
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy Volume 4 (2026), Article ID: JSWWP-179
https://doi.org/10.33790/jswwp1100179Review Article
Integrating Neurobiology, Self Psychology and Social Work Concepts in Understanding the 12 Steps of Alcoholics Anonymous
Irek Banaczyk, MSSW, LCDC, LCSW-S and Arlene Montgomery*, MSSW, PhD, LCSW-S
Assistant Professor of Instruction, School for Social Work, The University of Texas at Austin, 306 Inner Campus Drive, Ste. 2.200, STOP D3500, Austin, TX 78712, United States.
Corresponding Author Details: Arlene Montgomery, MSSW, PhD, LCSW-S, Assistant Professor of Instruction, School for Social Work, The University of Texas at Austin, 306 Inner Campus Drive, Ste. 2.200, STOP D3500, Austin, TX 78712, United States.
Received date: 11th November, 2025
Accepted date: 05th January, 2026
Published date: 08th January, 2026
Citation: Banaczyk, I., and Montgomery, A., (2026). Integrating Neurobiology, Self Psychology and Social Work Concepts in Understanding the 12 Steps of Alcoholics Anonymous. J Soci Work Welf Policy, 4(1): 179.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
This report describes interactive workshops at two conferences in 2025 for professional and student Social Workers and professionals from other disciplines. The authors modeled linking selected Social Work concepts, Self Psychology concepts, and Interpersonal Neurobiology concepts to each of the 12 Steps of Alcoholics Anonymous (AA) followed by the participants practicing doing the same and then sharing with the group. Each of the 12 Steps of AA was examined for the belief that the step addressed and for the nervous system function(s), the Social Work and Self Psychology concept(s) and treatment implications, including certain relevant cultural and ethical issues.
For example, Step 1 is ”Do It Yourself” which reflects the following: denial [1] that life has become unmanageable [2]; employing self regulation strategies with substances instead of people [3] as a way to manage separation distress, loss, and panic [4] leading to extreme self dependence to the exclusion of developmentally appropriate reliance on others [5]. Attunement from others may have become anxiety/ fear-producing (i.e., examine cultural belief of toxic individualism) rather than tolerating small doses of tending and empathy designed to correct emotional experiences of depending on imperfect others to maintain sobriety [6] and ethical value of the importance of human relationships [7].
Another example is Step 2: “No One is Coming” that may be the originally-adaptive belief of the danger from involvement with others [8] that is supported by the amygdala’s danger-detection of powerful others with bad intentions [9]. Over-compensation via grandiosity, i.e., extreme self-dependence [5], is reflected in Maslow’s [10] hope vs. despair stage of development and Panksepp’s seeking others as one of the in-born emotional circuits [4]. Extreme ambivalence toward depending on more-powerful, potentially hurtful others may have resulted in the belief that the road to sanity is not to count on others under any circumstance, but rather depend on a substance, over which one has the fantasy of complete control. Dignity and Worth of a Person [7] are the focus of the repair of the experience of isolation as is the examination of cultural pressure to use substance for ease of relating to others [3].
Briefly reviewed for workshop attendees were concepts that informed the hand-outs and the chart material used to speculate on the associations among the above concepts that are linked in some way to each of the 12 Steps (see figures throughout this report). The clinical goal is to contribute to case conceptualization and treatment planning for appropriate interventions, thereby providing a focus on the underlying dynamics holding in place the belief that each step is addressing. This workshop format is easily replicated, as all handouts (including relevant literature) and the charts are contained in this report. The format is described in detail. Some reflections are offered for incorporating the factors that are influential, but invisible in their contribution to both being an obstacle to change and part of the effort to address achieving and maintaining sobriety.
Keywords: 12 Steps of Alcoholic Anonymous (AA); Self Psychology concepts; Social Work concepts; Neurobiology structure and function; empathy
Introduction
It is our experience that addictions of all sorts remain stigmatized generally, and in particular, in our own clinical treatment culture and are often avoided by many psychodynamic clinicians, among others. There is a gulf and, frankly, some hostility between those who do and do not treat addictions. In our experience, each “side” does not trust the other to address salient treatment issues. Our goal was to draw from multiple streams of conceptualizations, including honoring several of the original thinkers from seemingly opposing traditions. We are reporting on our presenting a platform for speculating with colleagues on the linkages among the mind (beliefs), the body (neurobiology), and relevant theoretical concepts with selected treatment implications. We emphasize “speculate” as this is an exercise in pulling together several lines of thought dating back over the last 100 years that have diverged and, on their face, may not seem all that related. Particularly speculative are associating the findings in the literature on the brain and peripheral nervous system structures and functions published over the last 30 years in order to illuminate mind-brain-body interconnections that may influence addictive behaviors. Treatment planning and implementation could be enhanced.
Over a number of years, as clinical colleagues we have often discussed the hidden family and cultural dynamics affecting and affected by substance use issues. As we considered the 12 Step approach, we tried to imagine the belief that each step was designed to address in the healing process. We made an effort to integrate certain concepts about how the nervous system works to support those beliefs, how developmental insults weakened a person’s sense of self, and ways social work interventions address treatment by challenging the currently dysfunctional beliefs, and most importantly, begin to replace the belief with more socially functional beliefs about self and the world with the hope that more adaptive behaviors would result. Certain related ethical and cultural aspects were considered.
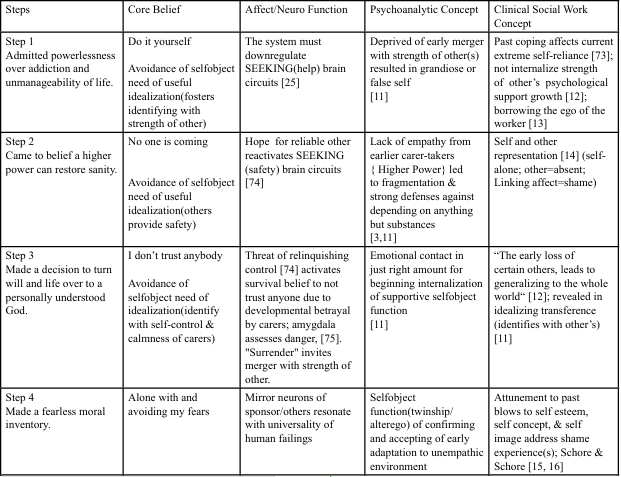
Figure 1: Example of an Integrated Chart for Beliefs, 12 Steps of Alcoholics Anonymous Neurobiology, Self Psychology and Social Work Concepts
A brief discussion of concepts from the literature that informed our workshop discussion follows. A comprehensive review of these sources is beyond the scope and purpose of this report, but familiar citations are referenced for further elucidation. Figure 1 above illustrates the final result of the authors’ effort to create a schematic that briefly links the phenomena under discussion. After Figure 2, (agenda) this report provides an abbreviated discussion of theoretical constructs from Self Psychology and Interpersonal Neurobiology as well as theoretical, spiritual, and cultural influences resulting in the treatment philosophy of Alcoholics Anonymous that we utilized for our power point and hand-outs. This is included in our report because, although Social Work concepts are well understood by our intended audience, currently the same is not as true for Self Psychology and Interpersonal Neurobiology fundamentals. The presentation began with a slide deck with selected constructs from Self Psychology as they required some description and discussion of the compatibility to well-known Social Work concepts.
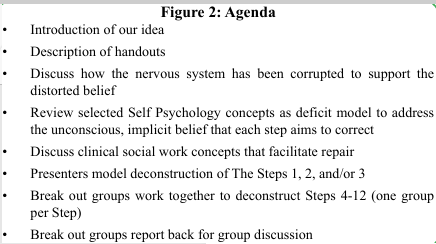
Figure 2: Agenda
Self Psychology Basics
Described below is a brief rendering of Heinz Kohut’s [5,11] theory of the stages of the development of normal narcissism (self-love) and the clinical application thereof. Some details are provided as the field of Social Work has not integrated whole-heatedly these concepts to date. Kohut’s developmental progression of self-love is often not appreciated for the clinical meaning he ascribed, that is, the normative love of the self develops through being looked at lovingly (mirror stage); being able to look lovingly at important others (idealizing stage); and being looked at lovingly as similar or the same-as (alter- ego/twinship stage). In common parlance, narcissism has come to represent grandiosity, elevating of the self over others, selfishness. arrogance, etc. However, Kohut’s conception was quite benign and described an emotionally/psychologically stabilizing coherent inner experience that confers resilience to normative distress. Kohut never defined the self, but rather the by-product of healthy narcissism (self- love) producing functionality within normal limits for one’s culture. Each stage requires empathy from caregivers as they focus on the “need” developmentally that is emotionally regulating. If outside normal limits, then maladaptive behaviors may stem from a delicate self-esteem that is easily injured and/or over-reactivity to perceived slight and defeats (“fragmentation” to use Kohut’s term). Access to normal childhood narcissism is barred [23]. The child’s nervous system is own their own to create a modicum of self-love that was denied to them by neglecting to process through the stages via care- giver empathic tending enough of the time.
Heinz Kohut thought that disappointments (or worse) in the caregiving experience could lead to maladaptive self-soothing regulatory functions; minor disappointments could lead to within normal-limits self-soothing functions. Kohut coined the term “selfobject” to convey the developing mind gradually “downloading” the brain’s experience of early merger with good enough (m)othering that could eventually become good enough self-regulation. His idea was that the original functions of the selfobject would be taken over by a “cohesive” self that would be properly self-regulating. A. Schore [24] later added that in times of stress, the cohesive self would turn to help from others that could temporarily re-regulate and return to baseline functioning. In contrast, the easily “fragmented” self seeks self-regulation from pathological sources (e.g., addictions, unreliable others, etc.).
The easily fragmented self had not properly experienced Kohut’s proposed stages of the development of normal narcissism (or self-love) necessary for resilience in everyday life. The uncompleted stages leave the mind and nervous system “hungry” [23] for that development stage to be re-started over and again in current life. The form that each arrested stage takes has some identifiable behaviors that indicate the unconscious effort for correcting the lack of certain experiences that could lead to the normal narcissism of self-love.
Stage 1 is the mirroring stage (0-2), a time when the infant/child experiences attunement to their needs to be special and unique (empathically admired by care-giver(s))
Stage 2 is the idealizing stage(2-5-ish), a time when the child connects with the calm & other strong qualities of others in a merger- like fashion(caregiver(s)empathically allow others to be admired)
Stage 3 is the alter-ego/twinship stage (elementary school), a time of needing to belong and be the same-as (peers empathically encourage learning to be part of a group in welcoming manner).
Following are some behavioral and emotional clues that the poorly developed stage is stirring the interpersonal environment toward correcting the past in the present relationship(s) [26]:
Mirroring stage: demanding admiration and confirmation of uniqueness
Idealizing stage: over-valuation of others to whom they imagine or have connections, e.g., best family, best pets, best sports team, finest car, and (watch out) best therapist which is calming and a source of borrowed strength.
Atler-ego/twinship: assuming sameness (e.g., people like us are….).
These thwarted needs may define a certain quality of transference/ counter-transference experience in therapy as the client’s nervous system signals the unmet needs in the clinical work; not a conscious process. It is common practice in Social Work to empathically identify unmet needs and craft the appropriate clinical response with empathy. We do not necessarily identify those responses as affected by Kohut’s concepts, but they are operative much of the time anyway. We are articulating them for the purpose of the workshop deconstruction of aspects of the 12 Step interventions. In our work, we may see the following behaviors, perspective, emotions:
Mirroring transference: grandiosity, entitlement, exhibition of accomplishments, unstable self-esteem, unwilling to be empathic, fear of revealing even minor flaws, strong need to control others view of them (Need=recognition & praise to shore up depleted self concept/esteem)
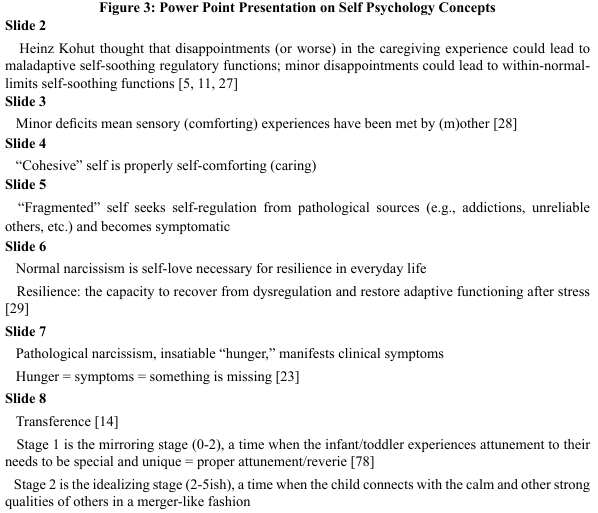
Figure 3: Power Point Presentation on Self Psychology Concepts
Idealizing transference: looking for others to admire for their prestige, accomplishments, standing in the community, moral stature, experts, glamorous, intelligence(especially the therapist) (Need=reflected glory to avoid feeling defective)
Alter-ego/twinship transference: vulnerable to adopting belief systems to ensure inclusion, similar lifestyle, clothes, opinions, appearance (Need=sameness to avoid rejection).
All the above, when not within normal limits, are compensating for unmet needs from early development. The goal is to re-start development in the stage(s) it left off in present-day interpersonal encounters and heal the narcissistic wound(s). However, many of the above compensating efforts simply re-create the original injury and others may withdraw, reject, and otherwise shun them, confirming the early trauma.
Note: a small group of those with damage to the ability to love themselves (normal narcissism) will fall into category of “contact shunning” and, out of fears, will isolate because their hunger for unmet needs is so intense as to be unbearable for the undeveloped nervous system (Need: to not feel pain of yearning). Counter- transference issues abound, but primarily the effort for the therapist to not recreate the original trauma of under-mirroring, not allowing ourselves to be idealized, or to tolerate being thought to be the “same as”. Addictions seem an obvious way to meet one’s own needs for depending on a reliable “other”.
Interpersonal Neurobiology
Currently, the discipline of Social Work is in the process of embracing neurobiological findings with contributors to the intersection of the two fields exemplified by Applegate and Shapiro’s 2005 book, Neurobiology for Clinical Social Work and Farmer’s 2009 book,
Figure 4: Selected Neurobiological Concepts
Neuroscience and Social Work Practice, to name some early works. It was only in 1990 that the Congress of the United States denoted that year as the beginning of the “Decade of the Brain” though John Bowlby’s work on biological underpinnings of loss, grief, and resulting attachment and emotional regulation issues from the 1940s has been integrated into social work perspectives since its introduction. Bowlby described the stages of grief and mourning and the psycho-social consequence of loss; importantly, a social worker, John Robinson, was involved in the early loss/grief research with Bowlby that eventuated into the attachment work of today [42]. Contributors other than social workers are too numerous to name, so suffice it to say that the authors chose to list commonly known and/ or briefly described brain functions for suggestions on the workshop participant’s hand-out that are self-evident as to their relevance for the 12 Step exercise. Following the model that John Bowlby provided for clinical thinking, the authors deconstructed each of the steps for what belief the step addressed. We could not emphasize that enough, each step addresses a once-adaptive, but currently maladaptive, belief that guides perspective on the world in general and toward certain people in particular. This belief is enacted in behaviors though it is unconscious. The belief provides support for choosing substances/ addictive behaviors over people.
Bowlby addressed the function of the insecure attachment behaviors as a regulation schema (avoid, anxiously signal, disorganized ways to interact) that has become dysregulating, but automatic. We have focused on the organizing belief that each of the 12 steps address, though invisible and largely out of conscious awareness. The “belief” or perspective motivates behaviors and is the focus of clinical interventions, if we can recognize them for their early and unarticulated original meanings.
Central Concepts from Recovery Literature
A significant contribution to the recovery movement emerged with the founding of Alcoholics Anonymous (AA) and the publication of its foundational text in 1939. As the first and longest-standing Twelve Step program, AA has inspired the development of more than sixty adjunctive and alternative mutual aid societies addressing a wide range of addictions and associated conditions, including substance dependence, gambling, sex and love addictions, codependency, and the experiences of family members affected by addiction, etc. [43].
AA’s Twelve Step program has achieved a truly global reach. Its core text has been translated into over one hundred languages, and meetings are accessible worldwide in person, by mail, online, and even aboard cruise ships [44]. Today, AA maintains an active presence in approximately 180 countries, encompassing more than 123,000 groups across the globe [44].
Given its accessibility and enduring relevance, AA represents a vital contribution to holistic healing and the restoration of individual well-being, aligning with the ethical principles outlined in the NASW Code of Ethics [7]. Accordingly, this presentation and report seek to articulate and illuminate the curative elements of the Twelve Steps (See Figure 5) as they relate to the treatment of addiction and the reparation of maladaptive core beliefs. These elements are examined through the lenses of Self Psychology, Neurobiology, and clinical Social Work concepts. From a Social Work perspective, the discussion explores implications for culturally responsive referrals, case conceptualization, and the development of integrated biopsychosocial–cultural–spiritual interventions.
Debate surrounding the disease model of addiction remains vigorous, with scholars offering both supporting and critical perspectives [26,45-51]. One of the earliest articulations of the disease perspective is attributed to Benjamin Rush [52], who proposed that “habitual drunkenness should be considered a disease... and treated as such.” This conceptualization profoundly influenced later thought, including that of Dr. William D. Silkworth, an early medical contributor to the AA movement. In his letter included in all editions of the “Big Book” of Alcoholics Anonymous, Silkworth described alcoholism as an illness involving both body and mind [53].
Although a detailed analysis of the competing arguments surrounding the disease model of addiction lies beyond the scope of this paper, addiction and recovery are conceptualized here as processes of deficit and repair occurring across the biological, psychological, sociocultural, and spiritual dimensions of the self. While these domains are often delineated separately, they are inherently interdependent and nonlinear a perspective grounded in systems theory and supported by developmental scholarship [54-58].
Within this framework, the emergence and maturation of the self occur within a dynamic, nonlinear system composed of multiple interacting levels of human experience across the lifespan. Optimal regulation within this system integrates several pathways: self regulation, somatosensory regulation, relational regulation, and pharmacological regulation [59]. This multidimensional integration underscores the necessity of approaching addiction and recovery not as isolated phenomena but as complex, systemic processes involving reciprocal influences among body, mind, relationships, spirit, and environment.
Alcoholics Anonymous owes its very existence, in part, to the influence of Dr. Carl Jung’s guidance to one of its early influencers, Roland H. After approximately a year of psychoanalytic treatment under Jung’s care, Roland relapsed into drinking. Upon returning to Switzerland for further help, Jung informed him that his condition lay beyond the reach of medical or psychotherapeutic intervention, explaining that recovery required a profound spiritual awakening.
Following this counsel, Roland joined the Oxford Group, a Christian movement emphasizing personal transformation through spiritual principles. Through this engagement, he achieved sobriety and subsequently inspired Bill W., cofounder of Alcoholics Anonymous, to pursue his own recovery events that directly contributed to the formation of AA [53].
This historical connection highlights the enduring importance of the spiritual dimension in recovery an aspect frequently minimized or overlooked within contemporary clinical discourse. Jung observed that Roland’s “craving for alcohol was the equivalent, on a low level, of the spiritual thirst of our being for wholeness expressed in medieval language as the union with God” [60]. Within this context, wholeness may be understood as an integrative process that restores the individual to psychological, physical, emotional, and social well- being. The present report, and the workshops from which it draws, are grounded in this integrative perspective, seeking to illuminate pathways toward a multidimensional recovery.
Description of how presenters used the handout materials in the workshops
The first time we presented the 12 Steps Meets Neurobiology was for the 2025 Texas National Association of Social Workers annual meeting that was virtual this year (we had over 100 participants and we were on the same computer together). We had prepared to use the break-out function on zoom so our participants would meet in small groups to work together to identify the core belief that a certain step was addressing and provided hand-outs on selected Interpersonal Neurobiology, Self Psychology and Social Work concepts e.g., early childhood missing functions, corrective therapeutic interventions, ethical issues, brain functions, to name a few. There was no correct answer. We were sharing our own clinical experiences of trying to connect similar, but siloed off, theoretical and treatment concepts to address the origin story of the core belief and ways to provide an alternative belief leading to maintaining a recovery trajectory. We intended to provide our effort to the participants (see Figure 1) on the first 3 steps (see Figure 5 the 12 Steps of AA) as a model and talk to one another and the group about our process. Then we intended to break out into small groups to practice doing the same and reporting back to the group, step by step, time permitting.
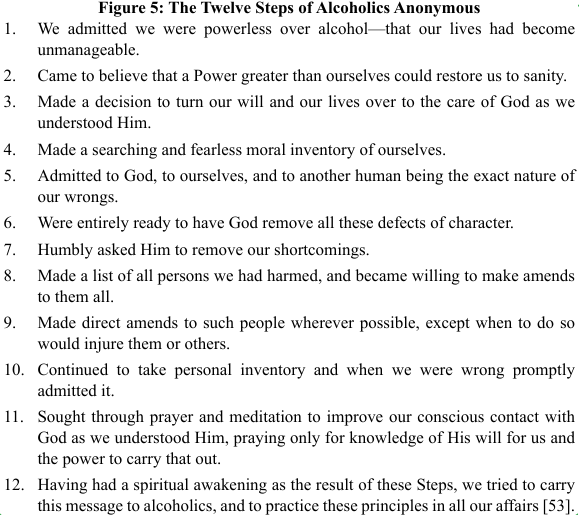
Figure 5: The Twelve Steps of Alcoholics Anonymous
However, just before we were to present, we learned that there would be no breakout groups, and a moderator was to manage the chat for participant comments (and he also had to manage helping some of the group find the handouts during the workshop). Hurriedly, we reorganized our plan and, after some brief introductory information sharing our roadmap for the seminar, we presented brief slide deck on Self Psychology concepts (See Figure 3). Not knowing our audience, we assumed that many may not have been acquainted with the work of Kohut directly, so the PPX provided a brief review, emphasizing the compatibility with Social Work and Social Welfare practice. We saw no reason to review Social Work concepts (See Figure 6) and the Interpersonal Neurobiology concepts (See Figure 4) were obvious.
We then discussed the first step and our thoughts about connecting these varied concepts, then checked in with the group, who right away wanted to skip to a step that the presenters had not shared, so we skipped to Step 6 for their input. This was done through the chat with the moderator helping and some back-and-forth occurred, as connections from other theories (i.e., Maslow’s hierarchy of needs), the possible belief the step was meant to address, Social Work interventions, a smattering of speculations about the neurobiological function that was either missing or operating to keep the belief in place, and the missing functions (deficit model of Self Psychology). The rest of the presentation was a discussion of one step and the possible influences on the early-in-development adaptation to the environment, what forces kept the belief in place, and both the obstacles and a way forward in recovery for any addiction. The group asked for our effort to fill out the chart (See Figure 1) for which the conference provided our contact information.
The second presentation of The 12 Steps Meets Neurobiology occurred the following week at the American Association of Psychoanalytic Social Work biennial conference. We met in person with about 15 participants (43 were signed up but it was Sunday morning, the last workshop of the conference and people were trying to catch their flights during the government shutdown of service in the Fall of 2025).
We again presented the PPX of basic tenets of Self Psychology that were particularly compatible with illuminating the missing care-taking experiences around which an originally adaptive, later maladaptive, belief would govern turning from people for regulatory bonding experiences and instead, to use more “reliable” substances or driven behaviors to regulate their nervous systems. The discussion was rich and lively, as we connected the deficit model of Heinz Kohut’s Self Psychology to the idea that each step of AA was designed to offer an alternative to regulation that involved other people, though not perfectly available. Our reasoning for devoting time to the Kohutian concepts of the development of the capacity to love the self (normal narcissism) was our conceptualizing self-development as having been derailed early in development and the AA model would help supply the missing function, thereby, provide repetitive emotionally corrective experiences. The handouts mentioned in above discussion of the first workshop were provided but are fairly self-explanatory (list of concepts from Neurobiology, Social Work and the Steps of AA).
As in the first workshop, the presenters interacted with one another to review our process of examining Step 1 for the missing function it provided that linked back to the unconscious belief for surviving (e.g., “Do It Myself” meaning that if I do not take care of myself in various ways, no one will). We described how we speculated on the neurobiological process that may have shut down the “seeking" emotion [4] so that the nervous system of the developing child’s brain/mind was deprived of the chance to connect with carers and share their emotional strength. The Social Work early concept from Ego Psychology [61] “borrowing the ego of the worker” [13] is especially apt.
In the interest of time, we did not review the other 2 Steps that we prepared and for which they had our chart but went directly to small groups choosing a step to consider with the handouts provided. The groups reported back to the workshop their use of the material to consider the linkages among them. Some had used the same step but had somewhat different ideas of the belief; all but one group used each of the handouts to settle on what may be the underlying neurobiological process; which aspect of the deficit model may be operative; and one or more concepts from Social Work practice may be relevant. Comments from the group about the usefulness of this exercise included an appreciation of the prompts from the handouts so notes would not have to be taken, having some concepts to work from (though many added their own theoretical concepts), and the empathy for the developmental insults that eventuated in a set of beliefs that adapted to a milieu that was less-than-optimal to forge regulating connections to others. Even though we were at the end of a three-day workshop and people were tired, there was an enthusiasm and intensity that permeated the 3 hour seminar, with open and vulnerable commentary using examples of clients, some personal thoughts, plus suggesting specific treatment considerations based on a variety of theoretical considerations.

Figure 6: Social Work Concepts
Concluding Reflections and Implications for Practice
Feedback from participants following the first presentation highlighted their appreciation for the clarity of the PPX framework as it related to Self Psychology. We were initially concerned about the risk of oversimplifying a complex theoretical model; however, the PPX concepts were intentionally selected to align with familiar social work principles and clinical practice. Participants’ responses suggested that this intentional framing facilitated accessibility without sacrificing conceptual depth. In retrospect, it would have been helpful to have the fully completed conceptual chart available (See Figure 1), as it visually captured our evolving hypotheses regarding the interrelationships among key constructs.
Although the format for participant interaction shifted unexpectedly during the first seminar, the use of a continuous chat stream proved generative. The real-time commentary allowed us to engage in reflective dialogue, posing questions to one another, inviting elaboration from our respective areas of expertise, and openly contemplating participants’ observations. Our intention was to model intellectual curiosity rather than endorse any singular interpretation of how theoretical concepts might apply. This stance appeared to invite participants to draw connections from their own theoretical orientations and clinical experiences, as well as from the provided materials.
Across both presentations and particularly during the in-person session participants engaged collaboratively in parallel learning processes that integrated personal and professional experience. This engagement deepened opportunities for co-creative and co-regulatory interaction. Notably, several participants remarked that the facilitation process itself embodied the relational qualities emphasized in the content, including warmth, curiosity, and attunement. They observed that the manner in which the material was presented was congruent with its relational and theoretical foundations.
From a professional development standpoint, these experiences suggest meaningful implications for practice. The process can be conceptualized as a model for mentoring, supervision, academic instruction, and direct clinical work. Parallel processes informed by Self Psychology such as mirroring, idealization, and twinship can be intentionally integrated across practice settings, supporting the professional growth of emerging Social Work practitioners and clients through empathic attunement and relational transmission of interdisciplinary and cross-theoretical knowledge. This dynamic was evident both within dyadic exchanges and at the group level, where diverse levels of expertise and experience contributed to a layered and generative learning environment. Such an approach can be deliberately replicated when grounded in sound theoretical principles as discussed within this report.
Competing Interests:
The authors declare that they have no competing interests.
References
Vaillant, G. E. (1995). The natural history of alcoholism, revisited. Harvard University Press. View
Perry, B. D., & Winfrey, O. (2021). What happened to you?: Conversations on trauma, resilience, and healing. Flatiron Books.View
Flores, P. J. (2004). Addiction as an attachment disorder. Jason Aronson. View
Panksepp, J., & Davis, K. (2018). The emotional foundations of personality. W. W. Norton & Company. View
Kohut, H. (1971). The analysis of the self. International Universities Press. View
Schore, A. N. (2019). The development of the unconscious mind. W. W. Norton & Company. View
National Association of Social Workers. (2021). Code of ethics of the National Association of Social Workers. NASW Press. View
Porges, S. W. (2014). The transformative power of feeling safe [Conference presentation]. Cape Cod Institute. View
LeDoux, J. E., Debiec, J., & Moss, H. (Eds.). (2003). The self: From soul to brain (Vol. 1001). New York Academy of Sciences. View
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50, 370–396. View
Kohut, H. (1977). The restoration of the self. International Universities Press. View
Berzoff, J. (1996). Drive theory. In J. Berzoff, L. M. Flanagan, & P. Hertz (Eds.), Inside out and outside in: Psychodynamic clinical theory and practice in contemporary multicultural contexts (pp. 18–43). Jason Aronson. View
Kaufman, A. (1963). [Concept of “borrowing the ego of the worker”]. In S. Loue & M. Sajatovic (Eds.), Oxford Research Encyclopedia of Social Work. Oxford University Press.
Schamess, G. (1996). Structural theory and ego psychology. In J. Berzoff, L. M. Flanagan, & P. Hertz (Eds.), Inside out and outside in: Psychodynamic clinical theory and practice in contemporary multicultural contexts (pp. 50–101). Jason Aronson.
Schore, J. R., & Schore, A. N. (2008). Modern attachment theory: The central role of affect regulation in development and treatment. Clinical Social Work Journal, 36(1), 9–20. View
Herman, J. L. (2018). Shattered shame states and their repair. In Attachment, trauma, and healing: Understanding and treating traumatic dissociation (pp. –). Routledge/Taylor & Francis.
Brown, B. (2012). Daring greatly: How the courage to be vulnerable transforms the way we live, love, parent, and lead. Gotham Books. View
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21(2), 95–103. View
Fonagy, P., Gergely, G., Jurist, E. L., & Target, M. (2002). Affect regulation, mentalization, and the development of the self. Other Press. View
Erikson, E. H. (1950). Childhood and society. W. W. Norton & Company. View
Elson, M. (1986). Self psychology in clinical social work. W. W. Norton & Company. View
Reich, A. (1960). Pathologic forms of self-esteem regulation. Psychoanalytic Study of the Child, 15, 215–232. View
Wolf, E. S. (1988). Treating the self. Guilford Press. View
Schore, A. N. (2003). Affect regulation and the repair of the self. W. W. Norton & Company View
Panksepp, J. (1988). Affective neuroscience: The foundations of human and animal emotions. New York, NY: Oxford University Press. View
McLellan, A. T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic medical illness. JAMA, 284(13), 1689–1695. View
Rowe, C. E., Jr., & MacIsaac, D. S. (1989). Empathic attunement: The “technique” of psychoanalytic self psychology. Jason Aronson. View
Palombo, J. (2017). The neuropsychodynamic treatment of selfdeficits: Searching for complementarity. Routledge. View
Schore, A. N. (2012). The science of the art of psychotherapy. W. W. Norton & Company. View
Sapolsky, R. M. (2005). Biology and human behavior: The neurological origins of individuality (2nd ed., Parts 1–2) [Video]. The Teaching Company. View
Bowlby, J. (1969). Attachment and loss: Vol. 1. Attachment. Basic Books. View
Morgan, M. A., & LeDoux, J. E. (1995). Differential contribution of dorsal and ventral prefrontal cortex to conditioned fear. Behavioral Neuroscience, 109, 681–688. View
van der Kolk, B. A., & Fisler, R. E. (1995). Dissociation and the fragmentary nature of traumatic memories: Overview and exploratory study. Journal of Traumatic Stress, 8(4), 505–525. View
Tronick, E. Z., & Weinberg, M. K. (1997). Depressed mothers and infants: Failure to form dyadic states of consciousness. In L. Murray & P. J. Cooper (Eds.), Postpartum depression and child development (pp. 54–81). Guilford Press. View
Vaughn, S. C. (1997). The talking cure. G. P. Putnam’s Sons. View
Wallin, D. J. (2007). Attachment in psychotherapy. Guilford Press. View
Tronick, E. Z. (1989). Emotions and emotional communication in infants. American Psychologist, 44(2), 112–119. View
Barbas, H. (1995). Anatomic basis of cognitive–emotional interactions in the primate prefrontal cortex. Neuroscience & Biobehavioral Reviews, 19, 499–510. View
Levin, F. M. (1997). Integrating some mind and brain views of transference: The phenomena. Journal of the American Psychoanalytic Association, 45(4), 1121–1151. View
Montgomery, A. (2013). Toward the integration of neuroscience and clinical social work. Journal of Social Work Practice, 27(3), 333–339. View
Whalen, P. J. (1998). Fear, vigilance, and ambiguity: Initial neuroimaging studies of the human amygdala. Current Directions in Psychological Science, 7(6), 177–188. View
Montgomery, A. (2020). Interpersonal neurobiology and attachment. In Encyclopedia of social work. View
White, W., & Kurtz, E. (2010). A message of tolerance and celebration: The portrayal of multiple pathways of recovery in the writings of Alcoholics Anonymous co-founder Bill Wilson. View
Alcoholics Anonymous World Services. (n.d.). A.A. around the world. View
Goldman, D., Oroszi, G., & Ducci, F. (2005). The genetics of addictions: Uncovering the genes. Nature Reviews Genetics, 6(7), 521–532. View
Hammer, R. R., Dingel, M. J., Ostergren, J. E., Partridge, B., & Koenig, B. A. (2013). The experience of addiction as a chronic disease: Comparing models of addiction. Social Science & Medicine, 76, 180–188. View
Heyman, G. M. (2009). Addiction: A disorder of choice. Harvard University Press. View
Leshner, A. I. (1997). Addiction is a brain disease, and it matters. Science, 278(5335), 45–47. View
Peele, S. (1985). The meaning of addiction: Compulsive experience and its interpretation. Lexington Books. View
Satel, S., & Lilienfeld, S. O. (2013). Addiction and the braindisease fallacy. Frontiers in Psychiatry, 4, Article 141. View
Volkow, N. D., Koob, G. F., & McLellan, A. T. (2016). Neurobiologic advances from the brain disease model of addiction. New England Journal of Medicine, 374(4), 363–371. View
Rush, B. (1784). An inquiry into the effects of ardent spirits on the human body and mind. Thomas Bradford. View
Alcoholics Anonymous World Services. (2001). Alcoholics Anonymous: The story of how many thousands of men and women have recovered from alcoholism (4th ed.). View
Applegate, J. S., & Shapiro, J. R. (2005). Neurobiology for clinical social work: Theory and practice. W. W. Norton & Company. View
von Bertalanffy, L. (1968). General system theory: Foundations, development, applications. George Braziller. View
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press. View
Payne, M. (2014). Modern social work theory (4th ed.). Oxford University Press. View
Turner, F. J. (Ed.). (2017). Social work treatment: Interlocking theoretical approaches (6th ed.). Oxford University Press. View
Perry, B. (n.d.). 10. Reward systems & maladaptive regulation [Video]. YouTube. View
Jung, C. G. (1976). Letters: Volume 1, 1906–1950 (G. Adler & Jaffé, Eds.; R. F. C. Hull, Trans.). Princeton University Press. View
Goldstein, E. G. (1995). Ego psychology and social work practice. Simon & Schuster. View
Rothschild, B. (2021). Revolutionizing trauma treatment: Stabilization, safety, & nervous system balance. W. W. Norton & Company. View
Brandell, J. R. (Ed.). (2011). Theory and practice of clinical social work (2nd ed.). Sage. View
Schafer, B. W., & Horejsi, C. R. (Eds.). (2006). Techniques and guidelines for social work practice. Pearson. View
Dana, D. A. (2020). The polyvagal theory in therapy. W. W. Norton & Company. View
Menakem, R. (2017). My grandmother’s hands: Racialized trauma and the pathway to mending our hearts and bodies. Central Recovery Press. View
Rogers, C. R. (1951). Client-centered therapy: Its current practice, implications, and theory. Houghton Mifflin. View
Schamess, G. (2006). Therapeutic process in clinical supervision: Part II. Clinical Social Work Journal, 34(4), 427–445. View
Koenig, T., & Spano, R. (2007). The cultivation of social workers’ hope in personal life and professional practice. Journal of Religion & Spirituality in Social Work: Social Thought, 26(3), 45–61. View
Opatrný, M., & Gehrig, R. B. (2021). Concepts and theory of spirituality in social work. In R. B. Gehrig, M. Opatrný, N. Birher, & K. Baumann (Eds.), Spirituality, ethics and social work (pp. 93–114). FreiDok plus. View
Kraut, R. (2020). Altruism. In The Stanford encyclopedia of philosophy (Fall 2020 ed.). View
Anonymous World Services, Inc. (1957). A.A. comes of age: A brief history of A.A. View
Bowlby, J. (1959). Maternal care and mental health. Geneva, Switzerland: World Health Organization. View
Panksepp, J. (1988). Affective neuroscience: The foundations of human and animal emotions. New York, NY: Oxford University Press. View
LeDoux, J. E. (1996). The emotional brain: The mysterious underpinnings of emotional life. New York, NY: Simon & Schuster. View
Perry, B. D., & Szalavitz, M. (2006). The boy who was raised as a dog: And other stories from a child psychiatrist’s notebook. New York, NY: Basic Books. View
Perry, B. D. (2017). The neurosequential model of therapeutics: Applying principles of neuroscience to clinical work with traumatized and maltreated children. In J. D. Ford & C. A. Courtois (Eds.), Treating complex traumatic stress disorders in children and adolescents (pp. 59–81). New York, NY: Guilford Press. View
Bion, W. R. (1962). Learning from experience. London, England: Heinemann. View
Whalen, P. J., Rauch, S. L., Etcoff, N. L., McInerney, S. C., Lee, M. B., & Jenike, M. A. (1998). Masked presentations of emotional facial expressions modulate amygdala activity without explicit knowledge. Science, 279(5358), 1771–1775. View
Bowlby, J. (1969). Attachment and loss: Vol. 1. Attachment. New York, NY: Basic Books. View
Bowlby, J. (1982). Attachment and loss: Vol. 1. Attachment (2nd ed.). New York, NY: Basic Books. View