
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy
Journal of Social Work and Welfare Policy Volume 4 (2026), Article ID: JSWWP-193
https://doi.org/10.33790/jswwp1100193Case Report
Empathy Over Efficiency: Rethinking Communication in Modern Medical Systems for Improved Patient Outcomes
Emma Nesselrodt1, BS, OMS-II and Keita Franklin2*, PhD
1West Virginia School of Medicine, Morgantown, West Virginia, United States.
2Co-Director Columbia Lighthouse, Columbia University, New York, United States.
Corresponding Author Details: Keita Franklin, PhD, Co-Director Columbia Lighthouse, Columbia University, New York, United States.
Received date: 30th March, 2026
Accepted date: 12th May, 2026
Published date: 14th May, 2026
Citation: Nesselrodt, E., & Franklin, K., (2026). Empathy Over Efficiency: Rethinking Communication in Modern Medical Systems for Improved Patient Outcomes.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Communication failures in medical care are commonly framed as deficits in individual clinician skill or empathy. We argue instead that they are predictable outcomes of health systems organized around efficiency, throughput, and task completion rather than relational continuity and psychological safety. Drawing on relationship-centered care (RCC) as a conceptual framework, this article examines how communication functions as a determinant of patient comprehension, trust, and engagement particularly during the disclosure of serious diagnoses and other moments of acute vulnerability. We propose that trauma-informed care offers a means of operationalizing RCC in clinical practice, translating relational values into observable behaviors at the bedside and in institutional design. We further contend that patient-centered care, while a meaningful corrective to paternalistic models, has too often been operationalized as information exchange and patient choice without addressing the relational conditions necessary for those principles to be realized. Drawing on existing scholarship across medicine, social science, and health policy, we identify how time pressures, productivity metrics, hierarchical delegation, depersonalizing institutional practices, and the rapid expansion of telehealth produce conditions in which relational care deteriorates. These failures can harm any patient, and they fall hardest on those with prior trauma, limited health literacy, or historical mistrust of medical institutions, for whom the resources to recover from a poorly handled disclosure are least available. We conclude that improving medical communication requires coordinated, system-level reform. Reframing communication as essential care infrastructure rather than as an ancillary skill positions it as a matter of social welfare and structural equity, not solely clinical quality.
Keywords: Relationship-centered care; trauma-informed care; medical communication; health equity; structural vulnerability; health policy; patient-provider relationships; social determinants of health
Vignette: At age fifty, a woman schedules a routine colonoscopy following standard preventive care recommendations. She is asymptomatic and expects reassurance or, at most, follow-up guidance. After the procedure, she hears nothing for over two months. When the call finally comes, it is not from a physician, but from an administrative staff member who informs her that she must schedule an appointment to receive her results. A telehealth visit is offered.
When the appointment begins, the nurse practitioner appears to be accessing the medical record in real time. Within the first moments of the call, the provider states, “I see here that you have colorectal cancer.” Without pause, context, or assessment of the patient’s understanding, the provider continues: “You’ll need to write down this number to call a surgeon. You’re going to need part of your colon removed.”
Less than two minutes into the encounter, the call has moved from routine check-in to a life-altering diagnosis and surgical referral. The patient, stunned, asks, “What do I have?” There is no discussion of the findings, no explanation of staging, no opportunity for questions, no acknowledgement of shock or fear, and no plan for emotional or informational support. The visit concludes with a phone number and a directive.
This interaction brief, transactional, and devoid of relational engagement illustrates a profound failure in patient-centered communication. This type of communication is the predictable outcome of systems organized around efficiency and throughput, in which relational care is treated as secondary or optional. The structural conditions of contemporary medicine productivity quotas, compressed visit times, fragmented care across multiple providers, and reimbursement models that reward volume over relational engagement shape what is possible at the bedside, often making it difficult for clinicians to communicate well even when they wish to do so [1,2]. The vignette is not a story about an uncaring provider. It is a story about a system that has not built the conditions under which careful, humane communication can reliably occur.
Communication failures of this kind cause distress, and they can produce measurable clinical and psychological harm [3,4]. How information is conveyed particularly during the disclosure of life-altering diagnoses shapes patient comprehension, trust, and long-term psychological adjustment [3,5]. For patients navigating serious illness, the clinical encounter is not only a site of diagnosis and treatment but a moment of profound vulnerability [4]. When communication is abrupt or poorly timed, it can compound psychological distress and undermine informed decision-making [4,5]. For patients with fewer resources to absorb that distress or seek clarification, these failures also widen existing health inequities [6]. Despite decades of attention to patient-centered care, medical training and health care systems continue to treat communication as a secondary skill rather than a core clinical and ethical competency [5]. This gap has significant implications not only for individual patients, but for health systems, professional accountability, and social welfare more broadly.
Introduction: Framing the Problem
Effective communication is foundational to quality health care. It influences patient understanding, treatment adherence, satisfaction, and clinical outcomes [3,7]. Yet in contemporary practice, communication is constrained by time pressures, productivity demands, and institutional structures that privilege biomedical tasks over relational ones [1,2]. As a result, even technically competent care can be experienced as harmful when it does not attend to the patient's emotional state or informational needs. When clinicians fail to identify and meet the unique needs and goals of patients, and to recognize that those needs can evolve throughout treatment, patient outcomes can suffer [4,5]. This article argues that current approaches to medical communication are insufficient because they are inadequately grounded in relational, trauma-informed, and structural understandings of care. Drawing on the framework of relationship-centered care - a model that emphasizes relationships as the foundation of effective, ethical, and humane medical practice [8,9] - we contend that communication should be understood not as an ancillary skill but as a core component of clinical practice and a matter of social welfare and health policy. Synthesizing scholarship across medicine, social science, and health policy, we examine how communication failures reflect systemic shortcomings in medical education, institutional design, and policy - and propose directions for reform. To address these limitations, the article draws on relationship-centered care as a framework that places interpersonal connection at the foundation of clinical practice. The following section introduces this framework in more detail and considers its implications for medical communication.
Relationship-Centered Care as a Conceptual Framework
Relationship-centered care (RCC) is a well-established framework in health care scholarship that emphasizes the centrality of relationships in the delivery of effective, ethical, and humane medical care [8,9]. The framework emerged in the mid-1990s through the work of the Pew-Fetzer Task Force on Advancing Psychosocial Health Education, an interdisciplinary group drawing on medicine, the social sciences, psychology, and ethics [8]. RCC recognizes that health care occurs within a web of interpersonal relationships, each of which shapes clinical outcomes and patient experience [9,10]. Building on this foundation, core principles of RCC include mutual respect between patients and providers; emotional presence and responsiveness as integral to care; recognition of power dynamics inherent in clinical encounters; and acknowledgment that providers are shaped by their relationships with patients, colleagues, institutions, and themselves [9,10]. RCC extends beyond the clinician–patient dyad to encompass clinician–family, clinician–clinician, and clinician–self relationships [8]. This framework is particularly relevant to medical communication because it reframes communication as a relational process embedded within broader social, institutional, and ethical contexts. From an RCC perspective, the failure illustrated in the vignette is not just a lapse in empathy or bedside manner; it represents a breakdown in relational accountability, preparation, and shared meaning-making at a moment of profound patient vulnerability. While patient-centered care has long emphasized respect for patient preferences and autonomy, RCC deepens this orientation by explicitly addressing the relational conditions necessary for those principles to be realized in practice. Without relational attention to timing, emotional readiness, trust, and power asymmetries, information however accurate can become harmful rather than supportive [2,5]. By situating communication within a relationship-centered framework, this article conceptualizes medical communication as a clinical intervention in its own right, one with direct implications for patient well-being, equity, and system performance. This lens provides a foundation for examining how communication failures arise, how they harm patients of all demographic backgrounds while falling hardest on those with the fewest resources to recover from them, and why policy and training and oversight reforms are necessary to address them. Patient-centered care (PCC) emerged as an important corrective to early paternalistic models of medicine, emphasizing respect for patient autonomy, preferences, and shared decision-making [2]. PCC seeks to improve patient satisfaction, informed consent, and attention to patient values within clinical encounters, though debates continue about how consistently these goals are achieved in practice [5]. Patient-centered culturally sensitive health care (PC-CSHC), a branch of PCC, extends these commitments to address health disparities by tailoring care to the cultural, racial, spiritual, and socioeconomic contexts of patients. PC-CSHC emphasizes shared decision-making and attention to barriers such as limited income, inadequate insurance, and low health literacy factors linked to poor outcomes, medical mistrust, and reduced patient engagement [11]. In practice, however, PCC has often been operationalized in ways that emphasize information exchange and patient choice without adequately addressing the relational conditions necessary for patients to process, integrate, and act on that information particularly in moments of vulnerability, crisis, or trauma [11]. When implemented as a set of discrete behaviors or scripted interactions, patient-centered care can become transactional and fail to account for power dynamics, emotional readiness, and the broader relational context of care. These limitations are amplified by the structural conditions of contemporary medicine increasingly time-constrained, technologically mediated, and fragmented care environments in which encounters involving serious diagnoses or life-altering decisions are often compressed into the same time slots as routine visits [1]. The result is that PCC's underlying values can be undermined by the very systems in which it is meant to be practiced, particularly for patients who require more time, relational support, or emotional care than standard workflows allow.
This distinction helps explain why patient-centered frameworks alone may fail to prevent the type of communication breakdown illustrated in the vignette. While patient-centered care emphasizes respect for patient preferences, it does not necessarily require providers or systems to attend to timing, emotional readiness, relational continuity, or the impact of power asymmetries at moments of crisis. Relationship-centered care explicitly includes these elements, making it better suited to address communication failures that carry profound psychological, ethical, and social consequences [2,5].
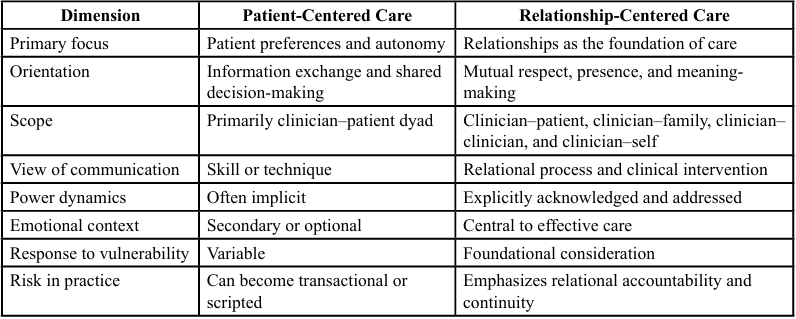
Table 1. Comparison of Patient-Centered and Relationship-Centered Care
While relationship-centered care clarifies what is missing from prevailing models, it offers limited guidance for how communication should unfold in moments of acute vulnerability when patients are receiving life-altering diagnoses, processing fear or shock, or navigating decisions that will shape the rest of their lives. RCC's emphasis on relational continuity, mutual respect, and shared meaning-making is the right foundation for these moments, but the framework does not translate these values into specific communication behaviors that providers can use when patients are emotionally overwhelmed or physiologically activated. Trauma- informed approaches address this gap by offering concrete principles safety, transparency, collaboration, and empowerment, among others that operationalize relational values into observable practices. The next section examines how trauma-informed communication extends and grounds the relational commitments of RCC, particularly in the moments when patients most need them.
Trauma-Informed Communication as a Foundation for Relationship-Centered Care
Relationship-centered care (RCC) provides a compelling conceptual framework for understanding medical communication as a relational process rather than a transactional exchange. However, RCC alone does not fully specify how providers and systems should communicate in contexts of vulnerability, fear, and physiological threat conditions that are common in medical environments and nearly universal when serious diagnoses are delivered. For this reason, we argue that RCC should be explicitly underpinned by trauma-informed communication.
Trauma-informed care (TIC) is a framework that recognizes the widespread prevalence of trauma in patient populations and structures clinical practice to minimize the risk of re-traumatization [12]. It is best understood as a universal precautions approach applied to all patients regardless of disclosed trauma history rather than as a treatment for diagnosed trauma-related conditions [13]. This distinguishes TIC from trauma-focused or trauma-specific therapies, which directly treat the consequences of trauma; TIC instead reorients the broader environment in which all care is delivered.
Trauma-informed care recognizes that many patients carry prior experiences of trauma and that medical encounters themselves can be experienced as threatening or destabilizing particularly when communication is abrupt or delivered without relational containment. Beyond recognizing trauma, the framework emphasizes practical, organization-spanning principles that can be translated into clinical communication behaviors. SAMHSA identifies six guiding principles safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice, and choice; and attention to cultural, historical, and gender factors that can be continuously assessed and embedded across systems of care [12].
Why trauma-informed communication is necessary in modern medical care
The vignette illustrates an interaction that can be clinically “efficient” while psychologically destabilizing: delayed results, limited preparation, and an abrupt disclosure of cancer followed by immediate instruction toward surgery. Such delivery shapes patient comprehension and informed consent, particularly during emotionally overwhelming encounters [3]. While this interaction aligns with what is often described in the clinical literature as the delivery of 'serious' or 'life-altering' information, recent scholarship cautions against reducing these encounters to procedural models of 'breaking bad news.' Back and colleagues [4] have argued that clinician communication skills should be regarded as a clinical procedure requiring deliberate training and assessment. They estimate that more than 219,000 physicians and advanced practice providers in the United States could benefit from evidence-based communication training, and they document that most clinicians currently in practice did not receive such training during their formative education. The result is a measurable gap between what serious illness conversations require and what clinicians have been prepared to deliver a gap that shapes patient trust, comprehension, and the alignment of care with patient values.
Trauma-informed care aims to improve patient outcomes by reducing the risk of re-traumatization in clinical settings [14]. Effective implementation requires clinicians to recognize that trauma presents differently across patients and to respond with active listening, emotional security, and shared decision-making [13]. Given the prevalence of trauma in patient populations, building trust through transparent, collaborative interaction is foundational to the framework's clinical application [12]. Training and ongoing education rather than one-time exposure are crucial to providing this care consistently [14].
Patient perspectives, rather than clinician convenience or institutional efficiency, must meaningfully inform how these conversations are conducted, evaluated, and taught. These risks are amplified in technology-mediated contexts. Telehealth has become a common mode of cancer care delivery, but research on oncology professionals' experiences suggests that delivering serious or bad news by video introduces relational challenges, including reduced nonverbal cues and concerns about diminished connection between clinician and patient [15].
Aligning trauma-informed principles with RCC
We propose that trauma-informed communication operationalizes RCC by translating relational values into observable practices. The following examples adapt SAMHSA's six guiding principles [12] to the clinical communication context, drawing also on the trauma-informed application work of Gerber et al. [13] and the cultural humility framework of Tervalon and Murray-García [16]:
• Safety (psychological as well as physical): Providers prepare the patient for what is coming (“I have difficult results to discuss”), assess whether the patient is in a private/supportive space, and pace information to avoid overwhelming cognitive load.
• Trustworthiness and transparency: Clear explanation of the process (why there was a delay; what the report shows; what is known vs. uncertain) reduces the patient’s sense of being managed or rushed.
• Collaboration and mutuality: The encounter is framed as a shared plan (“Let’s go through the findings together and decide next steps”) rather than a directive.
• Empowerment, voice, and choice: Patients are offered structured choices (timing of follow-up, inclusion of family, written summary, option for second opinion, and time to ask questions) to counteract helplessness during threatening news. Providers should also discuss patients' goals of care directly, supporting informed decisions tailored to their preferences and needs.
• Cultural, historical, and gender considerations: Communication explicitly recognizes differential trust in institutions and varied preferences for information and decision- making, rather than assuming a single “ideal” patient response.
• Peer support: While peer support typically operates adjacent to the clinician-patient encounter, providers can recognize its value by connecting patients with patient navigators, survivor mentors, or peer support groups when appropriate, particularly for patients facing serious illness, prior trauma, or marginalization.
Importantly, these trauma-informed principles extend beyond the clinician–patient dyad. They depend on workflows, staffing models, and institutional norms precisely the relational ecology emphasized by RCC. When systems delegate serious diagnosis disclosure without safeguards, compress visits into productivity-driven time slots, or rely on telehealth without structured protocols for delivering bad news, they inadvertently create conditions that increase patient distress and erode trust.
Trauma-informed communication in digital and telehealth settings
Gerber et al. [13] argue that trauma-informed principles can be meaningfully applied to telehealth, and that telehealth's flexibility and reduced power asymmetries can support core TIC values such as safety, trustworthiness, and collaboration when implemented with intention. In telehealth contexts, trauma-informed communication requires intentional design adequate visit length for serious results, advance preparation, structured pauses for emotion, and clear follow-up plans. A trauma-informed, relationship-centered approach also highlights why one-off communication workshops often fail: providers require longitudinal training, coached practice, and system reinforcement [4].
A Conceptual Model for Trauma-Informed, Relationship Centered Communication
We propose that relationship-centered care and trauma-informed communication can be understood as complementary and mutually reinforcing components of effective medical communication. In this conceptual model, relationship-centered care [8-10] serves as the overarching framework, establishing relationships as the ethical and clinical foundation of care. Trauma-informed communication, drawing on the principles articulated by SAMHSA [12] and applied to healthcare settings by Gerber and colleagues [13], functions as the operational mechanism through which relational values are enacted in practice particularly in moments of vulnerability, uncertainty, or threat. When trauma-informed principles such as safety, transparency, collaboration, and empowerment are embedded within relationship- centered systems, they shape both individual clinician behaviors (e.g., pacing, preparation, empathic presence) and institutional practices (e.g., workflows for delivering serious diagnoses, telehealth protocols, follow-up supports). Together, these elements form a pathway from values to action a synthesis the authors propose as a means of strengthening medical communication in moments of acute patient need. This model highlights that communication failures are rarely the result of individual clinician shortcomings alone, but rather reflect misalignment between relational values, trauma-informed practices, and the systems in which care is delivered. Despite the clarity of this model, its implementation is routinely undermined by the structural and institutional realities of contemporary health care.
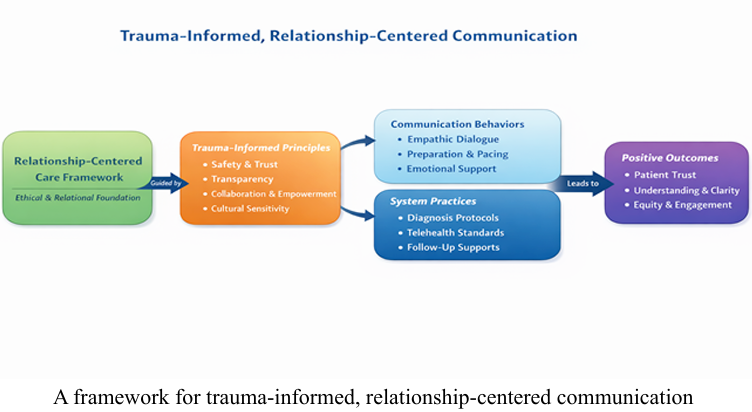
A framework for trauma-informed, relationship-centered communication
Structural and Institutional Barriers to Trauma-Informed, Relationship-Centered Communication
While Relationship-centered care and trauma-informed communication provide clear guidance for ethical and effective clinical interactions, their implementation is often constrained by structural and institutional conditions that shape how care is delivered. Communication failures such as those illustrated in the vignette are rarely the result of individual clinician disregard or incompetence. Rather, they are the predictable outcomes of systems designed around efficiency, throughput, and risk management rather than relational continuity, psychological safety, and patient understanding [1]. Contemporary health care environments place increasing pressure on providers to deliver complex information within compressed timeframes. Productivity expectations and system-level pressures frequently limit the duration and flexibility of clinical encounters, even when patients are receiving life-altering diagnoses [1]. In such contexts, communication becomes task- oriented focused on conveying results and initiating referrals rather than relational, reflective, or responsive to patient emotional states. These pressures undermine providers’ ability to pace conversations, assess understanding, and provide the emotional containment required for trauma-informed care.
Hierarchical structures within medical institutions further complicate communication practices. Decisions about who delivers serious diagnoses are often driven by availability, workflow logistics, or delegation norms rather than by relational continuity or clinical appropriateness. As a result, patients may receive devastating news from providers with whom they have no established relationship, in settings that do not allow for follow-up questions or emotional support. This leaves patients with unanswered questions and uncertainty about the progression of their care. Patients with chronic illnesses and complex diagnoses will have multiple healthcare providers involved in various aspects of their treatment, thus contributing to discontinuity in care and increasing the likelihood of gaps in communication between providers. This not only can further the distress and confusion patients may experience but can also jeopardize patient safety and quality of care received [17]. These gaps erode trust and can leave patients feeling abandoned when relational stability is most needed. Communication and continuity within healthcare teams is vital for improving patient outcomes and satisfaction [17], but many common healthcare practices and policies can further create impersonal relationships.
Haque and Waytz [18] describe deindividuating practices as one of several mechanisms through which dehumanization occurs in medical settings. Routines such as standardized uniforms, hospital gowns, masks, and patient wristbands while functional for institutional purposes can blur the recognition of patients and providers as distinct individuals. When roles overlap and team members become individually unidentifiable, personal accountability for decision- making and patient outcomes can erode. Similarly, dressing patients in identical gowns and assigning patient identifiers can make providers feel less personally connected to those they treat, with implications for empathic engagement [18].
The combined effect of standardized institutional procedures and depersonalizing practices is to weaken the recognition of patients as unique individuals a recognition that trauma-informed, relationship- centered communication depends on. For healthcare providers to better support and care for patients, they must view patients as individuals, personalize treatment plans and have conversations aimed at better understanding unique circumstances–all of which are complicated by the growing use of technology in healthcare systems.
Technology-mediated care introduces additional institutional challenges and further diminishes personal relationships between patients and healthcare providers. While telehealth and the use of patient portals have expanded access and convenience, they have been integrated rapidly, often without parallel investment in communication standards or training specific to high-stakes conversations [15]. Delivering serious diagnoses via telehealth or patient portals without clear protocols for preparation, privacy assessment, emotional support, and follow-up reflects a system- level failure to align technological innovation with trauma-informed, relationship-centered principles [13]. In these settings, efficiency gains may come at the cost of increased patient distress and disengagement.
Importantly, these structural barriers disproportionately affect patients who are already vulnerable, including those with limited health literacy, prior trauma exposure, mistrust of medical institutions, or fewer social supports [5,6]. When communication is rushed, opaque, or directive, patients with fewer resources are less able to seek clarification, advocate for themselves, or pursue second opinions, deepening the disconnect between high patient satisfaction with care and poor understanding of it that is most pronounced among those with low literacy and social disadvantage [5]. Thus, communication failures function not only as clinical shortcomings but as mechanisms through which health inequities are reproduced. From a social welfare and policy perspective, these patterns underscore the need to move beyond individual-level solutions. Training providers to communicate more empathically and empower patients to be involved in decision making are necessary but insufficient if institutional conditions consistently undermine trauma-informed, relationship-centered practice. Without structural alignment through policy, reimbursement models, accreditation standards, and organizational accountability communication failures will remain a predictable feature of modern health care delivery.
Implications for Medical Education and Professional Training
The structural barriers described above are reinforced and often normalized through medical education and professional socialization. Although communication is widely acknowledged as important, it is frequently treated as an ancillary competency rather than as a core clinical skill requiring the same rigor, supervision, and assessment as diagnostic or procedural expertise [4]. As a result, providers may enter practice technically proficient yet underprepared to navigate high-stakes, emotionally charged conversations in trauma-informed, relationship-centered ways.
Many medical curricula rely on brief workshops, simulated patient encounters, or checklists that emphasize technique over relational presence. While these approaches may improve discrete behaviors, they are insufficient for preparing providers to manage real-world complexity, particularly in moments involving serious diagnoses or patient distress [4]. Many simulation curricula prioritize physical examination skills and differential diagnosis over patient education and relational engagement. Without longitudinal reinforcement and reflective supervision, communication skills risk becoming scripted performances rather than integrated clinical capacities. What is sometimes called the hidden curriculum the implicit lessons learners absorb through clinical observation rather than formal teaching further undermines relationship-centered communication. When on clinical rotations, students learn implicitly which behaviors are valued through observation of senior providers, time pressures on clinical services, and institutional reward structures. If learners observe rushed disclosure of serious diagnoses, delegation of difficult conversations without relational continuity, or prioritization of efficiency over patient understanding, these practices become normalized even when they conflict with formal teaching on empathy and patient-centered care.
A trauma-informed, relationship-centered approach to communication requires a shift in how communication is taught, practiced, and evaluated across the continuum of medical education. Rather than treating communication as a discrete skill, training programs and patient encounters should conceptualize it as a form of clinical judgment one that requires situational awareness, emotional attunement, ethical reasoning, and adaptability. This includes preparing providers to recognize patient vulnerability, anticipate emotional responses, and intentionally structure conversations to support safety, comprehension, and agency.
Several educational implications follow from this reframing. First, communication training should be longitudinal, extending across undergraduate medical education, graduate medical education, and continuing professional development [4]. Second, training must include supervised practice in real clinical contexts, particularly for delivering serious or life-altering information. Third, reflective spaces such as facilitated debriefings or mentorship are essential for helping providers process the emotional labor of these encounters and integrate trauma-informed principles into their professional identity.
Importantly, education alone cannot carry the full burden of change. Even well-trained providers will struggle to practice trauma-informed, relationship-centered communication if institutional conditions consistently undermine these values. Nevertheless, medical education plays a critical role in shaping professional norms, expectations, and accountability. By explicitly aligning communication training with relationship-centered and trauma-informed frameworks, medical education can help interrupt cycles in which systemic pressures are reproduced through professional practice.
Policy and System-Level Implications
If trauma-informed, relationship-centered communication is to become a standard of care rather than an aspirational ideal, it must be supported through policy, regulation, and institutional accountability. Communication failures such as those illustrated in the vignette persist because health care systems have not consistently aligned incentives, standards, and oversight with relational and psychological dimensions of care. Addressing these gaps requires attention to multiple policy domains.
Accreditation and Professional Standards
Accrediting bodies play a critical role in shaping professional priorities. Although communication competencies appear in accreditation standards, they are not always operationalized or evaluated with the rigor applied to technical skills. Accrediting organizations for undergraduate and graduate medical education could strengthen expectations by explicitly requiring demonstrated competence in trauma-informed, relationship-centered communication, particularly for high-stakes encounters such as serious diagnoses, end-of-life discussions, and major treatment decisions. Such standards should emphasize observed practice and reflective supervision rather than reliance on self-report or isolated simulations.
Reflective supervision, drawn from social work, mental health, and clinical education traditions, offers a concrete model for developing these capacities. Unlike case review or task-focused supervision, reflective supervision creates structured, ongoing space for clinicians to examine the emotional and relational dimensions of their work what they are carrying from difficult encounters, what assumptions or biases are surfacing, and where their own social location shapes their interactions with patients. Embedded within reflective supervision is the practice of cultural humility, which Tervalon and Murray-García [16] propose as a more suitable framework than cultural competence for clinical training. Where cultural competence implies the mastery of another culture's content, cultural humility involves a lifelong commitment to self-evaluation, attention to power imbalances in the clinician-patient relationship, and the development of nonpaternalistic partnerships with patients and communities [16]. For trauma-informed, relationship-centered communication to function across diverse patient populations, accreditation standards should explicitly support both reflective supervision and the cultivation of cultural humility as ongoing professional practices rather than one time training requirements.
Reimbursement and Time Structures
Payment models strongly influence how clinical time is allocated. Fee-for-service structures and productivity metrics often de- incentivize the extended, flexible encounters necessary for trauma- informed communication. Policy reforms that recognize time spent on complex communication through billing codes, bundled payments, or value-based models would signal that relational work is legitimate clinical labor rather than an optional add-on. Without such alignment, providers may be forced to choose between meeting institutional expectations and meeting patient needs.
The limits of existing protocols illustrate why structural support matters. The SPIKES protocol a six-step framework for delivering bad news developed by Baile and colleagues [19] and now widely taught in medical education addresses important elements of difficult conversations, including private settings, attention to what the patient already understands, empathic response to emotion, and a clear plan moving forward. SPIKES is teachable, replicable, and has been associated with increased clinician confidence in delivering serious diagnoses. From a relationship-centered, trauma-informed perspective, however, it remains partial. SPIKES treats the disclosure as a single, discrete encounter rather than as one moment within a longer relational arc; it does not explicitly address prior trauma, cultural dynamics, or the power asymmetries inherent in the clinician- patient relationship; and it presupposes that the clinician has the time, setting, and institutional support to follow the protocol precisely what fee-for-service and productivity-driven systems often fail to provide. Protocols like SPIKES can support but cannot replace the structural conditions that make relational communication possible.
Telehealth Governance and Protocols
As telehealth becomes a growing component of health care delivery, policy frameworks must distinguish between routine care and encounters that require heightened relational safeguards. Delivering serious diagnoses via telehealth should not default to the most convenient modality or available clinician, and patient portals should not be an alternative to personal communication.
Clear institutional protocols supported by regulatory guidance are needed to ensure appropriate preparation, privacy, and follow-up when telehealth is used for high-stakes communication [13]. Without such infrastructure, telehealth becomes another setting in which efficiency-driven communication patterns are reproduced, often with reduced opportunity for emotional attunement and relational continuity [15].
Organizational Accountability and Quality Measurement
Current quality metrics rarely capture the relational and psychological dimensions of care. Patient satisfaction surveys and complaint-based systems provide limited insight into whether communication supported understanding, trust, and emotional safety. Policymakers and health systems should consider developing and validating measures that assess communication quality in ways that reflect patient experience and equity, particularly for populations at higher risk of trauma or marginalization.
A growing body of measurement work points toward what such instruments could include. The Discrimination in Medical Settings (DMS) Scale, validated by Peek and colleagues [20], captures patient-reported experiences of discrimination during clinical encounters the kinds of interactions that standard satisfaction surveys are not designed to detect. The Consumer Assessment of Healthcare Providers and Systems Cultural Competence Item Set (CAHPS- CC) extends mainstream patient experience surveys with domains specifically relevant to diverse populations, including doctor-patient communication, equitable treatment, trust, and access to interpreter services [21]. Both instruments respond to a documented gap: standard quality measurement tools do not adequately assess whether patients have been treated with respect for their identity, free from assumptions or stereotyping, or supported in ways that account for their cultural context.
Incorporating measures of this kind into quality improvement and reporting structures would elevate communication from an individual skill to an organizational responsibility. It would also surface inequities that current measurement approaches obscure. As measurement research in this area continues to develop, health systems should treat the assessment of culturally responsive, identity respecting communication as a core component of quality, not as an optional supplement.
Equity and Social Welfare Considerations
From a social welfare perspective, communication failures function as a structural determinant of health [6]. Patients with fewer resources, lower health literacy, language barriers, or prior experiences of trauma are disproportionately harmed when communication is rushed, opaque, or directive.
Policies that strengthen communication standards therefore serve as equity interventions, reducing the likelihood that vulnerability is compounded by system design [6]. Framing communication as a matter of social welfare underscores the ethical obligation of institutions to protect patients from avoidable psychological harm particularly when those patients are already navigating inequitable access to care, language barriers, or institutional mistrust shaped by histories of medical harm.
Taken together, these policy levers highlight that improving medical communication is not solely a matter of clinician education or individual intention. It is a systems-level challenge that requires coordinated action across education, reimbursement, technology governance, and accountability mechanisms. Without such alignment, trauma-informed, relationship-centered communication will remain unevenly practiced and inequitably distributed.
Discussion and Conclusion
The clinical encounter described at the outset of this article is striking and familiar. A serious diagnosis is delivered efficiently, accurately, and without malice yet in a manner that leaves the patient disoriented, frightened, and unsupported. This vignette illustrates how harm can occur even in the absence of technical error, and how communication itself functions as a determinant of patient well-being.
By situating medical communication within a relationship- centered and trauma-informed framework, this article argues that communication failures are best understood as systemic rather than individual shortcomings. Relationship-centered care provides a necessary conceptual foundation by recognizing that clinical care is inherently relational and that outcomes are shaped not only by what is said, but by how, when, and within what relational context information is conveyed. We have proposed that trauma-informed communication operationalizes these relational commitments, translating values such as safety, transparency, collaboration, and empowerment into observable practices, particularly in moments of vulnerability.
The analysis highlights how contemporary health care systems frequently undermine these principles. Time pressures, productivity metrics, hierarchical delegation, and rapid adoption of technology without corresponding communication safeguards create predictable conditions in which relational care deteriorates. These conditions can harm any patient, and they fall hardest on those with prior trauma exposure, limited health literacy, fewer social supports, lower socioeconomic status, or historical mistrust of medical institutions. In this way, communication failures function as mechanisms through which inequities are reproduced, making medical communication a matter of social welfare as well as clinical quality. Importantly, this article does not argue that providers lack compassion or awareness. Rather, it demonstrates how professional training and institutional design shape what is possible in practice, and how standardization in healthcare systems can erode the recognition of patients as individuals.
When communication is treated as a secondary skill taught episodically, assessed superficially, and unsupported by system-level incentives providers are left to navigate ethically complex encounters within structures that reward efficiency over presence. Education reforms, while essential, cannot succeed in isolation without parallel policy alignment.
The policy implications outlined here underscore that trauma- informed, relationship-centered communication is achievable using existing levers: accreditation standards that emphasize observed practice, reimbursement models that recognize relational labor, telehealth governance that differentiates routine care from high- stakes communication, and quality measures that reflect patient experience and equity. Together, these approaches shift responsibility from individual providers to the systems that shape care delivery.
Reframing communication as infrastructure for care has practical and ethical significance. Just as health systems invest in technologies, protocols, and procedures to reduce physical harm, they bear responsibility for designing environments that minimize avoidable psychological harm. Communication is not ancillary to care; it is care. When delivered without preparation, relational continuity, or attention to patient vulnerability, even accurate information can destabilize, disempower, and disengage a patient. When delivered within trauma- informed, relationship-centered systems, communication can foster understanding, trust, and agency outcomes essential to both health and social welfare.
As healthcare continues to evolve amid technological advancement and increasing complexity, a key challenge is how to communicate differently. Aligning values, training, and policy around trauma- informed, relationship-centered communication offers a path forward one that honors the humanity of patients and providers alike, and recognizes that what is said to patients in moments of vulnerability matters as much as any intervention provided.
Conflicts of Interest:
The authors declare no conflicts of interest.
References
Shanafelt, T. D., Dyrbye, L. N., & West, C. P. (2017). Addressing physician burnout: The way forward. JAMA, 317(9), 901–902. View
Mead, N., & Bower, P. (2000). Patient-centredness: A conceptual framework and review of the empirical literature. Social Science & Medicine, 51(7), 1087–1110. View
Ong, L. M. L., de Haes, J. C. J. M., Hoos, A. M., & Lammes, F. B. (1995). Doctor–patient communication: A review of the literature. Social Science & Medicine, 40(7), 903–918. View
Back, A. L., Fromme, E. K., & Meier, D. E. (2019). Training clinicians with communication skills needed to match medical treatments to patient values. Journal of the American Geriatrics Society, 67(S2), S435–S441. View
Epstein, R. M., & Street, R. L., Jr. (2011). The values and value of patient-centered care. Annals of Family Medicine, 9(2), 100- 103. View
Bowen, E. A., Murshid, N. S., & Smith, J. C. (2016). Trauma- informed social policy: A conceptual framework for policy analysis and advocacy. American Journal of Public Health, 106(2), 223–229. View
Stewart, M. A. (1995). Effective physician-patient communication and health outcomes: A review. CMAJ: Canadian Medical Association Journal, 152(9), 1423–1433. View
Tresolini, C. P., & Pew-Fetzer Task Force on Advancing Psychosocial Health Education. (1994). Health professions education and relationship-centered care. Pew Health Professions Commission. View
Beach, M. C., & Inui, T. S. (2006). Relationship-centered care: A constructive reframing. Journal of General Internal Medicine, 21(S1), S3–S8. View
Suchman, A. L. (2006). A new theoretical foundation for relationship-centered care: Complex responsive processes of relating. Journal of General Internal Medicine, 21(S1), S40- S44. View
Garcia, K. A., Wippold, G. M., Goodrum, N. M., Williams, M. M., & Kloos, B. (2025). Bridging health self-efficacy and patient engagement with patient-centered culturally sensitive health care for Black American adults. Journal of Community Psychology, 53(1), e23147. View
Substance Abuse and Mental Health Services Administration. (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach (HHS Publication No. SMA 14- 4884). U.S. Department of Health and Human Services. View
Gerber, M. R., Elisseou, S., Sager, Z. S., & Keith, J. A. (2020). Trauma-informed telehealth in the COVID-19 era and beyond. Federal Practitioner, 37(7), 302–308. View
Menschner, C., & Maul, A. (2016). Key ingredients for successful trauma-informed care implementation. Center for Health Care Strategies. View
Heyer, A., Granberg, R. E., Rising, K. L., Binder, A. F., Gentsch, A. T., & Handley, N. R. (2021). Medical oncology professionals' perceptions of telehealth video visits. JAMA Network Open, 4(1), e2033967. View
Tervalon, M., & Murray-García, J. (1998). Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. Journal of Health Care for the Poor and Underserved, 9(2), 117–125. View
Noest, S., Ludt, S., Klingenberg, A., Glassen, K., Heiss, F., Ose, D., Rochon, J., Bozorgmehr, K., Wensing, M., & Szecsenyi, J. (2014). Involving patients in detecting quality gaps in a fragmented healthcare system: Development of a questionnaire for Patients' Experiences Across Health Care Sectors (PEACS). International Journal for Quality in Health Care, 26(3), 240- 249. View
Haque, O. S., & Waytz, A. (2012). Dehumanization in medicine: Causes, solutions, and functions. Perspectives on Psychological Science, 7(2), 176–186. View
Baile, W. F., Buckman, R., Lenzi, R., Glober, G., Beale, E. A., & Kudelka, A. P. (2000). SPIKES A six-step protocol for delivering bad news: Application to the patient with cancer. The Oncologist, 5(4), 302–311. View
Peek, M. E., Nunez-Smith, M., Drum, M., & Lewis, T. T. (2011). Adapting the Everyday Discrimination Scale to medical settings: Reliability and validity testing in a sample of African American patients. Ethnicity & Disease, 21(4), 502–509. View
Weech-Maldonado, R., Carle, A., Weidmer, B., Hurtado, M., Ngo-Metzger, Q., & Hays, R. D. (2012). The Consumer Assessment of Healthcare Providers and Systems (CAHPS) Cultural Competence (CC) Item Set. Medical Care, 50(9 Suppl 2), S22–S31. View