
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy Volume 4 (2026), Article ID: JSWWP-181
https://doi.org/10.33790/jswwp1100181Research Article
Validating the Beliefs and Attitudes About Helping Questionnaire: An Exploratory Factor Analysis
Angela R. Wood1*, Ralph J. Wood2, Coleen Cicale1, Edward P. Hebert2, and Renee Underwood2
1Department of Health and Human Sciences, Southeastern Louisiana University, United States.
2Department of Kinesiology and Health Sciences, Southeastern Louisiana University, United States.
Corresponding Author Details: Angela R. Wood, Ph.D., LCSW-BACS, Assistant Professor, Department of Health and Human Sciences, Southeastern Louisiana University, SLU BOX 10863, Hammond, LA 70402, United States.
Received date: 24th November, 2025
Accepted date: 16th January, 2026
Published date: 19th January, 2026
Citation: Wood, A. R., Wood, R. J., Cicale, C., Hebert, E. P., and Underwood, R., (2026). Validating the Beliefs and Attitudes About Helping Questionnaire: An Exploratory Factor Analysis. J Soci Work Welf Policy, 4(1): 181.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Tools related to assessment of motivational interviewing (MI) practitioners are widely available such as the MITI, to assess skills, and MIKAT to assess knowledge. Informal self-assessments of the spirit of motivational interviewing also abound. Assessing the compatibility of one’s beliefs and attitudes about being a helper and helping others is largely missing. A survey was developed based on the spirit of MI and was piloted within a larger study of empathy among college students. An exploratory factor analysis resulted in a three-factor structure but did not demonstrate partnership, acceptance, compassion and empowerment as separate components, but rather as one factor. The second factor reflected items that were antithetical to MI, and the third factor recognized personal or self-awareness of the helper. Limitations of the study and recommendations for future research are noted.
Keywords: Motivational Interviewing, Helping Professionals, Person-centered Therapy, Factor Analysis, Attitudes, Beliefs, Questionnaire.
Introduction
Tools related to assessment of motivational interviewing (MI) practitioners are widely available such as the Motivational Interviewing Treatment Integrity tool, MITI [1], to assess skills, and Motivational Interviewing Knowledge and Attitudes Test, MIKAT [2], for evaluation of training outcomes. Informal self-assessments of the spirit of MI also abound [3]. Questionnaires that evaluate the compatibility of a helper’s beliefs and attitudes with the spirit of MI are missing. Helpers from a variety of settings and disciplines may have varying beliefs about their role in the helping process. These beliefs impact how they interact; what they say and how they say it. These interactions are vital to the development of rapport, the foundation of a successful helping relationship.
The spirit of MI forms the foundation of the approach. Four elements, partnership, acceptance, compassion, and empowerment. make up the spirit of MI. Partnership encompasses collaboration; an invitation to the client to share ideas and give input. Acceptance involves a non-judgmental attitude and accurate empathy toward the client. Compassion moves from an understanding and acceptance of the person to a desire to help and to care about the client. Empowerment brings out strengths and respects the autonomy of the client. These elements work together to guide the practitioner’s style, approach, and use of microskills such as open-ended questions, affirmations, reflections, and summaries. Miller and Rollnick [4] call it a “heart set and mind set.” It is a way of being with clients that helps form trust and safety needed to support the change process.
The spirit of MI fits with a patient-centered approach to care. While practitioners in a variety of helping professions by and large have good intentions to help others, beliefs about how to help clients change may conflict with the spirit of MI. For example, helping professionals may believe that being direct and providing warnings about behaviors or decisions that could result in negative consequences for the client is needed. This type of confrontation or directiveness, however, often results in decreased motivation for change and increases discord and disengagement in the therapeutic relationship [5]. Partnership, acceptance, and empowerment are negated.
Assessing the fit of the practitioner with the spirit of MI can help trainers, educators, coaches, and supervisors better understand potential barriers or challenges in teaching or coaching MI strategies which may impact the content and processes chosen for the workshop, class, or session. Various factors seem to predict implementation of motivational interviewing including practitioner demographics, knowledge of the approach, self-efficacy, attitudes toward the credibility and compatibility of the approach, and organizational factors [6]. Bell and Roomaney [7] had similar findings to Ager et al. [6] such as those who are younger, have more education, and a counseling background along with baseline MI skills best predicted adoption of motivational interviewing. Practitioner attitudes toward an evidence-based practice also predict successful implementation. Bell and Roomaney’s [7] qualitative study noted positive attitudes of some participants toward MI, recognizing the benefits of the approach. On the other hand, participants in Bell and Roomaney’s study also reported that staff who held negative attitudes toward MI, preferring an authoritative approach, did not appropriately apply MI skills. Similarly, Hatch et al. [8] found that resistance to MI was rated as one of the top influential staff-level barriers found in an organization-wide implementation study.
Thus, understanding a practitioner’s attitudes toward motivational interviewing (specifically the spirit) may be beneficial in understanding the potential for successful adoption and implementation into practice. Current assessments related to motivational interviewing are targeted toward training participants and current MI practitioners. Some of these tools measure knowledge acquisition, such as pre- and post-test training questionnaires which specifically use MI lingo and concepts. Several motivational interviewing tools are targeted toward observational measures of fidelity, particularly ones that assess skill acquisition. These tools do not measure attitudes and beliefs toward motivational interviewing. To better assess trainees’/students’ goodness of fit with MI, the researchers reviewed the elements of the spirit of motivational interviewing and developed questions to capture the essence of partnership, acceptance, compassion and empowerment. The inventory, the Beliefs and Attitudes About Helping Questionnaire, was piloted as part of a larger study [9].
Literature Review
Research studies that have included measures of attitudes or the spirit of motivational interviewing target training outcomes, such as skill acquisition, or barriers and facilitators to adoption of MI. An older study by Ager et al. [6] measured a variety of possible predictors of adoption and implementation of MI including attitudes toward MI pre- and post-training. Six items measured participants’ eagerness to learn and use MI. Questions like, “‘I believe that MI is an effective treatment for substance-involved individuals” were assessed using a 5-point Likert scale, from strongly disagree to strongly agree. The items specifically targeted attitudes toward MI.
Another study sought to develop an easy MI evaluation tool for use in supervision with community-based providers, different from formal coding instruments often used in clinical controlled studies. Baez et al. [10] included a measure of the spirit of MI in the Motivational Interviewing Evaluation Rubric (MIER). Used as an observation tool, providers are observed and rated based on a rubric that included high, medium, and low ratings of four items related to the spirit of MI. While the terms acceptance, compassion, and empowerment are not used, ratings of empathy, respect for autonomy, and two items related to partnership seem to fit. More testing is needed for the MIER, but results from this study are promising.
In a similar effort to measure fidelity and implementation of MI by non-clinical staff, Hohman and Matulich [11] administered questionnaires to clients at two residential treatment programs. One set of questions measured staff’s adherence to the spirit of MI and additional questions used a validated measure of working alliance for comparison. The study found that 10 of the items measured spirit factors of autonomy, collaboration and evocation. Construct validity was supported by significant correlations between the Motivational Interviewing Measure of Staff Interaction with the validated Working Alliance Inventory [11]. Again, this measure is based on client responses and perceptions.
Patient-centered collaborative care approaches fit with the spirit of MI. Patient-centered care emphasizes respect for the individual needs, values and preferences of patients and promoting collaboration between patients and providers [12]. One measure, the Patient- Practitioner Orientation Scale (PPOS), targets only medical care and doctors. Two items of 18 on the PPOS are patient-focused, “Patients should be treated as if they were partners with the doctor, equal in power and status,” and “A treatment plan cannot succeed if it is in conflict with a patient’s lifestyle or values” [12]. While these items fit with the spirit of MI and aspects of motivation for change, the remaining items on the scale do not apply to other helping professions and does not address all four elements of the spirit of MI.
Self-administered measures directly related to the spirit of MI have not been tested and are targeted toward social service or counseling professionals rather than helping professions in general. For example, the Self-Assessment Tool questions found in the book “The Aspirational Spirit of Motivational Interviewing” includes items that may not apply or resonate with healthcare providers. “I proceed in sessions without needing to have all the answers or a fixed plan,” and “I explore the client’s own ideas before offering solutions” [3]. While this tool is closely aligned to the questionnaire developed by the authors in the current study, Waitt’s self-assessment tool has not been tested or validated.
To fill this gap in assessing attitudes and beliefs toward the spirit of MI across helping professions, the Beliefs and Attitudes About Helping Questionnaire was developed by two of the authors and piloted as part of a larger study on empathy among college students in health and human science degree programs [9].
Development of the Questionnaire
The first two authors, both trained in and are trainers of, motivational interviewing, identified key beliefs and attitudes associated with each component of Miller and Rollnick’s [4] spirit of motivational interviewing. For partnership, we identified how collaboration involves identifying the client’s goals and resisting the urge to try to solve the problem or identify steps for the client. Partnership asks the provider to focus on the client’s desires and needs and minimizing our expert role. The client is the expert on themselves [4]. We developed items such as, “I believe the patients/clients have the ability solve their own problems,” and “I believe that the patient is the ‘expert on themselves.’”
The component acceptance relates to empathy and non judgmentalism. There is a belief in the person’s inherent worth [4]. Items were written such as, “I believe all patients/clients are capable of changing,” and “I believe all patients/clients are unique and have significant value.” Where acceptance seeks to understand and not judge, compassion connects with the provider’s desire to help out of a sense of caring and concern. These items included “I chose to go into a helping profession to make an impact on my patients/clients.” and “I chose to go into a helping profession to care for my patients/ clients.”
Items such as “The goal for interactions with my patients/clients is to empower them,” “Patients/clients should be empowered to be autonomous,” “Patients/clients have the right to do what they want to do even if it may be harmful,” and “It is important to identify your patient’s/client’s strengths” represent the component empowerment. Empowerment refers to helping clients identify and use their strengths to achieve their goals [4]. The belief is that clients have what they need, we just need to help them bring it out [4].
Reverse items included directive beliefs such as “Sometimes you just have to tell your patient/client ‘how it is,’” “The goal for interactions with my clients is to fix them,” and “One of the most helpful things that I can do for my patients/clients is to give them advice.” These were written to capture beliefs that conflict with the spirit of MI and therefore are not corresponding items specific to the components of the spirit of MI.
The survey asks responders to rate their beliefs or attitudes on each item using a 4-point Likert scale, where 1 = strongly disagree and 4 = strongly agree.
Methodology
After receiving approval from the Institutional Review Board, data were collected March 27, 2023, through May 5, 2023. Using a cross-sectional design, an online survey was used to collect the data. Participation was sought through email messages sent to all registered students within the university’s health and human sciences college. Participants were informed that the research team was studying empathy among students enrolled in a variety of health and human science degrees, their participation was voluntary, and their responses were anonymous. The survey contained demographic questions, the Interpersonal Reactivity Index [13] to measure empathy, and the 24- item Beliefs and Attitudes about Helping.
Data Analysis
To examine the underlying structure of a newly developed survey assessing the compatibility of individuals’ beliefs and attitudes about being a helper and helping others, an exploratory factor analytic approach was utilized. The instrument was developed in the spirit of Motivational Interviewing (MI) and piloted within a larger study of empathy among college students.
The analytic sample consisted of 519 participants (n=519), exceeding commonly recommended sample size thresholds for exploratory factor analysis and supporting the stability of the factor solution [14]. Missing data were handled using listwise deletion, consistent with SPSS default procedures.
Prior to factor extraction, the suitability of the data for factor analysis was assessed. Sampling adequacy was evaluated using the Kaiser–Meyer–Olkin (KMO) measure, and Bartlett’s Test of Sphericity was conducted to determine whether the correlation matrix was factorable. The KMO value was .707, exceeding the suggested suitability score, according to Williams et al. (2010). The Bartlett’s Test of Sphericity was statistically significant, χ²(36) = 725.88, p < .001, supporting the appropriateness of factor analysis.
A principal components analysis (PCA) with oblique (Oblimin) rotation was conducted. An oblique rotation was selected based on the theoretical expectation that beliefs and attitudes related to helping would be conceptually related. Factors were retained using the Kaiser criterion (eigenvalues > 1.0) and visual inspection of the scree plot, with interpretability guided by theoretical alignment with MI-informed helping principles. Following factor extraction, internal consistency reliability analyses were conducted for subscales corresponding to each factor using Cronbach’s alpha.
Results
As indicated in Table 1, the sample was primarily female (82.2%); over 70% were 18-23 years old, the age range of traditional college students; and most (61.1%) were upperclassmen and graduate students. Slightly over 74% reported their race/ethnicity as White, followed by African American (17.2%).
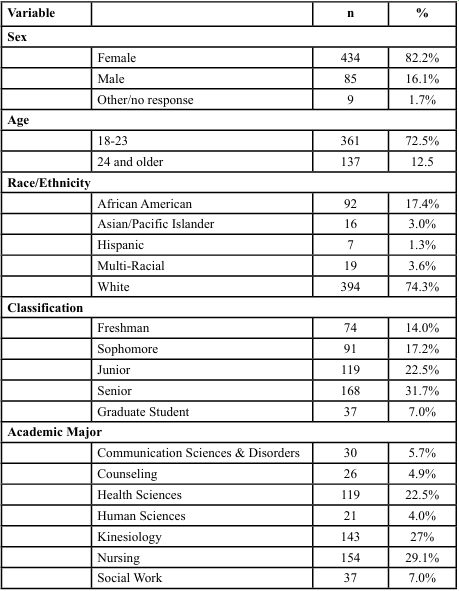
Table 1: Descriptive Characteristics of the Sample (N=530)
Factor Structure
The analysis yielded a three-component solution, accounting for 58.47% of the total variance. The eigenvalues for the three retained components were 2.28, 1.96, and 1.02, respectively. Inspection of the scree plot supported the retention of three components, with a clear leveling of eigenvalues after the third component.
Component 1: Collaborative, Values-Consistent Helping (MI Spirit)
The first component accounted for 25.36% of the variance and reflected a collaborative, values-consistent helping orientation. Items loading strongly on this component emphasized compassion and desire to help, belief in the client’s inherent value as a person, importance of client strengths. Pattern matrix loadings ranged from .61 to .80, indicating a strong and coherent factor. This component aligns closely with the spirit of Motivational Interviewing, particularly the components of compassion, empowerment, and acceptance.
Component 2: Directive Helping Orientation
The second component accounted for 21.75% of the variance and consisted of items reflecting a directive approach to helping, including beliefs about giving advice, providing solutions, and telling individuals what to do. Pattern matrix loadings ranged from .58 to .80, indicating a well-defined and interpretable factor. This component distinguishes directive helping beliefs from more collaborative helping orientations and represents a conceptually distinct dimension of helper attitudes.
Component 3: Autonomy
The third component accounted for 11.37% of the variance and included items related to autonomy. Items on this component demonstrated strong negative loadings (ranging from −.70 to −.78), reflecting item wording and direction rather than conceptual opposition.
Component correlations were small, supporting conceptual relatedness without redundancy. Component 1 demonstrated a modest negative correlation with Component 3 (r = −.22), while correlations between Component 1 and Component 2 (r = −.01) and between Component 2 and Component 3 (r = −.13) were minimal.
Reliability Analyses
MI Spirit Subscale
Internal consistency reliability was examined for the MI Spirit subscale derived from Component 1. This subscale consisted of three items and demonstrated a Cronbach’s alpha of .64, based on 528 valid cases. The mean score was 11.28 (SD = 1.05). Although modest, this alpha value is considered acceptable for a brief, newly developed scale used in exploratory research.
Directive Helping Orientation Subscale
The Directive Helping Orientation subscale, corresponding to Component 2, consisted of four items. Reliability analysis yielded a Cronbach’s alpha of .67, based on 525 valid cases. The mean score was 9.39 (SD = 2.41). This value indicates acceptable internal consistency for an exploratory attitudinal measure.
Autonomy Subscale
Reliability analysis for the Autonomy subscale (two items) revealed low internal consistency, with a Cronbach’s alpha of .42, based on 528 valid cases. The mean score was 6.86 (SD = 1.01). As a result, this subscale was not treated as a reliable composite measure.
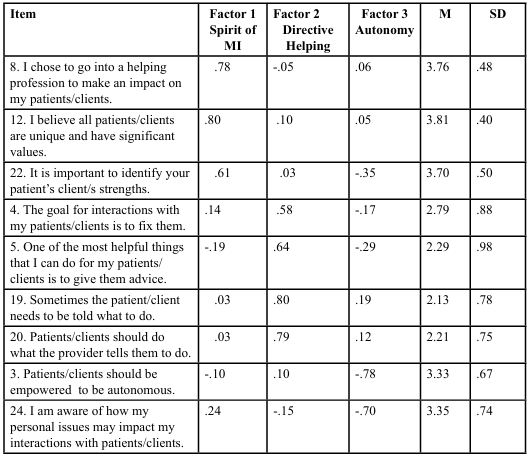
Table 2: Factor Loadings
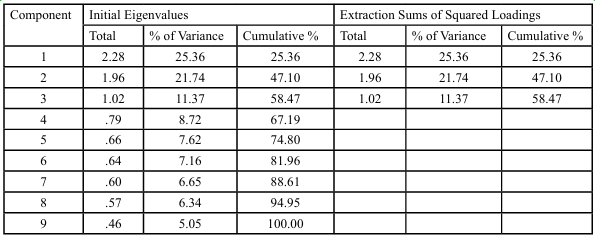
Table 3: Total Variance Explained
Discussion
From the reliability analyses, two subscales, the MI Spirit (compassion and acceptance) and Directive Helping Orientation, demonstrated acceptable internal consistency for exploratory research, particularly given the brief nature of the scales and the early stage of instrument development. These findings provide preliminary support for the use of these subscales in pilot research and educational contexts.
In contrast, the Autonomy subscale did not demonstrate adequate internal consistency. The Cronbach’s alpha of .42 suggests that the items included in this subscale do not currently function as a coherent unidimensional construct. Examination of item content and item-total statistics indicates that the items may reflect conceptually distinct processes, including empathic orientation, beliefs about others’ capacity for change, and perceived emotional influence. Additionally, differences in item directionality and the inclusion of potentially reverse-worded items may have contributed to negative inter- item covariances. The instability of reliability estimates is further amplified by the very small number of items, as alpha coefficients are known to be particularly sensitive in short scales [15].
Importantly, this pattern is consistent with best practices in exploratory scale development, where early psychometric testing is expected to identify items or subscales requiring refinement. Rather than indicating a flaw in the analytic approach, these findings provide valuable guidance for improving the conceptual clarity and measurement precision of the instrument.
Limitations
Several limitations should be considered when interpreting these findings. First, the study employed a principal components analysis rather than a common-factor extraction method, which may limit conclusions about latent constructs. However, PCA is appropriate for early-stage scale development and data reduction, particularly in pilot research contexts.
Second, although the sample size was large and adequate for factor analysis, the sample consisted exclusively of college students, which may limit the generalizability of findings to professional helpers or clinical populations. Replication with more diverse samples is warranted.
Third, internal consistency reliability for two of the identified subscales was modest, reflecting the brief nature of the scales and the exploratory stage of instrument development. In particular, the Autonomy subscale demonstrated low reliability, indicating the need for item refinement, rewording, or expansion before it can be used as a composite measure. Finally, all data were based on self-report, which may be influenced by social desirability or response bias, especially when assessing helping-related beliefs and attitudes.
Despite these limitations, the findings provide preliminary support for a multidimensional conceptualization of helper belief compatibility, distinguishing collaborative, directive, and emotionally oriented helping attitudes in ways that are theoretically consistent with Motivational Interviewing. The results offer a strong foundation for continued scale refinement and validation.
Recommendations for Scale Refinement
Future development of the Autonomy domain should focus on item revision and construct clarification. Specifically, clarifying the construct, reviewing directionality of the items, and expanding the items to lengthen the scale. Clarifying construct boundaries by determining whether encouraging autonomy and the importance of change to the client represent autonomy as a single dimension or multiple related but distinct constructs. Clarifying construct boundaries allows for improved reliability, stronger construct validity, closer alignment with theory, and more precise interpretation by ensuring that scale items reflect coherent psychological processes rather than conceptually distinct domains.
Reviewing and correcting item directionality, including careful evaluation of reverse-coded items, helps ensure psychological consistency across scale items. Reverse-coded items are often included to reduce acquiescence bias; however, when they are poorly worded or conceptually misaligned, they can introduce confusion, increase measurement error, and produce negative or weak inter- item correlations. Ensuring that all items reflect the construct in a consistent psychological direction improves item clarity, strengthens inter-item relationships, and enhances both internal consistency reliability and factor interpretability. This process is especially important in scales assessing complex relational constructs, where subtle wording differences can alter respondents’ interpretations.
Expanding the item pool within a domain improves internal consistency and allows for more stable and accurate reliability estimation. Reliability coefficients such as Cronbach’s alpha are sensitive to the number of items, and very short scales often yield attenuated or unstable estimates even when items are conceptually related. Adding well-aligned items increases scale breadth, reduces the influence of idiosyncratic item variance, and enhances the precision with which the underlying construct is measured. A larger item pool also supports more robust factor analytic testing, facilitates item reduction based on empirical performance, and strengthens the foundation for future confirmatory analyses.
Conclusions
Future studies could assess the correlation between the factor scores of the Beliefs and Attitudes questionnaire as well as each individual item with each dimension of the Davis Interpersonal Reactivity Index (which was collected in this current data set). This would help identify which questionnaire items most closely fit the element of Acceptance (specifically empathy). It would also be beneficial to identify other validated scales that represent other elements of the spirit of MI such as empowerment and partnership.
The authors of this study are interested in assessing the baseline beliefs and attitudes of individuals entering into helping professions (beginning training in MI) and how these beliefs might influence their ability to learn and implement motivational interviewing into their professional practice. The Attitudes and Beliefs About Helping Questionnaire provided a starting point for attempting to measure the spirit of MI. Overall, these findings support continued refinement and validation of the instrument and highlight the value of iterative psychometric testing in the development of measures grounded in complex relational constructs such as those informed by Motivational Interviewing.
Competing Interests:
The Authors have no competing interests to disclose.
References
Moyers, T.B., Manuel, J.K., & Ernst, D. (2014). Motivational Interviewing Treatment Integrity coding manual 4.1. Unpublished manuscript. View
Leffingwell, T. R. (2006). Motivational Interviewing Knowledge and Attitudes Test (MIKAT) for evaluation of training outcomes. MINUET, 13, 10-11. View
Waitt, A., Cameron, S., Bonaiuto, D., Galletto, A., Jordan, A., & Wood, A. (2024). The aspirational spirit of motivational interviewing. View
Miller, W. R., & Rollnick, S. (2023). Motivational interviewing: Helping people change and grow (4th ed.). Guilford Press. View
Laws, M. B., Rose, Gary, S., Beach, M. C., Lee, Y., Rogers, W. S., Velasco, A. B., & Wilson, I. B. (2015). Patient-provider concordance with behavioral change goals drives measures of motivational interviewing consistency. Patient Education and Counseling, 98(6), 728-733.
Ager, R., Roahen-Harrison, S., Toriello, P. J., Kissinger, P., Morse, P., Morse, E., Carney, L., & Rice, J. (2011). Predictors of adopting motivational enhancement therapy. Research on Social Work Practice, 21(1), 65-76. View
Bell, D. L., & Roomaney, R. (2020). Exploring the barriers that prevent practitioners from implementing motivational interviewing in their work with clients. Social Work, 56(4), 416- 429. View
Hatch, M. R., Carandang, K., Moullin, J. C., Ehrhart, M. G., & Aarons, G. A. (2021). Barriers to implementing motivational interviewing in addiction treatment: A nominal group technique process evaluation. Implementation Research & Practice, 2(Jan-Dec), 1-10. View
Wood, A. R., & Wood, R. J. (2025). A cross-sectional study of empathy among college students in health and human sciences degree programs. Journal of Public Health Issues and Practices, 9(1):231. View
Baez, J. C., Galanis, R., & Magill, M. (2020). When the right measure doesn’t exist: A novel motivational interviewing tool for community programs. Child and Adolescent Social Work Journal, 37, 195-205. View
Hohman, M., & Matulich, W. (2010). Initial validation of the Motivational Interviewing Measure of Staff Interaction. Alcoholism Treatment Quarterly, 28, 230-238. View
Bunc, K. T. (2025). Validation of the Slovenian version of the Patient-Practitioner Orientation Scale – PPOS. ACTA Medico-Biotechnica, 18(1), 48-60. View
Davis, M. H. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology, 10, 85. View
Williams, B., Onsman, A., & Brown, T. (2010). Exploratory factor analysis: A five-step guide for novices. Journal of Emergency Primary Health Care (JEPHC (3), 1–13. View
Tavakol, M., & Dennick, R. (2011). Making sense of Cronbach's alpha. International Journal of Medical Education, 2, 53–55. View