
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of CAM Research Progress
Journal of CAM Research Progress
Journal of CAM Research Progress Volume 1 (2022), Article ID: JCRP-101
https://doi.org/10.33790/jcrp1100101Research Article
Non-Pharmacological Treatments in Juvenile Fibromyalgia. Systematic Review of Clinical Trials
Eva María Martínez Jiménez
Department of Nursing, Physiotherapy and Podiatry, Universidad Complutense de Madrid, Spain.
Corresponding Author Details: Eva María Martínez Jiménez, Department of Nursing, Physiotherapy and Podiatry, Universidad Complutense de Madrid, Spain. E-mail: evamam03@ucm.es
Received date: 27th December, 2021
Accepted date: 10th January, 2022
Published date: 12th January, 2022
Citation: Martínez Jiménez, E.M. (2022). Non-Pharmacological Treatments in Juvenile Fibromyalgia. Systematic Review of Clinical Trials. J CAM Research Progress, 1(1): 101.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Introduction
Fibromyalgia is a chronic, debilitating, non-inflammatory musculoskeletal pain syndrome. In 1992, fibromyalgia was recognised by the World Health Organisation as a debilitating disease [1]. It is characterised by constant widespread pain, especially due to tender or trigger points, paraesthesia, sleep disturbances, fatigue, irritable bowel, burning during urination, headache, memory loss, difficulty concentrating and mood disorders [1,2]. It is usually diagnosed in adolescence. It can occur in school-aged children, with headache occurring in 68% of subjects [3].
Juvenile fibromyalgia syndrome (JFS) has few prevalence studies, but those that do exist report 2-6% of cases of juvenile fibromyalgia in school-aged children, and as in the adult population, the disorder affects more females than males in children and adolescents. In general the onset of JFS is recorded during early adolescence, younger children are also identified [4]. The mean age of diagnosis is 14.5 14.5 years, although the range is 5 to 18 years overall [5]. The average age of diagnosis is 14.5 14.5 years, although the range is from 5 to 18 years.
The approach to this disease is hampered by the fact that there are NO accurate diagnostic tests. Muscle pain and other patient-reported symptoms [6]. The diagnosis of JFS is based on the self-reported symptoms of the 1990 American College of Rheumatology (ACR) diagnostic criteria, which are more appropriate for adults [7]. The number of tender points needed for diagnosis in an adult is 11, whereas an adolescent or child with JFS is 11, whereas an adolescent or child with JFS is 11. The number of tender points needed for diagnosis in an adult is 11, whereas an adolescent or child with juvenile fibromyalgia has 9.7 points. Therefore, these studies may underestimate the true prevalence of JFS. In addition to the typical symptoms of adults with fibromyalgia, school or juvenile patients with fibromyalgia have their own symptoms [6].
These include joint laxity or hypermobility, increased autonomic dysfunction, and specific psychopathological comorbidities, including depression and anxiety disorders [7]. Other symptoms of patients with fibromyalgia may also be found in school or juvenile fibromyalgia. Other symptoms of patients with juvenile Fibromyalgia include stiffness, subjective joint swelling and abdominal pain [6]. These symptoms may be more common in children with onset of the disease before the age of ten [4,6,7]. The following symptoms may be more common in children.
Although the role of psychological factors in the aetiology of fibromyalgia is unknown, more severe symptoms that complicate the treatment of juvenile fibromyalgia have been associated with psychological disturbances. One example is anxiety, which is associated with low-functioning patients with juvenile fibromyalgia [7]. The role of psychological factors in the aetiology of fibromyalgia is unknown. Truancy and avoidance of usual daily activities and peer relationships. Measures of well-being should be assessed. It is imperative to include information about the child's family, social and academic environment in the primary assessment, because of its importance in treatment [7-9]. Evidence for the efficacy of medications for the treatment of juvenile fibromyalgia syndrome is currently limited. While there are medications approved by the US Food and Drug Administration (duloxetine, milnacipran and pregabalin) for adults with fibromyalgia syndrome, there are none for the treatment of JFS.
There are none for the treatment of FMS. A variety of medications are commonly prescribed for the treatment of FMS, including (but not limited to) non-opioid analgesics, opioids, anticonvulsants, antidepressants, and muscle relaxants [12]. The following are commonly prescribed for the treatment of FMS.
The objective of the present research is to find out which physical therapy treatments have shown efficacy in the treatment of juvenile fibromyalgia.
Material and method
A literature review was carried out in the Medline-pubmed, Cochrane and PeDro search engines during the month of September 2021. The following keywords used were "Fibromyalgia", "adolescent" and "Physical Therapy Modalities". The booleans used were AND.
- Inclusion criteria all articles 10 years prior to September 2021.
- Exclusion criteria articles that were not experimental studies.
- Inclusion criteria all articles 10 years prior to September 2021.
- Exclusion criteria articles that were not experimental studies.
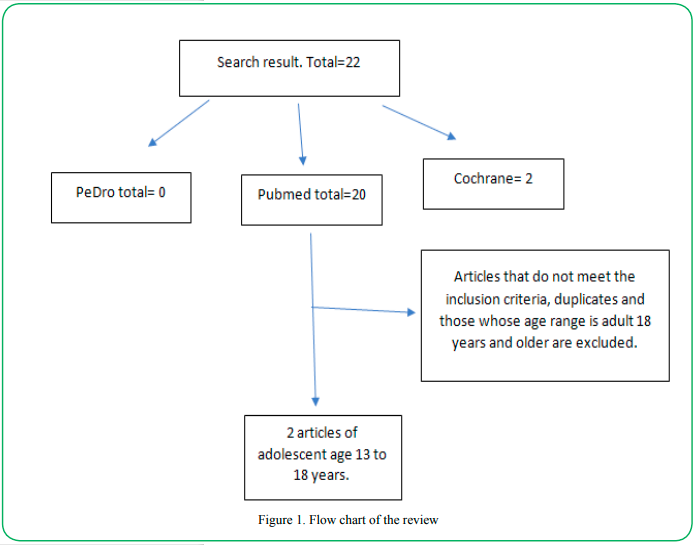
Figure 1. Flow chart of the review
Results
Two trials were found in the study population that met the inclusion and exclusion criteria.
Both studies highlight the importance of integrative neuromuscular exercise and cognitive behavioural therapy as an effective treatment tool as it produces:
- Greater pain reduction in combination than cognitive behavioural therapy alone [13].
- In combination they produce a significant improvement in functionality and a reduction in fear of movement [14].
Conclusions
In non-pharmacological treatment, the combination of integrative neuromuscular exercise and cognitive behavioural therapy is currently the most evidenced therapy to reduce pain, fear of movement and improve functionality.
Competing Interests:
Author report no conflict or competing interest.
References
Yunus, M.B., Masi, A.T. (1985). Juvenile Primary Fibromyalgia Syndrome. A Clinical Study of Thirty-three Patients and Matched Normal Controls. Arthritis & Rheumatism, 28, doi:10.1002/art.1780280205.View
Zemel, L., Blier, P.R. (2016). Juvenile Fibromyalgia: A Primary Pain, or Pain Processing, Disorder. Seminars in Pediatric Neurology, 23.View
Matera, E., Palumbi, R., Peschechera, A., Petruzzelli, M.G., Sciruicchio, V., de Tommaso, M., Margari, L. (2019). Juvenile Fibromyalgia and Headache Comorbidity in Children and Adolescents: A Literature Review. Pain Research and Management.View
Kashikar-Zuck, S., King, C., Ting, T. v., Arnold, L.M. (2016). Juvenile Fibromyalgia: Different from the Adult Chronic Pain Syndrome? Current Rheumatology Reports, 18.View
Coles, M.L., Uziel, Y. (2021). Juvenile Primary Fibromyalgia Syndrome: A Review- Treatment and Prognosis. Pediatric Rheumatology, 19.View
Ting, T. v., Hashkes, P.J., Schikler, K., Desai, A.M., Spalding, S., Kashikar-Zuck, S. (2012). The Role of Benign Joint Hypermobility in the Pain Experience in Juvenile Fibromyalgia: An Observational Study. Pediatric Rheumatology, 10, doi:10.1186/1546-0096-10-16.View
Cunningham, N.R., Tran, S.T., Lynch-Jordan, A.M., Ting, T. v., Sil, S., Strotman, D., Noll, J.G., Powers, S.W., Arnold, L.M., Kashikar-Zuck, S. (2015). Psychiatric Disorders in Young Adults Diagnosed with Juvenile Fibromyalgia in Adolescence. Journal of Rheumatology, 42, doi:10.3899/jrheum.141369.View
Schanberg, L.E., Keefe, F.J., Lefebvre, J.C., Kredich, D.W., Gil, K.M. (1998). Social Context of Pain in Children with Juvenile Primary Fibromyalgia Syndrome: Parental Pain History and Family Environment. Clinical Journal of Pain, 14, doi:10.1097/00002508-199806000-00004.View
Schanberg, L.E., Keefe, F.J., Lefebvre, J.C., Kredich, D.W., Gil, K.M. (1996). Pain Coping Strategies in Children with Juvenile Primary Fibromyalgia Syndrome: Correlation with Pain, Physical Function, and Psychological Distress. Arthritis and Rheumatism, 9, doi:10.1002/1529-0131(199604)9:2<89::AID-ANR1790090204>3.0.CO;2-J.View
Daffin, M., Gibler, R.C., Kashikar-Zuck, S. (2020). Measures of Juvenile Fibromyalgia. Arthritis Care and Research, 72, doi:10.1002/acr.24197View
Kean, J., Monahan, P.O., Kroenke, K., Wu, J., Yu, Z., Stump, T.E., Krebs, E.E. (2016). Comparative Responsiveness of the PROMIS Pain Interference Short Forms, Brief Pain Inventory, PEG, and SF-36 Bodily Pain Subscale. Medical Care, 54, 414– 421, doi:10.1097/MLR.0000000000000497.View
Gmuca, S., Sherry, D.D. (2017). Fibromyalgia: Treating Pain in the Juvenile Patient. Pediatric Drugs, 19.View
Kashikar-Zuck, S., Black, W.R., Pfeiffer, M., Peugh, J., Williams, S.E., Ting, T. v., Thomas, S., Kitchen, K., Myer, G.D. (2018). Pilot Randomized Trial of Integrated Cognitive-Behavioral Therapy and Neuromuscular Training for Juvenile Fibromyalgia: The FIT Teens Program. Journal of Pain, 19, doi:10.1016/j.jpain.2018.04.003.View
Tran, S.T.; Guite, J.W.; Pantaleao, A.; Pfeiffer, M.; Myer, G.D.; Sil, S.; Thomas, S.M.; Ting, T. v.; Williams, S.E.; Edelheit, B.; et al. (2017). Preliminary Outcomes of a Cross-Site Cognitive– Behavioral and Neuromuscular Integrative Training Intervention for Juvenile Fibromyalgia. ArthritisCare and Research, 69, doi:10.1002/acr.22946.View