
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 1 (2019), Article ID: JMHSB-104
https://doi.org/10.33790/jmhsb1100104Research Article
The Influence of Sheltering or Protective, Parental Behaviors Following Child Trauma; Hurricane Katrina
Adrian Anderson
Department of Social Work, Savannah State University, Social Science Bldg., RM 243, P.O. Box 20553, 3219 College Street Savannah, Ga. 31404, United States.
Corresponding Author Details: Adrian Anderson, Associate Professor, Department of Social Work, Savannah State University, Social Science Bldg, RM 243, P.O. Box 20553, 3219 College Street, United States. E-mail: andersona@savannahstate.edu
Received date: 30th September, 2019
Accepted date: 31st October, 2019
Published date: 01st November, 2019
Citation: Anderson A (2019) The Influence of Sheltering or Protective, Parental Behaviors following Child Trauma; Hurricane Katrina. J Ment Health Soc Behav 1: 104.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This study examined the relationship between parental behaviors and trauma experienced by 42 school-aged children (6 to 12 years of age) impacted by a natural disaster; Hurricane Katrina. Results showed that one of the parental behaviors examined, open communication, was positively associated with higher Post-traumatic Stress Disorder Reaction Index scores in the child population. This finding indicates that open communication from parent-to-child may increase trauma symptoms in school-aged children following a traumatic event. Results of this research may contribute to mental health intervention practices following child trauma, and disaster related prevention planning. The influence of parental behaviors following child exposure to trauma may be of particular importance to mental health practitioners, emergency management agencies and emergency and disaster relief workers.
Key words: Parental Behaviors; Child Trauma; PTSD in Children; Parental First Aide; Open Communication; Trauma in Children
Introduction
On August 29, 2005, Hurricane Katrina struck New Orleans destroying levees and floodwalls leaving the city 20 feet under water [1]. Close to 25 percent of the residents who lived in areas damaged or flooded by Hurricane Katrina were children under the age of 18 [2]. Hurricane Katrina potentially displaced 136,000 schoolaged children and 183,000 children over-all. Research estimates that 47,000 children under the age of five lived in neighborhoods that experienced flooding or damage from Hurricane Katrina [2]. Furthermore, research has shown that some school-aged children impacted by Hurricane Katrina suffered from Post Traumatic Stress Disorder [3].
Prior to and following Hurricane Katrina, many of the social service agencies and their employees evacuated the city of New Orleans. Hurricane Katrina had a significant impact on the social service system, resulting in the closures of hospitals, schools, day care centers, public transit services and roads. Research conducted with 665 households of displaced, Louisiana residents following Hurricane Katrina showed that nearly half of the parents reported that at least one child in their household suffered from emotional or behavioral difficulties that were not present pre-Katrina, yet several parents and caregivers reported difficulties in finding accessible mental health services [4].
Research has shown that parental support is one of the most important protective factors following a traumatic event [5,6]. Parental response is the first response that may buffer the impact of trauma and becomes particularly important when natural disasters disrupt the delivery of community services. Parental response is also important following family dislocation that may result from a natural disaster. Some families transition to unfamiliar communities in which parents may require time to learn about social services available to children.
Research Question and Conceptual Framework
Research presented in this article explored the relationship between sheltering or protective parental behaviors, and Post-traumatic Stress Disorder reaction scores of school-aged children following Hurricane Katrina. This information may be useful for mental health practitioners, emergency management agencies, emergency and disaster relief workers, and peremptory planning by parents when mental health services may be interrupted in areas devastated by a natural disaster or shortly following family dislocation.
A key component of this study focused on protective, parental practices that may serve to mitigate symptoms of trauma following exposure to a traumatic event. This study used the term sheltering interchangeably with protective. The term sheltering has not been used in previous research pursuits. Shelter is defined by the [7] as something that screens or protects from harm. Sheltering behaviors may serve to shield children from harm or unsafe conditions within a devastated community. These parental behaviors may screen children from negative influences in unfamiliar communities when families are dislocated as a result of a natural disaster. Sheltering behaviors may also shield children from trauma by decreasing their opportunity to witness violence and other traumatic events following a natural disaster.
There is an abundance of research on a wide range of protective, parental behaviors that far exceed the parental behaviors examined in this study. However, the six protective or sheltering behaviors examined in this study are as follows: (1) daily parental monitoring or supervision, (2) family rituals in which research by Steinglass et al. [8] has shown to encompass three categories: family celebrations, family traditions and ritualized routines, (3) open communication in which Riesch [9] posits is a free-flowing exchange of information without constraint, (4) active facilitation of extracurricular activities at school, (5) joint leisure activities, and (6) parental involvement with the child’s school.
Evidence-based practice which involves integrating practice expertise with the best available external evidence from systematic research served as an impetus for research in this area [10]. These six parental practices were chosen for research based on observation and practice experience over the course of several years. Although anecdotal, observation and practice experience with many families has revealed positive emotional and behavioral outcomes in children when parents have engaged in these six behaviors. Previous research has also shown that each of the six parental practices is likely to lead to positive emotional and behavioral outcomes in children [9,11- 18]. Gambrill asserts that evidence-based practitioners should use research methods to evaluate whether evidence-based actions result in the desired outcomes [10]. Furthermore, Rubin and Babbie posits that evidence-based practitioners should engage in research pursuits that may lead to the best scientific evidence available when deciding which intervention to use with individuals and families [19].
Research has pointed to parental behaviors that protect or shelter children from the negative effects of psychological stress; parental supervision, predictable routines, direct communication, effective use of leisure time, children’s involvement in extracurricular activities and parental involvement with their child’s school [20,21,22].
Sheltering or protective behaviors also correspond with supportive parental behaviors. Parental support, often used interchangeably with parental response, has many definitions. However, the common goal is to provide a context that promotes positive adjustment and behavioral outcomes in children. The International Society for Traumatic Stress Studies [23] suggest that following a traumatic event parents can support their children by engaging in the following behaviors: (1) let the child(ren) know that it is normal to feel upset when something scary or bad happens, (2) encourage the child(ren) to express thoughts and feelings and suspend judgments, (3) protect the child(ren) or adolescent(s) from further exposure to events that are traumatic as much as possible, (4) revert to routines that are normal as much as possible, (5) educate school personnel about the needs of the child(ren), (6) allow the child(ren) to cry or feel sad, and (7) give the child(ren) a sense of choice and control by offering reasonable options pertaining to daily activities (choosing clothes, meals etc.).
Previous Research
Researchers have extensively examined parental behaviors that are protective and supportive in nature which ranges from parental supervision, family rituals, open communication between parent and child, parental facilitation of extracurricular activities with children, joint leisure activities between parent and child, and parental involvement in children’s school based activities, and their relationships with behavioral outcomes in children. Yet, there is limited research that examines the relationship between the six parental behaviors in this study, and behavioral outcomes in children who were directly exposed to Hurricane Katrina.
Supervision
Previous research has shown that protective parental behaviors are associated with positive outcomes in children. Parental monitoring or supervision encompasses parental behaviors such as parents knowing about their children’s friends, where their children are after school, where their children go during the evening or at night and what children do with their free time [24]. Research conducted with a sample population of 287 school-aged children has shown that parental monitoring is negatively related to behavioral problems and substance abuse in children [24]. Research by Shiff et al. [13] has shown that parental supervision is associated with a reduction in aggression and delinquency in children. Astone et al. [25] conducted research in which findings showed that parental supervision was positively associated with outcomes in children such as regular school attendance, continuous school attendance until the completion of high school and aspirations to attend college.
Family Rituals
Family rituals or rich and meaningful, repetitious and symbolic activities that transmit family values and enduring goals are the core of family life [8,14,26-28]. Family rituals encompass three categories: family celebrations, family traditions and ritualized routines [8]. Family celebrations may include religious and secular holidays, and rites of passage such as funerals, baptism and bar mitzvahs that call forth highly patterned, symbolically rich behaviors that are often cherished by individuals and family members [8]. Family traditions which are more idiosyncratic to the family include activities such as family reunions, birthday traditions, vacations and visits to and from other family members’ homes [8,26,27]. Patterned routines provide families with a sense of order and comfort, and include activities such as bedtime and dinnertime rituals, leisure time rituals, bath time rituals and customary greetings and partings [8,26].
Findings from research has shown that family rituals are associated with prosocial behaviors in children, and negatively associated with externalizing behaviors [29]. Furthermore, research has shown that family rituals are associated with a decrease in parental distress, and lower levels of parental distress have been shown to decrease the likelihood of Post Traumatic Stress Disorder in children following a traumatic event [27,30].
Open Communication
Communication among family members has generally been accepted as a significant component of interpersonal relationships, and various types of communication patterns have been associated with positive adaptation in children that include outcomes such as reduced family conflict and fewer incidents of dropping out of school to delinquent behaviors such as auto theft, vandalism or carrying a concealed weapon [9,11,25,31]. Open communication, often used interchangeably with positive communication, is associated with the ability to express opinions and ideas. Open communication is also characterized by an emphasis on freedom or a free-flowing exchange of information; emotional and factual [9]. Problem communication, used interchangeably with negative communication, is often perceived by adolescents as one-sided, devoid of certain topics, closed and conflictual, and is characterized by hesitancy to share [9].
Research conducted by Clark et al. [11], using a sample of high school students, found that problem communication was associated with severe forms of delinquent behavior. For instance, problem communication was associated with grand theft, rape, robbery, motor vehicle theft, breaking and entering, carrying concealed weapons, and selling drugs. Problem communication may serve to impede a free-flowing exchange of information while open communication may serve as a vehicle to enhance parents’ knowledge about exposure to an extreme traumatic stressor that children may witness in their communities. Research has shown that inner city youth often disagree with their mothers about the level of violence in the community. For example, Ceballo et al. [31] found that mothers of inner-city youth underrate their children’s exposure to violence. Furthermore, research suggests that mother-child agreement about community violence is related to better psychological functioning in children [31]. Furthermore, findings from a study conducted by [32] found that adolescents suffering from trauma reported that talking to parents and having parents listen to them following a traumatic incident helped them deal with the aftermath of trauma.
Active facilitation of extracurricular activities
Research has shown that children involved in structured leisure activities that include skill building and mentoring such as music, theater, scouts and politics have lower rates of antisocial behavior in comparison to peers in less structured activities [33]. A study conducted by Darling et al. [12] found that youth who participate in extracurricular activities have better grades, academic aspirations and adjustment in school relative to their peers. Mahoney et al. [34] found that extracurricular activities, through after school involvement, was associated with a reduction in depressed moods of children from families with detached parents. Child involvement in extracurricular activities is increasingly important considering that individuals with Post Traumatic Stress Disorder may be at higher risk of suffering from Major Depressive Disorder [35].
Joint leisure activities
Joint leisure activities may be of particular importance for children following a natural disaster. Research has shown that organized leisure activities serve as a protective factor in children who are adjudicated offenders [21]. Furthermore, the time a child spends with a parent(s) engaging in leisure or fun activities is used by some families to transfer values, teach social skills and enhance family cohesion [36]. Research has also shown that regular family leisure activities have a significant, positive impact on youth’s perception of family satisfaction [15]. For instance, Zabriskie et al. [15] found a relationship between higher levels of involvement in core family activities (playing together in the yard, playing board games, and watching television together), and family satisfaction among youth. Joint leisure activities may be important for children suffering from Post Traumatic Stress Disorder in which symptoms include diminished participation and interest in activities the child previously enjoyed or feelings of estrangement or detachment from others [35].
Parental involvement in school-based activities
Research has shown that parental involvement with school, such as monitoring and promoting homework, interaction with school officials and parent-child communication about school progress, has positive behavioral and academic outcomes in children [16,29,37-39]. Research conducted by Stone [37] also found a positive relationship between parental involvement in school and higher grade point averages of children, and a negative relationship between parental involvement in school and drop out rates of children. The importance of parental involvement in school-based activities is critically important with children suffering from PTSD. Symptoms that may place children at higher risk of school drop out include difficulty concentrating, diminished responsiveness to the external world, and a reduction in participation in activities the child previously enjoyed [34].
Method
Participants
This study used data from the Project Last Elementary Age Grief and Trauma Intervention; a model, developed by Salloum [40] and funded by the Institute of Mental Hygiene. The project took place from January to May 2006 [41]. Parental consent forms were signed by parents of children who participated in Project Last Elementary Age Grief and Trauma Intervention. The secondary, data analysis study on sheltering was approved by Children’s Bureau of New Orleans, and Tulane University’s Institutional Review Board. The total sample size of children for research on sheltering was 42 (N = 42). The total sample size of parents who corresponded to child participants was 34 (N = 34). A total of seven parents/caregivers had more than one child participant in this study which explains the discrepancy in the number of parents whom completed questionnaires and the total number of child participants. Specifically, there were six caregivers in which each caregiver was a custodian of two child participants in this study, and one caregiver was a custodian of three child participants in this study. Thus, a total of fifteen children used in the child sample were part of a sibling relationship.
Project Last Elementary Age Grief and Trauma Intervention was developed to help school-aged children (1) learn about grief and traumatic reactions, (2) express their thoughts and feelings about the traumatic event through coherent narratives and expressing the of the traumatic event, and to (3) reduce traumatic stress symptoms [41]. The model included topics such as anger management, relaxation, connecting with supportive adults, family support, coping with anniversaries, spirituality and beliefs, dreams, safety, and worst moments [41].
The model was implemented in three elementary schools in New Orleans: Behrman, Harte and Eisenhower. These three schools were located in impoverished areas of the city. Child participants had to meet the following requirements to participate in Project Last Elementary Age Grief and Trauma Intervention: (1) returned signed parental consent forms, (2) enrolled in the second through sixth grades at Behrman, Eisenhower or Harte elementary schools, (3) were not actively suicidal, (4) grieving at least one month post death or experience a moderate level of PTSD symptomology resulting from death, or any hurricane related stressor (Salloum & Overstreet, 2007). A score of at least 25 on the University of California Los Angeles Post-traumatic Stress Disorder Reaction Index [Revision 1] was the criteria for moderate PTSD symptomology.
Measures
Post-traumatic stress disorder diagnoses and symptoms in children were assessed using the University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index [Revision 1] which is designed to screen for exposure to a wide range of traumatic events experienced by youth from 7 to 18 years of age. The UCLA PTSD Reaction Index also screens for symptoms outlined in the Diagnostic and Statistical Manual of Mental Disorders (fourth edition). The instrument screens for trauma symptoms resulting from exposure to natural disasters, medical trauma, community violence and abuse [42].
Research on the psychometric properties has yielded a convergent validity coefficient of .70 in comparison with the PTSD module which is included with the Epidemiological version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS-E), and a convergent validity coefficient of .82 in comparison with the Clinician-Administered PTSD Scale for Children and Adolescents [CAPS-CA] [42-44]. Furthermore, several research reports have shown that this instrument is highly reliable yielding a Cronbach alpha coefficient of .90 [42].
Parental behaviors were assessed using the sheltering instrument which was developed for an adult population; specifically, parents or guardians of children impacted by Hurricane Katrina [45]. The instrument screens for a change in parental behaviors that comprise the sheltering construct. The internal consistency reliability coefficient or Cronbach alpha coefficient for the sheltering instrument is α = .61.
Data Analysis
The Point biserial correlation was used to examine PTSD reaction scores and sheltering variables within this study. The Point biserial correlation (rpb) is considered the most appropriate analysis when examining the relationship between a truly dichotomous variable and a continuous variable. The sheltering variables under examination were dichotomous, and the PTSD Reaction Index scores of child participants were ratio variables. The following sheltering variables were examined; (1) supervision, (2) family rituals, (3) open communication, (4) active facilitation of extracurricular activities at school, (5) joint leisure activities, and (6) parental involvement with the child’s school.
Results
Table 1 (Appendix A) shows that 32 caregivers in the sample were female (94.1 percent) and 2 were males (5.9 percent). The average age of caregivers was 37.74 years (SD = 8.404). Table 1 shows that over half of the caregivers (52.9 percent) reported being single; only 9 respondents reported being married (26.5 percent). Most caregivers reported being employed (76.5 percent), while only 8 respondents reported being unemployed (23.5 percent). The highest percentage of respondents (35.3 percent) reported yearly wage earnings below $9,999 while 2 respondents (5.9 percent) reported yearly income J Ment Health Soc Behav JMHSB, an open access journal Volume 1. 2019. 104 levels that exceeded $50,000. A total of 6 (17.6 percent) parents were custodians of 2 siblings that participated in this study, and 1 (2.9 percent) parent was custodian of 3 siblings that participated in the study.
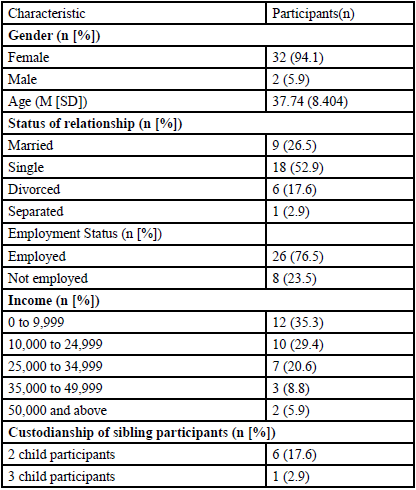
Table: 1 Demographic Information: caregiver (N = 34)
Table 2 (Appendix B) shows that the sample consisted of male and female children with an average age of 9.83 years (SD = 1.529). Results from Table 2 show that 28 child participants were male (66.7%), and 14 child participants were female (33.3%). Grades of participants ranged from second through sixth (M = 4.17). The sample consisted of 39 African American child participants (92.9%), and 3 Caucasian child participants (7.1%). A total of 15 (35.7%) child participants in this study were part of a sibling relationship.

Table: 2 Demographic Information: children (N = 42)
The primary research question was concerned with relationships between sheltering or protective variables, and Post-traumatic Stress Disorder Reaction Index scores in school-aged children. Results from Table 3 (Appendix C) showed a positive association between open communication and PTSD Reaction Index scores in J Ment Health Soc Behav JMHSB, an open access journal Volume 1. 2019. 104 children. Table 3 shows that increases in open communication was significantly associated with increases in PTSD Reaction Index scores of children, rpb(40) = .425, p < .001. However, results failed to show a relationship between PTSD Reaction Index scores and the remaining sheltering variables.
Table: 3
Implications for Practice
An important finding from this study showed that open communication was positively associated with higher PTSD scores in children impacted by Hurricane Katrina. This finding indicates that parental communication may influence trauma symptoms in school-aged children following a traumatic event. The results of this study inform mental health practitioners, emergency and disaster relief workers about the importance of exploring parent-to-child communication patterns during mental health assessments. Open or honest communication about family issues from parent-to-child may entail disclosure of severe parental distress. This level of disclosure by a parent may serve to increase trauma symptoms in school-aged children. Thus, this study highlights the importance of assessing for the type and direction of communication that occurs between parent and child following a traumatic event.
The results of this study may also aide in prevention planning by mental health practitioners, emergency and disaster relief workers in areas that may be prone to hurricanes, floods or other types of natural disasters. Pre-planning efforts may include family and community education about the importance and types of parent-to-child communication patterns that are associated with positive outcomes in children following exposure to trauma.
Limitations
Findings from this study must be carefully interpreted. Future research may explore to determine the content of parent-to-child communication following a traumatic event, and whether gender is associated with the type of communication between the parent and child. Research has shown that children’s susceptibility to PTSD is strongly associated with parental distress [30,46-48]. Furthermore, research conducted with 665 households of displaced, Louisiana residents showed that caregivers scored very low on a standardized mental health screening tool; over half of female caregivers scored at levels consistent with clinically-diagnosed psychiatric problems such anxiety disorders and depression (Abramson & Garfield, 2006). Female caregivers were six times as likely to report coping difficulties with the daily demands of parenting after Katrina than before [4]. Of the 34 caregivers used in the study, 32 (94.1%) were female.
Discussion
Previous research has shown that protective parental behaviors or sheltering behaviors are associated with positive outcomes in children. Findings from this study showed that increases in open communication were significantly associated with increases in trauma symptoms of children following this specific natural disaster; Hurricane Katrina. The remaining sheltering variables showed no significant associations with trauma symptoms in the child population.
There are many factors that may have contributed to the findings of this research pursuit. Resilience in the child population under study, the dynamic process that encompasses positive adaptation within the context of adversity, may have been a contributing factor in the findings of this research pursuit [49]. Internal and external factors associated with the development of resilience in children that preceded Hurricane Katrina such as self confidence, self-reliance, positive future expectations and exposure to prosocial adults and influences in the wider social environment such as school may have diminished the relationship between sheltering behaviors, PTSD reaction scores and distress in children [49,50,51]. This sample of children may have had high levels of resilience prior to the storm.
Gender of child participants is another consideration that must be taken into account when interpreting the results of this study. Male children constituted two-thirds of the child sample (66.7%), and research has consistently shown that female children report higher levels of anxiety and PTSD symptoms than boys [52-54].
This sample consisted of only a few families that were able to return to New Orleans within four months following Hurricane Katrina. This indicates a shorter length of displacement for the families that participated in the original study in contrast to families who had not returned. Research has shown that continued length of displacement following a natural disaster is strongly related to the presence of PTSD symptoms in children [55].
Conflicts of Interest (COI) Statement
The author has declared no conflict of interest.
References
Federal Emergency Management Agency. (2006). About Hurricane Katrina.
Gabe, T., Falk, G., & McCarty, M. (2005). Hurricane Katrina: Social-Demographic Characteristics of Impacted Areas (Order Code RL33141). Congressional Research Service Report for Congress. The Library of Congress.View
Salloum, A., Garside. L., Irwin, L., Anderson, A., Francois, A. et al. (2009). Grief and Trauma Group Therapy with Children after Hurricane Katrina. Social Work With Groups 32: 64-79.View
Abramson, D., & Garfield, R. (2007). On the Edge: Children and Families Displaced by Hurricanes Katrina and Rita Face a Looming Medical and Mental Health Crisis.View
National Institute of Mental Health. (2006). Reliving Trauma.
Salloum, A. (2004). Group Work with Adolescents After Violent Death: A Manual for Practitioners. New York: Brunner- Routledge.
Oxford English Dictionary. (2007).
Steinglass, P., Bennet, L.A., Wolin, S.J., & Reiss, D. (1987). The Alcoholic Family. New York, NY: Basic Books, Inc.
Riesch, S.K. (2003). Effects of Communication Skills Training on Parents and Young Adolescents From Extreme Family Types. J Child Adolescent Psychia Nurs 16: 162-175.View
Gambrill, E. (1999). Evidenced-Based Practice: An Alternative to Authority-Based Practice. Families in Soc 80: 341-350. View
Clark, R.D., & Shields, G. (1997). Family Communication and Delinquency. Adolescence 32: 81-93.View
Darling, N., Caldwel, L.L., & Smith, R. (2005). Participation in School- Based Extracurricular Activities and Adolescent Adjustment. J Leisure Res 37: 51-77.View
Schiff, M., & McKay, M.M. (2003). Urban Youth Disruptive Behavioral Difficulties: Exploring Association with Parenting and Gender. Family Process 42: 517-529.View
Skibbee, B.D. (2001). The relationship between parental mental health, family environment, and the resiliency of adolescents of alcoholic parents. Dissertation Abstracts International: Section B: The Sci Eng 62: 565.View
Zabriskie, R.B., & McCormick, B.P. (2003). Parent and child perspectives of family leisure involvement and satisfaction with family life. J Leisure Res 35: 163-189.View
Potvin, P., Deslandes, R., & Leclerc, D. (1999). Family characteristics as predictors of school achievement: parental involvement as a mediator. McGill J Edu,View
Cartwright-Hatton, S. (2005). Parenting Skills Training: An Effective Intervention for Internalizing Symptoms in Younger Children? J Child Adolescent Psychiat Nurs18: 45-52.View
Sartor, C.E. (2002). The Relationship between Positive Parental Involvement and Identity Achievement during Adolescence. Adolescence 37: 221-235.View
Rubin, A., & Babbie, E.R. (2005). Research Methods for Social Work. Belmont, CA: Brooks-Cole- Thomson Learning. View
McCabe, M.C., Clark, R., & Barnett, D. (1999). Family Protective Factors among urban African American youth. J Child Psychol 28: 137-156.View
Hoge, D.R., Andrews, D.A., & Leschield, W.A. (1996). An investigation of risk and protective factors in a sample of youthful offenders. J Child Psychol Psychiat 37: 419-424.View
Center for Disease Control (2007) Scientific Information: Risk and Protective Factors.
International Society for Traumatic Stress Studies (2005) Children and Trauma.View
Raboteg-Saric, Z., Rijavec, M., & Brajsa-Zganec, A. (2001). The relation of parental practices and self-conceptions to young adolescent problem behaviors and substance use. Nord J Psychiat 55: 203-209.View
Astone, M.N., & McLanahan, S.S. (1991). Family Structure, Parental Practices and High School Completion. Am Sociological Rev 56: 309-320.View
Schuck, L.A., & Bucy, E.J. (1997). Family Rituals: Implications for Early Intervention. Topics Early Childhood Educa 17: 477-489.
Schuck, L.A. (1998). The relationship between family rituals and social skills in preschoolers from low-income families. Dissertation Abstracts International: Section B: The Sci Eng 58: 6848.
Fiese, B.H. (1993). Family Rituals in Alcoholic and Nonalcoholic Households. Family Relations 42: 187-199.
Koblinsky, A.S., Kuvalanka, A.K., & Randolph, M.S. (2006). Social Skills and Behavior Problems of Urban, African American Preschoolers: Role of Parenting Practices, Family Conflict, and Maternal Depression. Am J Orthopsychiat 76: 554-563.View
Hamblen, J. (2006). PTSD in Children and Adolescents. United States Department of Veterans Affairs. National Center for PTSD.
Ceballo, R., Dahl, T.A., Aretakis, M.T., & Ramirez, C. (2001). Inner-City Children’s Exposure to Community Violence: How Much Do Parents Know? J Marriage Family 63: 927-940.View
Morin, S.M., & Welsh, L.A. (1996). Adolescents’ perceptions and experiences of death and grieving. Adolescence 31: 585-596.View
Mahoney, L.J., & Stattin, H. (2000). Leisure activities and adolescent antisocial behavior: The role of structure and social context. J Adolescence 23: 113-128.View
Mahoney., L.J., & Schweder, E.A. (2002). Structured after-school activities as a moderator of depressed mood for adolescents with detached relations to their parents. J Community Psychol 30: 69-86.View
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (2000) Washington, DC, Am Psychiat Associa.
Shaw, S.M., & Dawson, D. (2001). Purposive leisure: Examining parental discourses on family activities. Leisure Sciences 23: 217-231.View
Stone, S. (2006). Correlates of Change in Student Reported Parent Involvement in Schooling: A New Look at the National Educational Longitudinal Study of 1988. Am J Orthopsychiat 76: 518-530.View
Miedel, T.W., & Reynolds, J.A. (1999). Parent Involvement in Early Intervention for Disadvantaged Children: Does It Matter? J School Psychol 4: 379-402.View
Sui-Chu, H.E., & Willms, J.D. (1996). Effects of Parental Involvement on Eighth-Grade Achievement. Sociolo Educat 69: 126-141.View
Salloum, A. (2005). Project LAST (Loss and Survival Team) Elementary Age Grief and Trauma Intervention Model.
Salloum, A., Overstreet, S. (2007). Effectiveness of a grief and trauma intervention for elementary age children. Manuscript submitted for publication.
Steinberg, A.M., Brymer, M.J., Decker, K.B., & Pynoos, S. (2004). The University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index. Current Psychiat Reports 6: 96-100.View
Radcliffe, J. (2006). Current Measures of PTSD for Children and Adolescents. J Pediatric Psycholol 31: 420-430.View
Ruggiero, K.J., McLeer, S., & Dixon, J.F. (2000). Sexual Abuse Characteristics Associated with Survivor Psychopathology. Child Abuse & Neglect 24: 951-964.View
Anderson, D.A. (2007). Sheltering: A Protective Parental Response to Children exposed to a Natural Disaster. Unpublished doctoral dissertation. Tulane University, Louisiana.
Wasserstein, S.B., La Greca, A.M. (1998). Hurricane Andrew: Parent conflict as a moderator of children’s adjustment. Hispanic J Behav Sci 20: 212-224.View
Bradburn, I.S. (1991). After the earth shook: Children’s stress symptoms 6-8 months after a disaster. Adv Behav Res Therapy 13: 173-179.View
McFarlane, A.C. (1987). Posttraumatic phenomena in a longitudinal study of children following a natural disaster. J Am Acad Child Adolescent Psychiat 26: 764-769.View
Luthar, S.S., Cicchetti, D., & Becker, B. (2000). The Construct of Resilience: A Critical Evaluation and Guidelines for Future Work. Child Development 71: 543-562.View
Masten, A.S., Hubbard, J.J., Gest, S.D., Tellegen, A., & Garmezy, N. et al. (1999). Competence in the context of adversity: Pathways to resilience and maladaption from childhood to late adolescence. Development and Psychopathology, 11, 143-169.View
Cicchetti, D., & Rogosch, F.A. (1997). The role of self-organization in the promotion of resilience in maltreated children. Development and Psychopathol 9: 797-815.View
Garrison, C.Z., Bryant, S., Addy, C.L., Spurrier, P.G., Freedy, J.R. et al. (1995). Posttraumatic stress disorder in adolescents after Hurricane Andrew. J Am Acad Child and Adolescent Psychiat 34: 1174-1184.View
Lonigan, C.J., Shannon, M.P., Finch, A.J., Daugherty, T.K., Taylor, C.M. et al. (1991). Children’s reaction to a natural disaster: Symptom severity and degree of exposure. Adva Behav Res Therapy 13: 135-154.View
Green, B.L., Korol, M., Grace, M.C., Vary, M.G., Leonard, A.C. et al. (1991). Children and disaster: Age, gender, and parental effects on PTSD symptoms. J Am Acad Child Adolescent Psychiat 30: 945-951.View
Lonigan, C.J., Grace, M.P., Taylor, C.M., Finch, A.J. Jr, Sallee, R.R. et al. (1994). Children Exposed to Disaster: II. Risk factors for the development of post-traumatic symptomatology. Journal of the Am Acad Child Adolescent Psychiat 33: 94-105.