
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 1 (2019), Article ID: JMHSB-105
https://doi.org/10.33790/jmhsb1100105Commentary Article
Psychosocial Oncology Disparities: Treating the Whole Person in Rural Indigenous Communities
Sky Niesen Smith DSW, LICSW
Assistant Professor, Department of Social Work, Minnesota State University, Mankato, United States.
Corresponding Author Details: Sky Niesen Smith, Assistant Professor, Department of Social Work, Minnesota State University, Mankato, office: 507-389-5084; TN 333, United States. E-mail: skyniesensmith@gmail.com
Received date: 10th October, 2019
Accepted date: 23rd November, 2019
Published date: 26th November, 2019
Citation: Smith, S.N. (2019). Psychosocial Oncology Disparities: Treating the Whole Person in Rural Indigenous Communities. J Ment Health Soc Behav 1: 105.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
In recent years, psychosocial services have been viewed as paramount in treating cancer, yet disparities exist in psychosocial services for rural cancer patients. Using ecological theory, cancer care focuses on more than medical intervention, favoring treatment of the “whole” person. For Indigenous people experiencing cancer, responsive psychosocial interventions and practice frameworks are needed to address health-related distress. Using the intersection of diversity and environment, this conceptual paper provides a review of literature on the topic of cancer care with Indigenous people living in rural areas and furthermore argues that social workers, given educational experiences and practice frameworks, are essential culturally-responsive providers of psychosocial oncology services. Social workers must be utilized and mobilized as health care leaders in order to improve quality of life by advocating for culturally responsive, equitable services for people confronting cancer. Social workers have knowledge and skills to be front-line providers, service mobilizers, and program developers of culturally-responsive psychosocial oncology services.
Key words: Psychosocial Oncology, Health Disparities, Rural Healthcare, Health-Related Distress
Psychosocial Oncology Disparities
Treating the Whole Person in Rural Indigenous Communities. A medical diagnosis is often a traumatic experience for an individual, impacting an individual’s sense of homeostasis [1]. Psychosocial functioning of people with cancer is dependent on access to proper medical care. In the rural context, individuals are often unable to access adequate psychosocial care in order to treat symptoms of distress during a medical crisis. For rural Indigenous people who reside in what is now known as the United States (U.S.), culturally responsive psychosocial cancer care may support effective communication among family members and biomedical teams. Although some knowledge exists in regard to biomedical services for rural Indigenous cancer patients, scant literature exists in the topic of elevating social work as essential in providing needed psychosocial oncology services. Health-related distress in cancer patients is influenced by cultural and environmental factors. Social workers have knowledge and competence in the area of working with these factors in levels of systems in order to understand individuals and families.
Background
Indigenous people with Tribal enrollment in the United States are Constitutionally guaranteed to receive medical care through the Indian Health Services (IHS) program. This program, under the federal Department of Health and Human Services, maintains a goal to provide culturally responsive comprehensive health services to American Indians and Alaskan Natives [2]. IHS includes 12 regional offices throughout the United States and numerous medical clinics and hospitals. For oncology care, IHS systems interface with specialty providers who maintain contracts to provide medical care. This interface may include travel arrangement and expenses (particularly for rural residents) as well as cancer care medical coverage. This paper argues that social workers, with specialized educational knowledge of culturally responsive practice frameworks, are integral in cancer care with rural indigenous populations. Social work educational policies, ethical standards, and practice theoretical frameworks allows social work to be well-positioned as a profession in providing and facilitating psychosocial oncology services to indigenous communities.
Culture is often a restraining force, or barrier, to meeting healthcare needs in rural areas. Although 15% of minorities live in rural areas, minorities comprise over 30% of those living in rural poverty [3]. Additionally, using the lens of minority status, greater disparities exist in healthcare even when other variables are comparable. Racial and ethnic minorities not only experience higher rates of cancer, but high rates of mortality due to surgeries and advanced diagnostic stage. Warne et al. [4] state that Indigenous people experience the “worst health disparities in the nation,” (p.567) with significant cancer mortality rates. In fact, Indigenous people living in what is now known as the U.S. have the highest mortality rates from cancer than other racial groups [5].
Healthcare Delivery
Rural Indigenous people live in geographically diverse areas in the U.S., often in remote and isolated areas and face elevated rates of depression, suicide, and chemical dependency [6-8]. As the result of geographical isolation, medical care in rural Native American communities is often provided by general practitioners, rather than specialists, serving as an additional barrier in accessing psychosocial oncology services [3]. Social workers, using a multi-dimensional ecological framework, are well-versed in incorporating culture as an essential component of practice. Medical host settings for social workers often struggle with cultural responsiveness [9] which highlights the importance of including social workers in addition to biomedical providers in cancer care.
Haozous et al. [10] discuss the unique ethical challenges of studying cancer care involving patients with Tribal affiliations and interfacing with Indian Health Services. In this context, approval from a Tribal Council is often necessary, with barriers in place associated with historical unethical conduct of researchers, which makes sampling potentially challenging [10]. Yet, culturally sensitive and appropriate psychosocial research may lead to improved care, offering distress relief for Indigenous cancer patients. Social work researchers may be used to better engage and understand tribal and community systems to support appropriate research designs and methodologies in order to increase awareness of challenges faced by Indigenous cancer patients.
Social Work Education
Social work’s Educational Policies and Accreditation Standards (EPAS) require that social work students develop competency in diversity and difference in practice with individuals, families, and communities. Throughout the social work curriculum, the intersection of diversity and other factors are understood as important factors in the human experience. Ecological theory related to the nonlinear relationship of the person and the environment is a unique framework of practice that is integral to the social work field. As the lack of culturally responsive biomedical care in oncology may reduce patients’ understanding of disease, impact quality of life, and impede psychosocial well-being, social workers are essential cancer care team members in order to understand strengths, systemic influences, and resources in rural Indigenous communities. Certainly, diverse rural contexts, with increased and unique psychosocial and medical concerns, require psychosocial treatment models that may vary from the psychosocial standards outlined by the [1] Report. As the result of social work’s specialized training in understanding diversity and the person-in-environment perspective, social workers can be leaders in crafting culturally appropriate screenings, interventions, and treatment models in cancer care.
Conceptual Frameworks
Intersectionality
Intersectionality, or the overlapping and intersecting of identity and culture, is an important concept to understanding in the relationship of rurality and culture. As psychosocial cancer care is uniquely conceptualized in rural areas, the additional lens of Indigenous culture is necessary in order to understand and evaluate the intersection and relationships of environmental systems. Social work, particularly in rural areas, considers the impact and interconnectedness of terrain, geography, weather, location, cultural and economic factors on individual and family systems. Additionally, the strengths of rural populations are integrated by rural social workers in mobilization of scant resources [11]. This culturally-responsive framework for practice is integral in considering the “whole” person in cancer care with rural Indigenous people. Social workers, using a framework of intersectionality theory, would provide an essential voice as members of an oncology care team when treating cancer in rural indigenous communities.
Strengths Perspective
In the rural context, especially in regard to rural indigenous populations, much research and literature focuses on a deficits perspective [11]. In social work practice and research, the strengths perspective is commonly used in order to assist client systems in recognizing and mobilizing resources already in place. This paper includes strengths as an important component of examining psychosocial oncology in rural Indigenous communities. Although much research exists looking at healthcare disparities and the lack of resources in the rural context, conceptually, this paper is guided by the strengths perspective. When systems are viewed as more than their deficits, resources already in place may be mobilized in order to grow and develop necessary areas in order to benefit systems. Rural environments often involve isolation of individuals, and so strengths are important to consider in terms of the dependence upon talents of people and services [11]. Indigenous people, in particular, have demonstrated incredible strength and resilience in adapting to discrimination, cultural genocide, and changing environmental influence. These strengths and traditions are essential in linking cancer patients to appropriate resources. Traditional healing paradigms are often sidelined and minimized in biomedical care yet may provide important resources for distress management [5]. Social work practice uses ecological theory in forming a strengths perspective essential for working with diverse rural populations. A component of culturally responsive practice is identifying cultural strengths in micro, mezzo, and macro systems. Indigenous knowledge is an example of macro-level incorporation of cultural responsiveness, especially as it relates to Westernized biomedical protocols. Social workers, using the strengths perspective, may facilitate communication and brokering among various macro-level paradigms in cancer care, particularly among tribal members, Indian Health Services, and medical providers.
Indigenous Methodologies
A key component to research and practice with Indigenous people is the epistemological shift from Western positivist paradigms to culturally responsive paradigms, which includes indigenous knowledge. Recognizing the historical marginalization and trauma of Indigenous people, ecological theory provides a culturally responsive framework that includes components of a non-linear relationship of the mind, body, spirit, natural world, and community [12]. Research and practice with indigenous populations includes a holistic framework that is, “well-ness oriented, community-based, focused on indigenous knowledge, and designed for bidirectional learning” [12].
Literature Review
Rural Context
Barriers: Barriers exist in cancer care for people living in the rural context, perhaps most notable is the transportation barriers people face in order to access cancer care and treatment. For indigenous people who may access primary care at Indian Health Services locations, travel for specialized care may take people out of their communities for length treatment stays in metropolitan areas at large treatment centers. Humble et al. [13] These treatment centers may include additional layers of psychosocial and physical barriers, including lack of cultural responsive frameworks, limited housing options, lack of community resources [13]. Additionally, rural areas often lack psychosocial care necessary to support patients and family members while they access care and endure cancer treatments. These barriers increase risk of social, geographical, and emotional isolation and subsequent psychosocial issues for rural Indigenous people [14].
Hale et al. [15] reveal barriers in rural areas that expand on socioeconomic macro-system concerns. For one, rural areas experience “brain drain” in which educated professionals leave family systems for opportunities provided by urban and suburban environments. This not only leads to impoverished resources in rural areas, but isolation of individuals as well [15]. In terms of education, rural residents have a greater chance of dropping out of school as well as lower math achievement than urban/ suburban residents. These factors may impact understand of health-related conditions and treatments [15].
In psychosocial cancer care, Andrykowski et al. [16] identifies the above barriers and others in terms of mental health (MH) services for cancer survivors. This study discusses several rural-specific barriers impacting access to and acceptance of psychological services. These barriers include lower education and income, greater family responsibilities, reduced internet access, stigma associated with acceptance of psychological services, reduced access to health information, limited access to other cancer survivors, and greater stress and fear overall [16]. In minority rural communities, these socioeconomic, healthcare, and environmental disparities are even greater than nonminority rural communities.
Itty et al. [5] identify barriers specific to Indigenous cancer patients living in rural/ reservation. As physicians and treatments are sparse in rural areas, misdiagnosis and late diagnosis of cancer is often found in this population. Also, physical barriers such as treatment distance and lack of transportation was identified as complications of cancer care in rural areas. Supportive cancer services, such patient navigators or social workers, may be limited in access. Geographic and social isolation was also noted by Indigenous rural cancer patients. Access to specialized cancer care may be financially exhausting or unobtainable given rural-specific barriers. For example, gas and hotel expenses for travel to an urban/ academic medical center is often an overwhelming financial barrier [5].
Protective factors: Biomedical providers must mobilize community and family strengths as a way to assist patients in coping with cancer. As a protective factor, rural indigenous communities often incorporate healers in that facilitate connections among family and community systems during an illness. This healing, or traditional medicine, is often considered just as essential as chemotherapy and radiation for Indigenous cancer patients. Patients may feel as though these healing methods are not taken seriously by treatment facilities. Cultural strengths found in healing traditions may decrease distress levels in Indigenous people receiving cancer treatment. These traditional healers prevalent in rural/ reservation settings and may be used as a way to provide balance during cancer treatments [5].
Rural cultural constructs: Rural families are often socially constructed in the relationship with the land. This relationship with the land is not only found in farming families, but in an overall awareness and emphasis on weather and other environmental influences on agriculture. Sociological concepts used to better understand rural culture involve the terms “Gemeinschaft” and “Geselleschaft.” Gemeinschaft refers to the importance of the relationship of local and regional communities on family systems. Geselleschaft is the importance of the influence of the larger society. In rural areas, the concept of Gemeinschaft is important in understanding familial influences. Since individuals and families are often isolated, the impact of local communities is far greater than broader influences. Although television and internet may provide exposure connecting rural individuals and families to broader society, this exposure may seem far away and abstract [11]. For the purposes of this paper, the intersection of rural and Native culture provides a unique challenge in cancer care that increases the need for the influence of oncology social workers practicing in this context.
Culturally Responsive Care
Practice with Indigenous cancer patients involves the concept of trust, especially given the historical traumas and cultural genocide associated with this population. Haozous et al. [12] explores the concept of mistrust of clinicians as a lack of effort on the part of clinicians in cancer care to understand Indigenous culture. Results of this study indicate the need for even very basic understanding of Indigenous culture as paramount in establishing trust and improving communication between clinicians and patients. For example, Hodge et al. [17] discuss the importance of community in indigenous culture. Hospitals may limit visitors to small groups or immediate family, thus creating a sense that the community is “shut out” from patient care. This impacts trust of providers and an increased sense of patient isolation [12]. Doorenbos et al. [18] discuss the need for oncology surgeons to gain cultural competence when practicing with Indigenous people. Findings of [18] indicate surgeons place a high value on cultural competence when working with diverse patients. Although the surgeons in the study indicated a motivation to increase cultural sensitivity, the authors argue the need for a comprehensive model in cancer care for “improved, theory-based interventions to achieve the goal of genuinely culturally competent care.” [18].
Itty and colleagues [5] identify culture as a significant role in managing cancer-related symptoms in rural Indigenous communities. Indigenous people living in rural areas view providers’ understanding of Indigenous culture as lacking. This poor communication and lack of cultural responsiveness from providers contributed to a misunderstanding of course of treatments, treatment options, and treatment side effects. Additionally, the patients in the study reported feeling that questions regarding treatment decisions were often left unanswered by the medical team, who used medical terminology rather than culturally responsive communication [5]. Oncology social work may be used in facilitating and supporting cultural responsive communication between patients and biomedical providers.
Psychosocial Distress
Haozous et al. [19] discuss distress in terms of “emotional pain” experienced by Indigenous people. This emotional pain mirrors the definition of distress as it includes, “sadness, depression, existential pain, and frustration or anger with cancer, its treatment, and the overall cancer journey” (p. 1054). In the context of systems, emotional pain is exacerbated by family obligations and the importance of community. Participants in the study reported feeling isolated from family members by accepting medical treatments. In addition, fatigue and pain related to cancer treatment kept participants from participating in ceremonial and spiritual practices. Overall, the side effects of cancer treatments involve all of the above components. Haozous and Knobf [19] describe participant experiences with coping with psychosocial distress. For example, one participant in describes the difficulty of separating physical, emotional, and spiritual pain by stating, “sometimes you can’t tell the difference where you’re actually hurting” (p. 1055). Using ecological theory, an essential component of culturally responsive cancer care with indigenous communities is including historical trauma as an aspect of psychosocial distress.
Hodge et al [17] examined cancer-related fatigue (CRF) in Indigenous cancer survivors as a possible quality of life concern in this population as it was explained by the study participants as being “out of balance” (p. 1237). CRF is explained as part of a cultural construct impacting quality of life, as equilibrium, balance, and harmony are integral concepts in Indigenous cultures. Although CRF may be the result of medical treatment, study participants feared being viewed as lazy or out of balance – essentially at fault for this common side effect of treatment. Additionally, participants described CRF as a separate disease from the cancer and the result of chemotherapy, or as participants described, poisoning ones’ body. Overall, Hodge et al. [17] discussed the importance of culturally responsive interventions to CRF. Although the study did not directly cite health-care related distress, CRF closely reflects an important element of distress in terms of an experience which impacts the ability to cope with cancer.
Web-based Psychosocial Services
Shepherd et al. [20] examined the impact of a web-based brief cognitive-behavioral treatment (CBT) support group intervention for breast cancer patients. Results of the study indicated a significant improvement of quality of life, distress, and anxiety. The authors argue that a web-based model of psychosocial service delivery may serve as a viable option for patients living in remote, rural areas [20]. Doorenbos et al. [18] evaluated a web-based psychoeducational support group design specifically for Indigenous cancer survivors. The groups were facilitated by nurses or social workers and followed a curriculum focusing on educational and support needs, including how to discuss a cancer diagnosis with family members. Groups were held at various sites with videoconferencing equipment [18]. Although web-based support services have shown effectiveness in delivering psychosocial services, a larger problem exists in terms of patient access of proper technology for these services. In the rural context, a disparity exists in internet use when compared to urban areas. This includes access to high-speed internet services as well as access to technology [15].
Historical Trauma and Healthcare
Cancer care focusing on rural indigenous populations must address the issue of historical trauma related to biological, emotional, developmental, spiritual, and systemic well-being. Warne et al. [4] discuss the historical relationship of Indigenous people and Western medicine from a lens of colonization. Although the rural context may provide an environmental rationale for healthcare disparities of Indigenous Americans, the inter-generational basis for disparities must also be examined. A model for conceptualizing chronic disease brings gestational, childhood, and adulthood experiences into account for understanding and treating disease. Using this model, distress in cancer care evokes a historical trauma response where loss must be addressed and validated from a historical lens across micro, mezzo, and macro systems. The traumatic experience of cancer brings about feelings of loss of connection with ancestors and culture resulting from historic genocide [4]. Using the ecological lens coupled with indigenous culture, the relationship of past, present, and future should become integrated in treating the whole person.
Oncology Social Work
The field of oncology social work involves providing psychosocial services for cancer patients and their families. The provision of psychosocial services improves quality of life and health outcomes in regard to cancer care. Oncology social workers follow a framework of identifying and screening patients in need of psychosocial services, assessing and developing plans that link patients to resource and services, coordinating and brokering services between patients and medical providers, and monitoring and evaluating effectiveness of services provided. This last step also includes adapting services for patients as needed. Social workers in cancer care also consider how a cancer diagnosis impacts interrelated environmental systems, such as families and communities [3]. This framework for practice includes the person-in-environment perspective. In rural areas, particularly with minority populations, oncology social work is elevated in importance in terms of connecting isolated individuals and families to resources.
Social work may provide an important role in culturally responsive cancer care. Rural social workers, specifically, have advanced knowledge of navigating rural ethics and systems, especially in managing dual relationships and community contexts [3]. In addition, social workers mobilize resources in order to draw on client strengths. Many Native American communities have tremendous resiliency, which includes a strong sense of family and community. Effective partnerships that focus on community strengths may increase collaboration among cancer care clinicians and indigenous communities in order to create culturally responsive constructs. Dr. Judith Kaur, an oncology researcher focusing on Native Health states that, “tribes are taking ownership of their health care and are interested in working together in partnerships” [21]. For these reasons, social workers are important in treating the “whole” person in the context of cancer care in rural indigenous communities. Cancer does not simply involve medical treatment, but treatment of the psychosocial, cultural, environmental, and spiritual aspects of a patient [1].
Discussion
Social Work Professional Standards
Social work education in the United States is monitored by the Council on Social Work Education’s (CSWE) Educational Policies and Accreditation Standards [22] and includes nine interrelated competencies with corresponding practice behaviors that ensure the development of competent, ethical, and dynamic social work professionals. Of the nine competencies, the second competency relates to the point of this paper: that social workers are adept culturally-responsive professionals and must be included in cancer care teams that serve rural Indigenous patients in order to increase quality of life, facilitate culturally appropriate communication with biomedical providers, honor cultural heritage, and decrease healthrelated distress. Competency 2 emphasizes that social workers not only understand diversity and difference, but also how the intersection of diverse constructs shape the human experience. Furthermore, social work education includes an understanding of oppression, discrimination, marginalization, and power [22]. For Indigenous people, an understanding of historic oppression is essential in cancer care. Social workers have the practice behaviors and skills that address complex constructs related to historic discrimination.
The National Association of Social Workers (NASW) [23] has a Code of Ethics that includes ethical obligations to clients. One example of social work’s emphasis on culturally responsive practice is Ethical Responsibility 1.06: Cultural Competence and Social Diversity. This responsibility includes understanding the role of culture, recognizing cultural strengths, demonstrating cultural competence, and obtaining education related to diversity. One of the social work profession’s core values is the “importance of human relationships” [23-34]. This professional emphasis again highlights the essential use of social workers as providers of psychosocial cancer care for rural indigenous communities. Racial and ethnic minorities may even decline cancer treatment based on a perceived lack of cultural responsiveness from biomedical providers [18]. Social workers, in this sense, may provide a life-saving role in terms of building and facilitating cultural responsiveness in cancer care. In order to fully reduce healthcare disparities, biomedical systems must fully synthesize the profession of social work in micro, mezzo, and macro systems of care. This may involve including social workers in medical education systems, in leadership roles in healthcare delivery systems, and engaging patients and families within clinics and hospitals.
Cultural Responsiveness in Psychosocial Oncology
In order for social workers to provide essential culturally responsive psychosocial oncology services, the formal services that address psychosocial health needs must contain an ecological framework of practice delivery. The IOM Report [1] outlines formal psychosocial services that respond to psychosocial needs. These formal services encompass interventions including education about disease to increase understanding of treatment and treatment options, support groups, psychotherapy, self-care promotion, monitoring of health behaviors, accessing resources such as transportation, support of the family and caregivers, support for life disruptions, financial planning, and health and disability insurance support (p. 82).
Practice Framework
Given the professional educational and ethical standards of social work described above, it is essential for cancer care providers to develop culturally-responsive practice frameworks that rely on this knowledge. This need is great for Indigenous people facing a cancer diagnosis. Social workers, with culturally-responsive educational backgrounds and ethical responsibilities that include understanding diversity, are paramount to providing these services in cancer care teams. Biomedical providers, often lacking in understanding of cultural constructs, require social workers to enhance well-being and quality of life of diverse patients. Taking the role of culture, community, the environment, and past/ present/ future interactions into account, a conceptual practice framework for cancer care teams may include the following:
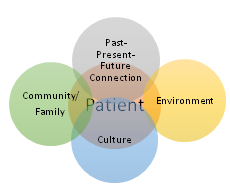
Figure: 1
Conclusion: The Whole Person
Biomedicine has created remarkable advances in cancer care. Cancer, which was once considered a death sentence, is now often a treatable disease. However, cancer technology is insufficient to manage the impact of disease on a patient’s psychological, social, and environmental systems. Ignoring psychosocial barriers impedes the patient’s ability to manage cancer treatments and negatively impacts health-related outcomes. Given the remarkably high cancer–related mortality of Indigenous people in the U.S., improved psychosocial care is needed. Using the intersection of rurality and diversity, strengths and barriers must be assessed and addressed by social workers in order to optimize biomedical care. In reviewing available research, there is scant information including social workers as providers of psychosocial services for Indigenous people facing cancer. Although biomedical providers may receive some education related to diversity, the ecological, person-in-environment framework may not be included. Social workers, given our required culturally responsive educational standards and ethical values, combined with our non-linear ecological orientation, are urgently needed as leaders in cancer care systems.
Conflicts of Interest (COI) Statement
The author has declared no conflict of interest.
References
Institute of Medicine (IOM) (2008) Cancer care for the whole patient. Washington, D.C.: National Academies Press.View
Indian Health Service (n.d.) Factsheet.View
Ginsberg, L. (2011). Social work in rural communities. Alexandria, VA: CSWE Press.View
Warne, D., & Lajimodiere, D. (2015). American Indian health disparities: Psychosocial influences. Soc Personality Psychol Compass 9: 567–579.View
Itty, T.L., Hodge, F.S., & Martinez, F. (2014). Shared and unshared barriers to cancer symptom management among urban and rural American Indians. The J Rural Health 30: 206-213.View
U.S. Department of Health and Human Services (2010) To live to see the great day that dawns: preventing suicide by American Indian and Alaska Native youth and young adults. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Bates, B. (2011). Rural Lung Ca. Survivors Face Higher Distress. Clin Psychiat News 39: 10.
Collie, K., Kreshka, M.A., Ferrier, S., Parsons, R., Graddy, K. et al. (2007). Videoconferencing for delivery of breast cancer support groups to women living in rural communities: A pilot study Psycho-Oncol 16: 778-782.View
Doorenbos, A.Z., Eaton, L.H., Haozous, E., Towle, C., Revels, L. et al. (2010). Satisfaction with telehealth for cancer support groups in rural American Indian and Alaska native communities. Clin J Oncol Nurs14: 765-770.View
Haozous, E.A., Knobf, M.T., & Brant, J.M. (2011). Understanding the cancer pain experience in American Indians of the northern plains. Psycho-Oncol 20: 404-410. View
Mackie, P.F.E., Zammitt, K., & Alvarez, M. (2016). Practicing rural social work. Chicago, IL: Lyceum Books.View
Haozous, E.A., Doorenbos, A.Z., & Stoner, S. (2016). Pain management experiences and the acceptability of cognitive behavioral strategies among American Indians and Alaska natives. J Transcul Nurs 27: 233–240.View
Humble, M.N., & Slater, G.Y. (2011). Cancer does not phase us: Exploring anxiety levels in rural oncology patients. J Human Behav Soc Environ 21: 644-653.
Thewes, B., Butow, P., & Stuart-Harris, R. (2009). Does routine psychological screening of newly diagnosed rural cancer patients lead to better patient outcomes? Results of a pilot study, Aust J Rural Health 17: 298-304.View
Hale, T., Cotton, S., Drentea, P., & Golder, M. (2010). Rural-urban differences in general and health-related internet use. Am Behav Sci 53.
Andrykowski, M.A., Steffens, R.F., Bush, H.M., & Tucker, T.C. (2014). Disparities in mental health outcomes among lung cancer survivors associated with ruralness of residence. Psycho-Oncol 23: 428-436.View
Hodge, F.S., Itty, T.L., Cadogan, M.P., Martinez, F., Pham, A. et al. (2015). The cultural constructs of cancer-related fatigue among American Indian cancer survivors. Supportive Care in Cancer, 24: 1235-1240.
Doorenbos, A.Z., Morris, A.M., Haozous, E.A., Harris, H., Flum, D.R. et al. (2016). ReCAP: Assessing cultural competence among oncology surgeons. J Oncol Pract 12: 61–62.View
Haozous, E.A., & Knobf, M.T. (2013). “All my tears were gone”: Suffering and cancer pain in southwest American Indians. J Pain Symptom Management 45: 1050–1060. View
Shepherd, L., Goldstein, D., Whitford, H., Thewes, B., Brummel, V. et al. (2006). The utility of videoconferencing to provide innovative delivery of psychological treatment for rural cancer patients: Results of a pilot study. J Pain Symptom Management 32.View
Twombly, R. (2008). Following her path, oncologist highlights issue of cancer in native Americans. JNCI J National Cancer Institute 100: 294–295.View
Council on Social Work Education. (CSWE) (2015). Educational policy and accreditation standards. EPAS Handbook. Washington, DC.View
National Association of Social Workers (NASW) (2018). Code of ethics of the National Association of Social Workers. Washington, DC.View
Galambos, C.M. (2005). Health care disparities among rural populations: A neglected frontier. Health Soc Work 30: 179-181.View
Haozous, E.A. (2010). Returning home. Creative Nurs 16: 75–77.
Haozous, E., Doorenbos, A.Z., Demiris, G., Eaton, L.H., Towle, C. et al. (2010). Role of telehealth/videoconferencing in managing cancer pain in rural American Indian communities. Psycho- Oncol 21: 219–223.View
Haozous, E.A. (2016). Cancer journey for American Indians and Alaska Natives in the Pacific Northwest. Oncol Nursi Forum 43: 625-635.View
Hepworth, H., Rooney, R.H., Rooney, G.D., Strom-Gottfried, K. (2012). Direct social work practice: Theory and skills (9th ed.). Pacific Grove, CA: Brooks/Cole.
Health Resources and Service Agency (HRSA) (2013) Illinois Department of Public Health. Center for Rural Health.View
National Comprehensive Cancer Network (NCCN) (2007) Distress management.View
Nelson, A. (2002). Unequal treatment: Confronting racial and ethnic disparities in health care. J National Med Associa 94: 666-668.View
Gitterman, A., & Germain, C.B. (2008). The life model of social work practice, advances in theory & practice (3rd.Ed.). Columbia University Press: New York, NY.View
Haozous, E.A., Eschiti, V., Lauderdale, J., Hill, C., Amos, C. et al. (2010). Use of the talking circle for Comanche women’s breast health education. J Transcultural Nurs 21: 377–385.View
Gitterman, A. (2014). Handbook of Social Work Practice with Vulnerable and Resilient Populations. Columbus University Press: New York, NY.View