
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of CAM Research Progress
Journal of CAM Research Progress
Journal of CAM Research Progress Volume 1 (2023), Article ID: JCRP-110
https://doi.org/10.33790/jcrp1100110Research Article
The Analysis of Chinese Medicine Body Constitutions of Polycystic Ovarian Syndrome Patients in Malaysia
Fatima Abadi, Lim Hui Yee, Lim Goon Month, Denise Hung Ting, Sin Yen Suan*
Department of Chinese Medicine, Centre of Complementary and Alternative Medicine, International Medical University, Malaysia.
Corresponding Author: Sin Yen Suan, Department of Chinese Medicine, Centre of Complementary and Alternative Medicine, International Medical University, 126, Jalan Jalil Perkasa 19, Bukit Jalil, 57000 Kuala Lumpur, Malaysia.
Received date: 27th June, 2023
Accepted date: 09th October, 2023
Published date: 10th October, 2023
Citation: Abadi, F., Yee, L.H., Month, L.G., Ting, D.H, & Suan, S.Y. (2023). The Analysis of Chinese Medicine Body Constitutions of Polycystic Ovarian Syndrome Patients in Malaysia. J CAM Research Progress, 2(1):110.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objectives: To identify the most common Chinese medicine body constitution among polycystic ovarian syndrome patients in Malaysia.
Methodology: An online questionnaire including the Constitution in Chinese Medicine Questionnaire, demographic information and medical history, was given to women diagnosed with polycystic ovarian syndrome in Malaysia from the 28th of October 2021 till the 10th of January 2022. The inclusion of participants was strictly controlled through the inclusion and exclusion criteria. Responses from participants were recorded using Microsoft Excel and Statistical Package for Social Sciences version 26 software was used to analyse the data using Pearson’s Chi-squared test and logistic regression analysis.
Results: A total of 135 women with PCOS were included in data analysis. The most common body constitution was found to be Qi stagnation constitution (23.7%), followed by Qi deficiency constitution (20%) and neutral constitution (13%). Qi stagnation constitution was associated with age, stress, depression and headaches during menstruation. Neutral constitution had a negative relationship with stress.
Conclusion: The most common body constitution among PCOS patients in Malaysia is Qi stagnation constitution. Patients who were Qi stagnation constituted most frequently combined with Qi deficiency. Further research is needed to determine the associated factors of this main constitution.
Keywords: Polycystic ovarian syndrome; questionnaire; body constitution; Chinese medicine; Malaysia.
Introduction
Polycystic ovary syndrome (PCOS) is an endocrine disorder affecting women of reproductive age. PCOS was originally termed Stein-Leventhal Syndrome after the two doctors responsible for its discovery; In 1935, a report by Drs Irving Stein and Michael Leventhal, published in the American Journal of Obstetrics and Gynaecology titled “Amenorrhoea Associated with Bi-Lateral Polycystic Ovaries”, kickstarted research into the condition we know today as PCOS [1]. The report was the first of its kind to connect the disorders of polycystic ovaries, hirsutism and amenorrhoea to one syndrome and provided readers with an outline of the disease [2]. Today, the prevalence rate of PCOS among women is estimated to be anywhere from 4 to 21% [3], depending on the country and diagnostic criteria used.
PCOS is a heterogenous condition characterised by hyperandro genism, polycystic ovaries and menstrual irregularities which manifest as oligomenorrhea/amenorrhea, difficulty conceiving, obesity, acne, hair loss and hirsutism [4]. It is considered to result from a combination of genetic, metabolic, foetal, and environmental factors [5] with the main pathogenesis being functional ovarian hyperandrogenism [6,7] and insulin-resistant hyperinsulinism, but still not yet fully understood. With the absence of full understanding of the pathogenesis in Western medicine, no cure currently exists, with the main goal of treatment being to improve and manage signs and symptoms, but there are a variety of treatment options available including lifestyle modifications, metformin and combined oestrogen-progestin oral contraceptives (COCs) [8,9]. However, due to an array of factors, many women have turned to complementary and alternative medicine such as Chinese medicine for relief from their condition [10,11].
PCOS is classified under diseases such as “infertility”, “amenorrhoea”, “delayed menstruation” and “obesity” according to its clinical manifestations in Chinese medicine perspective [12,13]. Chinese medicine treatment has been proven to be effective in treating and managing PCOS [14-17] but questions surrounding the aetiology and pathogenesis remain. Treatment in Chinese medicine is mainly based on syndrome differentiation which concludes the aetiologies and pathogenesis of the disease. Given its varied clinical manifestations, a review [18] of 181 articles found there to be 90 original syndrome differentiations for PCOS in Chinese medicine with the top syndromes being Kidney deficiency, phlegm-dampness accumulation, blood stasis syndrome and Liver Qi stagnation.
One solution to the many questions around the pathogenesis of PCOS in Chinese medicine and its many syndromes could be the identification of the main body constitution in traditional Chinese medicine (TCM) of women diagnosed with PCOS. In Chinese medicine, a patient’s body constitution (BC) refers to the innate, relatively stable acquired disposition of an individual throughout their life which is closely correlated to the syndrome differentiation and treatment formulation [19]. Chinese medicine theory considers BCs as the internal determinants of occurrence, development, and prognosis of a disease. The knowledge of this main constitution could assist in the Chinese medicine diagnosis of PCOS to further investigate the treatment principles and management of PCOS patients. Some authors believe the identification of BC can help in the prevention of PCOS by providing interventional treatments to susceptible BCs [20,21]. In 2009, the Constitution in Chinese Medicine Questionnaire by Wang Qi was implemented as a TCM health screening program in China by the National Public Health Service. The questionnaire describes and provides a basis for the identification of nine BCs [19]; neutral, Qi deficiency, Yang deficiency, Yin deficiency, phlegm dampness, damp-heat, blood stasis, Qi stagnation and intrinsic constitution.
Given the high prevalence of PCOS, it is critical that efforts be made to identify the best possible treatment options as well as prevention methods. However, in order to investigate these possibilities, the main BC must be identified. Currently, no relevant research on the Malaysian population has been done.
Materials and Methods
Study design, duration and settings
This cross-sectional study was conducted between the 28th of October 2021 and 10th of January 2022 through snowball sampling via Google Forms and hard copy of the questionnaire, depending on patient preference. Female patients aged between 18 to 50, of Malaysian nationality, who had been diagnosed with PCOS and agreed to participate were recruited into the study.
The survey used in this study included the participants’ demographic background, medical history, and the Constitution in Chinese Medicine Questionnaire (CCMQ). Microsoft Excel was used to build up the database of results and further analysis was done using Statistical Package for Social Sciences version 26 software (SPSS V.26.0) (IBM, Armonk, NY, USA).
Recruitment of participants
Participants were recruited from online PCOS forums and Chinese medicine centres located in Selangor and Kuala Lumpur, Malaysia from 28th October 2021 to 20th January 2022, namely IMU Chinese Medicine Centre, Xi Fertility TCM Centre and Sunway TCM Centre. Consent forms were obtained from all participants either through the online form or written copies. Patients were not excluded based on taking Western medication, but they were required to include details of their medication history in the demographic record sheet.
The diagnostic criteria of PCOS were based on the 2003 Rotterdam criteria and AES definition 2008 which requires the presence of two of the three findings below.
I. Hyperandrogenism (clinical or biochemical)
II.Ovulatory dysfunction
III. Polycystic ovaries on ultrasound screening
Participants were not required to provide proof of diagnosis for inclusion into this study.
Inclusion and exclusion criteria
Inclusion criteria:
I. Female aged 18-50 years old;
II. Malaysian citizen;
III. Willing to participate;
IV. Diagnosed with PCOS;
Exclusion criteria:
I. Patients who refuse to participate;
II. Participant who does not meet the inclusion criteria;
III. Patients diagnosed with conditions such as hypogonadotropic hypogonadism, premature ovarian failure, ovarian tumours, congenital adrenal hyperplasia, androgen-secreting tumour, Cushing’s syndrome, uterine disorders, or chromosomal abnormalities;
IV. Patient with mental disorder;
V. Pregnant or menopausal patients;
VI. Incomplete questionnaires.
Sample size calculation
The adequate sample size required for the study was estimated using the following formula [22,23] as stated in Figure 1, where n is the sample size, Z is the z-score corresponding to the confidence interval, P is the expected prevalence of the disease and d is the level of precision. For the purpose of this study, Z was taken as 1.96 corresponding to a 95% confidence interval, P was determined to be 0.126 following the results of a study [24] estimating the prevalence of PCOS to be 12.6% and d was set to 0.05; giving rise to a sample size of 169 participants (Figure 2).

Figure 1: Formula used for sample size calculation.

Figure 2: Sample size calculation.
Design of questionnaire
The survey form consisted of patient's consent form, demographic, and Questionnaire of body constitution in Chinese Medicine. In accordance with the protocol of International Medical University (IMU), approval by the IMU Joint-Committee on Research and Ethics 2021 was sought (Project ID: BCM I-2021 (10)) prior to the recruitment of participants and recorded consent was collected from all participants. The data collected was kept private and confidential. Demographic information obtained included patient's general information, such as name, age, occupation, gynaecological history, medication history and laboratory test results.
The questionnaire used for BC classification strictly adhered to Prof Wang Qi's Constitution in Chinese Medicine Questionnaire25,26, which is a globally standardised questionnaire widely used in clinical research. Participants in this study had the option of taking the questionnaire in Chinese, English, or Malay. The Chinese questionnaire was adopted from the globally standardized version developed by Prof. Wang Qi, while the English and Malay questionnaires were reviewed and validated by two registered TCM practitioners in Malaysia who excel in these three languages. Prior to the study, all participants and researchers were required to sign a written consent form.
A pilot study was conducted in which 30 people, including 10 individuals proficient in Malay language and 4 Chinese medicine practitioners, provided feedback on the questionnaire's language, grammar, and accessibility. Based on the feedback, changes were made to the questionnaire's language, and images were added to help the subject understand the questions.
Calculation of Body Constitution
A 5-point Likert scale was applied to each question within the Constitution in Chinese Medicine Questionnaire; the raw score for each section was converted to conversion score based on the formula: Conversion score (%) = (original score-number of questions) × 100 / (number of questions × 4). For non-neutral constitutions, a conversion score ≥40 was considered “yes”, scores between 30-39 were considered as a “tendency” and a score of <30 was considered “no”. For neutral constitution, the neutral conversion score must be ≥60 and conversion scores of all 8 non-neutral constitutions <30 for “yes”, neutral conversion score ≥60 and all 8 non-neutral constitutions scores 30-39 were considered as “tendency”; if above criteria are not met, the patient is not a neutral constitution. Due to this study’s small sample size, limitations in data analysis, and recommendations made by authors [20,21,27,29] of similar studies, the BC with the highest score was assigned as each person's main BC; an exception was made where the neutral constitution was the highest score but the remaining 8 constitution scores were above 30, in which case the second highest BC was assigned as the main.
Data extraction and analysis
The original data was carefully checked to ensure the absence of missing or incorrect information; data from participant who did not meet the inclusion criteria as well as incomplete questionnaires done by participants were excluded from analysis. Microsoft Excel was used to calculate the conversion scores of each BC and build the database for extracted data. SPSS V.26.0 software was used for analysis. Frequency analysis, Pearson’s chi-square test and logistic regression analysis were used to analyse the distribution of BC in Chinese medicine among PCOS patients. Due to the small sample size, certain predictor and outcome variables were merged to allow for more accurate data analysis. P<0.05 indicated the statistical significance of differences.
Results
A total of 169 women claiming to have been diagnosed with PCOS were recruited into this study. Of the 169 participants, 8 women were excluded due to pregnancy, 1 woman due to menopause, 9 due to unconfirmed diagnosis of PCOS, 3 due to admission of mental disorders that could affect their ability to answer the questionnaire, 10 due to diagnosis of associated disorders previously mentioned in the exclusion criteria and 3 due to incomplete information. The final number of participants included in data analysis was 135 patients.
The demographic and lifestyle characteristics can be found in Table 1. The mean age of the participants included in this study was 30.87 years, with the youngest participant being 18 years old, the eldest being 49 years of age and 39% being between the ages of 31 and 35 years. Of the 135 participants, 46% had a BMI considered obese under Centre for Disease Control standards [29], 42% were of the Malay race, 67% held a diploma or bachelor's degree and 60% were married.
Calculations according to the initial criteria set forth by Wang Qi (Table 2) showed the presence of a high number of mixed BCs (79%) among the patients, ranging from 2 to 8 BCs per person. Of the single BC types, neutral constitution was the most common (13%) followed by Qi deficiency (2%), Qi stagnation (1%) and Yin deficiency (1%). The distribution of BCs amongst the 135 patients shows the most common BC to be Qi stagnation (24%), followed by Qi deficiency (20%), neutral (13%), Yang deficiency (10%), damp-heat (9%), Yin deficiency (7%), phlegm-dampness (7%), intrinsic (7%) and blood stasis (4%) respectively. The full distribution of BCs can be found in Table 3 and Figure 3.
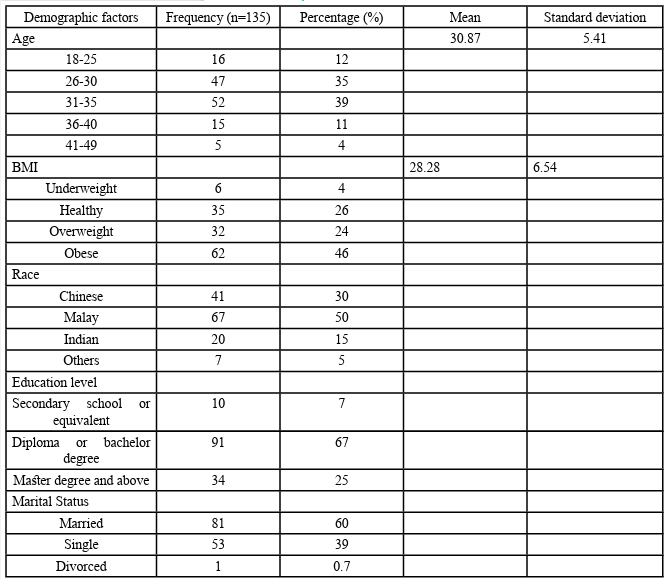
Table 1. Demographic and lifestyle characteristics of patients with polycystic ovarian syndrome in Malaysia

Table 2. Distribution of mixed constitutions among polycystic ovarian patients in Malaysia
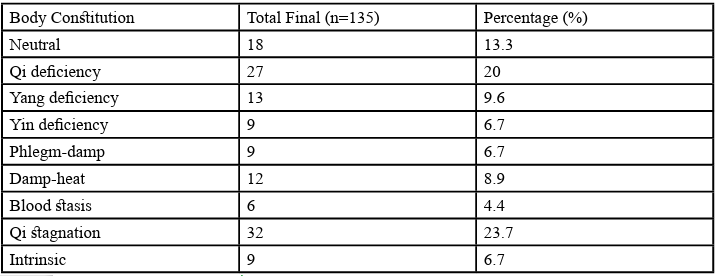
Table 3. Distribution of body constitutions among polycystic ovarian syndrome patients in Malaysia

Figure 3. Pie chart of distribution of body constitutions among polycystic ovarian syndrome patients in Malaysia
Through analysis of the frequency of BCs associated with the most common BC in the original mixed BC model, it was found that Qi stagnation (Table 5) overlapped the most with Qi deficiency body constitution, followed by phlegm-dampness and damp-heat. Analysis of the second most common body constitution, Qi deficiency (Table 6), found that Qi deficiency mostly overlapped with Qi stagnation, Yin deficiency and damp-heat. It is not possible for other biased constitutions to appear in a patient with neutral constitution as the identification of neutral constitution requires a conversion score of less than 3 in all other constitutions.
This study also used Pearson’s chi-squared test (Table 7) to analyse the association between BMI, age range and each of the 9 BCs, compared with all other 8; e.g. neutral constitution and non-neutral constitutions with BMI. No relationship of statistical significance (p<0.05) was found in the analysis of BC and BMI but a statistical significance was found in the chi-squared analysis of age range and BC, showing a statistically significant difference between age and neutral constitution (p=0.012), phlegm-dampness constitution (p=0.020) and Qi stagnation constitution (p=0.042). A statistically significant difference was also noted between Qi stagnation and stress and depression (Table 8).
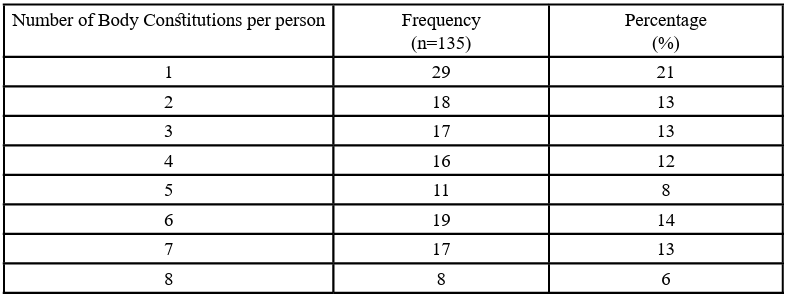
Table 4. Number of mixed body constitutions per person

Table 5. Frequency analysis of the body constitutions coexisting with Qi stagnation as the main body constitution
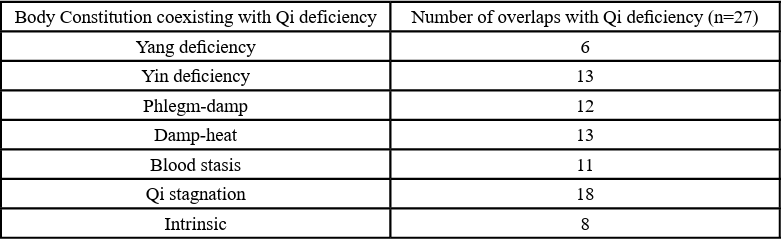
Table 6. Frequency analysis of the body constitutions coexisting with Qi deficiency as the main body constitution
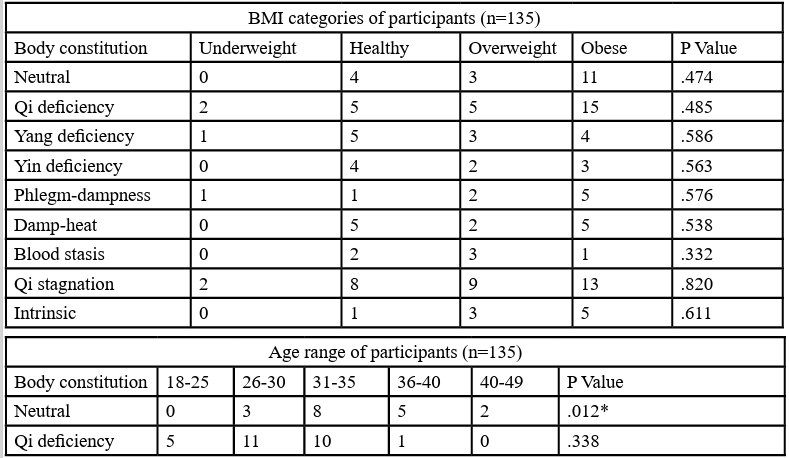
Table 7. Chi-squared analysis of BMI and age range against body constitutions individually
Table 8. Chi squared test of Qi stagnation constitution demographic factors among PCOS patients in Malaysia in comparison with non-Qi stagnation constitutions
The responses of the top 3 body constitutions, Qi stagnation, Qi deficiency and neutral constitution were further analysed individually using logistic regression analysis (Table 9 and 10), setting the absence of that body constitution as the reference. (In analysing the aetiology and associated symptoms of neutral constitution, all non-neutral constitutions were set as the reference values). For Qi stagnation a statistical difference was noted relative to non-Qi stagnation body constitutions in regards to headaches during menses (B=1.038), being of Malay race (B=-3.796), Indian race (-3.640) and age (B= 2.140). For Qi deficiency constitution, a statistically significant difference was shown in regards to being of Indian (B=17.634) or Chinese race (B=17.279) and having symptoms of diarrhoea during menses (B=1.270). For neutral constitution, a statistical significance was noted for feeling stressed (B=-3.048), depressed (B=-3.369) and having lumbar soreness (B=-2.548) symptoms during menses.

Table 9. Logistic regression analysis of demographic details of the top 3 body constitutions of PCOS patients in Malaysia
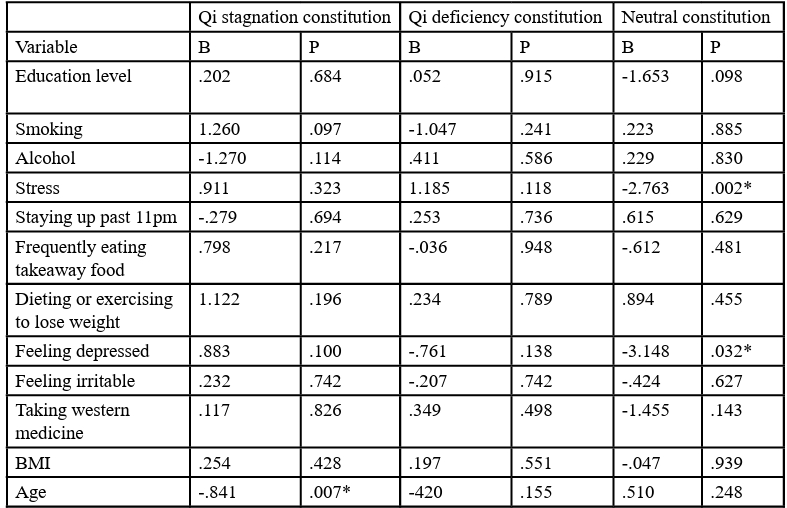
Table 10. Logistic regression analysis of associated menstrual symptoms of the top 3 body constitutions of PCOS patients in Malaysia
Discussion
Despite the magnitude of research into the aetiology and pathogenesis of PCOS from both the Chinese medicine and Western medicine perspectives, many questions remain, and the complexity of the clinical manifestations of PCOS as well as its broad diagnostic criteria can be understood as the reason for the many unanswered questions. This study found a high percentage (79%) of PCOS patients in Malaysia with mixed body constitutions, ranging from 1 to 8 body constitutions per person. Although this may appear peculiar from a research standpoint, it is consistent with previous research into Chinese medicine body constitutions and the manifestations of PCOS in a clinical setting. Due to the diverse, complex clinical manifestations of PCOS, there has been a unified consensus among researchers about the heterogeneity of the syndrome differentiation of PCOS patients [12]. As body constitution has been explained as the foundation of syndrome differentiation, with the existence of combined Chinese medicine syndromes in PCOS patients, the presence of a high number of mixed constitutions in this study is not atypical.
Following in the footsteps of similar studies [20,21,27,28], after assigning the highest-scored body constitution for each patient as their main body constitution, frequency analysis showed Qi stagnation to be the most common main constitution. According to the theories of Ye Tianshi, the Liver is the innate organ of women and women naturally have more Liver-like tendencies [12]. Therefore, difficulty in controlling the seven emotions is more likely to harm the Liver in women and cause the stagnation of Liver Qi as the Liver fails to control the free flow of Qi. Previous research has also suggested women have a greater tendency towards Qi stagnation than men.30 In relation to PCOS, several studies have shown Qi stagnation to be one of the most common syndrome differentiations of polycystic ovarian syndrome [18,21,31-34]. A review of the most common formula prescribed for treating PCOS in Taiwan was found to be Jia Wei Xiao Yao San (Augmented Rambling Powder), for dispersing Liver Qi [35]. Stagnation of Liver Qi disrupts the normal flow of Qi and blood, which is essential for regular menstruation and fertility. This condition can lead to delayed menstruation, amenorrhea, and infertility, along with a depressed emotional state and irritability. All of these are the clinical findings of the main criteria for PCOS.
Frequency analysis of the associated body constitutions of Qi stagnation constitution identified Qi deficiency constitution to be associated with Qi stagnation in 28 of the 32 cases. A China-based study36, on the correlation between body constitution and syndrome differentiation, found the second most common body constitution in PCOS patients, Qi stagnation and Qi deficiency, was associated with Liver Qi stagnation syndrome and Kidney deficiency syndrome occurring concurrently. Therefore, the finding of this common combination within PCOS patients in Malaysia is consistent with previous understanding of PCOS and the results of similar studies.
While the logistic regression model did not show a statistically significant relationship between Qi stagnation and stress or depression, the chi-squared test did show a significant connection. This finding is consistent with the Chinese medicine understanding of Qi stagnation, where the Liver controls the free flow of Qi and balances emotions. When the free flow of Qi is affected, the Liver is unable to balance emotions and emotional abnormalities such as depression and inability to handle stress occur. This is agreeable with the findings of similar studies [30] where Qi stagnation constitution was positively associated with the risk of depression. The logistic regression model noted a negative correlation between individuals of Indian and Malay race, and Qi stagnation constitution, compared to other constitutions. This may be related to factors like differing stress levels, mental health trends, access to coping mechanisms, and help seeking behaviours among different racial groups [37]. However, the available studies in this area are limited, making it challenging to draw conclusions regarding this relationship.
Albeit not the main objective of this study, queries into the associated symptoms of the top 3 body constitutions were also made. Findings suggest there is a statistically significant relationship between Qi stagnation constitution and menstrual headaches, Qi deficiency constitution and diarrhoea and neutral constitution and lumbar soreness. An analysis [38] of Qi stagnation constitution and premenstrual syndrome in China found headaches to be the complaint of 73% of the women, of which the majority 28% had Qi stagnation constitution. The occurrence of menstrual headaches has been attributed by many practitioners to be the result of Qi stagnation [39]. Qi stagnation can develop into Liver Yang hyperactivity or blood stasis over time, which leads to fire rising and attacking the head or the obstruction within the vessels which deprives the head of nutrition, respectively, both of which lead to pain. Furthermore, as Qi deficiency constitution can easily turn into Spleen deficiency [25], and Spleen is the site of transportation and transportation of water and grain, when there is a deficiency of Spleen Qi, the transport and transportation function is disturbed and the water and grain will stagnate into phlegm, leading to the occurrence of diarrhoea during menstruation more in women with Qi deficiency constitution [40].
Investigations into the associations among the patients with neutral constitution mainly found negative correlations between stress and lumbar soreness during menstruation. According to Prof. Wang, people with neutral body constitution have stronger environmental adaptability as well as greater emotional and mental stability and are less likely to encounter illness. This can be interpreted as those with neutral constitution being less likely to perceive themselves as stressed and having better control over their emotions compared with individuals with unbalanced body constitutions. As those with neutral constitution have stronger constitution, they were also less likely than other constitutions to experience adverse menstrual symptoms. However, despite this, the neutral constitution was still the 3rd most common constitution among PCOS patient in Malaysia. While this may seem contradictory with the theories of body constitution, the neutral constitution has shown a high prevalence in patients with hypertension, impaired glucose regulation and dysmenorrhea in other body constitution studies [41-43]. This implies that having neutral constitution cannot be considered as an exemption from diseases, however, it is possible [41] that diseased individuals with neutral constitutions may have better survival rates and less severe forms of their condition. Nonetheless, a quantitative measurement method for the severity of PCOS must be identified to test this hypothesis in women with PCOS in Malaysia.
Conclusion
This study was able to recruit a total of 135 participants of diverse backgrounds and races. Qi stagnation was found to be the most common body constitution, followed by Qi deficiency and neutral constitution. Qi stagnation was most associated with Qi deficiency among these patients. As the first study of its kind into the body constitutions of PCOS patients in Malaysia, this research was able to identify the body constitutions of PCOS patients in Malaysia while presenting ideas for the associations and relationships of these constitutions.
However, this study had limitations due to the small sample size, which did not meet the initial proposed sample size. Many of the associated factors and symptoms, such as stress, depression, irritability, and pain, were only questioned using "yes/no" questions, which raises concerns about the validity of the relationships identified and necessitates further research into these factors.
Acknowledgements
A main source of struggle throughout this research was reaching the required sample size. I would also like to express my most sincere gratitude to the physicians at Sunway TCM Centre and Xi Fertility Centre for allowing us to reach out to their patients to participate in this research. I would especially like to thank the clinical assistants and part timers at Xi Fertility who despite their busy schedules and workload did their best to help us find and contact patients. A very special thank you to Deena Marzuki at “mypcosiloveyou” as well, who contributed a great deal to this research by promoting our questionnaire to her followers.
And finally, thank you to the many women who took the time out of their day to fill in our lengthy questionnaire. I wish the very best in health for all of you.
Funding
This research received funding from International Medical University as approved by the IMU Joint-Committee on Research and Ethics (project ID:BCM I-2021(10))
Ethics statement
This study has been approved by IMU Joint-Committee on Research and Ethics on 28 October 2021 under project ID:BCM I-2021(10). (Attached the confirmation of approval letter)
List of abbreviations
1. PCOS: Polycystic ovarian syndrome 2. TCM: Traditional Chinese medicine 3. CCMQ: Constitution in Chinese Medicine Questionnaire 4. CHM: Chinese Herbal Medicine 5. FSH: Follicle Stimulating Hormone 6. BC: Body Constitution
References
Stein, I.F., & Leventhal, M.L. (1935). Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol. 29(2):181-91. DOI: 10.1016/S0002-9378(15)30642-6View
Azziz, R., & Adashi, E.Y. (2016). Stein and Leventhal: 80 years on. Am J Obstet Gynecol. 214(2):247.e1-247.e11. DOI: 10.1016/j.ajog.2015.12.013View
Lizneva, D., Suturina, L., Walker, W., Brakta, S., Gavrilova Jordan, L., & Azziz, R. (2016). Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil Steril. 106(1):6–15. DOI: 10.1016/j.fertnstert.2016.05.003View
Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004 Jan; 19(1):41-7. DOI: 10.1093/ humrep/deh098View
Dumesic, D.A., Oberfield, S.E., Stener-Victorin, E., Marshall, J.C., Laven, J.S., & Legro, R.S. (2015). Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr Rev. 36(5):487-525. DOI: 10.1210/er.2015-1018View
Ehrmann, D.A., Barnes, R.B., & Rosenfield, R.L. (1995). Polycystic ovary syndrome as a form of functional ovarian hyperandrogenism due to dysregulation of androgen secretion. Endocr Rev. 16(3):322-353. DOI: 10.1210/edrv-16-3-322View
Rosenfield, R.L., & Ehrmann, D.A. (2016). The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr Rev. 37(5):467-520. DOI: 10.1210/er.2015-1104View
Mahoney, D. (2014). Lifestyle modification intervention among infertile overweight and obese women with polycystic ovary syndrome. J Am Assoc Nurse Pract. 26(6):301-8. DOI: 10.1002/2327-6924.12073View
Lord, J.M., Flight, I.H., & Norman, R.J. (2003). Insulin sensitising drugs (metformin, troglitazone, rosiglitazone, pioglitazone, D-chiro-inositol) for polycystic ovary syndrome. Cochrane Database Syst Rev. (3):CD003053. DOI: 10.1002/14651858.CD003053. Update in: Cochrane Database Syst Rev. 2009;(3):CD003053View
Shen, W., Jin, B., Pan, Y., Han, Y., You, T., Zhang, Z., et al. (2021). The Effects of Traditional Chinese Medicine-Associated Complementary and Alternative Medicine on Women with Polycystic Ovary Syndrome. Evid Based Complement Alternat Med. 2021: 6619597. DOI: 10.1155/2021/6619597View
Arentz, S., Smith, C.A., Abbott, J.A., & Bensoussan, A. ( 2014). A survey of the use of complementary medicine by a self selected community group of Australian women with polycystic ovary syndrome. BMC Complement Altern Med. 14:472. DOI: 10.1186/1472-6882-14-472View
Lin, L., Lin, Q. (2012). Clinical research on regular of TCM syndrome elements of polycystic ovary syndrome. Journal of Gansu College of Traditional Chinese Medicine. 29(06):45-8. DOI: CNKI:SUN:GSZX.0.2012-06-021
Yang, H.P. (2017). The Combination of Chinese Traditional Medicine and Western Medicine Is More Effective on the Therapy of Polycystic Ovary Syndrome in Patients with Kidney Deficiency and Liver Stagnation [Master’s Thesis]. China: Anhui University of Traditional Chinese Medicine; Available from: https://kns.cnki.net/KCMS/detail/detail.aspx?dbname=C MFD201801&filename=1017199382.nhView
Zhou, K., Zhang, J., Xu, L., Lim,C.E.D. (2021). Chinese herbal medicine for subfertile women with polycystic ovarian syndrome. Cochrane Database Syst Rev. 6(6):CD007535. DOI: 10.1002/14651858.CD007535.pub4View
Hu, J., Shi, W., Xu, J., Liu, S., Hu, S., Fu, W., et al. (2021). Complementary and Alternative Medicine for the Treatment of Abnormal Endometrial Conditions in Women with PCOS: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid Based Complement Alternat Med. 2021:5536849. DOI: 10.1155/2021/5536849View
Peng, D.M. (2020). Study on the Effect of Warming Needle Moxibustion in Treating Patients with Pcos Infertility with Kidney Deficiency, phlegm and Blood Stasis Syndrome [Master's Thesis]. China: Guangzhou University of Traditional Chinese Medicine. Available from: https://tra.oversea.cnki. net/KCMS/detail/detail.aspx?dbname=CMFDTEMP&filena me=1021022858.nh
Wooltorton, E. (2003). Diane-35 (cyproterone acetate): safety concerns. CMAJ. 168(4):455–6. PMID: 12591790; PMCID: PMC143555View
Shi, M.Y., Zhao, Y., & Wang, T.F. (2014). Literature Research on TCM Syndrome and Syndrome Elements Distribution Pattern of Polycystic Ovary Syndrome. World Chin Med. 9(12). DOI: 10.3969/j.issn.1673-7202.2014.12.030
Sang, X.X., Wang, Z.X., Liu, S.Y., & Wang, R.L. (2018). Relationship Between Traditional Chinese Medicine(TCM) Constitution and TCM Syndrome in the Diagnosis and Treatment of Chronic Diseases. Chin Med Sci J. 33(2):114-119. DOI: 10.24920/21806View
Yang, J.W. (2012). Clinical Investigation about the Relevance of Polycystic Ovarian Syndromes and the Chinese Constitution Types [Master’s Thesis]. China: Guangzhou University of Traditional Chinese Medicine. Available from: https://kns.cnki. net/KCMS/detail/detail.aspx?dbname=CMFD2011&filena me=1011135602.nhView
Li, R., Fu, J., Du, L., Yu, S., & Xu, M. (2013). Survey of Distribution Characteristic of Traditional Chinese Medicine Constitution in Patients with Polycystic Ovary Syndrome. China J Chin Med. 28(8):1192-3. DOI: 10.16368/j.issn.1674 8999.2013.08.016
Pourhoseingholi, M.A., Vahedi, M., & Rahimzadeh, M. (2013). Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 6(1):14–7. PMID: 24834239; PMCID: PMC4017493.View
Daniel, W.W., Cross, C.L, editors. (2013). Biostatistics: a foundation for analysis in the health sciences. 10th ed. UK: John Wiley and Sons Inc.View
Dashti, S., Abdul, Latiff L., Abdul, Hamid H., Mohamad Saini S., Shah Abu Bakar A., Binti Sabri NAI., et al. (2019). Prevalence of Polycystic Ovary Syndrome among Malaysian Female University Staff. J Midwifery Reprod Health. 7(1):1567 1575. DOI: 10.22038/jmrh.2018.30370.1329View
Wang, Q. (2006). Primary compiling of the Constitution in Chinese Medicine Questionnaire. Chin J Clin Rehabil. 10(3):12 14. Available from: https://cir.nii.ac.jp/crid/1573387450497432 576?lang=en#citations_containerView
China Association of Chinese Medicine. (2009). ZYYXH/T 157-2009. Classification and Determination of Constitution in TCM. Bejing. Available from: https://www.cnki.net/KCMS/ detail/detail.aspx?dbcode=SCHF&dbname=SCHF&filename= schf201005001001&uniplatform=OVERSEA&v=kQJcQGV3 wCNMDePQ_qxE5QF4hJWDpgzYciDQznrYuOOuxEeui0VE w1eNzCZfqDkEJbf9Bf8h3wU%3dView
Lai, N.S., Lu, M.C., Chang, H.H., Lo, H.C., Hsu, C.W., Huang, K.Y, et al. (2021). Association of Traditional Chinese Medicine Body Constitution and Health-Related Quality of Life in Female Patients with Systemic Lupus Erythematosus: A Cross-Sectional Study. Evid Based Complement Alternat Med. 2021:5568219. DOI: 10.1155/2021/5568219View
Jiang, Q.Y., Li, J., Zheng, L., Wang, G.H., Wang, J. (2018). Constitution of traditional chinese medicine and related factors in women of childbearing age. J Chin Med Assoc. 81(4):358 365. DOI: 10.1016/j.jcma.2018.01.005View
Centers for Disease Control and Prevention [Internet]. About Adult BMI. U.S. Department of Health & Human Services. 2021 [cited 2022 Jan 30]. Available from: https://www. cdc.gov/healthyweight/assessing/bmi/adult_bmi/index. html#InterpretedAdultsView
Liu, M., Jiang, Y., Wang, X., Liu, Q., Wu, H. (2017). The Role of Rumination and Stressful Life Events in the Relationship between the Qi Stagnation Constitution and Depression in Women: A Moderated Mediation Model. Evid Based Complement Alternat Med. 2017:7605893. DOI: 10.1155/2017/7605893 View
Yang, Q., Pan, Z., Sun, C., Sun, M., Kuang, H. (2022). Analysis on Regularities of Syndrome Differentiation and Prescription in Treatment of Polycystic Ovary Syndrome with Chinese Medicinals. Shandong J Tradit Chin Med. 41(12):1259-1263. DOI:10.16295/j.cnki.0257-358x.2022.12.001
Wang, X. (2020). Correlation Analysis of Syndrome Type of Traditional Chinese Medicine,Sex Hormone and Metabolic Index in Patients with Polycystic Ovary Syndrome and Insulin Resistance [Master’s Thesis]. China: Heilongjiang University of Traditional Chinese Medicine. DOI: 10.27127/d.cnki. ghlzu.2020.000316
Di, S., Wang, X., Zhang, H., Ma, S. (2017). Research progress on treating PCOS by differentiation syndrome of TCM in recent decade. Glob Tradit Chin Med. Glob Trad Chin Med. 10(09):1143-6. DOI: CNKI:SUN:HQZY.0.2017-09-037
Zhao, N., Yang, Z., Quan, C. (2017). Correlation Analysis of Clinical Classification and TCM Syndrome Type in Polycystic Ovary Syndrome. J Hunan Univ Chin Med. 37(09):966-8. DOI: CNKI:SUN:HNZX.0.2017-09-012.
Liao, W.T., Chiang, J.H., Li, C.J., Lee, M.T., Su, C.C., Yen, H.R. (2018). Investigation on the Use of Traditional Chinese Medicine for Polycystic Ovary Syndrome in a Nationwide Prescription Database in Taiwan. J Clin Med. 22;7(7):179. doi: 10.3390/jcm7070179View
Gao, J., Hou, L., Li, Y., Liu, Y. (2017). Correlation of traditional Chinese medicine syndrome and traditional Chinese medicine constitution in patients with polycystic ovary syndrome. Tianjin J of Tradit Chin Med. 34(9):606-9. DOI: CNKI:SUN:TJZY.0.2017-09-010.
Ting, RS-K., Pei, L.F. (2021). Counseling Chinese Communities in Malaysia: The Challenges and Needs in Mental Health Service Deliverance. Research Anthology on Rehabilitation Practices and Therapy. DOI: 10.4018/978-1-7998-3432-8.ch058View
Wang, L. (2010). Investigation on Female Premenstrual Syndrome of Chinese Syndrome (Deficient Syndrome) Distribution and Relevant Constitution [Doctoral Dissertation]. China: Guangzhou University of Chinese Medicine. Available from: https://oversea.cnki.net/KCMS/detail/detail.aspx?dbcode =CDFD&dbname=CDFD0911&filename=2010125587.nhView
Yu, T. (2021). Clinical Observation of Tongqiaohuexue Decoction Combined with Acupuncture in the Treatment of Qi Stagnation and Blood Stasis Type Menstrual Headache [Master’s Thesis]. China: Heilongjiang University of Traditional Chinese Medicine. DOI: 10.27127/d.cnki.ghlzu.2021.000189
Liu, Y., Bai, S., Ma, J., Wu, F., Wu, Z., Yang, Q., et al. (2015). Research Progress of Functional Diarrhea Treated with Chinese Medicine. J Liaoning Univ Tradit Chin Med. 17(2):78-80. DOI: 10.13194/j.issn.1673-842x.2015.02.028
Zhu, Y., Shi, H., Wang, Q., Wang, Y., Yu, X., Di, J., Zhang, X., Li, Y., Li, T., & Yan, H. (2017). Association between Nine Types of TCM Constitution and Five Chronic Diseases: A Correspondence Analysis Based on a Sample of 2,660 Participants. Evid Based Complement Alternat Med. 2017:9439682. doi: 10.1155/2017/9439682View
You, H., Zhang, T., Feng, W., Gai, Y. (2017). Association of TCM body constitution with insulin resistance and risk of diabetes in impaired glucose regulation patients. BMC Complement Altern Med. 17(1):459. doi: 10.1186/s12906-017-1964-0View
Chong, T.F., Ser, X.E., Ooi, L.K. et al. (2018). Body constitution and dysmenorrhea: a study on university students in Malaysia. Orient Pharm Exp Med. 18(4):377–80. DOI: 10.1007/s13596 018-0328-8View