
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 8 (2023), Article ID: JCNRC-191
https://doi.org/10.33790/jcnrc1100191Research Article
Examination of the Medical Error Tendencies of Midwives and Nurses Working in Maternity Clinics
Sevda Karakaş1, Özlem Şahan2, Rukiye Höbek Akarsu3*, and Rabia Atilla4
1Assistant Proffesor, Department of Nursing, Faculty of Health Sciences, İstanbul Arel Üniversity, İstanbul, Turkey.
2Assistant Proffesor, Department of Midwifery, Faculty of Health Sciences, Antalya Bilim Üniversitesi, Antalya, Turkey
3Associate Proffesor, Department of Nursing, Faculty of Health Sciences, Yozgat Bozok Üniversitesi, Turkey.
4Assistant Proffesor, Department of Nursing, Faculty of Health Sciences, Niğde Ömer Halisdemir Üniversitesi, Turkey.
Corresponding Author Details: Rukiye Höbek Akarsu, Associate Proffesor, Department of Nursing, Faculty of Health Sciences, Yozgat Bozok Üniversitesi, Turkey.
Received date: 05th October, 2023
Accepted date: 15th November, 2023
Published date: 17th November, 2023
Citation: Karakaş, S., Şahan, Ö., Akarsu, R.H., & Atilla, R., (2023). Examination of the Medical Error Tendencies of Midwives and Nurses Working in Maternity Clinics. J Comp Nurs Res Care 8(1):191.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Aim: This research was conducted descriptively to determine the medical error tendencies of midwives and nurses working in maternity clinics and the factors affecting them.
Materials and Methods: The sample of the study consisted of 135 midwives and nurses who agreed to participate in the study between January 2022 and February 2023. The Medical Error Tendency Scale in Nursing (METSN) and a descriptive information form developed by the researchers in line with the literature were used for data collection. Kruskal-Wallis and Mann-Whitney U tests were applied for data analysis.
Results: The average age of the midwives and nurses participating in the study was 28.88±6.0 years, and the average duration of work was 5.84±5.9 years. It was determined that 25.4% of midwives and nurses made medical errors, and 57.8% witnessed medical errors. The mean total score of METSN was 226.20±31.78 (min-max: 126-245), and the mean scores of the sub-dimensions of the scale were determined as 84.27±10.23 for the "Medication and Transfusion Practices" sub-dimension, 55.30±9.88 for the "Prevention of Infections" sub dimension, 22.82±4.36 for the "Prevention of Falls" sub-dimension, 40.93±6.12 for the "Patient Monitoring and Material Device Safety" sub-dimension, and 22.87±4.38 for the "Communication" sub dimension.
Conclusion: In our study, it was found that one-fourth of midwives and nurses made medical errors, and the risk of making medical errors was higher in midwives and nurses who had previously made medical errors and witnessed medical errors. The high rates of medical error tendencies and witnessing medical errors detected in our study indicate that there is a high tendency for medical errors in maternity clinics.
Keywords: Midwife; Nurse; Obstetrics; Childbirth; Medical error; Medical error tendency.
Introduction
Maternity clinics are units where patient circulation and workload are intense, unexpected emergencies can occur in both the mother and the baby, and numerous invasive procedures are performed. It is known that medical errors are most commonly observed in maternity clinics in our country and worldwide [1-3]. While gynecologists rank first in medical malpractice claims in gynecology clinics, nurses and midwives rank second. Due to the fact that midwives and nurses carry out many practices related to patient care and medical treatment in maternity clinics, they encounter a higher risk of making medical errors compared to other healthcare professionals [4].
According to the World Health Organization (WHO), approximately 134 million medical errors occur each year in low- and middle income countries due to unsafe healthcare services, resulting in the deaths of 2.6 million people due to medical errors [5]. The report by the WHO states that the frequency of medical errors ranges from 3.2% to 16.6% in countries such as Australia, Canada, the United Kingdom, New Zealand, the United States and Denmark [6]. It is known that the rate of medical errors in Turkey is approximately 16.6% and that the rate of midwives and nurses being sued due to medical errors has increased by 10% in the last four years, and the leading medical errors are incorrect drug administration [1,7].
The main medical errors reported in studies in the literature include medication errors, hospital-acquired infections, diagnostic errors, errors resulting from inadequate patient monitoring, falls, errors resulting from lack of communication, errors due to incorrect or inappropriate material use, and treatment errors [2,7,8]. In a study conducted by White et al. in 2005, the most common reasons for medical errors in maternity clinics were reported to be inadequate diagnosis, treatment, and communication [9].
The frequency of malpractice lawsuits related to pregnancy follow-up and childbirth continues to increase. In Turkey, 30% of the files consulted by the Institute of Forensic Medicine are related to obstetrics and 90% of these are related to pregnancy follow-up and childbirth [10]. Midwives and nurses, who play an active role in the follow-up of pregnancy and childbirth, have the responsibility to provide quality and safe healthcare services covering the mother, fetus, and newborn. The most fundamental approach in delivering quality and safe healthcare services is to prevent medical errors [3,11].
Medical errors that occur in maternity clinics can result in irreversible conditions such as death and disability. In order to achieve the goal of "Zero Medical Errors" in healthcare services, it is important to carry out healthcare practices and make complete notifications of medical errors, as well as to investigate the root causes of reported medical errors [8,12,13]. This study was conducted to determine the level of medical error tendencies and the factors affecting medical error tendencies of midwives and nurses working in maternity clinics, where the risk of making medical errors is high.
Materials and methods
Purpose of the research
This research was conducted to determine the level of medical error tendencies and the factors affecting medical error tendencies of midwives and nurses working in maternity clinics.
Research Type
The research is of a descriptive type
Study Population and Sample
The study population consisted of all midwives and nurses working in maternity hospitals affiliated with the Ministry of Health in the Marmara region. An attempt was made to reach the entire population before selecting a sample. The sample of the study consisted of 135 midwives and nurses who agreed to participate in the research.
Data Collection Tools
Research data were collected using the "Introduction Information Form" and the "Medical Error Tendency Scale in Nursing."
Introduction Information Form
The introductory information form includes questions about the research topic and socio-demographic characteristics. The introductory information form, developed by the researchers in line with the literature, consists of a total of 9 questions related to medical errors and socio-demographic characteristics, including age, title, education level, duration of working in obstetrics and gynecology clinics, witnessing medical errors, making medical errors, the institution's approach to medical errors, and receiving training on patient safety [2,3,7].
Medical Error Tendency Scale in Nursing
In order to measure nurses' tendencies toward medical errors, the "Medical Error Tendency Scale in Nursing" was developed by Özata and Altunkan in 2010. The scale consists of 49 items and 5 sub-dimensions: drug and transfusion applications (18 items), falls (5 items), hospital infections (12 items), patient monitoring/material safety (9 items), and communication (5 items). The scale is a 5-point Likert type, and expressions are evaluated as follows: 1: never, 2: very rarely, 3: sometimes, 4: mostly, 5: always. The evaluation of the scale is based on the mean score. As the mean score of the scale increases, it indicates that nurses have a low tendency to make medical errors, and as the mean score decreases, it indicates that nurses have a high tendency to make medical errors. The Cronbach's alpha value of the scale was determined as 0.90 by Özata and Altunkan. In this study, the Cronbach's Alpha coefficient was found to be 0.982 for the "Medical Error Tendency Scale in Nursing," 0.970 for the "Drug and Transfusion Applications" sub-dimension, 0.959 for the "Hospital Infections" sub-dimension, 0.931 for the "Patient Monitoring and Material Safety" sub-dimension, 0.937 for the "Falls" sub-dimension, and 0.926 for the "Communication" sub-dimension [14].
Data Collection
In our study, data were collected online (Google Forms) between January 10, 2022, and February 30, 2023. Before the study, a pilot study was conducted with 10 nurses to test the expression and comprehensibility of the data collection tools. Midwife nurses who worked for less than a year in the maternity clinic were not included in the study (n=15).
Ethical Aspect of the Research
In order to conduct the research, ethical approval was obtained from the Istanbul Arel University Ethics Committee (17.12.2021, 2021/17). The research was conducted in accordance with the principles of the Helsinki Declaration. During the online data collection phase using Google Forms, participants' personal information was not visible.
Data Analysis
The data were evaluated using the Statistical Package for Social Sciences (SPSS) 24.0 Windows program, and a significance value of p < 0.05 was accepted. The skewness and kurtosis test was used to analyze the normality distribution of the mean scores and sub dimensions of the Medical Error Tendency Scale in Nursing, and it was determined that the scale and sub-dimensions did not follow a normal distribution. In the analysis of the data, arithmetic mean, frequency, standard deviation, percentage, median, Cronbach Alpha internal consistency analysis, Kruskal-Wallis, and Mann-Whitney U tests were applied.
Results
The descriptive characteristics of nurses and midwives and their experiences related to medical errors are presented in Table 1. It was determined that 77.0% of the midwives and nurses participating in the study were university graduates, 32.6% were midwives and 67.4% were nurses. It was determined that the average working time of midwives and nurses was 5.85±5.9 years. When the participants' experiences regarding medical errors were examined; 77.8% of the participants received patient safety training and 57.8% witnessed a medical error; 25.4% made medical errors; 28.2% stated that the attitude towards medical errors in the institution where they work is a personal approach.
The average total score of the Medical Error Tendency Scale and the average scores for the sub-dimensions of the scale for nurses and midwives are presented in Table 2. When examining the scores of the Medical Error Tendency Scale and its sub-dimensions, it was concluded that the nurses and midwives who participated in the study have a low tendency to make medical errors.
The descriptive characteristics of nurses and midwives, along with their experiences related to medical errors, were compared with the "Medical Error Tendency Scale in Nursing" and its subscale mean scores, as shown in Table 3. There were no significant differences in the "Medical Error Tendency Scale in Nursing," its subscales, titles, the clinics participants worked in, and whether they received patient safety training (p>0.05).
Participants who did not report making medical errors had higher mean scores in the "Medical Error Tendency Scale in Nursing" (U=1165, p=.008), the "Medication and Transfusion Practices" subscale (U=1138, p=.005), the "Hospital Infections" subscale (U=1041, p=.001), the "Falls" subscale (U=1092, p=.001), and the "Communication" subscale (U=1243, p=008) compared to those who reported making errors.
Participants who did not witness medical errors in their workplace had higher mean scores in the "Communication" subscale of the "Medical Error Tendency Scale in Nursing" (U=1763, p=021) compared to those who witnessed errors. However, there was no statistically significant difference in the mean scores of the "Medical Error Tendency Scale in Nursing," the "Medication and Transfusion Practices" subscale, the "Hospital Infections" subscale, the "Patient Monitoring and Material Safety" subscale, and the "Falls" subscale based on whether participants witnessed medical errors in their workplace (p>0.05).
Participants who reported that their institution adopted a systemic approach in the event of a medical error had higher scores in the "Medical Error Tendency Scale in Nursing" (KW=7.69, p=.021) compared to those who reported a personal approach. Additionally, the "Falls" subscale scores (KW=11.70, p=.003) were higher in participants who reported adopting a personal approach and those who reported not having an opinion compared to those who reported a systemic approach.
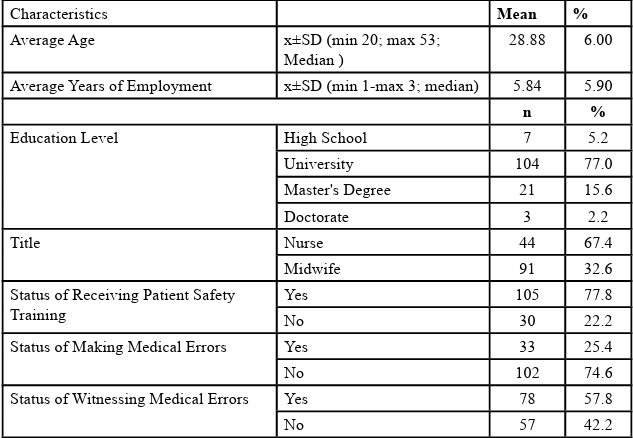
Table 1: Descriptive characteristics of nurses and midwives and their experiences regarding medical errors (n= 135)
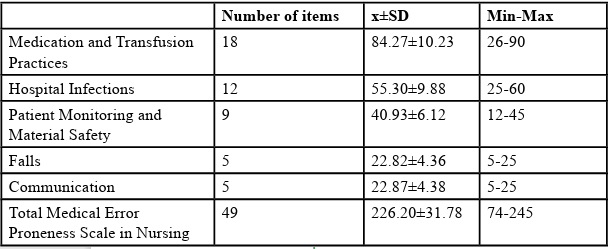
Table 2: Findings regarding the average scores of the Medical Error Tendency Scale and its sub-dimensions for nurses and midwives (n=269)
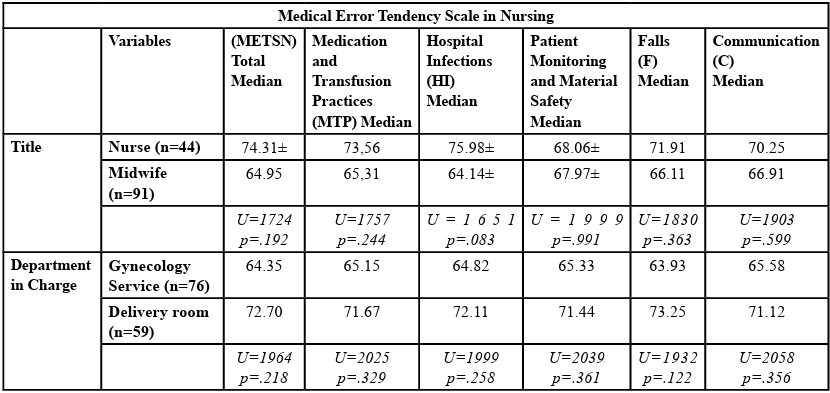
Table 3: Factors affecting the medical error tendencies of nurses and midwives (n=135)
Discussion
Due to the multifaceted and active involvement of nurses and midwives in independent and dependent functions in obstetrics and gynecology clinics, they are more frequently exposed to the risk of medical errors compared to other healthcare professionals [3,4,8,12]. Studies in the literature have reported medical error rates among nurses and midwives to be between 13% and 20% [3,8,15,16]. In our study, it was found that one-quarter of midwives and nurses had committed a medical error (25.4%). Our study's result was higher than the results reported in the literature. The high rate of medical errors in our study might be attributed to the fact that the study was conducted in obstetrics and gynecology clinics with a high risk of medical errors.
Medical errors made during the delivery of healthcare services negatively impact both healthcare workers and the patient and their family. The identification of situations where individuals have witnessed medical errors is also concerning. In studies available in the literature, high rates of witnessing medical errors have been observed. In this study, it was determined that 57.8% of participants had witnessed a medical error. Kandemir and Yüksel's study reported a rate of 46.4%, Kıymaz and Koç's study reported 40.1%, and Özen et al.'s study reported 53.1%. Our study's results are in line with the results reported in the literature. The high rates of witnessing medical errors among healthcare professionals suggest that medical error reporting may be incomplete [8,12,13].
The increase in the total score average obtained from the Medical Error Tendency Scale in Nursing (METSN) indicates a lower tendency for nurses to commit medical errors. In our study, the average total score obtained from the METSN, which we used to determine the level of medical error tendency, was found to be 226.20±31.78. Considering that the total score range that can be obtained from the scale is between 49 and 245, it can be concluded that nurses have a moderate tendency to make medical errors. The result of our study showed similarity with the results reported in the literature. In Özen et al.'s study conducted in 2019, the average total score obtained from the METSN was reported as 223.10±19.51, while Türk et al. reported an average METSN score of 199.59±26, and Baştürk reported an METSN total score of 223.6±12.8 [13,17,18].
In our study, we examined 5 sub-dimensions of the scale, namely medication and transfusion applications, falls, patient monitoring/ material safety, communication, and hospital infections. One of the sub-dimensions of the scale with the lowest overall score (84.27±10.23) in our study was "Medication and Transfusion Practices." This result indicates that nurses have a high tendency to make errors in medication and transfusion practices. Medication errors are the most common type of error that affects patient safety and is largely preventable. In Koçak and Yaman's study, approximately half of the nurses working in obstetrics and gynecology clinics were found to have made a medication error, and the majority of medication errors consisted of wrong drugs, wrong doses, and wrong patient types [19].
Another sub-dimension with a low overall score (40.93±6.12) in our study was "Patient Monitoring, Material, and Device Safety." Similar to our study results, Durmuş et al. (2022) reported an average score of 39.57±6.71 for the "Patient Monitoring, Material, and Device Safety" sub-dimension in their study. It can be said that nurses and midwives have a tendency to make errors in patient monitoring, material, and device safety. In obstetrics clinics, insufficient patient monitoring during labor is among the most common reasons for malpractice lawsuits and errors that could lead to medical errors [20]. Regular checks of medical devices and materials, as well as in-service training for nurses and midwives regarding device and material usage, are important [1,20].
Two areas where the tendency to make medical errors was high in our study were "Medication and Transfusion Practices" and "Patient Monitoring, Material, and Device Safety." It can be said that nurses and midwives working in obstetrics and gynecology clinics make the most medical errors in these two areas. In our study, when we compared METSN scores according to age, education level, marital status, and whether they received patient safety training, no significant differences were found. However, it was determined that those who made medical errors and those who witnessed medical errors had a higher risk of making medical errors. Baştürk's study also reported that nurses who made medical errors had a higher tendency to make medical errors [17].
Conclusion and Recommendations
Obstetrics and gynecology clinics are units with a high risk of maternal and fetal morbidity and mortality. The high rates of medical errors and witnessing medical errors in our study confirm that there is a high tendency for medical errors in obstetrics and gynecology clinics.
Patient safety begins with preventing medical errors. In line with the goal of "Zero Medical Errors" in healthcare services, it is important to perform healthcare practices correctly and to report medical errors accurately. Investigating and researching all risk factors that may cause medical errors, especially in units with a high risk of medical errors such as obstetrics and gynecology clinics, and increasing the knowledge and awareness of nurses and midwives through in-service training are important. Increasing the prevalence of patient safety and quality improvement efforts in hospitals and conducting detailed investigations into the root causes of medical errors are recommended.
Competing interest:
All authors declare that there is no conflict of interest.
References
Çom, U., Üzün, İ., & Gümüş, B. (2020). Evaluation of medical malpractice claims in gynecology and obstetrics cases resulting in death. Journal of Contemporary Medicine, 10(4), 567-572.View
Ghaith, S., Campbell, R.L., Pollock, J.R., Torbenson, V.E., & Lindor, R.A. (2022). Medical Malpractice Lawsuits Involving Trainees in Obstetrics and Gynecology in the USA. Healthcare, 10, 1328. https://doi.org/ 10.3390/healthcare10071328View
Kostov, I., Ingilizova, G., & Slavov, S. (2021). Medıcal errors ın obstetrıcs and gynecology ın bulgarıa–a survey of the judıcıal practıce. Knowledge-International Journal, 46(4), 499-503.View
Hızarcı, Ş., Bakır, S., & Kavlak, O. (2021). Kadın hastalıkları ve doğum kliniğinde çalışan hemşire ve ebelerin tıbbi hatalarda hukuki sorumluluklara yönelik bilgi ve tutumlarının incelenmesi. Sağlık ve Hemşirelik Yönetimi Dergisi, 8(2), 221 231View
World Health Organization. Patient Safety. 2019.https:// www.who.int/news-room/fact-sheets/detail/patient-safety# (Accessible date: Marc 20, 2023).View
World Health Organization. World Alliance for Patient Safety Forward Programme. (2018). http://www.who.int/patientsafety/ en/brochure_final.pdf. (Accessible date: April 10, 2023).View
Çakmak, C., Konca, M., & Teleş, M. (2018). Türkiye ulusal güvenlik raporlama sistemi (grs) üzerinden tıbbi hataların değerlendirilmesi. Hacettepe Sağlık İdaresi Dergisi, 21(3), 423 448.View
Kandemir, A., & Yüksel, S. (2020). Cerrahi hemşirelerinin tıbbi hata tutum ve eğilimlerinin belirlenmesi. Anadolu Hemşirelik ve Sağlık Bilimleri Dergisi, 23(2), 287-297. Doi: 10.17049/ ataunihem.659960.View
White, A. A., Pichert, J.W., Bledsoe, S.H., Irwin, C., & Entman, S.S. (2005). Cause and effect analysis of closed claims in obstetrics and gynecology. Obstetrics & Gynecology, 5(1)1031 1038. doi: 10.1097/01.AOG.0000158864.09443.77.View
Büke, E., Çağdır, A.S., & Soysa, Z. (2004). Davalı durumdaki kadın doğum hekimi. Uzmanlık Sonrası Eğitim ve Güncel Gelişmeler Dergisi, 1, 65-69.
Demir S., & Hotun, Ş.N. (2014). Perinatal hasta güvenliginde hasta teslimi: kullanılan iletişim teknikleri. Hemşirelikte Eğitim ve Araştırma Dergisi, 11 (3), 32-37.View
Kıymaz, D., & Koç, Z. (2018). Identification of factors which affect the tendency towards and attitudes of emergency unit nurses to make medical errors. Journal of Clinical Nursing, 27(5-6), 1160-1169.View
Özen, N., Onay, T., & Terzioğlu, F. (2019). Hemşirelerin tıbbi hata eğilimlerinin ve etkileyen faktörlerin belirlenmesi. Sağlık Bilimleri ve Meslekleri Dergisi, 6(2), 283-92.View
Özata, M., & Altunkan, H. Hemşirelerin Tıbbi Hataya Eğilim Ölçeğinin Geliştirilmesi ve Geçerlilik Güvenirlilik Analizinin Yapılması. Editör: Kırılmaz H. II. Uluslararası Sağlıkta Performans ve Kalite Kongresi; 2010b; Ankara: Baydan Ofset; 2010. p. 415-31
Er, F., & Altuntaş, S. (2016). Hemşirelerin tıbbi hata yapma durumları ve nedenlerine yönelik görüşlerinin belirlenmesi. Sağlık ve Hemşirelik Yönetimi Dergisi, 3(3),132-9.View
Güleç, D., & İntepeler, Ş.S. (2016). Tıbbi Hatalarda Tutum Ölçeğinin Geliştirilmesi. Hemşirelikte Araştırma Geliştirme Dergisi, 15(3),26-41. View
Baştürk, H. (2019). Hemşirelerin tıbbi hata yapma eğilimlerinin ve etkileyen faktörlerin belirlenmesi, Manisa Celal Bayar Üniversitesi Sağlık Bilimleri Enstitüsü, Yükseklisans Tezi, Manisa.View
Türk, G., Özdemir, S., & Elem, K.G. (2019). İntörn hemşirelerin tıbbi hata eğilimlerinin incelenmesi Turkiye Klinikleri J Nurs Sci., 11(4),374-80. Doı: 10.5336/Nurses.2019-65927.View
Koçak, D., & Yaman, Ş. (2015). Kadın doğum kliniklerinde çalışan hemşirelerin yaptıkları ilaç hataları ve etkileyen faktörler. Hemşirelikte Eğitim ve Araştırma Dergisi, 12 (2), 99 104.View
Durmuş, S. Ç., Erdem, Y., & Yılmaz, E. D. (2022). Hemşirelerin tıbbi hata yapma eğilimleri: bir kamu üniversitesi tıp fakültesi hastanesi örneği. Kırıkkale Üniversitesi Tıp Fakültesi Dergisi, 24(1), 153-162.View