to determine the effects of perception and insurance status on utilization.
Many studies have identified financial barriers to health care access and utilization, especially as they relate to inability to afford insurance. This research also found cost (financial) barriers were the most common reason respondents did not seek care. While insurance is an important component in access to health care, other factors may also be important. Even when free care is provided, many uninsured individuals delay seeking medical care. Nonfinancial barriers (accessibility, acceptability and accommodation) were also found to be common reasons why people delay or do not use health care. These non-financial barriers may exceed financial barriers in importance. This conclusion implies that even when free care may be available, some people may not be able to, or elect not to, or may elect not to use community health care clinics. In the current research, while cost was the most often reported barrier to utilizing care, this research demonstrates that insurance status may be a driver in the perception of the quality of care and treatment, which could act as a barrier to utilization. A majority of respondents would prefer to receive care form a private provider because they perceived the care is better. More research should be conducted to better assess the impact of the perception of care on utilization of free or reduced cost community clinics by the under or uninsured.
The large overall sample size (n = 141) is a strength of this study as is the utilization of a standardized script and consistent training of staff prior to implementation of the study regardless of location. Additionally, data transfer and coding for SPSS was checked by three individuals prior to analyses to ensure no data errors occurred. In general, the design of the study as well as training helped to reduce bias (cognitive, social, and statistical). However, weaknesses do exist. While the overall sample size was large, most responses came from the urban clinic (n = 104) versus the rural clinic (n = 37). This could have resulted in selection bias. Additionally, the differences in participant characteristics such as insurance status observed in this study might slightly impact the generalizability of our findings. Finally, data was only drawn from clinics located in Southwest Missouri, part of the Ozarks Region. While results may be generalizable to areas within the Ozarks with similar demographics, caution should be taken when trying to generalize these results across other areas.
All authors declare they have no competing interests. This project was funded by a Missouri State University Summer Research Faculty Grant.
References
Smith, K. (2023). A (Brief) history of health policy in the United States. Delaware Journal of Public Health, 9(5), 6-10. View
Shi, L., and Singh, D.A. (2022). Delivering health care in America: A systems approach (8th ed.). Burlington, MA: Jones & Bartlett Learning. View
Taylor, E.F., McLaughlin, C.G., Warren, A.W., and Song, P.H. (2006). Who enrolls in community-based programs for the uninsured, and why do they stay? Health Affairs, 25(3), 183- 191. View
Denavas-Wait, C., B.D. Proctor, and J.C. Smith. (2010). Income, Poverty, and Health Insurance Coverage in the United States: 2009. U.S. Department of Commerce. View
Gornick, M.E. (2003). A decade of research and disparities in Medicare utilization: Lessons for the health and health Care of vulnerable men. American Journal of Public Health, 93, 753- 759. View
Adashi, E.Y., Geiger, H.J., M.D. Fine. (2010). Health care reform and primary care – the growing importance of the community health center. New England Journal of Medicine, 362(22): 2047-2050. View
Shi, L., Lebrun, L. A., Tsai, J., and Zhu, J. (2010). Characteristics of ambulatory care patients and services: A comparison of community health centers and physicians’ offices. Journal of Health Care for the Poor and Underserved, 21(2010), 1169- 1183. View
Almufleh, A., T. Gabriel, L. Tokayer, M. Comerford, A. Alaqeel and P. Kurlansky. (2015). Role of community health outreach program “Living for Health” in improving access to federally qualified health centers in Miami-Dade County, Florida: A cross-sectional Study. BMC Health Services Research, 15:118: 1-8. View
Isola, S. and Reddivari, A.K. (2023). Affordable Care Act. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. View
Cohen, R.A., E.M. Briones, I. Sohi. (2025). Health Insurance Coverage: Early release of estimates from the National Health Interview Survey, 2024. National Center for Health Statistics. View
Sommers, B.D. and Epstein, A.M. (2010). Medicaid expansion – the soft underbelly of health care reform? The New England Journal of Medicine, 363(22), 2085-2087. View
Gertz, A.M., Frank, S., and Blixen, C.E. (2011). A survey of patients and providers at free clinics across the United States. Journal of Community Health, 36, 83-93. View
Politzer, M., J., Yoon, J., Shi, L., Hughes, R.G., Regan, J, and Gaston, M.H. (2001). Inequality in America: The contribution of health centers in reducing and eliminating disparities in access to care. Medical Care Research and Review, 58(2), 234- 248. View
Rust, G., Fryer, G., Phillips, R., Strothers, H., and Satcher, D. (2004). Modifiable determinants of healthcare utilization within the African-American population. Journal of the National Medical Association, 96(6), 1169-1177. View
Shi, L., and Stevens, G.D. (2005). Vulnerability and unmet health care needs. The influence of multiple risk factors. Journal of General Internal Medicine, 20, 148-154. View
Elovainio, M., T. Jaaskelainen, S. Koskinen, A. Aalto. (2025). Risk factors for unmet health care need: Evidence from the Large Population-Based Healthy Finland 2022-Cohort. European Journal of Public Health, 00: 1-7. View
Kullgren, J. T., McLaughlin, C. G., Mitra, N., and Armstrong, K. (2012). Nonfinancial barriers and access to care for U.S. adults. Health Services Research, 47(1), 462-485. View
Hadley, J. and Cunningham, P. (2004). Availability of safety net providers and access to care of uninsured persons. Health Services Research, 39(5), 1527-1546. View
Kendall, D., Wofford, D, Murdock, K. (2023). Revitalizing safety net hospitals: Protecting low-income Americans from losing access to care. Third Way, Washington, DC, USA. View
Miller, G.R., N.A. Kayani, S.G. Homan. (2005). Report on the health care safety net in Missouri. Missouri Department of Health and Senior Services.
Zurl, H., Pohl, K.K., Korn, S.M., Piccolini, A., Qian, Z., Xiao, B., …, Cole, A.P. (2025). Racial disparities in the use of MRI and PET scan among Medicare beneficiaries with prostate cancer. The Prostate, 85(15), 1386-1394.
Strauss, A., and Corbin, J. (2014). Basics of qualitative research: Research techniques and procedures for developing grounded theory, 4th ed. Newbury Park, CA: Sage. View
Marshall, G. N., and Hays, R. D. (1994). The Patient Satisfaction Questionnaire Short Form (PQS-18). Santa Monica, CA. RAND. View
Census Quick Facts. (2024). View
STROBE. (2025). STROBE Checklist of items that should be included in reports or observational studies. View
National Institute of Health (NIH), (2026). An ecosystem of health disparities and minority health resources: Missouri Insurance Tables. Washington, DC. View