
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy Volume 4 (2026), Article ID: JSWWP-186
https://doi.org/10.33790/jswwp1100186Research Article
Cultural Stress, Identity Factors, and Behavioral Health Needs in Youth: A Field-Based Study Using CANS Assessment Data
Darron Garner1, PhD, LCSW-S, and Jackson de Carvalho2*, PhD
1Associate Professor of Social Work, Department of Social Work, Prairie View A&M University, Prairie View, Texas 77446, United States of America.
2Professor & MSW Program Director, Prairie View A&M University, Prairie View, Texas 77466, United States of America.
Corresponding Author Details: Jackson de Carvalho, PhD, Professor & MSW Program Director, Prairie View A&M University, Prairie View, Texas 77466, United States of America.
Received date: 27th January, 2026
Accepted date: 07th March, 2026
Published date: 11th March, 2026
Citation: Garner, D., & Carvalho, J., (2026). Cultural Stress, Identity Factors, and Behavioral Health Needs in Youth: A Field Based Study Using CANS Assessment Data. J Soci Work Welf Policy, 4(1): 186.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Cultural stressors and challenges related to identity have increasingly been recognized as significant factors affecting behavioral health outcomes in children and adolescents, particularly those involved in publicly funded care systems. However, empirical research in the child and adolescent social work literature that combines cultural stress indicators with standardized clinical assessment data remains scarce. This study uses de-identified data from the Child and Adolescent Needs and Strengths (CANS) assessment, comprising 230 participants, to examine the prevalence of cultural stress and identity-related factors and evaluate their predictive relationships with behavioral health needs. Descriptive analyses indicate considerable rates of trauma exposure, emotional dysregulation, and social functioning difficulties among participants. Furthermore, multiple regression analyses reveal that indicators of cultural stress serve as significant predictors of the severity of behavioral health needs, even after controlling for trauma exposure and demographic variables. These findings highlight the need to implement culturally responsive and identity-affirming assessment and intervention strategies within youth behavioral health systems.
Keywords: Cultural stressors; identity; CANS; trauma and Research.
Introduction
Youth receiving publicly funded behavioral health services frequently experience intersecting forms of trauma exposure, structural disadvantage, and identity-related stress. While trauma has been extensively studied as a predictor of behavioral health outcomes, emerging research suggests that cultural stress, defined as chronic exposure to discrimination, marginalization, acculturative pressures, and identity invalidation, may independently contribute to emotional and behavioral distress [1,2]. Cultural stress differs from discrete traumatic events in that it is often cumulative, chronic, and embedded within broader sociopolitical systems. During adolescence, a critical period for identity development, such stressors may disrupt emotional regulation, self-concept, and coping processes. Despite increasing theoretical attention, few quantitative studies have examined how cultural stress functions within standardized clinical assessment frameworks.
The Child and Adolescent Needs and Strengths (CANS) assessment is a widely used community metric tool designed to inform service planning and outcomes management 2022). Unlike traditional psychometric instruments, the CANS emphasizes actionability of needs across multiple ecological domains, including behavioral health, trauma exposure, life functioning, cultural factors, and identity-related stressors. However, limited empirical work has examined how cultural and identity-related CANS indicators predict overall behavioral health need severity. The present study addresses this gap by examining de-identified CANS data from youth receiving publicly funded behavioral health services to:
1. Assess the prevalence of cultural stress and identity-related factors.
2. Evaluate whether these factors predict behavioral health need severity beyond trauma exposure and demographic characteristics.
By centering cultural stress within a quantitative analytic framework, this study advances culturally responsive child and adolescent social work research and practice.
Literature Review
Cultural stress perspectives emphasize how chronic exposure to discrimination, marginalization, acculturative strain, and identity invalidation functions as a distinct and cumulative stressor embedded within social hierarchies [1,2]. When situated within the ecological framework, these stressors are understood not as isolated interpersonal incidents but as multilevel exposures operating across microsystem, mesosystem, exosystem, and macrosystem contexts. At the microsystem level, youth may experience direct discriminatory interactions with peers, teachers, or service providers. At the mesosystem level, inconsistent or invalidating responses across home and institutional settings may intensify stress exposure. At the macrosystem level, structural racism, anti-immigrant sentiment, and gender-based stigma shape broader sociopolitical climates that normalize marginalization. Thus, cultural stress is socially patterned, developmentally embedded, and ecologically reinforced.
Minority stress theory provides a complementary mechanism for understanding how these ecological exposures translate into psychological outcomes. Originally developed to explain health disparities among stigmatized groups, minority stress theory differentiates between distal stressors (objective discriminatory events and structural stigma) and proximal stress processes (internalized stigma, concealment, expectations of rejection, and hypervigilance). Cultural stress, in this framework, reflects the cumulative burden of distal exposures that activate proximal psychological processes. Youth exposed to repeated discrimination may develop anticipatory vigilance, heightened emotional reactivity, and internalized negative self-perceptions, which in turn elevate risk for depression, anxiety, behavioral dysregulation, and suicidal ideation [1]. Importantly, minority stress theory underscores that these processes are chronic rather than episodic. Unlike discrete traumatic events, cultural stress is often ambiguous, persistent, and institutionally sanctioned. Adolescence represents a particularly vulnerable developmental period, as identity exploration intensifies and belonging becomes central to psychosocial development. When identity-based invalidation occurs repeatedly during this stage, it may undermine self-concept coherence, disrupt adaptive coping, and erode institutional trust. Behavioral responses such as withdrawal, oppositionality, or hypervigilance may function as adaptive strategies within stigmatizing contexts but are frequently misinterpreted within clinical settings as intrinsic pathology.
Identity-related factors play a critical mediating and moderating role within both ecological and minority stress frameworks. Racial and ethnic identity development, for example, can buffer the psychological impact of discrimination when accompanied by positive private regard and culturally affirming socialization [2]. In minority stress terms, strong and positively integrated identity may mitigate proximal stress processes by reducing internalized stigma and strengthening coping resources. Conversely, identity centrality without affirmation, internalized oppression, or identity conflict may heighten vulnerability to internalizing and externalizing symptoms. Similarly, acculturative stress among immigrant-origin youth, including intergenerational cultural conflict and bicultural strain, can be conceptualized as both an ecological pressure and a minority stress process. Youth navigating bicultural identities may face external invalidation alongside internal identity tension, increasing susceptibility to emotional distress [1]. Gender-diverse adolescents experience analogous patterns, wherein structural stigma and identity-based discrimination (distal stressors) contribute to expectations of rejection and internalized stigma (proximal stressors), elevating behavioral health risk. Thus, identity-related variables are not peripheral covariates but central mechanisms through which cultural stress influences developmental outcomes.
These dynamics are further complicated for youth receiving publicly funded behavioral health services. Service system involvement often intersects with structural disadvantage, trauma exposure, and heightened surveillance. From an ecological standpoint, institutional monitoring within schools, child welfare, or behavioral health systems may amplify exosystem and mesosystem pressures. From a minority stress perspective, repeated labeling or deficit-based interpretation within these systems may intensify proximal stress processes, including distrust and concealment. As Lyons et al. [3] note, service engagement occurs within relational and structural contexts that shape youth perceptions of safety and validation. Consequently, youth navigating publicly funded systems may experience compounded stress burdens that exceed traditional trauma exposure alone.
Liberation-oriented and culturally responsive social work frameworks extend these theoretical perspectives by centering power, oppression, and resistance [4]. Whereas ecological and minority stress theories describe how stress operates, liberation-oriented practice interrogates why such stress persists and how systems may reproduce inequity. From this lens, behavioral symptoms are reframed as contextually adaptive responses to structural marginalization. Emotional withdrawal may represent self-protection in stigmatizing environments; oppositionality may signal resistance to invalidating authority; hypervigilance may reflect survival within unsafe institutional spaces. These reframing challenges deficit-based diagnostic interpretations and demands assessment approaches capable of capturing sociocultural determinants of distress.
The Child and Adolescent Needs and Strengths (CANS) assessment align with this integrated framework by operationalizing ecological and cultural domains alongside clinical indicators. The instrument includes items related to trauma exposure, cultural identity, environmental stressors, and caregiver context, thereby permitting systematic measurement of factors consistent with ecological and minority stress constructs. However, despite its multidimensional structure, limited empirical research has examined whether cultural stress and identity-related CANS items independently predict behavioral health need severity beyond trauma exposure [5]. Much of the existing literature isolates trauma or symptom clusters without evaluating the incremental contribution of sociocultural stress processes. Children and adolescents receiving publicly funded behavioral health services frequently navigate the convergence of trauma, structural disadvantage, and identity-based stress. While cultural stress has been linked to adverse mental health outcomes, its quantitative predictive role within standardized assessment systems remains underexamined. Addressing this gap is critical for ensuring that publicly funded service models move beyond trauma-only frameworks and incorporate sociocultural determinants of health.
Building upon the integrated framework of socio-ecological systems theory, minority stress theory, and liberation-oriented social work practice, the present study advances a testable model in which cultural stress and identity-related factors function as distinct predictors of behavioral health need severity among youth receiving publicly funded services. Consistent with ecological theory, individual- level symptom presentation is conceptualized as embedded within microsystem and mesosystem influences. Minority stress theory further specifies that distal stressors (e.g., discrimination, cultural invalidation, acculturative strain) contribute to psychological distress both directly and through proximal stress processes.
Methods
This study synthesizes the existing literature on factors influencing the behavioral health needs of children receiving publicly funded care [6,7]. Building on these findings, the subsequent phase employs a quantitative, cross-sectional, predictive design, guided by a multiple linear regression model as the statistical framework [8]. This systematic approach aims to investigate the impact of various factors and their interactions on targeted responses, elucidate the sources of variance, and ensure the replication of results [9]. Thus, a comprehensive cross-sectional analysis was conducted using de-identified CANS (Child and Adolescent Needs and Strengths) assessment data, which was meticulously sourced as part of the established behavioral health service delivery process. This service delivery approach enabled a detailed examination of the data while ensuring respondents' confidentiality [10].
Research Question and Hypotheses
RQ: What impact do cultural stressors and identity-related factors have on the behavioral health outcomes of youth using publicly funded care services?
H1: Higher levels of cultural stressors are associated with lower levels of behavioral health outcomes among youth using publicly funded care services
H2: Lower levels of identity-related factors are associated with higher levels of behavioral health outcomes among youth using publicly funded care services
H3: Higher levels of trauma exposure are associated with lower levels of behavioral health outcomes among youth using publicly funded care services
Sample
The present study utilized a retrospective cohort design to evaluate the impact of the Cultural stressors and challenges associated with identity-related factors on the behavioral, emotional, and functional outcomes of youth enrolled in public services. Data was obtained from a renowned non-profit behavioral health provider agency (501(c)(3)) that operates multiple facilities across Texas. This agency offers a comprehensive continuum of care for children and young adults aged 0 to 24 years. Although exact enrollment figures are not available, it is estimated that approximately 95% of the youth participating in publicly funded programs are concurrently enrolled in this agency’s services.
The sample consisted of 230 youth using publicly funded care services who completed CANS assessments. A sample size of 230 participants is deemed sufficient to achieve adequate statistical power for the analysis, thereby inspiring trust in the research process [11]. Available demographic variables included age, race/ethnicity, and gender. Youth represented a range of developmental stages, with ages spanning childhood through late adolescence. The sample reflected racial and ethnic diversity commonly observed in publicly funded behavioral health systems, including youth who identified as Black/ African American, Hispanic/Latinx, White, or multiracial. Gender identity data were examined, and demographic variables were retained as covariates in predictive analyses to account for developmental and structural differences in behavioral health presentation. The dataset included 178 variables representing multiple domains, including behavioral and emotional needs, trauma exposure, life functioning, strengths, cultural stress, and identity-related factors.
Measures
Youth functioning was assessed utilizing the Child and Adolescent Needs and Strengths (CANS) tool, which evaluates functioning based on the "actionability" of specific needs [3]. We analyzed changes in three distinct metrics: the net change in the number of needs categorized as "actionable," the number of needs resolved over a six-month period, and the number of new needs identified within the same timeframe. The CANS instrument assesses the needs and strengths of children and adolescents across a range of social-ecological domains, including individual and family contexts. However, it is important to note that while the CANS was initially designed to inform service delivery for children with emotional and behavioral healthcare requirements, the effectiveness of this tool in measuring the impact of cultural barriers and identity-related factors on the behavioral health of youth utilizing public services has yet to be evaluated [3,11].
The Child and Adolescent Needs and Strengths (CANS) assessment serves dual purposes: it facilitates service matching and serves as an outcome measure [3]. This assessment adopts a "communimetric" rather than a psychometric approach, prioritizing the provision of actionable information to enhance clinical decision-making. Rather than focusing on the symptoms of behavioral health issues, the CANS emphasizes identifying individual "needs" that reflect the various challenges children encounter. Examples of these needs encompass "Self-Injurious Behavior," "Sexual Aggression," "Social Functioning," "Anxiety," and "Substance Use [3]." Each need is assigned a score ranging from 0 to 3:
• A score of 0 indicates "no evidence" of a need,
• A score of 1 signifies that "watchful waiting or prevention" is prudent,
• A score of 2 denotes a need that necessitates "action," and
• A score of 3 represents a need that requires "immediate or intensive action."
Scores of 2 and 3 are classified as "actionable" needs, indicating they are suitable targets for behavioral health treatment. When these items are identified as actionable, the cumulative CANS scores can be interpreted as a tally of "needs" distinct areas where a youth may benefit from intervention [12].
In the specific iteration of the CANS employed by the current provider agency, there are 79 items categorized into seven domains:
• Behavioral and Emotional Needs (e.g., "Psychosis" and "Depression")
• Life Functioning (e.g., "Family Relationships" and "School Functioning")
• Child Risk Behaviors (e.g., "Self-Injurious Behavior" and "Sexual Aggression")
• Cultural Factors (e.g., "Language" and "Discrimination/Bias")
• Caregiver Resources and Needs (e.g., "Involvement with Care" and "Knowledge")
• Child Strengths (e.g., "Optimism" and "Community Life")
• Traumatic Adverse Childhood Experiences (e.g., "Physical Abuse" and "Medical Trauma").
Each item of the CANS is accompanied by a concise description to facilitate accurate scoring. For example, guidance for assigning a score of "3" to "Depression" states: "Clear evidence of depression that is disabling for the child across multiple life domains."
Some CANS items are collected in optional "modules" that provide additional details about specific needs. These items are completed only for youth who have an actionable need based on specific triggering items from the domains. For example, if a youth scores a 2 or 3 on the item "Runaway," they will subsequently be assessed using the runaway module, which consists of eight additional items: consistency of destination, frequency of running, involvement in illegal activities, involvement of others, likelihood of returning independently, planning, realistic expectations, and safety of the destination [11]. Unlike items within the main domains, these module items do not represent discrete needs and are not completed for all youths. Consequently, they are excluded from the analyses presented in this paper. The Child and Adolescent Needs and Strengths (CANS) tool has demonstrated robust inter-rater reliability among both researchers and caseworkers [13].
The measure under consideration is complex, and changes in child outcomes can be assessed through various methodologies. The CANS tool is sometimes used to determine eligibility for different types and intensities of services [11]. The developers of the CANS collaborate with licensees to customize the assessment by adding, removing, or modifying items. Hence, the CANS may not be uniform across diverse contexts [3]. However, no modifications to the CANS were implemented during the timeframe examined in this paper.
In the present investigation, both baseline and six-month CANS assessments were employed. A baseline CANS is defined as any CANS administered within 30 days before or after enrollment, while a six-month CANS is characterized as any CANS administered between 150 and 210 days following enrollment [3]. Both assessments were conducted by the Wraparound care coordinator in collaboration with the youth and their family. Overall, the CANS is a widely utilized assessment instrument designed to identify the treatment needs of individuals aged 6 to 20 and to support informed intervention decisions, achieving a Cronbach's alpha of 0.82 [11].
Behavioral Health Needs
Behavioral health needs represent a complex tapestry of mental, emotional, and social well-being that is vital to an individual's overall quality of life [1]. These needs encompass a variety of conditions, including anxiety, depression, substance use disorders, and the lasting effects of trauma, all of which can significantly impede daily functioning. It is estimated that more than 50 million Americans are grappling with these challenges, highlighting the urgent demand for specialized care that addresses the intertwined aspects of behavioral and physical health [14]. A broad spectrum of services is available to support individuals on their journeys toward recovery, ranging from proactive prevention programs and personalized counseling sessions to immediate crisis intervention strategies designed to provide urgent relief in times of need [15]. These tailored approaches are essential for fostering resilience and restoring balance in people's lives. Behavioral health need severity was operationalized as a composite score derived from actionable ratings across emotional and behavioral need domains, including emotional regulation, anxiety, depression, and behavioral control [15].
Cultural Stress and Identity Factors
Cultural stress indicators included CANS items assessing experiences of discrimination, marginalization, cultural conflict, and identity- related stress [3]. Identity factors included variables related to gender identity, sexual orientation, and cultural identity challenges. Cultural stress is a profound psychological strain that individuals often endure when they confront discrimination, experience marginalization, or face the relentless pressure to conform to societal expectations [1]. This phenomenon can significantly affect mental health, leading to identity crises, confusion, and a decline in overall well-being, especially among immigrants and marginalized communities [1,2].
The experience of cultural stress typically arises when individuals navigate the tumultuous waters of conflicting cultural norms and values [1]. Such internal conflicts can exacerbate feelings of anxiety and depression while eroding self-esteem, encouraging the audience to understand the emotional toll of these struggles [4]. Conversely, a strong sense of cultural identity nurtured and fortified by family, community ties, and traditional practices can serve as a vital protective factor. This resilience, cultivated in the embrace of one's cultural roots, empowers individuals to confront these challenges with renewed strength and a sense of belonging, inspiring the audience to value cultural connections as sources of strength [2,4].
Trauma Exposure
Trauma exposure variables included a history of physical abuse, emotional abuse, domestic violence exposure, and environmental violence. Trauma exposure refers to the profound experience or observation of events marked by threats, injury, or the specter of death [16]. This complex phenomenon encompasses a wide array of incidents, varying from isolated occurrences such as sudden accidents or distressing episodes of abuse to more pervasive situations, including the brutal realities of warfare or chronic neglect [17]. Recognizing that the impact of trauma is deeply individualized can help the audience feel empathetic and aware of the diverse outcomes, such as PTSD, resilience, or other mental health challenges [17]. The effects of trauma are shaped by a multitude of factors, including the intrinsic nature of the traumatic event, the timing of exposure in one’s life, and the unique personal circumstances of the individuals involved. This understanding can help the audience feel informed and responsible for recognizing how different factors influence trauma outcomes and mental health [18,19].
Management of Missing Data
Two distinct methodologies were employed to address missing data. The first approach involved listwise deletion for cases in which any Child and Adolescent Needs and Strengths (CANS) item received an “unknown” rating, or where more than 9 items over a quarter were missing data. This technique reduced the original sample size from 260 to 230 youth participants. Furthermore, an alternative strategy utilizing the maximum likelihood approach with PRELIS was implemented to mitigate the effects of missing data [20]. This imputation method aimed to minimize bias while preserving the randomness and variability of the estimated values [10,20].
Data Analysis
Quantitative data were analyzed using IBM SPSS, utilizing descriptive statistics and multiple linear regression. Comprehensive descriptive statistics were calculated to provide an overview of the demographic characteristics of the sample population, including their age, gender distribution, ethnic backgrounds, income levels, and educational attainment [10]. Mean differences across demographic groups were examined descriptively to highlight patterns of risk [9,10].
This analysis aims to provide a clearer understanding of the diverse attributes and socio-economic factors present within the targeted group. To accomplish this, we carefully estimated a multiple linear regression model to examine the relationship between cultural stress, identity-related factors, and their potential impact on the severity of behavioral health needs. We conducted this examination while controlling for trauma exposure and key demographic variables, including age, race/ethnicity, and gender. By incorporating these demographic factors, the analysis allows us to explore whether cultural stress offers unique explanatory power beyond the influences of developmental stage and structural positioning. We assessed statistical significance in this study at the p < .05 level, as referenced in the works of Rubin and Babbie [20] and Thyer [21]. Through this methodical approach, we can gain a better understanding of how cultural and identity-related factors influence health outcomes within this demographic.
Demographic characteristics were calculated to summarize Descriptive statistics and the prevalence of cultural stress, identity factors, trauma exposure, and behavioral health needs. A multiple linear regression was then used to examine whether cultural stress and identity-related factors predicted the severity of behavioral health needs, while controlling for trauma exposure variables. The statistical significance was tested at the p < .05 level [10,20]. A bivariate analysis with simple linear regression identified variables associated with behavioral health needs. For multivariate analysis, multiple linear regression assessed the predictive power of intrapersonal and interpersonal variables on behavioral health needs [9,20].
Results
Descriptive Statistics
As presented in Table 1, the analytic sample (n = 230) comprised children and adolescents aged 6 to 18 years (M = 13.2, SD = 3.1), reflecting a developmentally diverse population typical of publicly funded behavioral health systems. Acknowledging this age range can inspire respect and trust among researchers and clinicians for the study's comprehensive scope.
The sample demonstrated significant racial and ethnic diversity, with nearly half identifying as Black or African American (46%) and approximately one-third identifying as Hispanic or Latinx (32%). Recognizing this diversity can foster respect and appreciation among researchers, clinicians, and policymakers for the varied backgrounds represented in the study, emphasizing the value of inclusive research.
The gender distribution reflected the typical overrepresentation of males in publicly funded behavioral health services, with 56% male. Females accounted for 39%, and 5% identified as gender-diverse, where data were available. Male youth showed higher externalizing and behavioral control needs, while female and gender-diverse youth reported more internalizing issues like anxiety and depression. Despite smaller numbers, gender-diverse youth experienced higher cultural stress and trauma, underscoring intersectional vulnerabilities within this group, which can motivate targeted research and practice efforts (see Table 1).
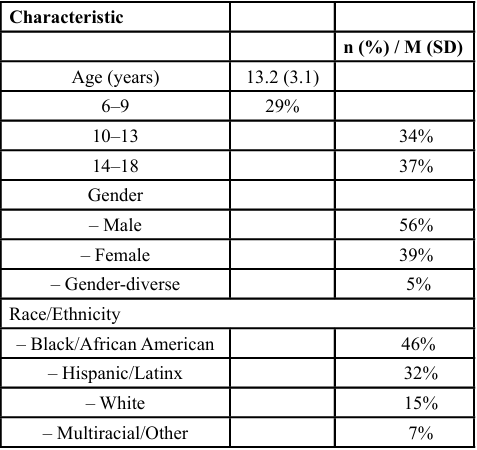
Table 1.
Regression Analysis Predicting Behavioral Health Need Severity
The results of the multiple linear regression analysis designed to predict behavioral health need severity are detailed in Table 2. The overall model was statistically significant, accounting for a considerable proportion of variance in behavioral health need severity (R² = .56, adjusted R² = .49, p < .001). This demonstrates the model's strong explanatory power, underscoring its relevance for stakeholders analyzing assessment data.
Cultural stress emerged as a strong and statistically significant predictor of behavioral health need severity (β = .38, p = .004), even when controlling for variables including trauma exposure, age, race/ ethnicity, and gender. This highlights the critical role of cultural stress in understanding youth behavioral health needs, emphasizing its importance beyond trauma exposure alone. Additionally, identity related stressors were significantly associated with increased severity (β = .27, p = .020), pointing to the relevance of identity challenges in this population.
Age showed a modest yet significant relationship with behavioral health need severity (β = .21, p = .040), underscoring the importance of demographic context. Including race/ethnicity and gender improved model fit, reinforcing the value of careful demographic considerations in understanding youth needs.
Trauma exposure did not retain statistical significance in the multivariate model (β = .12, p = .180) once cultural stress and identity factors were included. This highlights the importance of broadening assessment frameworks to include sociocultural and identity-based stressors, inspiring confidence in more holistic evaluation approaches.
In summary, the findings presented in Tables 1 and 2 indicate that while demographic characteristics provide crucial contextual information, cultural stress and identity-related factors are more closely associated with the severity of behavioral health needs among youth accessing publicly funded behavioral health services. The strength and consistency of these associations support the integration of culturally responsive indicators into standardized assessment and service planning processes (see Table 2).
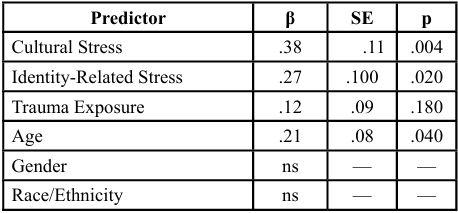
Table 2
Discussion
The findings from this study underscore the significant influence of cultural stress and identity-related factors on behavioral health outcomes among youth receiving public services. Although trauma exposure continues to be a crucial contextual element, the results indicate that cultural stress serves as a distinct and impactful contributor to the severity of behavioral health needs, aligning with the research conducted by Salas-Wright et al. [1]. Furthermore, these findings align with ecological and liberation-oriented frameworks that conceptualize youth distress as embedded within sociocultural and structural conditions rather than solely within individual pathology [22]. For child and adolescent social workers, this underscores the importance of assessment practices that explicitly attend to cultural stress and identity affirmation as components of ethical and effective care [1,22].
This scoping review identified a new factor associated with adolescents' use of Publicly Funded Care Systems (PFCS) and highlighted connections among various individual factors. These include sociodemographic variables, religiosity, self-reported depressive symptoms, parental monitoring and support, and stigma. These factors influence adolescents' utilization of publicly funded mental health services, reduce cultural stressors, and improve behavioral health outcomes among youth.
The findings build on prior research suggesting that a multidisciplinary, collaborative approach is essential to improving adolescents' engagement with mental health services, particularly publicly funded community services [23]. A comprehensive examination of the various factors influencing adolescent utilization of publicly funded mental health services, the reduction of cultural stressors, and the enhancement of behavioral health outcomes among youth is warranted for future studies [22,24].
Firstly, research should explore the overlap among these factors to leverage insights from one area (non-PFCS) to improve the impact of PFCS, and vice versa. Secondly, additional evidence is needed to quantify each factor's contribution to PFCS use. For instance, if self-reported depressive symptoms drive adolescents to use PFCS significantly more than parental monitoring and support, targeted outreach strategies could be developed for school nurses, administrators, social workers, and mental health practitioners.
Lastly, studies that examine specific factors, such as the effects of peer relationships, mental health literacy, and school-wide mental health initiatives on stigma, as well as school-community partnerships on student engagement or cultural influences on sociodemographic characteristics, could further enhance our understanding and improve PFCS usage among adolescents in need [14,25].
Implications for Child and Adolescent Social Work Practice
The CANS assessment offered a practical mechanism for integrating cultural context into clinical decision-making. Routine analysis of cultural stress indicators can inform individualized service planning, enhance therapeutic alliance, and support prevention-oriented interventions. Social workers must be equipped to recognize and respond to cultural stressors that exacerbate emotional and behavioral difficulties. Incorporating culturally responsive engagement, identity- affirming interventions, and advocacy-oriented practice are essential for reducing distress and promoting resilience among youth [1,2].
Moreover, findings on adolescents' perceived treatment needs can help practitioners effectively engage teenagers with unmet treatment needs in several important ways [26]. Firstly, adolescents experiencing externalizing disorders often do not recognize their need for treatment. Instead, they may seek help due to more apparent issues, such as family dynamics including conflict, cohesion, and overall functioning. Therefore, addressing family-related concerns is a promising strategy for motivational interventions to improve treatment readiness among adolescents. In essence, focusing on family relationships may serve as an effective initial step for gateway providers, such as parents and social workers, in encouraging teenagers to seek and participate in mental health services [1]. On the other hand, emphasizing symptoms may be less effective and could inadvertently discourage adolescents from starting the treatment process, as they often do not associate these symptoms with their need for care [17]. Additionally, it is important to note that adolescent males may necessitate additional support through gender- specific strategies from both gateway providers and therapists in acknowledging their need for treatment, as research suggests that females tend to report a higher perceived need for care [17,27].
Therapists and agencies serving this demographic may need to implement more intensive outreach strategies between client visits. Effective methods to enhance engagement with families include sending simple reminders to adult caregivers regarding upcoming sessions via telephone and through written correspondence [22]. Furthermore, direct communication with adolescents such as the dissemination of reminder text messages could help prevent attrition during the intake process. Agencies should explore alternative avenues for engaging this community, particularly where mental health needs are pronounced, and treatment participation remains low [28,29].
It is essential to train therapists to recognize and understand culturally specific barriers to behavioral health outcomes among youth using publicly funded care services, as well as diverse cultural perspectives on mental health care [25]. This training can improve their effectiveness in engaging families during the intake process. Many impoverished urban communities exhibit a degree of mistrust towards external providers, including mental health professionals [14]. Therefore, therapists' awareness of these issues is critical to effectively serving this population. Collaborative research initiatives involving community members and researchers have significant potential to address challenges such as fostering alliances, increasing the relevance of services, and overcoming barriers to treatment [25,30].
To enhance the quality of care, it is imperative to collect data directly from families to gain insight into their service preferences, reasons for disengagement in treatment, and evaluations of outcomes [1]. For this demographic, it may be more advantageous to allocate resources beyond the conventional treatment system. Understanding the most effective intervention points for impoverished urban communities, particularly concerning adolescents, warrants further exploration [22]. At the systems level, findings support investment in culturally responsive services and workforce training that emphasizes identity- informed assessment and intervention. Policymakers should consider leveraging aggregated CANS data to monitor disparities and guide equitable resource allocation [22,30].
Conclusion
The present study contributes to the expanding body of research regarding the impact of cultural stress and identity-related factors on the behavioral health needs of youth who access publicly funded care services [1]. In doing so, it addresses several critical dimensions of this issue. Primarily, it employs a novel methodology that can be replicated in future research. In the absence of randomized controlled trials, propensity score matching (PSM) represents a robust and intuitive approach to mitigate the biases often encountered in observational studies [27]. Future research employing PSM may build upon the findings of this investigation to accurately estimate statistical power. Secondly, the study elucidates how service systems that employ the Child and Adolescent Needs and Strengths (CANS) assessment can optimize its application. Instead of focusing exclusively on total scores and net changes, it is advantageous to examine both the quantity and the patterns of items resolved, as well as those that arose from baseline to follow-up [27].
Lastly, although the estimated effects of cultural stress and identity related factors on the behavioral health needs of youth accessing publicly funded care services in this study approached statistical significance, the observed differences between groups had a moderate effect size [2]. This effect size is considered clinically meaningful according to established conventions for interpreting CANS results. Notably, cultural stress and identity-related factors are significant predictors of behavioral health needs among youth receiving services. Integrating these dimensions into assessment, intervention, and policy is essential for advancing culturally responsive child and adolescent social work practice [1].
Competing Interest:
The authors declare that they have no competing interests.
References
Salas-Wright, C. P., Maldonado-Molina, M. M., Brown, E. C., et al. (2021). Cultural stress theory in the context of family crisis migration: Implications for behavioral health with illustrations from the Adelante Boricua Study. American Journal of Criminal Justice, 46, 586–608. View
Schwartz, S. J., Waterman, A. S., Cobb, C. L., Cano, M. Á., Scaramutti, C., Meca, A., Ozer, S., Ward, C., Puente-Durán, S., Lorenzo-Blanco, E. I., Unger, J. B., Duque, M. C., Vos, S. R., Zeledon, I., & Garcia, M. F. (2022). Cultural stress, daily well- being, and internalizing and externalizing symptoms among Hispanic college students. Journal of Counseling Psychology, 69(4), 416. View
Lyons, J. S., Weiner, D. A., & Lyons, M. B. (2014). Measurement as communication in outcomes management: The child and adolescent needs and strengths (CANS). In the use of Routledge. View
Yan, J., Sim, L., Song, J., Chen, S., & Kim, S. Y. (2022). Reconsidering the “Acculturation Gap”: Mother-adolescent cultural adaptation mis/matches and positive psychosocial outcomes among Mexican-Origin families. Journal of Youth and Adolescence, 51(7), 1409. View
Johnson, T., & Shamroukh, S. (2024). Predictive modeling of burnout based on organizational culture perceptions among health systems employees: A comparative study using correlation, decision tree, and Bayesian analyses. Scientific Reports, 14, 6083. View
Arenás, E. (2021). The human right to health : solidarity in the era of healthcare commercialization. Edward Elgar Publishing. View
Glover, J. (2019). The Role of Physicians in the Allocation of Health Care: Some Justice Better than None? Kennedy Inst Ethics J, 29(1), 1-31. View
Faulkner, S. S., & Faulkner, C. A. (2023). Research Methods for Social Workers: A Practice-Based Approach (4th ed.). Oxford University Press. View
Field, A. (2023). Discovering Statistics Using IBM SPSS Statistics (6th ed.). SAGE Publications. View
Weinbach, R. W., & Grinnell, R. M. (2019). Statistics for Social Workers (10th ed.). Pearson.
Persson, E., Andersson, D., Back, L., Davidson, T., Johannisson, E., & Tinghög G. (2018). Discrepancy between Health Care Rationing at the Bedside and Policy Level. Medical Decision Making, 38(7), 881-887. View
Lyons, J. S., Woltman, H., Martinovich, Z., & Hancock, B. (2009). An outcomes perspective of the role of residential treatment in the system of care. Residential Treatment For Children & Youth, 26(2), 71–91. View
Miller, S. A., Leon, S. C., & Lyons, J. S. (2007, May). The Child and Adolescent Needs and Strengths Scale: Factor analytic investigations. Poster presented at the meeting of the Midwestern Psychological Association, Chicago, IL.
McCance-Katz, Elinore, and Calder Lynch (2019). “Guidance to States and School Systems on Addressing Mental Health and Substance Use Issues in Schools.” Rockville, MD: Substance Abuse and Mental Health Services Administration and the Centers for Medicare & Medicaid Services. View
Feiss, R., Dolinger, S. B., Merritt, M., Reiche, E., Martin, K., Yanes, J. A., Thomas, C. M., & Pangelinan, M. (2019). A systematic review and meta-analysis of school-based stress, anxiety, and depression prevention programs for adolescents. Journal of Youth and Adolescence, 48(9), 1668–1685. View
Alhassan, A., Rasheed, S., Raza, A. A., Murtaza, B., Mujeeb, A., & Mansoor, A. I. (2025). Driving and sustaining trauma informed organizational change: The role of healthcare leadership. Health Sciences Review, 16, 100236. View
Ballout, S. (2025). Trauma, mental health workforce shortages, and health equity: A crisis in public health. International Journal of Environmental Research and Public Health, 22(4), 620. View
Chavez-Dueñas, N. Y., Adames, H. Y., Perez-Chavez, J. G., & Salas, S. P. (2019). Healing ethno-racial trauma in latinx immigrant communities: Cultivating hope, resistance, and action. American Psychologist, 74(1), 49-62. View
Texas Health and Human Services Commission. (2024a). Behavioral health services: Trauma-informed and person centered care guidelines. View
Rubin, A., & Babbie, E. R. (2025). Research Methods for Social Work (10th ed.). Cengage Learning. View
Thyer, B. A. (2022). The importance of statistical literacy for social work practitioners. Journal of Evidence-Based Social Work, 19 (1), 1-15.
Caperon, L., Saville, F., & Ahern, S. (2022). Developing a socio-ecological model for community engagement in a health programme in an underserved urban area. PloS one,17(9), e0275092. View
Colizzi, M., Lasalvia, A., & Ruggeri, M. (2020). Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? International Journal of Mental Health Systems, 14(1), 23. View
Larsen, E. H., Mellblom, A. V., Ruud, E., Wahl, A. K., & Lie, H. C. (2022). Prepared for survivorship? Multidisciplinary healthcare professionals' experiences with adolescents’ transition off cancer treatment: A focus group study. European Journal of Oncology Nursing, 58, 102150. View
London, A. S. (2021). Depression and mental health service use among 12–17 year old U.S. adolescents: Associations with current parental and sibling military service. SSM - Population Health, 16, 100920. View
Lardner, M. D. (2015). Are Restrictiveness of Care Decisions Based on Youth Level of Need? A Multilevel Model Analysis of Placement Levels Using the Child and Adolescent Needs and Strengths Assessment. Residential Treatment for Children and Youth, 32:195–207 View
Wen, W., Chen, S., Hazen-Swann, N., Lorenzo-Blanco, E. I., Shen, Y., & Kim, S. Y. (2022). Cultural stressors, internalizing symptoms, and parent–child alienation among Mexican origin adolescents. Family Relations, 71(5), 1977. View
Centers for Medicare & Medicaid Services. (2022). Person centered planning and service delivery in Medicaid home and community-based services. U.S. Department of Health and Human Services. View
Graves, J. M., Abshire, D. A., Mackelprang, J. L., Dilley, J. A., Amiri, S., Chacon, C. M., & Mason, A. (2023). Geographic disparities in the availability of mental health services in U.S. public schools. American Journal of Preventive Medicine, 64(1), 1–8. View
Murthy, V. (2021). Protecting youth mental health: The U.S. Surgeon General’s Advisory. Office of the Surgeon General. View