
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 2 (2020), Article ID: JMHSB-114
https://doi.org/10.33790/jmhsb1100114Mini Review
TEAM-CBT and Social Work: Skills to Breakdown Client Resistance and Promote Change in Micro Practice
Fredi Giesler, MSW, Ph.D., Ashlynn Oborn*
Sociology, Social Work and Criminology, Idaho State University, 921 S. 8th Avenue, Stop 8114, Pocatello, ID 83209, United States.
Corresponding Author Details: Ashlynn Oborn, Sociology, Social Work and Criminology, Idaho State University, 921 S. 8th Avenue, Stop 8114, Pocatello, ID 83209, United States. E-mail: oborashl@isu.edu
Received date: 16th January, 2020
Accepted date: 10th March, 2020
Published date: 13th March, 2020
Citation: Giesler, F., Oborn, A. (2020). TEAM-CBT and Social Work: Skills to Breakdown Client Resistance and Promote Change in Micro Practice. J Ment Health Soc Behav 2(1):114.
Copyright: ©2020, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Social workers often struggle with how to cope with client resistance. This paper provides social workers with additional resources for reducing client resistance, increasing motivation to change, and developing an empathetic alliance with clients by introducing key concepts used in TEAM-CBT. TEAM-CBT was created by David Burn, MD to assist clinicians to identify the source of client resistance, to develop critical empathy skills to foster a healthy therapeutic relationship, and to help the client find their motivation. TEAM stands for testing, empathy, assessment of resistance, and methods. This client-centered approach aligns well with the National Association of Social Work (NASW) values and Council of Social Work Education (CSWE) practice competencies by encouraging evidence-based assessment of treatment, focusing on empathy and client validation to encourage the growth of a strong therapeutic relationship, identifying the client’s strengths that are evident in their resistance, and using client self-determination to assist in the discovery of motivation. The authors critically examine the elements of TEAM-CBT as a mental health intervention approach that is compatible with social work values and the standards for competent social work practice. This critical analysis provides social workers with guidance for empowering clients to change problematic behaviors.
Introduction
Social Workers strive to improve the mental, physical, and emotional states of their clients in order to improve the quality of life for individuals, families, communities, and society as a whole [1, 2]. Social workers apply the values of service, social justice, dignity and worth of the person, the importance of human relationships, integrity, and competence to guide their work [2]. As social workers increase their competency in practicing engagement, assessment, intervention, and evaluation they are better able to support their clients [1] through the stages of change [3, 4]. However, in working with patients and clients, social workers will occasionally meet resistance to therapeutic interventions and observe a lack of progress in the planned change process [5].
David Burns, MD studied closely with Aaron Beck during the pioneering of Cognitive Behavioral Therapy (CBT) and has developed a number of CBT techniques that are explored briefly in this paper [6]. While it is not the purpose of this paper to provide an in-depth analysis of the differences between CBT and TEAM-CBT (described below), the authors will provide an in-depth analysis of TEAM-CBT, which Burns created to work in tandem with traditional CBT approaches [7]. Originally, Burns planned to call his approach, TEAM, in order to apply it broadly to clinical mental health practice, but due to marketing advice he changed the name to TEAM-CBT to add validity and credibility to this intervention [8, 9].
Burns [6] sought to find a way to reduce or eliminate the resistance that keeps a client stuck and unable to achieve their goals. After years of clinical work and research exploring the reasons behind some individuals reporting a complete recovery and others remaining unchanged after receiving the same therapeutic techniques, Burns created TEAM-CBT [6]. In Burns’ [6] model of Cognitive Behavioral Therapy (CBT) TEAM stands for testing, empathy, assessment of resistance (formerly, paradoxical agenda setting), and methods. The purpose of this paper is to examine the intersection of TEAMCBT with the values of the National Association of Social Workers (NASW) and the practice competencies promoted by the Council on Social Work Education (CSWE). This examination will broaden social work resources for reducing client resistance and support client self-determination through a client-centered approach at the micro level of practice. While TEAM-CBT can be applied at any level of social work practice to improve empathy and interpersonal communication, to break down resistance to change and to enable clients to achieve their goals, the focus of this paper is on social work micro practice [6].
TEAM-CBT
Testing
A central element to TEAM is collecting data regarding client levels of depression, anxiety, and distress at the beginning and end of each therapy session [7]. Testing allows the social worker to evaluate the effectiveness of individual sessions in lowering client levels of distress and provides valuable data for use in guiding future treatment plans and interventions [10]. In addition, studies have shown that clients are more likely to have positive results from treatment when the clinician regularly collects data from their sessions [10]. Observing even minute improvements throughout the course of a therapeutic intervention can serve as a powerful motivator for clients in their continued progress [12]. In contrast, when feedback from data collected routinely shows no improvement, or a decline in client self-reported progress the social worker can be alerted to the ineffectiveness of the current treatment approach and collaborate with the client to implement a new course of action [12]. Burns and Burns [7] argues it is unethical for a therapist to provide therapy without routinely collecting client feedback on progress. The testing process is critical in both assessing the effectiveness of the intervention, as well as to identify the client perception of the quality of the relationship with the therapist [7].
Burns has created a variety of short assessment tools to aid in this assessment process. These include the Brief Mood Survey (BMS), Suicidal Urges Scale, and Evaluation of Therapy Session [7,13]. The authors have been unable to confirm the psychometric efficacy of these specific measures, as they have yet to be evaluated, however, a variety of equivalent, psychometrically validated tools are available, including: Beck Anxiety Inventory [14], Generalized Anxiety Disorder Screener (GAD-7) [15], Beck Depression Inventory Second Edition [16], and the Real Relationship Inventory (RRI-C) [17].
Empathy
Burns and Burns [7] encourage the use of testing to measure the quality of the therapeutic relationship and the extent to which the clinician is capable of empathizing with the client. Research suggests that the concept of empathy is a complex interaction to measure [18]. However, research has found that the client’s opinion of the therapist’s ability to empathize is an important predictor of client outcomes, but may be perceived differently by the client and the therapist [7, 18, 19]. At times, the therapist may be surprised to learn that their client did not feel connected or heard in a session, or conversely that the client felt a greater connection than what was initially perceived. This correlates with the prevailing research on empathy which has found that while a client and the clinician may report similar views of their ability to collaborate, their views of the therapeutic bond are rarely the same [20]. Research suggests that when the social worker is aware of the differences they were rarely, or often inadequately explored with the client [20]. Burns [21] has suggested that most clinicians are threatened by the client’s opinion of their work. If the perceptions of the client and social worker differ there is an increased likelihood for termination or limited progress on client outcomes [22], but when client perceptions are similar to the social worker it is probable that the client will experience positive outcomes [23]. Social Learning Theory suggests that the client is motivated to achieve their goals, in part, due to the positive relationship they have with the social worker [24].
In an effort to foster the development of empathy skills and facilitate a strong therapeutic alliance, Burns teaches clinicians the Five Secrets of Effective Communication [7, 25]. According to Burns [7, 25] The Five Secrets of Effective Communication can be applied in any order, but in order to be effective, the social worker must be genuine and sincere [7, 25]. These skills include: The Disarming Technique, Thought and Feeling Empathy, Inquiry, “I Feel” Statements, and Stroking [7]. Each of these strategies are explained below.
The Disarming Technique includes identifying and acknowledging the truth in the other person’s experience, regardless of what the social worker perceives [7]. This skill is critical for lowering the defenses of the client and reducing resistance [7]. Thought Empathy is the use of paraphrasing what the client has said to both confirm correct understanding and to help the client see that the social worker is engaged and interested in what the client is saying [7]. Feeling Empathy involves the social worker verbally acknowledging and reflecting the feelings they perceive the client is experiencing [7, 25]. The social worker asks the client probing questions (Inquiry) to encourage the client to share more about their experience and their feelings [7, 25]. The social worker will experience their own feelings in regards to what is shared by the client during this exchange, but usually the social worker would not share their feelings. However, Burns encourages the social worker to thoughtfully share their feelings in response to what the client reports [7, 25]. For example, the social worker might say, “I’m feeling surprised by what you have shared.”, or “I’m feeling sad about what you have experienced.” Carl Rogers [26] also encourages the social worker to be genuine and fully aware of their own feelings when working with clients. Burns and Burns [7] and Rogers [26] learned from their clinical work that by sharing their perceptions with the client a stronger therapeutic alliance and improved client selfawareness resulted. For example, the social worker might say, “It seems like we will be able to work well together.” Stroking, or giving affirmations, is applied by the social worker throughout communication with the client to convey genuine respect and recognition of client strengths [7]. The social worker’s unconditional positive regard conveys acceptance of the client just as they are [26]. Rogers [26] hypothesized that only when the therapist is genuine and empathetic will change be able to occur.
Assessment of Resistance (Paradoxical Agenda Setting)
According to Burns and Burns [7] Assessment of Resistance is critical for understanding client motivation to change. Client resistance to the therapeutic experience is often regarded by clinicians as the reason for the lack of success during sessions and decreases the clinician’s ability to implement the interventions and techniques in a competent way [27, 28]. It is possible that client resistance is heightened when the social worker actively offers advice and solutions for solving the client’s problems [29]. Social workers struggle with identifying the motivators for client resistance and would benefit from specific training in identifying and processing client resistance [29]. Motivational techniques have proven helpful in minimizing resistance and producing favorable outcomes for the client [13, 30]. The client may struggle with change due to ambivalence or being conflicted about alternatives. When the social worker begins to advocate in favor of change the client is likely to choose to argue or resist the change [30, 31]. Burns and Burns [7] suggest that engaging in efforts to persuade the client to change results in more strenuous resistance.
During Assessment of Resistance the therapeutic relationship shifts to a greater focus on problem-solving with the client [7]. The social worker engages in a four-step process to explore outcome and process resistance for depression, anxiety, relationship issues and addictions [7]. Step one: the client is invited to identify their level of readiness to begin to problem solve. Step two: if ready to move forward, the client identifies a specific problem they wish to work on during the session, including details and examples of when this problem has manifested. Step three: the social worker then conceptualizes the type of problem as a mood problem, relationship problem, habit or addiction, or a non-problem (i.e., unexpressed grief) in order to explore the possible form of resistance the client may experience [7]. Step four: the social worker explores with the client Outcome Resistance- a reluctance to change how things are, and Process Resistance- a lack of desire to go through the needed steps to change [7]. For example, the client may have identified a problem with addiction, but may have some ambivalence about whether they want to give up the addiction and/or may dread the process of abstaining from mood altering substances. Similar to Motivational Interviewing (MI) [30], the social worker seeks to guide the conversation to allow the client to express their reason or desire to change. If applied to the Stages of Change Theory, clients may be in the precontemplation or contemplation stage and feeling ambivalent about making a change, which indicates the client may not be ready to focus on goal achievement [4]. It will be ineffective for the social worker to begin problem solving or introducing interventions if the client is ambivalent toward change; the client must be ready, willing, and able to engage in the relevant intervention approach [7].
Methods
Burns and Burns [67] found that through the use of empathy and assessment of resistance, client resistance is removed, client motivation identified, and the client becomes ready to engage in the intervention process. Burns has identified over 50 techniques, exercises, or methods for use during intervention to help with primary mental health issues, including problematic habits, depression, anxiety,relationship problems, and addictions [7, 13]. Some of these techniques include: the Daily Mood Log, Identify the Distortions, the Externalization of Voices, the Acceptance Paradox, the Paradoxical Double Standard Technique, the Hidden Emotion Technique, Cognitive Flooding, the Feared Fantasy, the Relationship Journal, the Interpersonal Downward Arrow, the Intimacy Exercise (one minute drill), the Addiction / Habit Log, and the Devil’s Advocate Technique (for more information on these specific approaches see the reference list) [13]. Many of these strategies and approaches have been given stimulating titles, but include strategies that are: compassion-based, truth-based, logic-based, humor-based, use semantics, quantify behaviors, use role-playing, explore philosophical/ spiritual activities, use visual imaging, explore motivation, apply classical or cognitive exposure, use interpersonal exposure, and apply interpersonal techniques [7]. The authors suggest there is a need for further research on the efficacy of these specific exercises, assessment tools and techniques.
The type of problem the client is seeking assistance with will determine which intervention is most appropriate. Much of Burns’ work includes the use of Cognitive Behavioral Therapy (CBT) [32] but TEAM can easily be applied to any intervention approach [7]. By using cognitive, motivational, exposure, and interpersonal techniques the social worker is able to introduce new skills and coping strategies to the client [7]. Not only will the effectiveness of the technique depend on the type of problem identified, but interventions vary by individual, as a technique that works for one individual may be less effective for another, making it critical for the social worker to be familiar with a wide variety of exercises, techniques and tools [7].
Social Work Values
Many factors are barriers to frequent family meals. These include sociocultural influence, busy schedules, home environment, activities schedule, work schedule, location, psychosocial stress, unhealthy eating habits, low social support, poor relationships, food availability, and financial incapability [16]. The media and sociocultural influence also play a role in triggering social pounds. The more often people turn to the media, the more often their perception of themselves may worsen [15].
Perpetuates & Protective Factors
The social work profession embraces six primary values that guide competent practice [2]. These are defined by the membership of the National Association of Social Workers (NASW) and include: integrity, competence, dignity and worth of the person, importance of human relationships, social justice and service [2]. Competent social workers demonstrate these values in their work with clients and constituents. The degree of compatibility of these values with TEAM-CBT is described below.
Integrity
Integrity is defined as a dedicated adherence to the mission, values and ethical principles of the social work profession [2]. Integrity is associated with honesty, morality, virtue, and uprightness [33]. Social workers strive to act in honest, trustworthy, and responsible ways when working with individuals, groups, communities, policy implementation and agency management [2]. Integrity also involves upholding the NASW Code of Ethics, including a commitment to the wellbeing of clients, colleagues, service providers, other professionals and the community [2]. The TEAM-CBT use of testing to guide the intervention process is indicative of practicing with integrity.
Competence
It is the responsibility of the social worker to pursue an eclectic knowledge base and develop competency within their area of practice [2, 34]. Social workers limit their work to areas where they have engaged in specific study, training, and supervision provided by expert professionals [2]. It is the responsibility of the social worker to stay current with new research on evidence-based practice published in professional journals, conference proceedings, and books [2]. The TEAM-CBT use of testing and evidence-based intervention methods and strategies is indicative of practicing with competence.
Dignity and worth of the person
Social workers strive to develop respect and appreciation for all people through the broadening of their understanding of cultural and ethnic diversity [1, 2]. Competent social workers treat individuals with care and respect, and acknowledge their strengths and value as human beings [2, 35]. Effective social workers recognize and employ the strengths, abilities and resources of the client to facilitate change and empower the client [35, 36]. All people possess strengths and resources that often go unrecognized. Social workers acknowledge these strengths and employ them to assist a client with achieving their goals [1]. Graybeal [37], was often surprised by the strengths, skills, and abilities of clients and recognized that these resources can lead to solutions for difficult problems. The TEAM-CBT attention to empathy and assessment of resistance are indicative of respecting self-determination and respect for client individuality.
Social Work Practice Competencies
Social Work education in the United States is founded on a set of nine practice competencies (professional identity and ethics, diversity practice, social justice, research, policy, engagement, assessment, intervention and evaluation) that offer consistent indication that people with a social work degree have the knowledge, skills, values, and critical thinking to effectively work with clients and constituents [1]. Five (diversity practice, engagement, assessment, intervention and evaluation) of these competency areas align with the TEAMCBT model and are described below.
Diversity
Clients identify with an ethnic, religious, sexual orientation, gender, age, ability, or economic resource group, which impacts their perceptions and their relationship with the social worker [40]. Likewise, social workers have an identity and personal experiences that impact how they view their clients and the nature of the relationship that they cultivate [40]. Competent social workers consider how power dynamics, privilege, marginalization, oppression and institutional structures influence how clients perceive opportunities,and the relevance of engaging in the change process [1]. Effective social workers must be aware of the impact of their own experiences on the therapeutic relationship, must see clients as experts of their own lives, and manage their personal biases [1]. The TEAM-CBT attention to empathy, assessment of resistance and implementation of individualized intervention strategies are indicators of commitment to diversity practice.
Engagement
Client engagement is indicated by their willingness to actively participate in treatment [42]. Social workers competently engage with clients and build a therapeutic relationship using empathy, personal reflection, and professional interpersonal skills [1]. Competent social workers have a working knowledge of human development, intervention theory, and interdisciplinary practice in order to understand the antecedents of behavior and effectively meet clients where they are [1]. All the elements of the TEAM-CBT model focus on continuous client engagement.
Assessment
Assessment is the act of collecting information from the client, their family and friends, other agencies, and where appropriate, community sources (i.e., teachers, principals or school counselors) [35]. This is done in order to identify client challenges and strengths, and gain a greater understanding of client mental and emotional well-being, social functioning, physical health status, interpersonal relationships, support systems, and other environmental influences that may be contributing to (or provide potential solutions for) their presenting problems [1, 35]. Competent social workers apply their knowledge of intervention theories to evaluate the information gained through the assessment process and apply it to the treatment plan [1]. Social workers partner with clients to set goals that are mutually developed and agreed upon with the client [1]. The TEAM-CBT focus on testing, assessment of resistance and implementation of individualized intervention strategies is aligned with competent social work assessment practice.
Intervention
Social workers use their knowledge of theory and evidence-based practices to assist the client in achieving their goals, increase their ability to cope with life stressors, and develop problem solving skills [1, 35]. Intervention with individuals and families often includes case management and connecting the client to needed resources and social support [35]. Appropriate interventions may also include assisting the client to change their thinking and/or behavior [41]. The TEAMCBT attention to the assessment of resistance and the implementation of individualized intervention strategies are indicators of competent intervention practice that is led by the client.
Evaluation
The intervention process should be evaluated routinely throughout the treatment process [1]. Monitoring client progress and outcomes allows the social worker to document the impact of the intervention [35]. Evaluation of services using qualitative and quantitative methods, provides social workers with critical feedback regarding their effectiveness in producing desired outcomes [1]. The TEAMCBT attention to on-going testing of client mood and the client-social worker bond are indicators of commitment to competent evaluation of practice outcomes.
TEAM Social Work
The remainder of this paper presents a practice model of TEAM Social Work, which integrates the evidence-based TEAM-CBT model with social work values and competent social work practice [1, 2, 9]. The following matrix illustrates how these systems intersect and this paper suggests how social workers can effectively apply this model for competent and evidence based social work practice. The model provides guidance for effectively engaging with clients and reducing their resistance to change, thus, increasing client motivation and commitment to goal achievement.
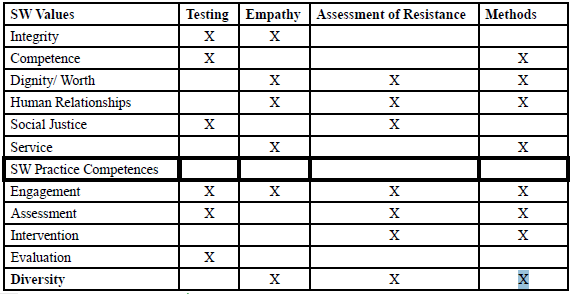
Figure 1. TEAM Social Work: A Practice Framework
Where TEAM-CBT Intersects with Social Work
Social work embodies the use of evidence-based practice and strives to use research as a guide to the implementation of assessments, interventions, and programs [1]. As outlined by the Council on Social Work Education (CSWE), a social worker must have a proficiency in both producing and applying research in order to be competent [1]. The competent social worker can integrate and effectively apply knowledge, values, and skills to a variety of practice contexts in order to promote client well-being [1]. Competent social workers use logic and scientific inquiry to assess the effectiveness of their work and to apply research findings to improve the effectiveness of their practice [1]. Thomas O’Hare [35] suggests that a competent social worker is an informed, critical thinker who combines their knowledge from research and evidence-based practice to facilitate client problem-solving. Competent social workers derive evidence-based intervention from the research literature and apply it in congruence with client values and preferences [43].
Social Work Values
Testing intersects with the social work values of integrity, competence, and social justice. The social work value of integrity requires the social worker to interact in a trustworthy and honest manner,and with an awareness of their responsibility to understand what their client needs [2]. Testing provides the opportunity to assess the accuracy of the social worker’s perceptions of the client and their challenges, bringing awareness to the social worker’s behaviors and how they are impacting their client [19].
It is critical for the social worker to be honest regarding their competence in meeting the needs of the client [2]. Social workers seek new learning and develop new skills, while being sure to practice within the confines of their expertise [2]. Testing can provide the needed feedback for assessing social worker competence in a specific area and show where added supervision or training may be needed. For example, when meeting with a female client struggling with depression, Dr. Burns perceived the client had made amazing progress in their sessions as she began to present as happy and full of high self-esteem [7]. In preparation to use her case as an example in a future training seminar he asked her to fill out a BMS and was shocked when her depression score was incredibly high. He used this information to explore what he had missed, genuinely expressing to the client that he must have dismissed something that was important. His client then shared that as a child she had been abused by her father, who would throw her against the walls of their home [7]. This was new information that had not previously been shared in this therapeutic relationship. A large part of practicing with competence is for the social worker to have the right information and not rely solely on their own impressions of the client or their situation [18].
Social Work Competencies
Testing the client’s current emotional status provides a structure for engaging with the client. This approach communicates that the social worker is not making any assumptions about how the client is feeling and collecting data allows for a nonjudgmental opening in the interaction. However, testing also comes with some cultural baggage that the social worker needs to consider. Some clients may view testing as a way to label and denigrate them [44]. Testing may prompt an inhibitive, emotional reaction to past feelings of trauma and oppression [41]. A competent social worker clearly and compassionately explains the purpose of testing and the control that it offers the client in the therapeutic relationship.
Testing is designed to tell the social worker about the client’s needs and to identify the degree of empathy the client is experiencing. In the TEAM-CBT model, Burns and Burns [7] recommend completion of the BMS [13] prior to the beginning of the meeting between the client and the social worker (in the waiting room). Though the reliability and validity of this tool has not been critically examined in controlled research, this tool is intended to provide feedback on how the client is feeling at that moment and can help guide a session into areas most relevant to their immediate emotional state. In practice the social worker and the client review the client’s responses at the beginning of the session. For example, in the waiting room a client might rate themselves a 20/20 on the question: How depressed do you feel right now? [13]. This score provides an opportunity for the social worker to ask the client to describe the experiences that led to this rating. The social worker does not engage in problemsolving, or diagnosis, or goal setting at this initial point in the session. A competent social worker is focused on developing a relationship with the client, connecting with them and demonstrating caring, compassion, and commitment toward the client [45].
While the research evidence for the validity of the BMS may be quite limited, there are numerous screening tools that a social worker can use in substitute for the BMS, which can also assess the client’s current mood and be employed in a similar fashion. As noted above, the Beck Anxiety Inventory [14], Generalized Anxiety Disorder Screener (GAD-7) [15], and the Beck Depression Inventory Second Edition [16] accurately measure client mood. In some instances, it might be appropriate for the social worker to help the client complete the survey, especially if the client has visual, reading, or cognitive limitations. Testing allows the social worker to gain a better understanding of the client’s environment and experiences that might be contributing to the client’s present mood.
Social workers value the dignity and worth of the individual and demonstrate concern and respect for client challenges and unique qualities [2]. It is critical for a social worker to have the ability to place themselves in the shoes of their client in order to better understand their needs and concerns in preparation for the creation of an effective intervention plan [46]. To become competent, a social worker must develop the ability to build relationships using interpersonal skills, reflection, and empathy [2]. These abilities will improve as the social worker’s personal values reflect the importance of the worth of the individual and of human relationships [1]. In fact, the degree of empathy and the quality of the relationship between the client and the social worker is a predictor of client outcomes [18, 19].
Burns and Burns [7] recommend that the social worker use a standardized measure to check in with the client and gauge their feelings of acceptance and understanding. The social worker might use the Real Relationships Inventory [17] or the Working Alliance Inventory [47]. Both are validated and reliable measures of the quality of the therapeutic relationship [18]. In fact, Burns has developed a measure of therapist empathy, which may be useful, since the client’s perception of empathy is the most valid measure of actual empathy [7, 18]. If the client perceives that the therapy session was helpful, then it was to them.
Diversity Practice
As the social worker begins to understand what is potentially influencing the client’s current mood and what may have motivated the client to seek social work services, the social worker is mindful of client cultural connections and identity [1]. Competent social workers demonstrate cultural sensitivity and validate the client as an expert in their own life experiences [1]. This recognition comes through active listening, being fully present with the client during the meeting and by having a general knowledge base of the community and population that is frequently served by the social service agency/ social worker [1]. This understanding should not be confused with the application of stereotypes or making assumptions about the client, but rather should guide the social worker in gaining a better understanding of client circumstances. Competent social workers maintain a person-in-environment focus and understand that social context influences the way a client perceives their circumstances [1, 40]. Acceptance and validation of client perspectives can result in the client perceiving that the social worker has empathy for the client [17, 48].
Social Work Values
Integrity, dignity and worth of the person, importance of human relationships and service are all identifiable in the skills introduced in Burns’ empathy training [7]. To effectively empathize, a social worker needs to understand their client’s experience and view things from their client’s perspective. Through this process a deep and engaging relationship can grow between the social worker and the client. This process is strengthened by social worker knowledge and understanding of the dignity and worth that is innate in the client they are serving. Using David Burns’ Disarming technique, responding with Thought and Feeling Empathy, and Inquiry, the social worker is better able to understand from the client’s perspective what they need [7]. David Burns allowed a medical student to observe a session with a client who frequently experienced psychotic episodes and who with Burns had made little progress [49]. During the session the client began to share how he had seen John the Baptist on his way to the session and received secret information that he was directed to share with other humans. Burns initially thought he would need to increase the client’s medications due to this perceived psychotic episode, but instead asked the medical student to share his thoughts. After a long pause, the medical student said to the client that if John the Baptist had a special message he would want to hear that message. The client became excited as he related his perceived conversation with John the Baptist. Because the medical student demonstrated respect for the client and his perspective, the client went on to share that he struggled deeply with sexual urges and difficulty with friendships because he didn’t believe he fit in anywhere [49]. At the end of the session the client identified that it had been the most helpful of all their sessions. As social workers validate and show an interest in the client’s perspective the therapeutic alliance will be strengthened, and they will better see life from the perspective of the client [18, 19].
Critical to the success of the intervention is the formation of a therapeutic alliance where the client feels the social worker will be honest, caring, and compassionate in their responses to client challenges [19]. Integrity can be seen when the social worker shares their own feelings about what the client is saying and demonstrates genuine regard for the client. For example, Dr. Burns shared a story on his podcast of a time he met with an individual who frequently made offensive jokes [50]. These jokes included the client jesting about Dr. Burns and himself going into the community and sexually assaulting women. Dr. Burns reported that he began to dread meeting with this client due to his level of discomfort. Dr. Burns chose to express his feelings of discomfort directly to the client and shared how he felt disconnected from the client. Dr. Burns asked the client if he had received any similar feedback from anyone else in his life and the client confirmed that he had and that he struggled with making connections with other people. Dr. Burns’ willingness to be open and discuss his feelings with the client led to deeper understanding of the client’s challenges with interpersonal relationship skills and strengthened the therapeutic relationship [7].
As a social worker is open and honest with their clients about the feelings that arise in therapy, they can bring awareness to potential problems that are occurring outside of their sessions. The genuineness of the relationship fosters a deep connection and a trusting relationship between the social worker and the client, and models how such relationships can be formed with others in the client’s life [26]. It is deeply critical, according to Burns and Burns [7], to show respect and a genuine liking for the client and is best accomplished as the social worker acknowledges the individual's inherent worth and strives to express this worth by identifying client strengths. It is also important for the social worker to remember that the value of service holds that the therapeutic relationship is for the benefit of the client and not the social worker [2]. It is critical that the social worker is mindful of this value when sharing their own feelings and experiences in a therapeutic setting.
Social Work Competencies
Competent social workers are empathetic to the needs of their clients [1, 19]. Demonstrating empathy is an important component of engaging with clients [1, 19]. Social workers must be able to accept, without judgement, the needs and concerns that clients bring to them, and they must seek feedback from the client to confirm that they have made a connection with the client [1, 17]. Seeking client feedback can be intimidating, but is vital to the therapeutic relationship [19, 45]. Social workers apply active listening skills and feelings reflection to confirm that they are effectively engaging with the client [45].
Assessment of Resistance
Social worker, Alex Gitterman [5] identifies that when a social worker labels a client as resistant there is a tendency to use this as an excuse to avoid making necessary changes to themselves or their agency. He encourages social workers to view client resistance as a transactional process in which each person affects and impacts the other, where the social worker encourages feedback regarding client experiences with the social worker and explores difficulties when they arise throughout the therapeutic relationship [5].
Assessment of Resistance is an opportunity for the social worker to encourage client selfdetermination and allow clients to take the lead in their own change process [2]. In the TEAM-CBT model the client is encouraged to examine what is valuable and rewarding about the behaviors they want to change [9]. Burns and Burns [7] engage the client in a type of cost benefit analysis of these behaviors and encourage the client to make an informed decision about changing them. This approach to establishing a set of goals is strengths-based and encourages the client to see how their problems can expose their greatest strengths [34].
Diversity Practice
As the social worker begins to understand what is potentially influencing the client’s current mood and what may have motivated the client to seek social work services, the social worker is mindful of client cultural connections and identity [1]. Competent social workers demonstrate cultural sensitivity and validate the client as an expert in their own life experiences [1]. This recognition comes through active listening, being fully present with the client during the meeting and by having a general knowledge base of the community and population that is frequently served by the social service agency/ social worker [1]. This understanding should not be confused with the application of stereotypes or making assumptions about the client, but rather should guide the social worker in gaining a better understanding of client circumstances. Competent social workers maintain a person-in-environment focus and understand that social context influences the way a client perceives their circumstances [1, 40]. Acceptance and validation of client perspectives can result in the client perceiving that the social worker has empathy for the client [17, 48].
Social Work Values
Integrity, dignity and worth of the person, importance of human relationships and service are all identifiable in the skills introduced in Burns’ empathy training [7]. To effectively empathize, a social worker needs to understand their client’s experience and view things from their client’s perspective. Through this process a deep and engaging relationship can grow between the social worker and the client. This process is strengthened by social worker knowledge and understanding of the dignity and worth that is innate in the client they are serving. Using David Burns’ Disarming technique, responding with Thought and Feeling Empathy, and Inquiry, the social worker is better able to understand from the client’s perspective what they need [7]. David Burns allowed a medical student to observe a session with a client who frequently experienced psychotic episodes and who with Burns had made little progress [49]. During the session the client began to share how he had seen John the Baptist on his way to the session and received secret information that he was directed to share with other humans. Burns initially thought he would need to increase the client’s medications due to this perceived psychotic episode, but instead asked the medical student to share his thoughts. After a long pause, the medical student said to the client that if John the Baptist had a special message he would want to hear that message. The client became excited as he related his perceived conversation with John the Baptist. Because the medical student demonstrated respect for the client and his perspective, the client went on to share that he struggled deeply with sexual urges and difficulty with friendships because he didn’t believe he fit in anywhere [49]. At the end of the session the client identified that it had been the most helpful of all their sessions. As social workers validate and show an interest in the client’s perspective the therapeutic alliance will be strengthened, and they will better see life from the perspective of the client [18, 19].
Critical to the success of the intervention is the formation of a therapeutic alliance where the client feels the social worker will be honest, caring, and compassionate in their responses to client challenges [19]. Integrity can be seen when the social worker shares their own feelings about what the client is saying and demonstrates genuine regard for the client. For example, Dr. Burns shared a story on his podcast of a time he met with an individual who frequently made offensive jokes [50]. These jokes included the client jesting about Dr. Burns and himself going into the community and sexually assaulting women. Dr. Burns reported that he began to dread meeting with this client due to his level of discomfort. Dr. Burns chose to express his feelings of discomfort directly to the client and shared how he felt disconnected from the client. Dr. Burns asked the client if he had received any similar feedback from anyone else in his life and the client confirmed that he had and that he struggled with making connections with other people. Dr. Burns’ willingness to be open and discuss his feelings with the client led to deeper understanding of the client’s challenges with interpersonal relationship skills and strengthened the therapeutic relationship [7].
As a social worker is open and honest with their clients about the feelings that arise in therapy, they can bring awareness to potential problems that are occurring outside of their sessions. The genuineness of the relationship fosters a deep connection and a trusting relationship between the social worker and the client, and models how such relationships can be formed with others in the client’s life [26]. It is deeply critical, according to Burns and Burns [7], to show respect and a genuine liking for the client and is best accomplished as the social worker acknowledges the individual's inherent worth and strives to express this worth by identifying client strengths. It is also important for the social worker to remember that the value of service holds that the therapeutic relationship is for the benefit of the client and not the social worker [2]. It is critical that the social worker is mindful of this value when sharing their own feelings and experiences in a therapeutic setting.
Social Work Competencies
Competent social workers are empathetic to the needs of their clients [1, 19]. Demonstrating empathy is an important component of engaging with clients [1, 19]. Social workers must be able to accept, without judgement, the needs and concerns that clients bring to them, and they must seek feedback from the client to confirm that they have made a connection with the client [1, 17]. Seeking client feedback can be intimidating, but is vital to the therapeutic relationship [19, 45]. Social workers apply active listening skills and feelings reflection to confirm that they are effectively engaging with the client [45].
Assessment of Resistance
Social worker, Alex Gitterman [5] identifies that when a social worker labels a client as resistant there is a tendency to use this as an excuse to avoid making necessary changes to themselves or their agency. He encourages social workers to view client resistance as a transactional process in which each person affects and impacts the other, where the social worker encourages feedback regarding client experiences with the social worker and explores difficulties when they arise throughout the therapeutic relationship [5].
Assessment of Resistance is an opportunity for the social worker to encourage client selfdetermination and allow clients to take the lead in their own change process [2]. In the TEAM-CBT model the client is encouraged to examine what is valuable and rewarding about the behaviors they want to change [9]. Burns and Burns [7] engage the client in a type of cost benefit analysis of these behaviors and encourage the client to make an informed decision about changing them. This approach to establishing a set of goals is strengths-based and encourages the client to see how their problems can expose their greatest strengths [34].
Diversity Practice
Competent social workers are sensitive to the impact that discrimination, oppression and social injustice play in the development of the therapeutic relationship [1]. Clients may be resistant to change because not trusting authority figures has offered them personal protection in prior relationships [40]. There is always a power differential between the social worker and the client, no matter how egalitarian that a social worker may relate to the client [45]. Competent social workers are aware of such differences and of their own limitations in understanding the client’s experiences [1]. The social worker must rely on the client to articulate the source of their resistance and reluctance to engage in the change process [1]. This respect for client expertise facilitates effective engagement with clients [1].
Social Work Values
If the social worker begins to problem solve before having listened, empathized, and validated the client’s feelings, the client is likely to become resistant [7, 29]. This resistance inhibits the client’s ability to apply any new coping or problem-solving strategies [19]. It is critical for a social worker to first empathize and assess the resistance of the client prior to stepping into problem solving. Only when the client has felt heard and when the resistance has been identified and motivation established will the client be open and willing to engage in problem-solving [19].
The social worker may feel it is their responsibility to facilitate motivation for their client to change; however, trying to persuade the client to be invested in services often increases resistance [51]. It is not the responsibility of the social worker to convince the client to work with them, rather it is the client who should convince the social worker to work with them [7]. Assessment of resistance provides a social worker with the ability to identify possible benefits to the client’s identified problem, as well as identify strengths that can be attributed to this resistance. For example, a client who is struggling with anxiety may be committed to perfectionism, which can be framed as striving to do the best, or a willingness to set and achieve goals. When the social worker labels the client’s identified problem as a strength, they validate the client’s resistance, which in turn allows the client to relinquish their resistance. The social worker is now positioned to engage the client’s willingness to do the work necessary to overcome the identified problem (process resistance) and achieve their desired outcome (outcome resistance) [7]. It is also important to note, clients who are willing to complete homework and practice skills outside of therapy sessions see the most improvement [52]. Burns and Burns [7] recommend that if the client continues to be reluctant to change their behavior they may not be ready to engage in behavior change and the social worker should continue to seek to understand the client’s perspective and focus on empathizing with the client.
Social Work Competencies
Competent social workers join with the client to determine the focus and priority of the therapeutic relationship [1]. The social worker engages with the client to develop a clear understanding of the goals and expectations, and any barriers to achieving the goal [1]. This process requires the social worker to spend a considerable amount of time collecting information from the client, clarifying and reflecting this information back to the client to establish a clear treatment plan [1]. This phase of the therapeutic relationship cannot be rushed, particularly if the social worker expects the client to be in full agreement with the treatment plan [45]. Clients must have a minimum level of motivation to achieve a goal or solve a problem [3]. A comprehensive assessment that affords the client and the social worker a clear understanding of the issue that motivated the client to seek social work services will effectively inform the intervention phase of the therapeutic relationship [45].
Methods
Generalist social workers seek to develop an eclectic knowledge base from which to consult throughout their professional career [34]. To expand this knowledge base, social workers immerse themselves in learning and implementing evidence-based interventions from a broad array of theories and applying those theories at the micro, messo, and macro levels [1]. These theories may include, but are not limited to, CBT [32], Dialectical Behavior Therapy (DBT) [53], Mindfulness [54], Group Therapy, Emotion-Focused Therapy (EFT) [55], Acceptance and Commitment Therapy (ACT) [56], Motivational Interviewing (MI) [30], Psychodynamic, Narrative Therapy [57], and Play Therapy [58].
Diversity Practice
Social Work evidence-based interventions include client preferences and are sensitive to cultural diversity [1, 59]. Power dynamics, historical and institutional discrimination, and personal experiences and values will impact client perceptions of the efficacy of a given intervention [40]. The social worker must be aware of these factors and explore with the client their perceptions of the intervention method used and its applicability to the client’s situation. Competent diversity practice means that the social worker behaves as a student of the client and views the client as an expert in their own life experiences [1]. While TEAM-CBT suggests over 50 different micro interventions, not all of these are appropriate for each client and the competent social worker is sensitive to these differences [1, 7].
Social Work Values
After the client’s motivation has been realized and their resistance has been addressed through the exhaustive assessment of resistance, the social worker is able to begin using intervention strategies, as the client will be much less resistant to learning and developing new skills [5, 7]. However, it is important for the social worker to partner with the client to identify the most appropriate intervention strategy [1]. Additionally, for the social worker to effectively incorporate interventions they must have developed competency through supervision and training [1, 2]. Social workers seek to provide services to their clients that will help them become resilient and develop sustainable problem-solving skills that enable the client to face future challenges independent of the social worker. Intervention strategies should be designed to assist the client to function well within their own interpersonal network, rather than focused on success in the clinical setting. Some interventions require the social worker and the client to practice new behaviors in the community or in non-traditional location, e.g. elevators or other public spaces [7].
Many of the case examples that Dr. Burns shares in his training sessions and podcasts involve pushing clients to engage in intervention strategies that the client perceives as terrifying, e.g. immersion and flooding exercises to cope with anxiety [7]. This is the point at which the quality of the relationship between the client and the social worker is crucial. The client and the social worker must be prepared to try and fail at different strategies in order to assist the client to meet their goal. This approach requires a trusting relationship, empathy, compassion, and practice competence [1]. These qualities reflect the social work values of competence, respect for the dignity and worth of the person, and service [2].
Social Work Competencies
The myriad interventions suggested by the TEAM-CBT model are generally based on rigorous research and scientific evidence [7]. The competent social worker joins with the client to select the best intervention approach for their identified problems and desired goals [1]. Many of the micro interventions suggested by the TEAM-CBT model come from a Cognitive Behavioral orientation, in that the social worker is facilitating a change in client thinking and cognitive distortions that are impacting their behavior [41,60].
Social workers may develop a primary theoretical practice orientation, but the competent social worker understands that the context of the problem and the selected intervention will impact the outcome [45]. In order to be effective, the social worker must discover what works, for whom, under what circumstances, and be mindful of the individuality of each client [2]. The TEAM-CBT approach to intervention fits well with this philosophy and supports the social worker to engage in continuing education and professional development [7]. Continued education ensures that the social worker develops a wide array of intervention skills, strategies and techniques to effectively meet the needs of their diverse clients [1].
Implications
When working with clients the social worker is often in a position of power or viewed as the expert in the room, which is likely to increase client resistance to change [5]. In contrast, when the social worker has developed the ability to empathize, validate, and allow the client to take the lead, the client becomes empowered to change [19]. Resistance comes when the client avoids change due to the difficulty of the process required to overcome or face the challenge, or when they are not committed to the expected outcome [9]. Regardless of the source of the resistance, the client is in control of the change process and it is important for the social worker to accept this reality and explicitly acknowledge it. This approach honors the value of client self-determination [2]. When the social worker and the client can develop a realistic and mutually respectful relationship the social worker can be a resource for the client to achieve behavior change goals [18]. When a social worker jumps into problem solving before the client has discovered their motivation for themselves the client feels the need, often unknowingly, to defend their current course of action and resist any suggestion for change [30].
TEAM-CBT presents social workers with a model to dissipate resistance to change by guiding the social worker to create an empathetic, client-centered atmosphere where the client can feel heard and validated [7]. This approach is clearly consistent with social work values and practice competency expectations [1, 2]. As social workers learn the skills of assessing resistance and develop the ability to identify the benefits and address secondary gain for problem protection, they will create a space where the client is able to independently discover their motivation and commitment to change.
Conclusion
This critical analysis provides the field of social work with guidance and insights into what may foster resistance to behavior change and how to partner with the client to facilitate motivation to change. When effectively implemented, TEAM-CBT is aligned with the social work value of client self-determination [2]. The TEAM-CBT model is based on research evidence relevant to client assessment, empathy and engagement, client motivation to change and application of intervention strategies [7]. These elements are the hallmarks of competent micro practice in social work [1]. As social workers begin to test the effectiveness of their services by using client satisfaction surveys before and after each session or group, they will better understand the effectiveness of the therapeutic relationship. When a social worker practices humility they can use the insights gained through evidence-based assessment tools to identify areas where they need to improve their own knowledge and skill.
Conflicts of Interest (COI) Statement
The author has declared no conflict of interest.
References
Council on Social Work Education (CSWE). (2015). 2015 Educational Policy and Accreditation Standards for Baccalaureate and Master’s Social Work Programs.View
National Association of Social Workers (NASW). (2017). Code of Ethics of the National Association of Social Workers.
Prochaska, J. O., & DiClemente, C. C. (1982). Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research & Practice, 19(3), 276–288.View
McConnaughy, E. A., Prochaska, J. O., & Velicer, W. F. (1983). Stages of change in psychotherapy: Measurement and sample profiles. Psychotherapy: Theory, Research & Practice, 20(3), 368–375.View
Gitterman, A. (1983). Uses of Resistance: A Transactional View. Social Work 28, 127-131.View
Burns, D. D. (1999). Feeling Good: The new mood therapy. New York, NY: Penguin Books.
Burns, D. D., & Burns, S. (2005). Tools, Not Schools, of Therapy. Los Altos Hills, Ca: Author.
Burns, D.D. (Producer). (2019, July 15). Is Cognitive Therapy a Cure-All for Everything? [Audio podcast].
Burns, D. D. (n.d.) From CBT to T.E.A.M.
Persons, J. B. (2007). Psychotherapists Collect Data During Routine Clinical Work That Can Contribute to Knowledge About Mechanisms of Change in Psychotherapy. Clinical Psychology: Science & Practice, 14(3), 244–246.
Lambert, M. J., Whipple, J. L., Hawkins, E. J., Vermeersch, D. A., Nielsen, S. L., & Smart, D.W. (2003). Is it time for clinicians to routinely track patient outcome?: A meta-analysis. Clinical Psychology: Science and Practice, 10, 288–301.View
Youn, S.J., Kraus, D. R., & Castonguay, L.G. (2012). The Treatment Outcome Package: Facilitating practice and clinically relevant research. Psychotherapy, 49, 115-122. doi:10.1037/ a0027932.View
Burns, D.D. (n.d.) Therapist’s Toolkit. Retrieved from https:// feelinggood.com/resources-fortherapists/therapists-toolkit/
Beck, A. T., & Steer, R. A. (1991). Relationship between the Beck Anxiety Inventory and the Hamilton Anxiety Rating Scale with anxious outpatients. Journal of Anxiety Disorders, 5, 213– 223.View
Esser, P., Hartung, T. J., Friedrich, M., Johansen, C., Wittchen, H.-U., Faller, H., … Mehnert, A. (2018). The Generalized Anxiety Disorder Screener (GAD-7) and the anxiety module of the Hospital and Depression Scale (HADS-A) as screening tools for generalized anxiety disorder among cancer patients. Psycho- Oncology, 27(6), 1509–1516.View
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory: Second edition manual. San Antonio, TX: Psychological Corporation.View
Kelley, F., Gelso, C. J., Fuertes, J. N., Marmarosh, C., & Lanier, S. H. (2010). The real relationship inventory: Development and psychometric investigation of the client form. Psychotherapy Theory, Research, Practice, Training, 47(4), 540-553. doi:10.1037/a0022082View
Elliott, R., Bohart, A. C., Watson, J. C., & Greenberg, L. S. (2011). Empathy. Psychotherapy, 48(1), 43-49. doi:10.1037/ a0022187View
Moyers, T. B., & Miller, W. R. (2013). Is low therapist empathy toxic? Psychology of Addictive Behaviors, 27(3), 878-884. doi:10.1037/a0030274 View
Bachelor, A. (2013). Clients’ and therapists’ views of the therapeutic alliance: Similarities, differences and relationship to therapy outcome. Clinical Psychology and Psychotherapy, 20, 118-135. doi:10.1002/cpp.792
Burns, D.D. (Producer). (2016, October 28). E=Empathy – Does It Really Make a Difference? [Audio podcast].
Hill, C., Nutt-Williams, E., Heaton, K., Thompson, B., & Rhodes, R. (1996). Therapist retrospective recall of impasses in long-term psychotherapy: A qualitative analysis. Journal of Counseling Psychology, 43, 207 –217.
Kivlighan, D.M., & Shaughnessy, P. (1995). Analysis of the development of the working alliance using hierarchical linear modeling. Journal of Counseling Psychology, 42, 338–349.View
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191-215.
Burns, D.D. (2008). Feeling Good Together: The Secret to Making Troubled Relationships Work. New York: Broadway Books.
Rogers, C. R. (1957). The Necessary and Sufficient Conditions of Therapeutic Personality Change. Journal of Consulting Psychology 21(2), pp. 95- 103.View
<./li>Burns, D., Westra, H., Trockel, M., & Fisher, A. (n.d.). Motivation and Changes in Depression. Cognitive Therapy and Research, 37(2), 368–379.
Aviram, A., Westra, H. A., Constantino, M. J., & Antony, M. M. (2016). Responsive management of early resistance in cognitivebehavioral therapy for generalized anxiety disorder. Journal Of Consulting And Clinical Psychology, 84(9), 783–794.View
Hara, K.M., Westra, H.A., Aviram, A., Button, M.L., Constantino, M.J., & Antony, M.M. (2015). Therapist awareness of client resistance in cognitive-behavioral therapy for generalized anxiety disorder. Cognitive Behavior Therapy, 44, 162-174.
Miller, W. R. & Moyers, T. B. (2017). Motivational Interviewing and the Clinical Science of Carl Rogers. Journal of Consulting and Clinical Psychology 85(8). pp. 757-766.View
Miller, W. R., & Rollnick, S. (2004). Talking Oneself Into Change: Motivational Interviewing, Stages of Change, and Therapeutic Process. Journal of Cognitive Psychotherapy, 18(4), 299–308. https://doi-org.libpublic3.library.isu.edu/10.1891/ jcop.18.4.299.64003View
Beck, A.T., & Clark, D. A. (1988). Anxiety and depression: An information processing perspective. Anxiety Research, 1(1), 23- 36.View
Integrity. (n.d.) Merriam-Webster Online. Retrieved October 2019.View
Lowery, C.T. (2016). Foundations of Social Work Practice: A Graduate Text. NASW Press.
O’Hare T. (2016). Essential Skills of Social Work Practice: Assessment, Intervention, and Evaluation. New York, NY: Oxford University Press.
Weick, A., Rapp, C., Sullivan, W.P. and Kisthardt, W. (1989) ‘A strengths perspective for social work practice’, Social Work, Vol. 34, No. 4, pp. 350-354.View
Graybeal, C. (2001). Strengths-based social work assessment: Transforming the dominant paradigm. Families in Society, 82(3), 233-242. doi:10.1606/1044-3894.236View
Van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. New York, NY: Viking Penguin.
Shepard, B. (2015). Community Projects as Social Activism: From Direct Action to Direct Services. Los Angeles: Sage Publications Inc.View
Morgaine, K., & Capous-Desyllas. (2015). Theoretical Perspectives on Social Work. In Anti- Oppressive Social Work: Putting Theory Into Action (pp. 48-94). Thousand Oaks, CA: Sage Publications Inc.
David, D., Cotet, C., Matu, S., & Mogoase, C. (2017). 50 years of rational-emotive and cognitive-behavioral therapy: A systematic review and meta-analysis. Journal of Clinical Psychology, 74, 304-318. doi:10.1002/jclp.22514View
Jacobsen, Courtney A. (2013). Social Workers Reflect on Engagement with Involuntary Clients. Retrieved from Sophia, the St. Catherine University repository website: View
Gibbs, L., & Gambrill, E. (2002). Evidence-based practices: Counter arguments to objections. Research on Social Work Practice, 12, 452-476. View
Lomax, R. G., West, M. M., Harmon, M. C., Viator, K. A., & Madaus, G. F. (1995). The impact of mandated standardized testing on minority students. The Journal of Negro Education,, 64(2), 171-185. doi:10.2307/2967240 View
Kadushin, A., & Kadushin, G. (2013). The Social Work Interview: A Guide for Human Service Professionals (5th ed.). New York, NY: Columbia University Press View
Eriksson, K., & Englander, M. (2017). Empathy in Social Work. Journal of Social Work Education, 53(4), 607–621. https://doi. org/10.1080/10437797.2017.1284629 View
Hatcher, R. L., & Barends, A. W. (1996). Patients’ view of the alliance in psychotherapy: Exploratory factor analysis of three alliance measures. Journal of Consulting and Clinical Psychology, 64(6), 1326-1336.View
Persons, J. B., & Burns, D. D. (1985). Mechanisms of action of cognitive therapy: The relative contributions of technical and interpersonal interventions. Cognitive Therapy and Research, 9(5), 539-551.View
Burns, D.D. (Producer). (2016b, December 12). The Five Secrets of Effective Communication (Part 1). [Audio podcast].View
Burns, D.D. (Producer). (2017, February 26). Ask David – How do you handle a patient youdon’t like (or who bores you)? [Audio podcast].
Miller, W. R., Benefield, R. G., & Tonigan, J. S. (1993). Enhancing motivation for change in problem drinking: A controlled comparison of two therapist styles. Journal of Consulting and Clinical Psychology, 61(3), 455–461.View
Burns, D. D., & Spangler, D. L. (2000). Does psychotherapy homework lead to improvements in depression in cognitive– behavioral therapy or does improvement lead to increased homework compliance? Journal of Consulting and Clinical Psychology, 68(1), 46–56.View
MLinehan, M.M. (1993). Skills Training Manual for Treating Borderline Personality Disorder. The Guilford Press.View
Baer, R., Smith, G., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45.
Johnson, S. M. (2019). Attachment Theory in Practice: Emotionally Focused Therapy (EFT) with Individuals, Couples, and Families (1st ed.). The Guilford Press.
Luoma, J. B., Hayes, S. C., & Walser, R.D. (2017). Learning ACT: An Acceptance & Commitment Therapy Skills Training Manual for Therapist. Oakland, CA: New Harbinger Publications, Inc.
Carr, A. (1998). Michael White’s Narrative Therapy. Contemporary Family Therapy: An International Journal, 20(4), 485–503.View
Kottman, T. & Meany-Walen, K. K. (2018). Doing Play Therapy: From Building the Relationship to Facilitating Change. New York, NY: The Guilford Press.
Drake, B., Hovmand, P., Jonson-Reid, M., & Zayas, L. H. (2007). Adopting and teaching evidence-based practice in master’slevel social work programs. Journal of Social Work Education, 43(3), 431-446. doi:10.5175/JSWE.2007.200600625.View
Ellis, A. (1995). Changing rational emotive behavior therapy to REBT. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 13(2), 85-89.View