
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 10 (2026), Article ID: JPHIP-259
https://doi.org/10.33790/jphip1100259Research Article
Self-Efficay with Using Recommended Personal Protective Equipment and COVID-19 Positivity: A Case- Control Study
Robert Niezgoda1,2*, Christine Petersen1, Natoshia Askelson3, Jonathan Platt1, John Flunker1, and Michael Pentella1
1Department of Epidemiology, College of Public Health, University of Iowa, Iowa City, Iowa, 52242, United States.
2Master of Public Health Program, School of Health Sciences, Missouri State University, Springfield, Missouri, 65897, United States.
3Department of Community and Behavioral Health, College of Public Health, University of Iowa, Iowa City, Iowa, 52242, United States.
Corresponding Author Details: Robert Niezgoda, PDH, MPH, Assistant Professor, Master of Public Health Program, Missouri State University, 901 S. National Avenue, Springfield, Missouri, 65897, United States.
Received date: 12th March, 2026
Accepted date: 07th May, 2026
Published date: 09th May, 2026
Citation: Niezgoda, R., Petersen, C., Askelson, N., Platt, J., Flunker, J., & Pentella, M., (2026). Self-Efficay with Using Recommended Personal Protective Equipment and COVID-19 Positivity: A Case- Control Study. J Pub Health Issue Pract 10(1): 259.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Proper use of personal protective equipment (PPE) and training have been identified as effective measures for decreasing transmission of SARS-CoV-2 in healthcare settings. However, health care personnel (HCP) self-efficacy of properly using recommended PPE and COVID-19 positivity has not been explored. HCP in clinical and non-clinical roles are a vital part of the healthcare system infrastructure. Understanding how self-efficacy of PPE use affected SARS-CoV-2 positivity is important to inform future pandemic and infection prevention interventions.
Objective: The study purpose was to evaluate associations between self-reported comfort with properly using recommended PPE as a measure of self-efficacy among HCP in clinical and non-clinical roles and COVID-19 positivity. We hypothesized that HCP with lower self-efficacy, will have higher odds of COVID-19 positivity.
Methods: We conducted a case-control study of the association between self-efficacy as measured by self-reported comfort with using recommended PPE and COVID-19 positivity among HCP using data from the PReventing Emerging infections through Vaccine Effective Ness Testing (PREVENT) study, a multicenter SARS-CoV-2 vaccine effectiveness case-control study of HCP (n=6,983) in academic medical centers located in 15 metropolitan areas of 13 U.S. states between January 2021 and May 2022. We used a categorical variable of self-reported comfort level with properly using recommended PPE (very comfortable, somewhat comfortable, somewhat uncomfortable, very uncomfortable) as the primary exposure variable conceptualized as an indicator of self-efficacy of using recommended PPE.
Results: HCP reporting being very uncomfortable with properly using recommended PPE had greater odds of COVID-19 positivity (aOR=1.58, 95% CI: 1.02, 2.44) compared to HCP who were very comfortable using recommended PPE.
Conclusions: Findings are important for future pandemic response efforts and infection control strategies. Additional research is warranted regarding HCP self-efficacy of PPE use, efficacy of PPE training modalities, and self-efficacy’s influence on other protective behaviors in the work setting and community.
Keywords: Self-Efficacy, PPE, Infection Control, Pandemic Preparedness, SARS-CoV-2
Introduction
Proper use of personal protective equipment (PPE) and training have been identified as effective measures for decreasing transmission of SARS-CoV-2 in healthcare settings [1-3]. Previous research has focused on efficacy of different types of PPE (gloves, face masks, N95 respirators, face shields), PPE use during procedures, monitoring of PPE use, and the need for training [1-3]. Other research has described PPE adherence, fit, proper use [4] attitude towards PPE, [5] PPE design, complexity of use, other technical aspects [6-8] and PPE skills training and awareness levels [9,10]. Additional research has focused on measures of high levels of self-efficacy as a predictor of engaging in protective health behaviors [11,12]. The impact of COVID-19 among healthcare personnel (HCP) and hospital risk factors such as use of PPE, clinical exposures, and self- reported community exposures have also been explored [13-16]. However, HCP self-efficacy of properly using recommended PPE and association of COVID-19 positivity when considering mode of training received (online, in-person, group) and other important factors have not been explored [1]. HCP in clinical and non-clinical roles are a vital part of the healthcare system infrastructure who vary by race, ethnicity, biological sex, educational attainment, socioeconomic status (SES), and clinical- and non-clinical roles [17,18]. It is important to understand how self-efficacy of PPE use affected SARS-CoV-2 positivity to inform future pandemic preparedness efforts and infection prevention interventions.
The current study is unique to examine the association of perceived self-efficacy and using recommended PPE and PPE training received with COVID-19 positivity. This is important as self-efficacy is a foundational predictor of short- and long-term success in health education and behavior change [11] which become vitally important for the protection of HCP during pandemic response. Self-efficacy is viewed as influencing many facets of one’s behavior and learning [11] and contributes to changing and maintaining behaviors through expected outcomes of behavior, ability to successfully complete the behavior, and actual outcomes of behaviors [11]. Levels of self efficacy are further affected by mental and physiological responses [11].
Self-efficacy expectations are explained to be learned through processes that perceived levels of self-efficacy [11]. These processes include “performance accomplishments” or direct experience; “vicarious experience” or observing others; “verbal persuasion” or verbal feedback; and “physiological state” or physiological responses (stress, agitation, etc.) [11].
HCP’s self-efficacy would therefore depend on personal experience of successfully using PPE, observing PPE use by other HCP, receiving feedback on PPE use from others, and physiological responses to the work environment during the COVID-19 pandemic. Anxiety, stress, negative self-perceptions, and perceived deficiencies would contribute to one’s self-efficacy to successfully complete tasks, learn, or change behaviors [11]. HCP in clinical and non-clinical roles would likely have different levels of self-efficacy based on these four processes. As would clinical HCP working directly with COVID-19 patients rather than non-COVID-19 patients. Previous work experience, experience using PPE, and many other factors would contribute to increased or decreased levels of perceived self-efficacy among HCP. Thus, context is an important factor for understanding self-efficacy as the circumstances surrounding the HCP would contribute to psychological and physiological responses that could subsequently negatively or positively impact HCP self-efficacy and subsequent performance of a task, i.e. proper use of PPE [11]. During the COVID-19 pandemic response, and in previous research, it has been demonstrated that higher levels of self-efficacy were associated with engaging in various protective health behaviors [12].
Self-reported comfort with proper use of PPE and reported PPE training received represent important components of self-efficacy. Self-reported comfort with proper use of recommended PPE demonstrates how HCP view their level of self-efficacy which may be influenced by levels of stress, anxiety, and ability within the context of a healthcare setting during a pandemic. Likewise, PPE training received represents learning through “performance accomplishments” when receiving hands-on training during which the HCP dons and doffs PPE during training or “vicarious experience” through purely observational trainings. While “verbal persuasion” learning processes would be incorporated through most training modalities.
The purpose of this study was to evaluate associations between self-reported comfort with properly using recommended PPE as a measure of self-efficacy among HCP in clinical and non-clinical roles in the healthcare setting and COVID-19 positivity. We hypothesized that HCP who report lower comfort with properly using recommended PPE, indicating lower self-efficacy, will have higher odds of COVID-19 positivity after adjusting for PPE training, occupational role, SVI, sociodemographic factors, vaccination status, average work hours, and COVID-19 variant timeframe.
Materials and Methods
Study Design, Setting, and Population
We conducted a case-control study of the association between self efficacy as measured by self-reported comfort with properly using recommended PPE and COVID-19 positivity among HCP. Our study used data from the PReventing Emerging infections through Vaccine EffectiveNess Testing (PREVENT) study, a multicenter SARS CoV-2 vaccine effectiveness case-control study of HCP in academic medical centers located in 15 metropolitan areas of 13 U.S. states [19]. Participants were enrolled between January 2021 and May 2022. HCP cases and controls were enrolled by each participating academic medical center using a nominal 1:3 case to control recruitment strategy. Study participants were recruited after having a SARS-CoV-2 reverse-transcription polymerase-chain reaction (RT- PCR) or antigen test [19]. Test information was validated with source document verification [19]. HCP working exclusively from home during the study period were not eligible to participate. Participants who had indeterminant COVID-19 test results (n=357) were excluded from this study (Figure 1). Details regarding the PREVENT study’s eligibility, inclusion and exclusion criteria, recruitment strategies, case and control definitions, data collection methods, and additional study procedures were described previously [19].
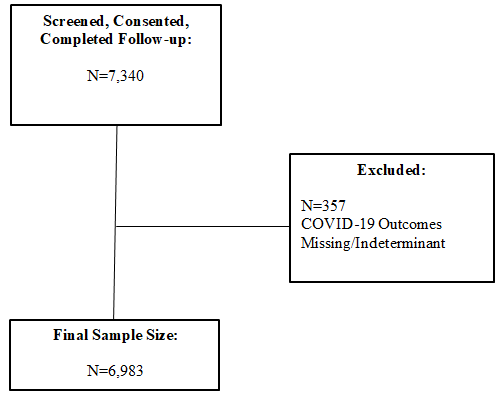
Figure 1. Aim 3 Final Sample Size Flow Chart
Primary Exposure:
A categorical variable was used for self-reported comfort level with properly using recommended PPE (very comfortable, somewhat comfortable, somewhat uncomfortable, very uncomfortable) as the primary exposure variable conceptualized as an indicator of self efficacy.
Secondary Exposures and Measures
PPE training received by employers was considered a confounding variable associated with PPE self-efficacy and COVID-19 positivity outcome. HCP self-reported PPE training received. Multiple types of PPE training were received and reported by HCP. A categorical variable was developed based on the multiple training modalities reported which included: online training only; individual training only; online and individual training; group training only; group and online training; individual and group training but no online training; all training forms; and no employer training received. ‘Online training only’ was used as the referent group to compare differences with the various combinations of in-person individual and group training modalities as it was one of the larger groups and very few HCP reported not receiving any training.
We characterized HCP self-reported job role to differentiate between clinical and non-clinical workers [19,20]. Clinical HCP included physician assistant, nursing staff, health aides/caregivers, therapists, physicians, and clinical trainees. Non-clinical roles included administrative staff, facilities, food service, housekeeping staff, research staff, and other non-clinical role. Those HCP who did not report a pre-defined role were classified as ‘other’ as they represented unique roles for which a clear clinical or non-clinical role could not be determined.
Demographic covariates of race (White, African-American/Black, Asian, other), ethnicity (Hispanic/Latino, Non-Hispanic/Non Latino), biological sex (male, female), age (18-49 years, 50 years or older), educational attainment (high school or less, some college, college graduate), and urban/rural designation (rural, urban) were included in the model. Age was transformed from a continuous variable into a dichotomous variable to identify HCP above 50 years of age based on previous studies and distribution of participant ages [21,22].
A population-weighted average Social vulnerability (SVI) percentile was calculated for each participant by ZIP Code using the CDC’s National Census Tract SVI dataset (2020) and the publicly available HUD-USPS ZIP Code Crosswalk data file (2020). Population- weighted averages of SVI themes for each ZIP code using previously described methods [23,24]. A three-level categorical variable of SVI levels of low (0.0 to <0.4), medium (0.4 to <0.6), and high (0.6 to 1.0) SVI was implemented to increase sample size in what would be considered the high SVI category [25] rather than quintiles described by Mofleh et al. [26] SVI theme levels (low, medium, high) were compared by each HCP ZIP code after the conversion process to determine level of misclassification.
Number of hours worked was included as a categorical variable (12 or fewer hours, 13 to 24, 25 to 36, and more than 36 hours). Rural-Urban Commuting Area (RUCA) codes were used to create a dichotomized ‘rural’ and ‘urban’ variable using participants’ ZIP code locators [27].
COVID-19 vaccination status and COVID-19 variant timeframe variables were included in the model. COVID-19 variant timeframes were based on CDC SARS-CoV-2 variant of concern classifications: Alpha variant/Wild type (before June 19, 2021), Delta variant (June 20, 2021-December 18, 2021), and Omicron (after December 19, 2021) [28].
Outcomes
COVID-19 positivity was the primary outcome. Cases were defined as symptomatic HCP who tested positive for COVID-19 based on a RT-PCR test or antigen test within a period from 14 days before until 14 days after onset of symptoms [19,26] Symptoms included: abdominal pain, bruised toes/feet, changes in smell or taste, chest pain or chest tightness, chills, cough, diarrhea, fatigue, fever (>100F or 37.8C), headache, loss of appetite, myalgia, nausea or vomiting, rhinorrhea, rigors, severe respiratory illness including pneumonia, shortness of breath or difficulty breathing, sinus or nasal congestion, and sore throat [19]. Symptomatic or asymptomatic HCP controls had negative RT-PCR test for SARS-CoV-2 or other laboratory- based nucleic acid amplification test [19].
Statistical Analysis
We evaluated descriptive statistics of demographics and vaccination history of study participant variables using frequencies, percentages, percent differences and corresponding 95% confidence intervals of differences by COVID-19 positivity outcome, to assess study population composition.
Generalized linear mixed models (GLMM) were used to evaluate the association of self-reported comfort with properly using recommended PPE, as a measure for HCP perceived self-efficacy, with COVID-19 positivity. Fixed effects included PPE training received, number of hours worked, HCP role, SVI, race, ethnicity, biological sex, age, educational attainment, urban/rural designation, COVID-19 vaccination, and COVID-19 variant timeframe. We included participating study site as a random effect for each model. Unadjusted and adjusted odds ratios (uOR, aOR) and 95% confidence intervals (95% CI) were determined for each variable within the model at the alpha=0.05 level of statistical significance.
Bivariate analysis using Pearson Chi-square was completed to examine distribution of self-reported comfort with properly using recommended PPE and training by HCP role, race, education, and COVID-19 outcome. All analyses were completed using SPSS Statistics for Windows, version 28.0.0.0, IBM Corp., Aronk, New York, United States.
Variable Selection
My initial variable selection was based on a literature review and identification of variables associated with COVID-19 morbidity and social vulnerability. Variables with demonstrated association with COVID-19 morbidity in the literature review were included in full model analyses [29]. Variables were then reviewed using directed acyclic graphs for causal pathways, confounders, and relationships with DAGgity v3.0, Nijmegen, The Netherlands [30]. The variance inflation factor (VIF) in the adjusted models was calculated to identify the presence of multicollinearity of the variables [31]. The Akaike information criterion (AIC) was used to examine model fit using backward step-wise modeling. Missingness of data in the dataset was reviewed to determine percent and distribution of missing data as well as need for data imputation.
Univariate analysis of the minimally sufficient variables was completed. We screened for effect modification by adding interaction terms in the adjusted model in a secondary analysis. Bivariate analysis using Pearson Chi Square to examine distribution of SVI, HCP role, race, and educational attainment by COVID-19 positivity was completed. Unadjusted (uOR) and adjusted odds ratios (aOR) and corresponding 95% confidence intervals (95% CI) were determined for each variable within the models.
Results
Characteristics of Study Sample
The study sample consisted of 6,983 HCP of the 7,340 HCP enrolled in the PREVENT study (Figure 1). The majority of HCP in this sample (3,137 cases, 3,846 controls) were white (81.2%, n=5,672), Non-Hispanic/Non-Latino (91.6%, n=6,399), females (83.2%, n=5,808), less than 50 years of age (77.1%, n=5,387), and from urban areas (96.4%, n=6,729) (Table 1). A higher percentage of HCP in the study were identified as having clinical roles (60.4%, n=4,218), and had completed college (71.4%, n=4,985). Most HCP reported that they were very comfortable with properly using recommended PPE (74.4%, n=5196) with only 3.64% (n=254) reporting being somewhat uncomfortable or very uncomfortable with properly using recommended PPE (Table 1). Multicollinearity was not present in the models based on VIF analysis [31]. Data imputation was unnecessary as missingness of data was of low occurrence across covariates (0.014% to 0.63%).
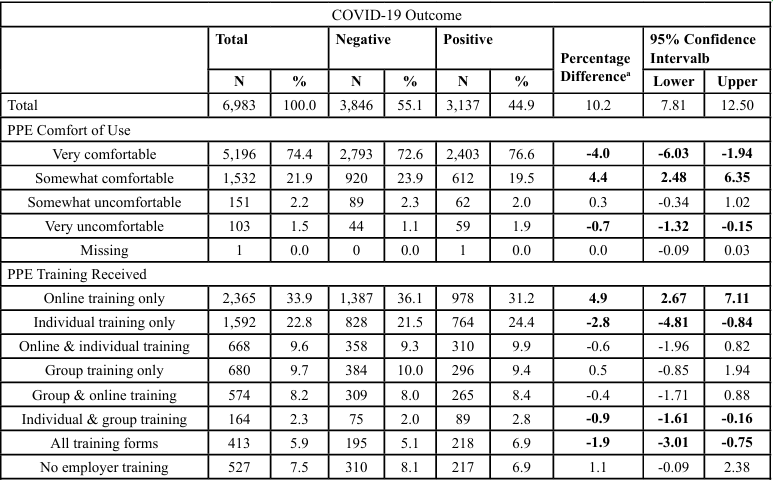
Table 1. Demographic Characteristics and SVI Distributions by COVID-19 Positivity
Self-Reported Comfort with Recommended PPE and COVID-19
HCP reporting being very uncomfortable with properly using recommended PPE had greater odds of COVID-19 positivity (aOR=1.58, 95% CI: 1.02, 2.44) compared to HCP who were very comfortable using recommended PPE (Table 2). HCP who reported being somewhat comfortable with using recommended PPE had lower odds of COVID-19 positivity (aOR=0.84, 95% CI: 0.74, 0.96).
Unadjusted models identified increased odds of COVID-19 positivity for HCP who received all training forms (uOR=1.47, 95% CI: 1.18, 1.82), in-person individual and group training (uOR=1.54, 95% CI: 1.11, 2.13), and in-person individual training only (uOR=1.24, 95% CI: 1.09, 1.42) (Table 2). However, most of these associations were not present in the adjusted models. Receiving all training forms of PPE training was significantly associated with greater odds of COVID-19 positivity (aOR=1.40, 95% CI: 1.11, 1.77), as well as in-person only training (aOR=1.16, 95% CI: 1.01, 1.34) compared to those HCP only receiving online training.
Bivariate analysis of comfort with properly using recommended PPE and training by COVID-19 outcome within HCP roles is provided in Table 3. This analysis illustrates the distribution of cases and controls within HCP roles by type of training received and self reported level of comfort with properly using recommended PPE. The secondary GLMM analysis completed to explore within group models for comfort using recommended PPE and training received by HCP roles (clinical, non-clinical, other) is presented in Table 4. We found that within groups, being very uncomfortable with using recommended PPE was associated with greater odds of COVID-19 positivity among HCP with non-clinical roles (aOR=1.81, 95% CI: 1.04, 3.16) while being somewhat comfortable with using recommended PPE was associated with lower odds of COVID-19 positivity (aOR=1.08, 95% CI: 0.86, 1.35). For HCP in clinical roles, being very uncomfortable with using recommended PPE was not associated with greater odds of COVID-19 positivity (aOR=1.47, 95% CI: 0.59, 3.66) while being somewhat comfortable was associated with lower odds of COVID-19 positivity (aOR=0.75, 95% CI: 0.63, 0.89). We also observed that receiving ‘All forms of PPE training’ (aOR=1.54, 95% CI: 1.17, 2.03) and ‘Individual and Group training’ (aOR=1.62, 95% CI: 1.07, 2.44) were both associated with greater odds of COVID-19 positivity among HCP with clinical roles (Table 4).
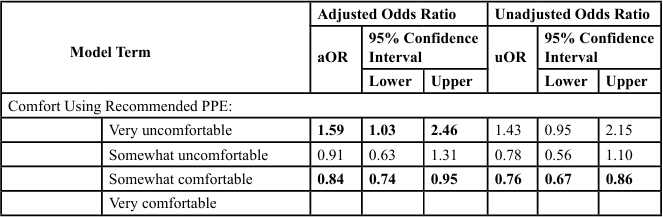
Table 2. Generalized Linear Mixed Model (GLMM) with Fixed and Random Effectsa
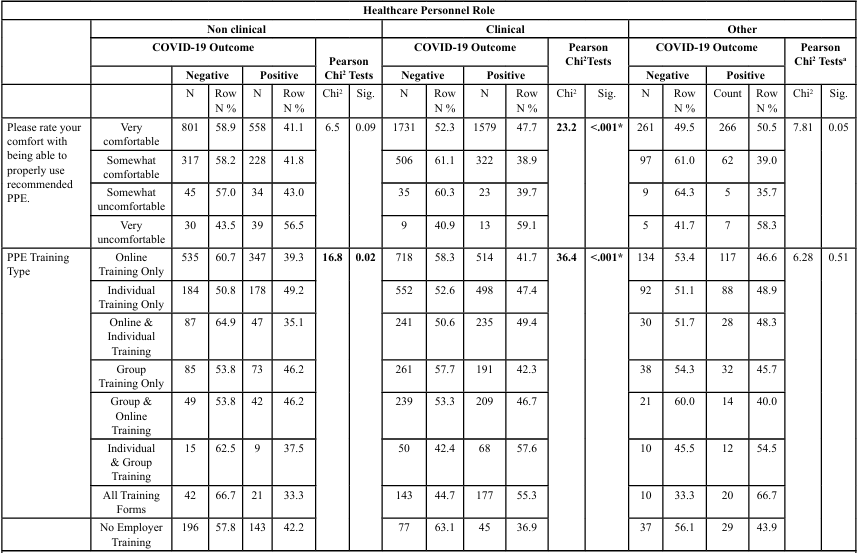
Table 3. Self-reported Comfort with PPE Use and Training Type by Healthcare Personnel (HCP) Role and COVID-19 Outcome
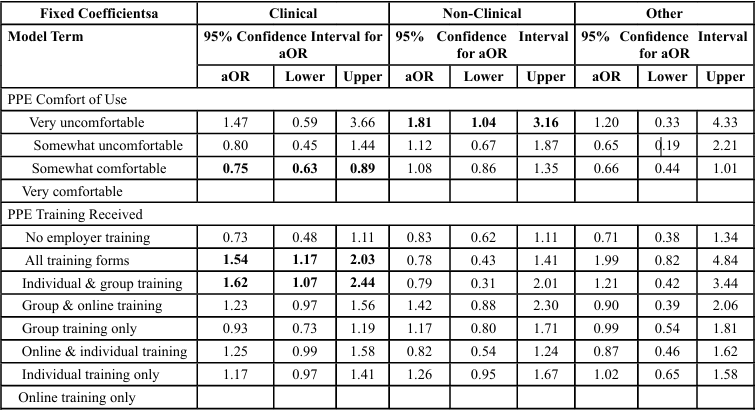
Table 4. Generalized Linear Mixed Model (GLMM) with Fixed and Random Effects by HCP Role
Discussion
We found that lower self-efficacy, as measured by self-reporting being very uncomfortable with properly using recommended PPE, was associated with greater odds of COVID-19 positivity which aligned with the study hypothesis. HCP in non-clinical roles were more likely to self-report being uncomfortable with properly using recommended PPE and have increased odds of COVID-19 positivity if uncomfortable. The observed association between receiving all forms of training and increased odds of COVID-19 positivity likely reflects greater training being directed at HCP in higher-risk clinical roles, rather than training itself being a risk factor. In the within group analysis, HCP in clinical roles had increased odds of COVID-19 positivity when they reported receiving ‘All forms of PPE training’ and ‘Individual and group training’. These findings were surprising and counterintuitive to the idea that additional training should increase self-efficacy and result in decreased COVID-19 positivity.
The results support the hypothesis that higher perceived self efficacy in the proper use of recommended PPE is associated with lower odds of COVID-19 positivity among HCP. Being very uncomfortable with using recommended PPE resulted in greater odds of COVID-19 positivity suggesting that lower self-efficacy resulted in greater odds of COVID-19 positivity. Our findings regarding PPE training and COVD-19 outcome did not align with previous research. Previous research suggests that more PPE training and more in person trainings where HCP practice using recommended PPE would result in increased self-efficacy, improved adherence with using recommended PPE, and subsequent decreased COVID-19 positivity [11]. In-person individual and group training formats did not have significant associations with COVID-19 positivity when compared to the ‘online training only’ modality. However, receiving all training forms was associated with increased odds of COVID-19 positivity. This finding should not be interpreted as more types or quantity of PPE training led to increased risk of disease transmission as HCP in clinical roles were more likely to report receiving all training forms. Instead, it is more indicative that more training was directed toward HCP in clinical roles as these HCP were more likely to have greater patient contact, increasing potential disease transmission.
Previous research demonstrated that self-efficacy was associated with successful health education and behavior change.11 Receiving PPE training and using PPE properly have both been identified as effective measures for decreasing transmission of SARS-CoV-2 in healthcare settings [1-3]. Type of training received would result in higher levels of self-efficacy and use of protective measures based on “performance accomplishments” whereby HCP learn through personal experience, watching others don or doff PPE, or receiving verbal instructions [12]. Thus, HCP in clinical or non-clinical roles receiving quality PPE training should experience increased self- efficacy in the proper use of PPE resulting in decreased transmission of SARS-CoV-2 and lower odds of COVID-19 positivity. However, one’s self-efficacy may be affected by mental and physiological responses such as anxiety, stress, and fatigue due to work and personal life circumstances experienced during the COVID-19 pandemic. Findings suggest that the COVID-19 healthcare setting with higher levels of anxiety and stress could possibly negatively impact the proper use of PPE by HCP in clinical roles resulting in subsequent exposure and disease transmission [11]. Similarly, HCP in non-clinical roles may experience increased stress and anxiety during the pandemic resulting in decreased self-efficacy of PPE use and higher odds of COVID-19 positivity.
HCP in clinical roles reported greater levels of comfort using recommended PPE, most likely due to previous use of PPE in clinical settings and training received prior to the pandemic, thus demonstrating increased levels of self-efficacy. This previous training and work experience may have resulted in higher levels of self-efficacy among HCP in clinical roles to engage in protective behaviors. This is supported by the within group analysis which demonstrated that HCP in non-clinical roles who were very uncomfortable with using recommended PPE had greater odds of COVID-19 positivity. However, having a somewhat comfortable level of properly using PPE had lowered odds of COVID-19 positivity compared to those who were very comfortable. This suggests that these HCP may have been more conscientious about their use of PPE resulting in greater protection. Our interpretation is that this observation suggests that HCP in clinical roles who routinely used PPE and received many types of PPE training may have been very comfortable using recommended PPE and very confident in their self-perception of being able to properly use recommended PPE consistently. This raises the possibility that overconfidence may have led to HCP inadvertently adopting more relaxed practices or experiencing cognitive fatigue, contributing to lapses in protocol adherence and subsequent increased odds of COVID-19 positivity. More research is needed to confirm this interpretation.
Additionally, because COVID-19 exposures were not restricted to the work setting, HCP level of self-efficacy with properly using recommended PPE may be another indicator of personal protective behaviors or may have influenced protective behaviors outside the work setting resulting in the observed associations with COVID-19 positivity. HCP level of self-efficacy as measured by self-reported level of comfort of properly using recommended PPE may be an easily attainable indicator for identification of HCP who may need additional training, monitoring, or counseling for stress and anxiety. These modifiable factors may be contributors to successful infection control and prevention practices during pandemic response efforts or other high stress clinical work settings involving infection control efforts.
Strengths and Limitations
Limitations were present in this study that likely obscured associations of self-reported comfort with using recommended PPE and COVID-19 positivity. Observations in the previous section highlight the greatest limitation of the study, such as the inability to differentiate workplace or community COVID-19 exposures. This study was unable to determine if SARS-CoV-2 transmission occurred within the work setting resulting in the observed increased odds of COVID-19 positivity or if community exposure occurred. Previous research indicated that community incidence and exposures were more associated with clinical HCP SARS-CoV-2 seropositivity rather than workplace exposure [32]. With this in mind, we assumed that HCP who received PPE training would also practice some level of protective actions when in public based on HCP level of perceived self-efficacy of properly using recommended PPE. This would likely decrease exposure in the community and result in lowered odds of COVID-19 positivity for HCP who view themselves capable of engaging in protective behaviors. The question then becomes, did level of self-efficacy of using recommended PPE contribute to behaviors outside of the workplace making it more or less likely that these HCP engaged in protective behaviors in the community? Unfortunately, without additional information this cannot definitively be stated that increased self-efficacy led to adherence to PPE recommendations or changed behaviors in the community resulting in lower odds of COVID-19 positivity. However, these results do indicate that an association exists between increased self-efficacy of properly using recommended PPE and lower odds of COVID-19 positivity regardless of being able to determine source of exposure within, or outside of, the healthcare work setting.
Another limitation is that additional questions of comfort with properly using recommended PPE and training were not specifically developed for the current study. This prevented the inclusion of questions that could have clarified differences between HCP levels of self-efficacy of properly using recommended PPE and COVID-19 positivity. For instance, feelings of anxiety may have been a factor in HCP rating of levels of comfort with using recommended PPE properly which could be linked to feelings of self-efficacy. Additionally, the wording of the question about comfort with recommended PPE use may have resulted in participants focusing on physical comfort rather than comfort with properly using recommended PPE. Information concerning physical comfort, adherence to proper use of PPE, previous PPE or infection control training received before the pandemic, work experience, knowledge of other infection control procedures, extent of patient contact, exposure to aerosol generating procedures, or other circumstances that impact SARS-CoV-2 transmission was not collected. Similarly, the subjective nature of the self-reported level of comfort with proper use of recommended PPE without a standardized or clear definition of “comfort.” This may have resulted in misclassification as some HCP may have over- or under-estimated their level of comfort with properly using recommended PPE.
Another limitation of this study involves possible issues with temporality and self-reporting bias by which cases may have increased doubts regarding using PPE properly, i.e.self-efficacy and reported level of comfort differently because of their illness. Similarly, controls may have overestimated their self-efficacy due to their lack of illness.
This study has important strengths that should be noted. The first strength is that this study highlights an important relationship between self-efficacy, training, and disease outcome. Our study shows that the amount of training received may not be the most effective metric reflective of PPE efficacy. Instead, it may be necessary to focus on measures of HCP self-efficacy to consider effectiveness in the prevention of disease transmission rather than process evaluations of the number and type of PPE trainings received.
The second strength of this study is that this is one of the first studies to examine comfort with properly using recommended PPE as a measure of self-efficacy when considering infection, such as COVID-19 positivity, as an outcome. This represents an effort toward clarifying relationships between self-efficacy in proper PPE use and infectious disease outcomes which have been lacking. Findings represent an important contribution to previous research that has primarily focused on physical discomfort, self-efficacy, and demographic characteristics as predictors of PPE use [4-6]. Previous research has relied heavily on descriptive or qualitative data of HCP attitudes, PPE use, and adherence to guidelines focused on efficacy of training modalities and monitoring proper PPE use without considering infectious disease outcomes [3,9,10]. These findings demonstrate the need for future studies to focus on self-efficacy rather than process measures such as number and types of PPE training. Our study also lends initial support to measuring self-efficacy as a part of infection control policies in addition to PPE training received.
Conclusions
These findings are important for future pandemic response efforts and infection control strategies. Asking HCP about their comfort with properly using recommended PPE could be a simple strategy to tentatively identify HCP level of self-efficacy. This may be an easily attainable indicator for identifying HCP who may need additional training, monitoring, or counseling for stress and anxiety to increase self-efficacy and ultimately reduce disease transmission. HCP with low self-efficacy with comfort using recommended PPE may be at increased risk of disease transmission in the work setting or community due to inconsistent PPE use or behaviors.
The current study raised many questions due to being based on data collected for other purposes as part of the PREVENT study. Additional research is warranted regarding HCP self-efficacy of PPE use, efficacy of PPE training modalities, and self-efficacy’s influence on other protective behaviors in the work setting and community. Future research is needed to focus on protective behaviors beyond PPE use in the work setting that may be affected by PPE training and self-efficacy. This includes adherence to social distancing and other protective. PPE training and modality should also be studied more vigorously from the standpoint of preventing disease transmission rather than focusing on process measures such as number of trainings completed, adherence to policies, proper PPE use, or other intermediary factors. These findings suggest that assessments of HCP self-efficacy, such as simple self-reported comfort-rating scales, could be useful screening tools for targeted interventions, including personalized retraining or psychosocial support during public health emergencies.
Competing Interest:
Authors do not have conflicts of interest nor have they received financial support.
List of Abbreviations:
PPE
SDoH
SVIPREVENT
HCPCOVID-19
CDCHUD
RT-PCRZIP
GLMMReferences
Soleman, S. R., Lyu, Z., & Okada, T, et al. (2023). Efficacy of personal protective equipment to prevent environmental infection of COVID-19 among healthcare workers: a systematic review. Environ Health Prev Med. 28(1). View
Soares, S. S. S., Souza, N. V. D de O, Silva, K. G., César, M. P., Souto, J da S. S., Leite JCR de AP. (2020). COVID-19 pandemic and rational use of personal protective equipment. Revista Enfermagem. 28. View
Shehab, M., Shuaibi, S., Qadhi, I., & Alfadhli, A. (2021). Effectiveness of inspectors’ team in increasing compliance with personal protective equipment use and reducing COVID19 infection spread among healthcare workers. Infection Prevention in Practice. 3(2):100137. View
Çiriş Yildiz, C., Ulaşli Kaban, H., Tanriverdi, F. Ş. (2022). COVID-19 pandemic and personal protective equipment: Evaluation of equipment comfort and user attitude. Arch Environ Occup Health. 77(1):1-8. View
Janson, D. J., Clift, B. C., & Dhokia, V. (2022). PPE fit of healthcare workers during the COVID-19 pandemic. Appl Ergon. 99:103610. View
Fan, J., Jiang, Y., & Hu, K., et al. (2020). Barriers to using personal protective equipment by healthcare staff during the COVID-19 outbreak in China. Medicine (United States). 99(48):e23310. View
McCarthy, R., Gino, B., d’Entremont, P., Barari, A., & Renouf, T. S. (2020). The Importance of Personal Protective Equipment Design and Donning and Doffing Technique in Mitigating Infectious Disease Spread: A Technical Report. Cureus. Published online 2020:e12084. View
Saran, S., Gurjar, M., & Baronia, A. K., et al. (2020). Personal protective equipment during COVID-19 pandemic: a narrative review on technical aspects. Expert Rev Med Devices. 17(12):1265-1276. View
Cash, R. E., Rivard, M. K., Camargo, C. A., Powell, J. R., & Panchal, A. R. (2021). Emergency Medical Services Personnel Awareness and Training about Personal Protective Equipment during the COVID-19 Pandemic. Prehospital Emergency Care. 25(6):777-784. View
Liow, M. H. L., Lee, L. C., Tan, N. C. K., et al. (2022). Personal protective equipment training for non-healthcare workers in the Covid-19 pandemic: Effectiveness of an evidence-based skills training framework. Infect Dis Health. 27(1):38-48.
Strecher, V. J., McEvoy DeVellis, B., Becker, M. H., & Rosenstock, I. M. (1986). The Role of Self-Efficacy in Achieving Health Behavior Change. Health Education & Behavior. 13(1):73-92. View
Zhang, N., Yang, H., Hong, D., Huang, X., Wang, L. (2022). Risk Perception, Self-efficacy, Lay Theories of Health, and Engagement in Health-Protective Behaviors Among Hospital Pharmacists During the COVID-19 Pandemic. Int J Behav Med. 29(2):247-252. View
Rahman, A. A., Saliluddin, S. M., Rusli, M. F., Singh, P. J., Rosli, N. M., & Shah, S. A. (2020). Healthcare workers issues and COVID-19 pandemic: A review. Gazi Medical Journal. 31(2). View
Shreffler, J., Petrey, J., & Huecker, M. (2020). The impact of COVID-19 on healthcare worker wellness: A scoping review. Western Journal of Emergency Medicine. 21(5):1059-1066. View
Jacob, J. T., Baker, J. M., & Fridkin, S. K., et al. (2021). Risk Factors Associated with SARS-CoV-2 Seropositivity among US Health Care Personnel. JAMA Netw Open. 4(3):e211283. View
Al Maskari Z, Al Blushi A, Khamis F, et al. (2021). Characteristics of healthcare workers infected with COVID-19: A cross-sectional observational study. International Journal of Infectious Diseases. 102:32-36. View
Rho, H. J., Brown, H., & Fremstad, S. (2020). A Basic Demographic Profile of Workers in Frontline Industries. View
National Center for Health Workforce Analysis. (2017). Sex, Race, and Ethnic Diversity of U.S. Health Occupations (2011-2015). View
Mohr NTD. (2022). PReventing Emerging Infections through Vaccine EffectiveNess Testing—COVID: Manual of Procedures. Accessed September 27, 2022. View
Plumb, I. D., Mohr, N. M., & Hagen, M., et al. (2023). Effectiveness of a Messenger RNA Vaccine Booster Dose Against Coronavirus Disease 2019 among US Healthcare Personnel, October 2021-July 2022. Open Forum Infect Dis. 10(10):ofad457. View
Pilishvili, T., Fleming-Dutra, K. E., & Farrar, J. L., et al. (2021). Interim Estimates of Vaccine Effectiveness of Pfizer- BioNTech and Moderna COVID-19 Vaccines Among Health Care Personnel 33 U.S. Sites, January–March 2021. MMWR Recommendations and Reports. 70(20):753-758. View
Pilishvili, T., Gierke, R., Fleming-Dutra, K. E., et al. (2021). Effectiveness of mRNA Covid-19 Vaccine among U.S. Health Care Personnel. New England Journal of Medicine. 385(25):e90. View
Tipirneni, R., Karmakar, M., O’Malley, M., Prescott, H. C., & Chopra, V. (2022). Contribution of Individual- and Neighborhood-Level Social, Demographic, and Health Factors to COVID-19 Hospitalization Outcomes. Ann Intern Med. 175(4):505-512. View
Morgan, M. E., Horst, M. A., & Vernon, T. M., et al. (2020). An analysis of pediatric social vulnerability in the Pennsylvania trauma system. J Pediatr Surg. 55(12):2746-2751.
Faber, J., Fonseca, L. M. (2014). How sample size influences research outcomes. Dental Press J Orthod. 19(4):27-29. View
Mofleh, D., Almohamad, M., & Osaghae, I., et al. (2022). Spatial Patterns of COVID-19 Vaccination Coverage by Social Vulnerability Index and Designated COVID-19 Vaccine Sites in Texas. Vaccines (Basel). 10(4):574. View
Ingram, D. D., & Franco, S. J. (2014). 2013 NCHS urban-rural classification scheme for counties. Vital Health Stat, 2. (166). View
Centers for Disease and Prevention. SARS-CoV-2 Variant Classifications and Definitions. SARS-CoV-2 Variant Classifications and Definitions. July 20, 2023. Accessed July 23, 2023. View
Hosmer, D. W., & Lemeshow, S. (2000). Applied Logistic Regression. 2nd Edition. View
Textor, J., van der Zander, B., Gilthorpe, M. S., Liśkiewicz, M., & Ellison, G. T. (2016). Robust causal inference using directed acyclic graphs: The R package “dagitty.” Int J Epidemiol. 45(6):1887-1894. View
Bhandar, A. (2023). Multicollinearity | Causes, Effects and Detection Using VIF (Updated 2023). Analitycs Vidhya.
Jacob, J. T., Baker, J. M., Fridkin, S. K., et al. (2021). Risk Factors Associated with SARS-CoV-2 Seropositivity among US Health Care Personnel. JAMA Netw Open. 4(3). View