
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy Volume 4 (2026), Article ID: JSWWP-187
https://doi.org/10.33790/jswwp1100187Research Article
Strengthening Professional and Community Capacity to Respond to Gender Based Violence in Eswatini: A Qualitative Intervention Study
Thabsile Lukhele
School of Social Work, Stephen F. Austin State University, 1936 North St, Nacogdoches, TX 75965, United States.
Corresponding Author Details: Thabsile Lukhele, School of Social Work, Stephen F. Austin State University, 1936 North St, Nacogdoches, TX 75965, United States.
Received date: 14th February, 2026
Accepted date: 19th March, 2026
Published date: 21st March, 2026
Citation: Lukhele, T., (2026). Strengthening Professional and Community Capacity to Respond to Gender-Based Violence in Eswatini: A Qualitative Intervention Study. J Soci Work Welf Policy, 4(1): 187.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Gender-based violence (GBV) remains a pervasive social welfare and public health concern in Eswatini, shaped by patriarchal family structures, cultural expectations, and women’s socio-economic dependence. These dynamics limit survivors’ agency and reinforce norms that discourage disclosure and help-seeking. This study examined a culturally responsive training intervention designed to strengthen professional and community capacity to prevent and respond to GBV in Eswatini. Guided by empowerment and systems theories, the intervention sought to enhance participants’ understanding of gender power relations, trauma-informed practice, and survivor- centered engagement. The qualitative intervention involved seven participants, including social workers, a psychologist/counselor, a traditional leader, and a church leader. A qualitative pre–post design was used to explore shifts in participants’ perceptions and practices. Data were collected through open-ended questionnaires administered before and after the training and analyzed using thematic analysis. Findings indicated increased recognition of GBV as embedded in patriarchal family power dynamics, deeper understanding of the long-term impacts of trauma on survivors, and greater confidence in survivor-centered and community-based responses. Although exploratory due to the small sample size, the findings highlight the potential of culturally grounded training to strengthen frontline responses to GBV. The study contributes to ongoing discussions on community-engaged and culturally responsive approaches to GBV prevention and response in resource-constrained contexts.
Keywords: Gender-based Violence, Eswatini, Trauma-informed Practice, Survivor-centered Approach, Cultural Responsiveness, Community Advocacy
Background of Study
Gender-based violence (GBV) remains a major global public health and human rights concern with significant physical, psychological, social, and economic consequences for survivors. It is widely understood as rooted in patriarchal systems and sociocultural structures that reinforce unequal power relations between men and women [1,2]. These inequalities restrict women’s autonomy and contribute to the normalization of violence within intimate relationships and communities. Survivors frequently experience long-term mental health effects, including fear, anxiety, depression, and post-traumatic stress, which can limit their participation in social and economic life [3,4]. As a result, GBV is increasingly recognized as both a social justice issue and a barrier to gender equality and sustainable development.
In Eswatini, GBV remains widespread and is shaped by cultural, social, and religious norms that influence expectations surrounding marriage, gender roles, and authority within families and communities. National data illustrate the magnitude of the problem. For instance, the Eswatini Violence Against Children and Youth Survey reports that approximately one in three women experiences sexual violence before the age of 18, while intimate partner violence affects many women during their lifetime. Cultural expectations that emphasize women’s endurance and male authority within households may discourage survivors from reporting abuse and contribute to the normalization or minimization of violence [5]. Although the government has introduced legal and policy frameworks such as the Sexual Offences and Domestic Violence (SODV) Act of 2018 and national gender policies, deeply entrenched patriarchal norms continue to limit the effectiveness of these interventions [6,7].
Within many communities, traditional and faith leaders play a central role in shaping attitudes toward gender relations, family dynamics, and conflict resolution. Their authority extends beyond religious or customary matters and often influences how cases of violence are interpreted and addressed. Despite their influence, these leaders are frequently underrepresented in formal GBV prevention and response initiatives [8]. Limited engagement of community leadership may weaken efforts to transform harmful gender norms and strengthen support systems for survivors.
At the same time, frontline professionals such as social workers, counsellors, psychologists, and community development practitioners often serve as the first point of contact for survivors. They play a critical role in identifying abuse, providing trauma-informed care, facilitating referrals, and supporting survivors through legal and social processes. However, many practitioners operate with limited specialized training, constrained resources, and insufficient guidance on implementing survivor-centered and culturally responsive approaches [9,10]. Strengthening professional competencies through targeted training and capacity-building initiatives is therefore essential for improving service delivery and coordination across sectors.
Research increasingly highlights the importance of multisectoral approaches that integrate legal frameworks, professional capacity building, and community engagement to address GBV effectively [11,12]. Participatory training initiatives that include both professional service providers and community leaders have shown promise in strengthening knowledge, shifting attitudes, and improving collaborative responses to violence [10,13]. However, in Eswatini, existing GBV research has largely focused on prevalence, risk factors, and legal frameworks such as the implementation of the Sexual Offences and Domestic Violence Act. Limited empirical attention has been given to how frontline professionals and community leaders conceptualize GBV within their sociocultural context or how training interventions may influence their knowledge, attitudes, and practices [14].
Addressing this gap is particularly important given the influential role that both professional service providers and community leaders play in shaping responses to violence. Strengthening their capacity has the potential to improve trauma-informed support, promote survivor-centered engagement, and challenge harmful norms that perpetuate violence within communities.
In response to these challenges, this study implemented a culturally responsive training intervention aimed at strengthening the knowledge, attitudes, and perceived competencies of professional service providers and community leaders in responding to gender based violence in Eswatini. The intervention promoted trauma informed, survivor-centered, and culturally grounded approaches while encouraging community leaders to challenge harmful sociocultural practices and support prevention efforts. By examining participants’ perspectives before and after the training, the study contributes context-specific evidence on how capacity-building initiatives can strengthen professional and community responses to gender-based violence.
Literature Review
Socio-cultural norms
Gender-based violence (GBV) in Eswatini is reinforced by deeply rooted sociocultural norms that shape gender roles and power relations. Women are socialized to be obedient and enduring, while men are positioned as household authorities, legitimizing control and normalizing violence as a form of discipline [5,15,16]. Cultural expectations, such as Tibi Tendlu, the belief that family matters must remain private, promote secrecy, suppress disclosure, and reinforce women’s subordination [1,17]. Marriage practices involving lobola further pressure women to remain in abusive unions due to stigma and economic implications for families, framing women as belonging to the husband’s household [18-21].
Stigma, shame, and victim blaming
Stigma, shame, and victim-blaming further deter survivors from seeking help. Women often fear being accused of provoking violence or destabilizing the family, making social judgment a strong barrier to reporting [22,23]. Regional studies show that victim-blaming erodes confidence in formal systems and delays help-seeking [24,25]. Limited awareness of rights also weakens access to services. Although the Sexual Offences and Domestic Violence (SODV) Act provides protection, many survivors and community members lack understanding of legal provisions, including marital rape and emotional abuse [22,26].
Patriarchal biases
Patriarchal biases within formal and traditional justice systems create institutional barriers. Police and traditional authorities often encourage reconciliation rather than legal action, treating GBV as a private matter and contributing to secondary victimization and impunity [4,18].
Structural challenges
Structural challenges, including limited shelters, strained social services, and rural inaccessibility, restrict survivors’ ability to obtain safety and support [8,27]. Weak multi-sector coordination and fragmented referral systems further hinder comprehensive care, mirroring global evidence on the need for integrated responses [11,28].
Socioeconomic dependence
Socioeconomic dependence remains a critical barrier, as high unemployment and poverty reduce women’s capacity to leave abusive relationships or pursue legal remedies [29]. Vulnerable groups, including young women, women with disabilities, and rural populations, face compounded discrimination, inaccessible services, and a lack of privacy [18].
Finally, mistrust of institutions stemming from slow processes, limited enforcement, and perceived impunity discourages reporting and perpetuates silence [22,30].
Strengthening Professional and Community Capacity Through Evidence-Based GBV Training
Combating gender-based violence (GBV) requires coordinated action across both professional and community sectors. The United Nations Population Fund [31] highlights that violence against women persists where survivor support systems are fragmented or under- resourced. In Eswatini, many women continue to experience limited decision-making autonomy in areas such as healthcare and finances, reflecting enduring gender inequalities within households [32].
Traditional leaders, including chiefs, church leaders, and community elders, play a central role as custodians of cultural norms. Their influence positions them to either reinforce patriarchal expectations or act as agents of cultural transformation [33]. As such, effective GBV interventions in Eswatini must engage these leaders to shift harmful norms and promote protective, community-based responses grounded in local cultural contexts.
Recent scholarship emphasizes the importance of behavior change initiatives, men’s engagement strategies, and culturally grounded educational programs to challenge the normalization of violence [5,35]. However, strengthening legal frameworks alone is insufficient. Sustainable change requires improved collaboration among service providers, the adoption of survivor-centered professional practices, and ongoing community dialogue that confronts harmful gender norms [14].
Given the complexity of GBV as both a social welfare and public health issue, there is a critical need for continuous and multidisciplinary training that strengthens the professional and relational competencies of those responding to survivors. In this context, training-based interventions have emerged as a key strategy for enhancing the capacity of both frontline professionals and community leaders.
Despite growing recognition of GBV as a major concern in Eswatini, limited research has examined the effectiveness of culturally grounded training interventions aimed at strengthening response capacity across these groups. This study is informed by evidence-based practice and draws on international interventions demonstrating the value of structured GBV training. For example, a study conducted in Pakistan implemented a Life Skills-Based Training program to strengthen healthcare providers’ responses to GBV, improving their ability to identify, respond to, and refer cases while fostering collaboration with community stakeholders [13].
Similarly, research conducted in Tanzania provides further support for the effectiveness of targeted GBV training programs among community-based practitioners and local leaders [10]. These interventions have been associated with improved understanding of GBV and enhanced responsiveness to survivors, although persistent barriers such as stigma, limited-service availability, and legal constraints continue to affect help-seeking. These challenges closely mirror those observed in Eswatini, underscoring the importance of contextually relevant interventions.
Collectively, existing evidence highlights the potential of culturally contextualized, participatory training approaches to strengthen GBV response systems. Such interventions have been associated with improvements in individual competencies as well as enhanced inter- sectoral collaboration and community engagement, both of which are essential for sustainable prevention and response efforts. However, there remains a need for context-specific evidence from Eswatini to assess how such interventions influence knowledge, attitudes, and practice among both professionals and community leaders.
Building on this gap, the present study examined the impact of a culturally responsive GBV training intervention implemented in Eswatini using a qualitative pre–post design. The following research questions guided the study:
1. How do professionals and community leaders understand gender-based violence in Eswatini, and what beliefs, cultural norms, and contextual factors shape these understandings?
2. How does the GBV training intervention influence participants’ knowledge, attitudes, and perceptions regarding GBV, trauma, family dynamics, and survivor-centered practice?
3. How do participants conceptualize their roles and responsibilities in preventing and responding to GBV before and after the training?
4. In what ways does the training enhance participants’ confidence, skills, and perceived capacity to support survivors and challenge harmful norms within their professional and community contexts?
Theoretical Framework
This study is guided by Systems Theory, Empowerment Theory, and the Strengths-Based Approach, which together provide a complementary framework for understanding and responding to gender-based violence (GBV) in Eswatini. Systems Theory situates GBV within interconnected social structures, including family dynamics, cultural norms, religious institutions, and legal systems, highlighting the need for coordinated, multisectoral responses. Empowerment Theory emphasizes strengthening awareness of rights, agency, and leadership capacity among survivors, professionals, and community leaders to challenge harmful norms and support survivor- centered interventions. The Strengths-Based Approach complements these perspectives by recognizing the resilience, cultural resources, and community assets that individuals and communities possess, promoting responses to GBV that foster dignity, healing, and collective capacity.
Systems Theory
Systems Theory provides a holistic perspective for understanding GBV as a multidimensional issue shaped by interacting individual, relational, community, and societal factors such as gender inequality, cultural norms, economic dependence, and institutional responses [35]. This perspective emphasizes that violence is embedded within broader social systems, including families, cultural traditions, religious institutions, and service networks, and therefore requires coordinated responses across sectors, including social services, healthcare, law enforcement, and community leadership [36-38].
Empowerment Theory
Empowerment Theory focuses on strengthening individuals’ and communities’ capacity to understand and act on their rights, promoting agency, autonomy, and self-determination [39,40]. In the context of GBV, empowerment supports survivor-centered practice by recognizing survivors’ strengths and encouraging professionals and community leaders to promote advocacy, ethical engagement, and social change [41,42]. Empowerment operates at individual, relational, and collective levels, supporting both personal recovery and broader transformation of harmful gender norms [43,44].
Strengths-Based Approach
The Strengths-Based Approach complements systems and empowerment perspectives by focusing on the resilience, capacities, and resources of survivors and communities. Rather than emphasizing deficits, this perspective highlights coping strategies, social networks, and cultural assets as foundations for healing and change [45]. In GBV interventions, strengths-based practice promotes dignity, hope, and community support while reinforcing the capacity of survivors and communities to respond to violence. Research suggests that empowerment and strengths perspectives provide strong theoretical grounding for social work practice [46-48], while systems theory further emphasizes the interconnected structures that shape GBV and the need for coordinated, multi-level responses.
The theoretical perspectives outlined above informed the design and structure of the training intervention implemented in this study. Systems theory guided the emphasis on multisectoral collaboration and the involvement of both professional service providers and community leaders in responding to GBV. Empowerment theory informed the focus on strengthening participants’ knowledge, leadership capacity, and ability to challenge harmful gender norms. The strengths-based approach shaped the training’s emphasis on recognizing survivor resilience, community assets, and culturally grounded resources for prevention and response. The key components of the training intervention and their theoretical grounding are summarized in Table 1.
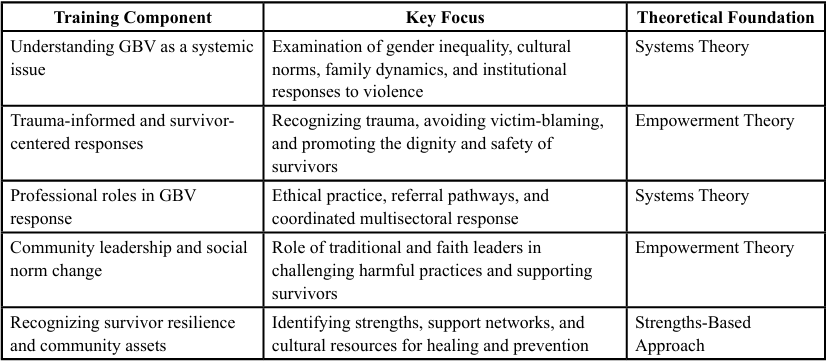
Table 1. Training Intervention and Theoretical Foundations
Methodology
Research Design
This study employed a qualitative intervention research design, guided by the participatory model of Fraser and Galinsky [49]. Intervention research emphasizes the systematic development, implementation, and evaluation of programs designed to address identified social problems while engaging practitioners and community members as co-creators of change. In this study, the design followed the cyclical steps of problem identification, intervention design, implementation, formative and summative evaluation, and refinement. A pre- and post-training qualitative assessment was conducted to explore shifts in participants’ knowledge, attitudes, and perceived competencies in addressing gender-based violence (GBV).
The design was grounded in the principles of participatory action and empowerment-based learning, ensuring that participants were not passive recipients of training but active contributors to its development and reflection. This approach allowed the study to capture rich, contextual insights about how cultural, religious, and systemic factors influence professional and community responses to GBV in Eswatini.
Sampling and Sampling Method
Participants were selected using purposive sampling to ensure the inclusion of individuals with direct experience responding to gender-based violence (GBV) against women. Purposive sampling was appropriate because it allowed the selection of participants who possessed the knowledge and practical experience necessary to provide rich, contextually grounded insights into GBV responses [50].
Eligible participants were required to be 18 years or older, actively working or serving in Eswatini at the time of the study, and have direct professional or community-based involvement with women experiencing GBV. Participants were required to demonstrate practical experience in providing support, guidance, intervention, or decision-making related to GBV cases and be willing to participate in the training intervention and evaluation activities. Individuals were excluded if they had no direct involvement in GBV-related work, held purely administrative roles without survivor interaction, were unable to commit to the training and evaluation process, or declined to provide informed consent.
A total of nine participants attended the training intervention, including five professionals (four social workers and one counselor) and four community leaders (traditional and church leaders). However, two participants did not complete the post-training evaluation and, therefore, were excluded from the analysis. The final sample used for the study consisted of seven participants, including four social workers, one counselor, one traditional leader, and one church leader. Participants were represented by identification codes in the reporting of findings to protect their identities.
Data Collection Methods
Data were collected using pre- and post-training qualitative surveys consisting of open-ended questions that explored participants’ understanding of gender-based violence (GBV), family dynamics, trauma impacts, and the roles of professionals and community leaders in prevention and response. The survey instruments were adapted from GBV training assessment tools developed by the United Nations Population Fund (UNFPA) and the World Health Organization (WHO) and contextualized for the Eswatini setting.
Training Intervention
The study implemented a structured training intervention designed to strengthen participants’ understanding of gender-based violence (GBV) and enhance their capacity to respond effectively within their professional and community roles. The training emphasized trauma-informed care, survivor-centered communication, and culturally grounded approaches to GBV prevention and response. Attention was given to recognizing the psychological impact of violence, promoting respectful and non-judgmental engagement with survivors, and strengthening referral and support mechanisms. In addition, the intervention highlighted the influential role of religious and traditional leaders in challenging harmful sociocultural norms, fostering community dialogue, and supporting survivor protection. Intervention fidelity was supported through a structured facilitation guide and delivery by the same primary facilitator. Participant engagement was monitored through discussions and role-plays, while field notes documented session flow and minor contextual adaptations. The training consisted of two sessions tailored to different participant groups, as summarized in Table 2.
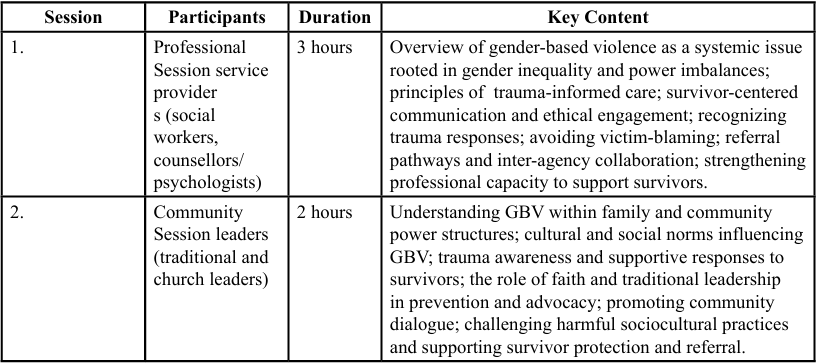
Table 2. Overview of Gender-Based Violence Training Intervention
Data Analysis
Data were analyzed using thematic content analysis [51]. This analytic approach involves identifying, organizing, and interpreting patterns of meaning within qualitative data to understand participants' shared and divergent experiences. The process followed six phases: (1) familiarization with the data, (2) generation of initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the final narrative report [52].
Thematic content analysis was chosen for its flexibility and ability to highlight both common patterns and context-specific insights. Pre- and post-training responses were compared to identify changes in knowledge, attitudes, and confidence, as well as emerging conceptual shifts regarding the roles of family dynamics, trauma, and leadership in GBV prevention. Representative quotations from participants were used to illustrate key findings, ensuring authenticity and transparency in interpretation.
The researcher served as the training facilitator and was therefore positioned as both practitioner and evaluator. To minimize bias, participants completed written questionnaires anonymously, and reflexive memos were used during analysis to examine assumptions and interpretations.
Trustworthiness
To enhance trustworthiness, several strategies were employed. Credibility was supported through systematic coding and repeated review of pre- and post-training responses.
An audit trail documenting coding decisions and theme development was maintained throughout the analytic process.
Reflexive memos were used to monitor potential researcher bias, given the researcher’s involvement in the training.
Transferability was supported through a thick description of the intervention context and participant roles.
Dependability and confirmability were strengthened by maintaining detailed analytic records and using verbatim participant quotations to illustrate themes.
Ethical Considerations
The study adhered to established ethical standards in social work research. Informed consent was obtained from all participants before participation. Participants were informed of their right to withdraw at any time without penalty and assured of confidentiality and anonymity. To protect participants, identifying details were omitted from all transcripts and reports. Given the sensitivity of GBV-related discussions, special attention was paid to emotional safety during data collection. Participants were encouraged to share only information they were comfortable disclosing, and psychological support or referrals were made available where needed. Ethical clearance was obtained from the Stephen F. Austin State University Institutional Review Board (IRB) before data collection.
Findings
Demographics:
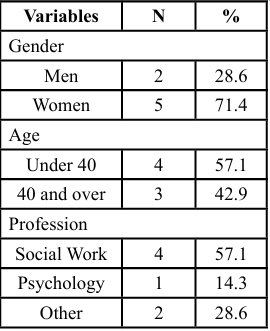
Table 3. Participants’ Demographic Characteristics
The sample comprised seven participants, the majority of whom were women (71.4%, n = 5). Participants were relatively evenly distributed by age, with 57.1% (n = 4) under 40 years and 42.9% (n = 3) aged 40 years and above. Social workers constituted the largest professional group (57.1%, n = 4), followed by one psychologist (14.3%, n = 1), with the remaining participants (28.6%, n = 2) representing other professional or community leadership roles.
Analysis of pre- and post-training reflections identified six themes reflecting shifts in participants’ knowledge, attitudes, and perceived competencies in responding to gender-based violence. Participants are identified using codes (P1–P7) to protect confidentiality.
Theme 1: Recognizing GBV as Rooted in Family Power Dynamics
Pre-training responses indicated that several participants initially understood GBV primarily because of interpersonal conflict or communication breakdown between partners. Participants often framed violence as emerging from disagreements within relationships rather than from broader structural inequalities.
For example, one participant noted:
“Sometimes abuse happens because couples cannot communicate properly or solve their problems.” (P2, pre-training)
Another participant similarly reflected:
“I believed violence mostly comes from arguments that escalate when partners cannot resolve their disagreements.” (P5, pre-training)
Following the training, participants demonstrated a broader understanding of GBV as embedded within patriarchal family structures and gendered power relations. Participants increasingly recognized how cultural expectations around family unity and women’s endurance may discourage survivors from reporting abuse.
One participant explained:
“Before, I thought abuse happened because partners failed to communicate. Now I understand it is linked to how power is arranged in families, where women are expected to endure and remain silent.” (P3, post-training)
Another participant added:
“Family expectations can make women feel they must stay quiet to protect the marriage, even when they are suffering.” (P6, post training)
This shift reflects principles of systems theory, which emphasizes how family structures, cultural norms, and community expectations interact to shape patterns of violence and responses to abuse. Similar findings have been reported in studies highlighting the role of patriarchal household dynamics in sustaining gender-based violence [2].
Theme 2: Deeper Understanding of Trauma Impacts and Survivor Needs
Pre-training reflections suggested that some participants initially viewed recovery from violence as requiring relatively quick disclosure or resolution of abuse. Trauma was sometimes understood as a short- term emotional response rather than a complex and ongoing process.
One participant stated:
“I believed survivors should speak about what happened so that they can move on and start healing.” (P1, pre-training)
Another participant similarly noted:
“Sometimes survivors delay reporting, but if they talk about it early, they can recover faster.” (P4, pre-training)
Post-training responses indicated a deeper understanding of trauma and its long-term effects on survivors. Participants emphasized the importance of patience, empathy, and allowing survivors to determine their own pace of healing.
One participant explained:
“I now see that trauma does not end when the violence stops. Survivors need patience, empathy, and space to heal at their own pace. (P2, post-training)
Another participant reflected:
“The training helped me understand that trauma can affect someone for a long time, and survivors need support rather than pressure to speak.” (P7, post-training)
Participants’ increased recognition of the long-term psychological impacts of violence reflects growing alignment with trauma-informed and survivor-centered approaches. From an empowerment perspective, acknowledging survivors’ experiences and supporting their autonomy are essential components of effective intervention.
Theme 3: Repositioning Traditional and Religious Leaders as Agents of Change
Before the training, some community leaders described their roles primarily in terms of maintaining harmony within families and communities rather than directly addressing violence.
One participant explained:
“Our role as leaders is usually to help families reconcile and maintain peace.” (P6, pre-training)
Another participant similarly noted:
“Sometimes leaders try to resolve conflict quietly so that the family can remain united.” (P7, pre-training)
After the training, several participants described a broader understanding of leadership roles in preventing and responding to GBV. Participants increasingly recognized that traditional and religious leaders could influence community attitudes and challenge harmful norms.
One participant stated:
“Our leaders shape how the community thinks. If they speak openly against GBV, people will listen, and behavior can change. (P6, post training)
Another participant reflected:
“As leaders, we must also speak against practices that harm women and encourage people to seek help.” (P7, post-training)
These reflections highlight increased awareness of the role of community leadership in shaping social norms and promoting collective responses to GBV.
Theme 4: Critical Engagement with Cultural Practices such as Lobola
Pre-training responses indicated that participants often viewed cultural practices such as lobola (bride price) primarily in positive cultural terms, with limited reflection on how such practices might influence gendered power dynamics.
One participant explained:
“Lobola is an important tradition that shows respect between families.” (P4, pre-training)
Another participant noted:
“It is part of our culture and helps unite families.” (P5, pre-training)
Following the training, participants demonstrated a more critical yet culturally respectful perspective on such practices. Participants acknowledged the cultural significance of lobola while also recognizing how it may reinforce expectations of women’s endurance in abusive relationships.
One participant reflected:
“I still value lobola, but I now see how it can make men feel entitled and make women feel they must stay, even when abused.” (P3, post training)
Another participant added:
“Some cultural expectations can make it harder for women to leave abusive relationships.” (P1, post-training)
These reflections suggest that participants began to critically engage with cultural practices while maintaining respect for cultural traditions, demonstrating increased awareness of how social norms interact with gender power dynamics.
Theme 5: Strengthened Ethical and Confidentiality Awareness
Pre-training reflections indicated that participants generally recognized the importance of confidentiality but often framed it as a procedural requirement rather than a key component of survivor protection.
One participant stated:
“Confidentiality is important because we must follow professional rules.” (P2, pre-training)
Another participant similarly noted:
“We should keep information private because it is part of ethical practice.” (P4, pre-training)
Post-training responses demonstrated a deeper understanding of confidentiality as essential for protecting survivor dignity and safety. One participant explained:
“I learned that confidentiality is not just a rule. It protects the survivor’s dignity and safety.” (P5, post-training) Another participant reflected:
“We must always ask consent before sharing someone’s story because it belongs to them.” (P3, post-training)
These reflections suggest increased awareness of ethical responsibilities in GBV work and a stronger commitment to survivor centered professional practice.
Theme 6: Increased Confidence in Advocacy and Community Dialogue
Before the training, some participants expressed uncertainty about how to address harmful social norms or intervene in community discussions about violence.
One participant stated:
“Sometimes it is difficult to speak against cultural beliefs because people may not accept it.” (P1, pre-training)
Another participant noted:
“I was not always sure how to challenge comments that normalize abuse.” (P4, pre-training)
After the training, several participants reported increased confidence in initiating conversations about GBV and promoting community awareness.
One participant shared:
“I feel more confident speaking up when I hear people normalize abuse. I can guide the conversation toward awareness.” (P4, post training)
Another participant explained:
“Now I feel better prepared to raise awareness and encourage people to support survivors.” (P6, post-training)
Participants described engaging in awareness-raising, supporting safe reporting pathways, and collaborating with community leaders as important advocacy strategies. These reflections suggest that the training strengthened participants’ confidence and capacity to promote dialogue and community-level change.
Across themes, participants demonstrated shifts in knowledge, attitudes, and perceived roles in addressing gender-based violence. These changes reflect the combined influence of systems thinking, which emphasizes the role of family, cultural, and institutional structures in shaping GBV, and empowerment processes, which strengthen participants’ capacity to advocate for survivor-centered responses and community-level change.
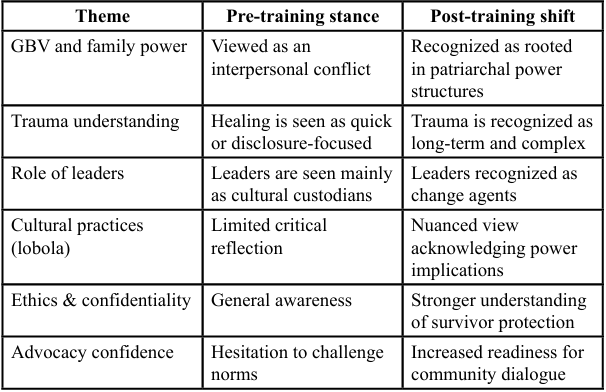
Table 4. Summary table
Discussion
This study examined how a culturally responsive training intervention influenced the capacity of professionals and community leaders in Eswatini to prevent and respond to gender-based violence (GBV). The findings suggest that targeted training can shift participants’ understanding of GBV from an interpersonal issue to a broader structural and community concern. Participants demonstrated increased awareness of patriarchal family power dynamics, deeper understanding of the long-term impacts of trauma on survivors, and greater confidence in survivor-centered engagement. These findings support the relevance of systems theory in understanding how family structures, cultural norms, and community institutions shape responses to violence, while also reflecting principles of empowerment theory that emphasize strengthening individual and community capacity to challenge inequality and support survivors.
Participants developed a more nuanced understanding of GBV as embedded within structural power relations rather than isolated interpersonal conflict. This shift from individualized explanations of abuse toward recognizing broader socio-cultural systems is consistent with feminist and socio-ecological perspectives on violence [11]. Such understanding is essential for addressing the underlying norms and power imbalances that sustain gender inequality.
The training also strengthened participants’ awareness of trauma and its prolonged psychological, emotional, and relational effects. Participants emphasized the importance of empathy, safety, confidentiality, and patience when supporting survivors, reflecting greater alignment with trauma-informed and survivor-centered practices. These approaches are widely recognized as critical for effective GBV responses, as dismissive or judgmental reactions from professionals can discourage help-seeking and reinforce silence [29].
Another important finding was the repositioning of traditional and religious leaders as potential agents of change in addressing harmful gender norms. In the Eswatini context, where cultural and religious leaders hold significant social authority, their engagement can influence community attitudes and promote dialogue around gender equality and violence prevention. Participants increasingly recognized the potential for these leaders to challenge harmful interpretations of cultural practices and encourage more equitable perspectives within communities.
The training also appeared to strengthen participants’ advocacy orientation, shifting their focus from individual case responses to broader community engagement and prevention. Participants highlighted the importance of involving families, community members, and institutions in addressing GBV, reflecting a systems-oriented understanding of prevention. However, sustaining such change requires ongoing training, mentorship, and coordinated collaboration across sectors, including social services, health systems, educational institutions, religious organizations, and traditional leadership structures.
Overall, the findings highlight the value of culturally responsive, dialogue-based training approaches that address both knowledge and belief systems. While the small sample size limits generalizability, the study provides exploratory insight into how targeted capacity- building initiatives can contribute to strengthening community and professional responses to GBV. Future research should expand the intervention to larger and more diverse groups, incorporate longitudinal follow-up, and examine longer-term behavioral and institutional outcomes. Continued engagement with traditional and religious leaders will remain essential for promoting sustainable, community-driven change in GBV prevention and response.
Implications of the Findings
Implications for Research
The findings are consistent with existing GBV research, highlighting the role of social and institutional systems in shaping responses to violence against women. This study extends the literature by applying an intervention research approach in Eswatini and by including both professionals and community leaders. Future research should examine the sustainability of empowerment-oriented interventions through longitudinal and multi-site studies that assess system-level change over time.
Implications for Theory
The findings reinforce the relevance of socio-ecological theoretical frameworks in understanding GBV in cultural contexts where patriarchal norms shape identity, family roles, and community authority. The study demonstrates that shifting beliefs about gender, power, and cultural practices requires engaging actors who hold moral legitimacy within the community. The intervention contributes to theory by illustrating how cultural responsiveness and reflection-based learning can facilitate attitudinal and behavioral change. It also underscores the importance of integrating indigenous knowledge, leadership structures, and cultural narratives into gender- transformative GBV interventions, rather than relying solely on Western models of advocacy and response.
Implications for Policy and Practice
The study highlights the importance of culturally responsive training initiatives for strengthening GBV prevention and response systems in Eswatini. Engaging both professional service providers and influential community leaders can support survivor-centered practice while challenging harmful gender norms within communities. Policymakers may consider incorporating such capacity-building initiatives into national GBV strategies to strengthen coordinated community responses.
Limitations and Future Directions
This study was limited by its small, region-specific sample and short intervention and follow-up periods, which restricts its transferability and the assessment of long-term change. Future research should build on these findings through larger, multi-site, and longitudinal studies across diverse regions and professional settings in Eswatini, with greater attention to culturally grounded and gender-transformative approaches, including engagement of community leaders, men and boys, and the use of hybrid or digital training models to strengthen sustainable GBV prevention and response.
Conclusion
This study demonstrated that culturally responsive, capacity building training can meaningfully shift how frontline professionals and influential community leaders in Eswatini understand and respond to gender-based violence. By engaging social workers, faith-based leaders, and traditional authorities together, the intervention created a shared space for critical reflection on how cultural norms, patriarchal family structures, religious interpretations, and practices such as lobola can reinforce women’s vulnerability and silence. Participants reported deeper insight into GBV as a systemic issue rather than an individualized or private matter, and greater appreciation of trauma- informed, survivor-centered approaches. Notably, traditional and church leaders began to re-envision their roles not only as custodians of culture but as advocates capable of challenging harmful norms and fostering supportive environments for survivors.
The findings underscore the importance of involving cultural leadership in GBV prevention efforts. Interventions that overlook these actors risk limited reach and sustainability, as cultural narratives and community authority significantly shape attitudes and behaviors. Strengthening leaders’ capacity to model respect, speak against violence, and promote healing has the potential to shift community beliefs, reduce stigma, and expand pathways to safety for survivors.
While the small sample size limits the generalizability of the findings, the training provides a promising foundation for broader community-based strategies. Scaling similar initiatives nationally, alongside ongoing mentorship and multi-sectoral collaboration, may contribute to more sustainable, gender-transformative change. Ultimately, empowering leaders holding moral and cultural influence is essential for promoting dignity, safety, and justice for women and girls in Eswatini.
Competing Interests:
The authors declare that they have no competing interests.
References
Dzinavane, M.T. (2016). Saying No to Gender-Based Violence: A Study of Musasa, A Non-Governmental Organization Based in Zimbabwe. Master of Arts in Development Studies, University of South Africa. View
Heise, L., Greene, M., Opper, N., Stavropoulou, M., & Harper, C. (2019). Gender inequality and restrictive norms: Root causes of violence against women and girls. The Lancet, 394(10204)1687– 1699. View
Hossain, M., Pearson, R. J., McAlpine, A., Bacchus, L.J., Spangaro, J., & Muthuri, S. (2021). Gender-based Violence and its association with mental health among Somali women in a Kenyan refugee camp: latent class analysis. J Epidemiol Community Health, 75, 327–34. View
World Health Organization (WHO). (2021). Violence against women prevalence estimates: Global, regional and national prevalence estimates for intimate partner violence against women and global estimates for non-partner sexual violence against women. Geneva: WHO View
Mpofu, S., & Tfwala, S. (2024). Gender-based violence and cultural norms in Eswatini. Journal of African Psychology, 12(1), 55–71. View
Yalcinoz-Ucan B, Zilney L, Zientarska-Kayko A, Ireland T, Browne DT. (2024). Examining the effectiveness of psychological interventions for marginalized and disadvantaged women and individuals who have experienced gender-based violence: protocol for a scoping review. BMJ Open. View
Hudspeth, J. (2022). Gender-based violence and the role of culture in Eswatini: Implications for social work practice. Southern African Journal of Social Work, 38(3), 215–230.
UNFPA. (2020). Engaging faith-based and traditional leaders in ending gender-based violence: Regional experiences from sub-Saharan Africa. Pretoria: United Nations Population Fund.
Fielding-Miller, R. (2017). Gender inequality and power in Swaziland. African Journal of Reproductive Health, 21(4), 49–60.
Mboya, P., Kimario, T., & Kapinga, R. (2023). Community based interventions for gender-based violence prevention and response in Tanzania: Lessons from a multi-sectoral training program. Africa Journal of Social Work, 13(1), 4
Bott, S., Guedes, A., Ruiz-Celis, A. P. & Mendoza, J. A. (2019). Intimate partner violence in the Americas: A call for action. The Lancet Global Health, 7(1), e2–e View
Kabeer, N. (2016). Gender equality, economic growth, and women’s agency: The central role of local ownership in development. Feminist Economics, 22(1), 1–26 View
Ali, N., Khan, R., & Fatima, S. (2025). Strengthening the health system response to gender-based violence through life skills- based training for healthcare providers in Pakistan. Journal of Gender and Health Development, 14(2), 85–99
International Commission of Jurists. (2020). Women’s access to justice in Eswatini. ICJ Africa. View
Milazzo, A. (2016). Why are adult women missing? World Bank Policy Research Working Paper No. 7508. View
Fielding-Miller, R., Dunkle, K., & Hadley, C. (2016). Cultural norms and gender-based violence in Swaziland. Social Science & Medicine, 168, 134–143. View
Sultana, F., (2020). Embodied Intersectionalities of Urban Citizenship: Water, Infrastructure, and Gender in the Global South, Annals of the American Association of Geographers, 110:5, 1407-1424. View
Nyawo, S. (2020). Women’s Leadership and Participation in Recent Christian Formations in Swaziland: Reshaping the Patriarchal Agenda? Alternation Interdisciplinary Journal for the Study of Arts and Humanities in Southern Africa SP30. View
Mthembu, T. (2019). The cultural meaning of lobola and women’s autonomy in Eswatini. African Sociological Review, 23(2), 89–105.
All Africa. (2015). Four in ten women believe wife-beating is justified. AllAfrica Global Media.
Klomegah, R. (2019). Social acceptance of wife beating in Sub- Saharan Africa. Violence and Victims, 34(2), 240–257.
ICJ & SWAGAA. (2020). Barriers to the Implementation of the SODV Act in Eswatini. International Commission of Jurists. View
Thetsane, R. M. (2019). Local Community Participation in Tourism Development: The Case of Katse Villages in Lesotho. Athens Journal of Tourism, 6, 123-140. View
Shannon, S., Lewis, N., Lee, H. and Hughes, S. (2019) Cannabidiol in Anxiety and Sleep: A Large Case Series. The Permanente Journal, 23, 18-041. View
Hatcher, A. M. (2020). Pathways of reporting violence in southern Africa. Social Science & Medicine, 252, 112917
Motsa, P., & Morojele, P. (2021). Cultural authority and resistance to GBV legislation in Eswatini. Agenda, 35(3), 92 102
Muluneh, M.D., Stulz, V., Francis, L. and Agho, K. (2020). Gender Based Violence against Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. International Journal of Environmental Research and Public Health, 17, Article No. 903. View
DPMO. (2023). National Strategy to End Violence in Eswatini 2023–2027. Deputy Prime Minister’s Office. View
Hossain, M., Zimmerman, C., Kiss, L., Abramsky, T., & Watts, C. (2021). Mental health impacts of gender-based violence: A systematic review of global evidence. World Health Organization Research Brief.
Sikweyiya, Y., Addo-Lartey, A. A., Alangea, D. O., Dako Gyeke, P., Chirwa, E. D., Coker-Appiah, D., Jewkes, R. (2020). Patriarchy and gender-inequitable attitudes as drivers of intimate partner violence against women in the central region of Ghana. BMC Public Health, 20(1). View
United Nations Population Fund (UNFPA). (2022). Population and development report for Africa. UNFPA Africa Regional Office. View
Nyawo, S. (2022). Should Women have 50% Share of Lobola? A, Feminist Reflection on Gender Disparities within Emaswati Culture. African Journals, 1(2). View
British Council. (2013). Gender in Nigeria Report 2012: Improving the Lives of Girls and Women in Nigeria. British Council. View
UN Women. (2024). Ending violence against women and girls in Southern Africa. UN Women Regional Office. View
Hamby, S. (2013). A strength-based approach to research and intervention: Understanding and addressing violence and resilience. Psychology of Violence, 3(4), 381–383.
Albanesi, C., Cicognani, E., & Zani, B. (2021). Community psychology and the study of gender-based violence: Strengthening systems through multi-level interventions. Journal of Communications & Applied Social Psychology, 31(2), 179–193
Allen, N. E., Larsen, S., Trotter, J., & Sullivan, C. M. (2013). Exploring the core service delivery process of an evidence based community advocacy program for women with abusive partners. Journal of Community Psychology, 41(1), 1–18. View
Meyer, S., & Frost, N. (2019). Mapping the systems of domestic violence: A multi-agency systems approach. Journal of Gender-Based Violence, 3(1), 87–102.
Perkins, D. D., & Zimmerman, M. A. (1995). Empowerment Theory, Research, and Application. American Journal of Community Psychology, 23, 569-579. View
Moore, A., Nguyen,A., Rivas, S., Bany-Mohammed, A., Majeika,J., Martinez, L., (2021). A qualitative examination of the impacts of financial stress on college students' well-being: Insights from a large, private institution. SAGE Open Med. 22:9:20503121211018122. View
Goodman, L., & Epstein, D. (2008). Listening to battered women: A survivor-centered approach to advocacy, mental health, and justice. American Psychological Association View
Wood, E. A. (2014). Free Choice and Free Play in Early Childhood Education: Troubling the Discourse. International Journal of Early Years Education, 22, 4-18. View
Joo, Y.B., Lim, Y.H., Kim, K.J., et al. (2019). Respiratory Viral Infections and the Risk of Rheumatoid Arthritis. Arthritis Research & Therapy, 21, Article No. 199. View
Speer, P. W., & Peterson, N. A. (2000). Psychometric properties of an empowerment scale: Testing cognitive, emotional and behavioral domains. Social Work Research, 24(2), 109–118. View
Venkat, R. P., (2017). Strengths-Based Approach in Social Work: A distinct ethical advantage. International Journal of Innovation, Creativity and Change. View
Joseph, R. (2020). The theory of empowerment: A critical analysis with the theory evaluation scale. Journal of Human Behavior in the Social Environment, 30(2), 138-157. View
Joseph, R., Herrera, I. D., & Doyle, K. (2022). Determining the theoretical quality of the Strengths Perspective: A critical analysis. Journal of Family Strengths, 20(1), 12. View
Joseph, R. (2025). A comparative analysis of the Strengths Perspective with the Theory Evaluation Scale. Research on Social Work Practice, 35(2), 233-243. View
Fraser, M. W., & Galinsky, M. J. (2010). Steps in intervention research: Designing and developing social programs. Research on Social Work Practice, 20(5), 459–466. View
Palinkas, L.A., Horwitz’s., S.M., Green, C.A., Wisdom, J.P., Duan, N., & Hoagwood, K. (2015). Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Methods Interpretation Research. Admin Policy Ment Health, 42(5), 533-44 View
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. View
Labra, O., Castro, C., Wright, R., & Chamblas, I. (2019). Thematic analysis in social work: A case study. In B. R. Nikku (Ed.), Global social work – Cutting edge issues and critical reflections, 183–202. View