
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 2 (2020), Article ID: JMHSB-118
https://doi.org/10.33790/jmhsb1100118Mini Review
How We Rise: Overcoming Trauma with Healthy Life Outcomes and Spiritual Counsel Approach
Sherri Harper Woods1*, DMin, LISW-S, EMDR Trained Therapist, Karen H. Larwin2, PhD, Katie M Allen3, MSW, LSW, Trauma-Informed Therapist
1*Assistant Professor, Master of Social Work Program Coordinator, Youngstown State University, One University Plaza, Youngstown, Ohio, United States.
2Associate Professor, Counseling, School Psychology, and Educational Leadership, Youngstown State University, One University Plaza, Youngstown, Ohio, United States.
3Graduate Assistant, Social Work Department, Youngstown State University, One University Plaza, Youngstown, Ohio, United States.
Corresponding Author Details: Assistant Professor, Master of Social Work Program Coordinator, Youngstown State University, One University Plaza, Youngstown, Ohio, United States. E-mail: sdwoods02@ysu.edu
Received date: 15th April, 2020
Accepted date: 19th May, 2020
Published date: 22nd May, 2020
Citation: Woods, S.H., Allen, K.M., & Larwin, K.H. (2020). How We Rise: Overcoming Trauma with Healthy Life Outcomes and Spiritual Counsel. J Ment Health Soc Behav 2(2):118
Copyright: ©2020, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Biopsychosocial-Spiritual (BPSS) interactive process involved in health and wellness includes the biological, psychological, social, and spiritual dimensions of well-being. Research has established the impact of adverse childhood experiences on the biological, psychological, and social dimensions of well-being. This study examines the impact spiritual counsel has in overcoming adverse childhood experiences and trauma with healthy life outcomes. In addition, it examines the impact of the therapeutic relationship on building hope and resilience can assist clinicians in providing environments for healing.
Keywords:
Adverse Childhood Experiences (ACES), Biopsychosocial-Spiritual Health, Resilience, Spirituality.
What are Adverse Childhood Experiences (ACEs)?
What are ACEs? The term Adverse Childhood Experiences (ACEs) is a term used to describe all types of abuse, neglect, and other potentially traumatic experiences that occur to people under the age of 18 [1]. The study conducted by the Center for Disease Control and Prevention and Kaiser Permanente on adverse childhood experiences emphasized the effect of trauma on the developing brain and health across the life span [2]. The Adverse Childhood Experiences (ACE) Study is one of the largest investigations aimed to assess the association between childhood maltreatment and laterlife health and well-being [3]. This was study originally conducted from 1995 to 1997 revealed the significant negative physiological and psychological outcomes of adverse childhood experiences that impact a child’s physical, mental, and emotional health and wellbeing into adulthood and prompted further studies.
In the original ACE study, researchers measured 10 ACEs. Counting each ACE as one, individuals were reported as having an ACE score of 0 to 10. Measures included:
• Physical, emotional, and sexual abuse.
• Physical and emotional neglect.
• Households with mental illness, domestic violence, parental divorce and separation, substance abuse, or incarceration [4].
What does the ACEs tell us?
One’s ACE score reflects the number of different types of adverse childhood experiences endorsed by the individual, with a higher score signifying the accumulation of diverse trauma [5]. As ACE scores increase, so does the risk for a variety of problems in adulthood, including chemical dependency, suicidality, depression, cigarette smoking, heart and pulmonary illnesses, obesity, liver disease, intimate partner violence, early initiation of sexual activity, promiscuity, sexually transmitted diseases, and unintended pregnancies [6]. Results of an ACE module in the 2010 Behavioral Risk Factor Surveillance Susrvey, a national cross-sectional, randomdigit- dial telephone survey of adults indicated that the highest ACE scores (four to six and seven to nine) were reported by a higher percentage of women compared to men and that exposure to one to three, four to six and seven to nine ACEs were associated with greater odds of reporting fair/poor general health, frequent mental distress, disability, myocardial infarction, and asthma relative to no ACE exposure. In addition, exposure to four to six and seven to nine ACEs were associated with a higher likelihood of coronary heart disease and stroke; exposure to one to three and four to six ACEs was associated with greater odds of diabetes compared to those with no ACE exposure [7].
A thorough assessment of childhood adversity can be a complicated task and includes tracing a person’s current behavior, investigating the actions, conduct, and responses to the context of their life. Understanding that a person’s behavior is related to the context of their interactions with systems of other people, including economic, political, legal, social, spiritual, and cultural enviroments [8] can impact the engagement, assessment, intervention, and evaluation of a client. To properly diagnose and treat client’s, practitioner’s need to be aware that there is an association between an individual whose experience included abuse, neglect, and household dysfunction on adult health and behavioral outcomes.
A growing body of research also suggests that ACEs such as sexual and physical abuse, neglect, witnessing of domestic violence, early parent loss, parental divorce, and out-of- home placement are often associated with subsequent psychological distress and mood disorders and other harmful effects on health throughout life [9-10]. Childhood adversity exposure is also a risk factor to maladaptive behaviors such as alcoholism, drug abuse, and suicidality [6,11,12].
The unresolved trauma of adverse childhood experiences can also place women at risk for developing depressive disorders, stressrelated disorders, unpleasant emotions, intense physical sensations, and impulsive and aggressive actions [[11,13]. To ignore the impact of ACEs on mental health is to provide ineffective treatment. The higher the ACEs number, the more at risk a person is for healthrelated risk factors and chronic health conditions. Use of the ACEs Questionnaire can provide an understanding of the impact of adverse childhood experiences on a person’s health and serve as a guide to treatment for social work clinicians.
How does adverse childhood trauma affect health?
Adverse childhood experiences are traumatic and affect our bodies, minds (thoughts and memories), emotions, and spirits because they are integrated systems [14]. A growing body of research suggest that ACEs such as sexual and physical abuse, neglect, witnessing of domestic violence, early parent loss, parental divorce, and out-ofhome placement are often associated with subsequent psychological distress and mood disorders and other harmful effects on health throughout life [9,10]. According to Van Der Kolk (2014), the emotions and physical sensations that were imprinted during the trauma are experienced not as memories but as disruptive physical reactions in the present [13]. The biological domains involved includes the central processes, somatic central processes, peripheral processes, and genetic predispositions. Likewise, the psychological domain includes the cognitive and affective predispositions. The social domain includes the activities of daily living, environmental stressors, interpersonal relationships, family environment, social support/isolation, social expectations, cultural factors, and previous treatment. The spiritual domain includes meditation, prayer, health behaviors, social support, meaning and purpose [15]. Women with histories of trauma tend to experience an array of mental health problems including anxiety, panic disorders, major depression, personality disorders, dissociative disorders, psychotic disorders, somatization, eating disorders, and post-traumatic stress disorder (PTSD) [16].
Psychological/Emotional Health
Multiple studies of adverse childhood experiences demonstrate that trauma is not a one-time event of the past. Unresolved trauma carries remnants within our mind, body, and brain in the present and can continue to carry the effects into the future resulting in psychological and emotional unhealth. Research indicates that childhood adversity is associated with poor psychological and emotional health [17].
There is a growing awareness and evidence that childhood adversity exposure (including neglect and emotional abuse) is a relevant risk factor for developing depressive disorders in adulthood and that early traumatized individuals may be more sensitized to the adverse effects of subsequent stressors, thereby increasing the likelihood of developing stress-related disorders, depression, alcoholism, drug abuse, and suicide attempts [6],[11],[12].
A study conducted by Felitti et al. showed that general population subjects who had experienced four or more categories of ACEs had an increased health risk of depression in the past year, and of alcoholism, drug abuse, and suicide attempts throughout the whole life span compared with those who had experienced none [6]. According to Van Der Kolk, unresolved trauma precipitates unpleasant emotions intense physical sensations, and impulsive and aggressive actions [13].
Findings also show a strong, graded relationship between cumulative ACE exposure and subsequent suicidali[12]. Studies conducted by Strine et al. found that ACEs and psychological distress were associated with an increased risk of self-reported alcohol problems in both men and women. Among women, results confirmed previous suggestions that a variety of ACEs including abuse (emotional, physical, sexual), neglect (emotional, physical) and household dysfunction (parental separation or divorce, drug use in household, and mental illness in household) were related to self-reported alcohol problems [9].
Those with an ACE score of six or above had a 15 percent or greater chance than those with an ACE score of zero of currently suffering from any of the ten leading causes of death in the United States, including chronic obstructive pulmonary disease (COPD), ischemic heart disease, and liver disease. They were twice as likely to suffer from cancer and four times as likely to have emphysema [13]. Women with histories of trauma tend to experience an array of mental health problems including anxiety, panic disorders, major depression, personality disorders, dissociative disorders, psychotic disorders, somatization, eating disorders, and post-traumatic stress disorder (PTSD) which subsequently result in physiological maladies [16].
Biological / Physiological
Early publications from the Adverse Childhood Experiences Study have also demonstrated a strong association between exposure to adverse childhood experiences and reproductive health outcomes unintended pregnancy and sexually transmitted disease (STD) infection [18]. The adverse consequences of participating in highrisk sexual behaviors are disproportionately higher in women than in men [18]. Likewise, Van Der Kolk (2014) research suggests that high ACEs results in earlier prevalence of obesity amongst females [13]. The Biopsychosocial model (Ashford, LeCroy & Winston, 2018) is a medical model of health assessment developed in the 1970s by George L. Engel [20] as an approach to establish a holistic view of a human being [19,20]. The expanded model that included the spiritual as a more inclusive approach was established following the movement promoting spirituality into the behavioral sciences and end of life practices. Dana E. King is credited for the movement to address faith, spirituality and medicine [21]. This model is used as an assessment tool to conceptualize the whole person and the totality of the client’s relational existence.
Social
Having been exposed to family violence as a child often makes it difficult to establish stable, trusting relationships as an adult. Adults reporting higher ACE scores (>3) have a greater propensity to negative mental processing which are associate with greater psychological distress [22]. This greater psychological destress, if untreated, can result in comorbidities and accelerated aging [23]. While some research has suggested that the impacts of ACEs can be detrimental and deterministic of the long-term outlook of overall health and wellness [13], more recent research suggests that changing the mindset and thinking patterns about relationships and attachment can support a healthier outlook [24].
Once ACES are identified, the next step for clinicians is to work with clients to build protective factors that will strengthen their psychological, emotional, and social health aspects of trauma recovery. A supportive community, therapy, sense-making, new knowledge, and faith have all worked together for healing [25]. Restoring sanctuary and utilizing spirituality as a strength-based approach to healing, are ways practitioners can lead clients on the path to hope, healing, and health in trauma recovery. Restoring sanctuary builds a trauma-informed healing environment. In order for practitioners to be identified as competent in trauma-focused practices, it is necessary for them to 1) demonstrate knowledge of the impact adverse childhood experiences has on physiological, psychological, and spiritual health 2) demonstrate clinical skills in administering the Adverse Childhood Experience Scale (ACES) 3) demonstrate an ability to identify the impact adverse childhood experiences has on psychological, physiological, and spiritual health 2), assess adverse childhood experiences, and 3) intervene with evidence-based trauma interventions. More documented work of this process is needed.
Current Investigation
The current investigation examines the role of spirituality and counseling in women’s lives who have experienced adverse childhood events, as measured by the ACEs inventory. In addition, this investigation incorporates a measure of social life/relationship satisfaction [26], and there measures intended evaluate the psychological/emotional health: the Subjective Happiness Scale [27], the Satisfaction With Life Scale [28], and the Brief Resiliency Scale [29].
Methods
Participants
Participants included individuals who were willing to complete the multiple inventories. The survey was sent out through a NE Ohio medical system and university. Participants were able to complete their responses electronically to the Survey Monkey database. The resulting results include n= 1736 female responses, representing an estimated 22.9% response rate of the expected n = 7554 sampling frame. The results
Instrumentation
Participants were asked to complete a survey that included the following inventories:
Satisfaction with Life Scale (SWLS)
Satisfaction with Life Scale (SWLS) is the level of satisfaction individuals have with their socio-cultural conditions. The items include: (1) In most ways, my life is close to my ideal;(2) The conditions of my life are excellent; (3) I am satisfied with my life;(4) So far, I have gotten all the important things in life; and (5) If I could live my life over, I would change almost nothing . This scale is intended to be a unidimensional measure of satisfaction with life. The SWLS is a very stable measure and has been found to perform better than single variable measures of satisfaction with life [30-32]. Despite criticisms, SWLS is the most frequently used measure of satisfaction with life in the existing literature [33]
Subjective Happiness Scale (SHS)
The Subjective Happiness Scale (SHS) by Lyubomirsky and Lepper (1999) is an instrument that measures the overall subjective happiness of an individual as "a global, subjective assessment of whether one is a happy or an unhappy person” (p. 139) [27]. According to the developers, the inventory was developed to fill a void in the existing measures in providing a global measure of psychological happiness. It consists of four items rated on a 7-point Likert scale. The items include: (1): In general, I consider myself… Not a very happy person (1) to A very happy person (7); (2): Compared with most of my peers, I consider myself… Less happy (1) to More happy (7); (3): Some people are generally very happy. They enjoy life regardless of what is going on, getting the most out of everything. To what extent does this characterization describe you? Not at all (1) to A great deal (7); and (4): Some people are generally not very happy. Although they are not depressed, they never seem to be happy as they might be. To what extent does this characterization describe you? Responses: Not at all (1) to A great deal (7). Despite its brevity, SHS has good psychometric qualities; it is characterized by "high internal consistency, a unitary structure, and stability over time" [34]. Based on Lyubomirsky (2008), the reliability estimates for the scale ranged from α=.79 to α= .94. This scale provides an overall subjective barometer of one's happiness [34].
Brief Resilience Scale (BRS)
Resilience could be the key to explaining resistance to risk across the lifespan and how people bounce back [35]. Resiliency is a disposition that ameliorates the adverse effects of stress and promotes positive outcomes. Because of these characteristics, resilience is part of research on job satisfaction [36,37], life satisfaction[38], and well-being [39,40]. This scale consisting of six items on a 5-point Likert-type scale ranging from strongly disagree (1) to strongly agree (5) [41]. Items include: (1) I tend to bounce back quickly after hard times; (2) I have a hard time making it through stressful events; (3) It does not take me long to recover from a stressful event; (4) It is hard for me to snap back when something bad happens; (5) I usually come through difficult times with little trouble; and (6) I tend to take a long time to get over set-backs in my life.
The Relationship Assessment Scale
The current study incorporates the Relationship Assessment Scale (RAS) developed by Susan Hendrick and associates [26]. The RAS was created initially as a brief measure of marriage quality, but later it was expanded for use with other intimate relationship situations such as parent-child, and close friends. This scale consisting of seven items on a 5-point Likert-type has exhibited high internal reliability [41]. The items include: (1) In general, how satisfied are you with your relationship?; (2)How good is your relationship compared to most?; (3) How often do you wish you hadn't gotten into this relationship?; (4) To what extent has your relationship met your original expectations?; (5) How much do you love your partner?; and (6)How many problems are there in your relationship? Even when applied to multiple types of relationships the RAS provides a stable measure “when completed with regards to romantic partners, parents, friends, and other types of relatives" [42].
Adverse Childhood Experiences (ACEs) Scale
The ACEs inventory was developed by Centers for Disease Control and Prevention (CDC) and Kaiser Permanente [1]. The ACEs inventory was administered to a sample of participants. The ACEs inventory asks participants to respond “yes” or “no” to the following ten items:
1. Did a parent or other adult in the household often swear at you, insult you, put you down, or humiliate you? Or act in a way that made you afraid that you might be physically hurt?
2. Did a parent or other adult in the household often push, grab, slap, or throw something at you? Or ever hit you so hard that you had marks or were injured?
3. Did an adult or person at least 5 years older than you ever touch or fondle you or have you touch their body in a sexual way? Or try to or actually have oral, anal, or vaginal sex with you?
4. Did you often feel that no one in your family loved you or thought you were important or special? Or your family didn’t look out for each other, feel close to each other, or support each other?
5. Did you often feel that you didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? Or your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
6. Were your parents ever separated or divorced?
7. Was your mother or stepmother: Often pushed, grabbed, slapped, or had something thrown at her? Or sometimes or often kicked, bitten, hit with a fist, or hit with something hard? Or ever repeatedly hit over at least a few minutes or threatened with a gun.
8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
9. Was a household member depressed or mentally ill or did a household member attempt suicide?
10. Did a household member go to prison?
In addition to the above inventories, participants were asked to indicate the following:
• Please briefly identify what has helped you in overcoming adversity.
• Please briefly identify someone who has helped you be successful.
• How would you describe your present health?
• What has made your life better/worth living?
Procedure
After the IRB approval was received for the research project, the link was sent to the local hospital system, to through the local university. The survey did not ask for any identifying information but did ask participants to indicate their gender, age range, martial status, ethnicity, topology, financial status and household makeup. The rate of response for males was less than 10%, therefore for this investigation, only female responses are included. Additionally, only those females that completed all the inventories listed above were included in this investigation.
Results
Descriptive Statistics
The basic descriptive statistics are provided regarding the study participants. Results indicate that n = 1347 (77.6%) of the participants report working in health care, and n = 1586 (91.4%) report that their race is Caucasian. The breakdown of the participants age ranges is provided in Table 1.

Table 1. Reported Age Range of Participants
As indicated above, the largest group of respondents indicate that they are 29-39 years of age (33.4%) followed by over 50 years of age (27.5). The relationship status of these individuals is provided in Table 2.

Table 2. Relationship Status
As seen in Table 2, most participants reported that they are married (n = 1174, 67.6%) followed by divorced (n = 281, 16.2%) Likewise, participants provided their educational level (Table 3).

Table 3. Reported Educational Level
As indicated above, 70.5% of the participants have some undergraduate level college education. Approximately 18% of the participants have an advance degree. Participants were asked to provide their income level (Table 4.)

Table 4. Reported Income Bracket
Participants overwhelmingly report that they earn a middleclass income. Likewise, most participants live in suburban (n = 7741, 44.4%), rural (n = 653, 37.6%), and urban (n = 305, 17.6%) communities. Lastly, participants were asked to indicate the makeup of their household. Results are provided in Table 5.

Table 5.Reported Household Makeup
Preliminary analyses examined the if there was an association between the participant’s ACE score (based on a low: 0 to 3, medium: 4 to 6, high: 7 to 10 level) and the participant’s reported age, income bracket, topology (urban, rural, suburban), and household make-up. These results are presented in Table 6.

Table 6.Association between Categorical ACE and Age, Income, Topology, and Household
As indicated above none of these variables are associated with the categorical levels of the ACEs score. Additionally, a Pearson’s Zero-Order Correlation was conducted to assess the relationship of the ACE score with RAS, SHE, SWL, BRS and the reported health outcome. Results are presented in Table 7.

Table 7.Pearson’s Correlation between ACE score and Inventory Scores
Results indicate that the ACE score is significantly correlated with all factors (RAS, SHS, SWL, BRS, and Health. Results indicate that the relationship between reported health (sickly, poor, fair, good, great) and ACEs scores is a small moderate positive relationship, r = .137, p<.010
Responses to these questions:
• Please briefly identify what has helped you in overcoming adversity.
• Please briefly identify someone who has helped you be successful.
• What has made your life better/worth living?
Revealed that 53 participants indicated that therapy helped them to overcome their adversity. Family was identified by 27.2, and jobs by 21.9% as those helping them to be successful. Interestingly, 63% of participants credited faith or spirituality as helping them overcome adversity.

Table 8.The results of the Between-Subjects Effects model are presented in
Specifically, those who indicated that they depended on faith or spirituality had higher scores across all of the measures (RAS, SWL, SHS, and BRS). These differences are illustrated graphically in Figure 1 for those who indicated Faith/Spirituality relative to those who did not.
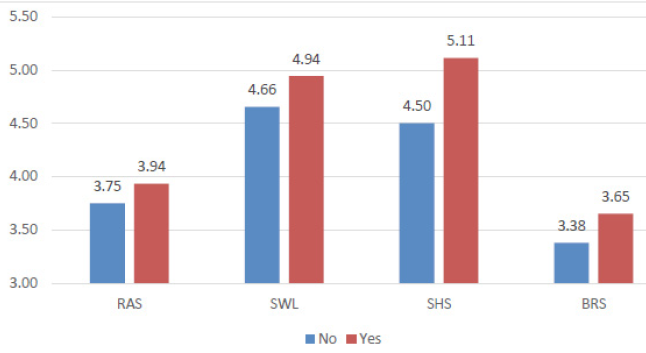
Figure 1.Yes indicating Faith/Spirituality on Dealing with Adversity and Overcoming Across RAS, SWL, SHS, and BRS
Also, those who reported Fair or Good health had higher scores on the RAS, SWL, SHS, and BRS overall. The difference for reported health on the participants RAS, SWL, SHS, and BRS are provided in Figure 2.
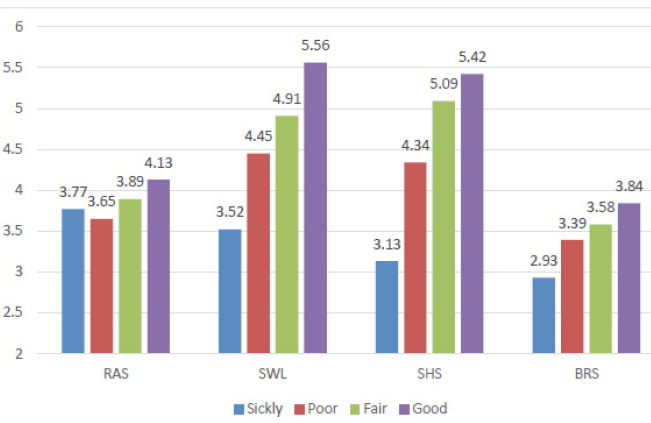
Figure 2.Reported Health on RAS, SWL, SHS, and BRS
Also, the lower the person’s ACE level, the greater their RAS, SWL, SHS, and BRS score. The participants reported ACE score (0 to 3, 4 to 6, 7 to 10) across RAS, SWL, SHS, and BRS is provided graphically in Figure 3.
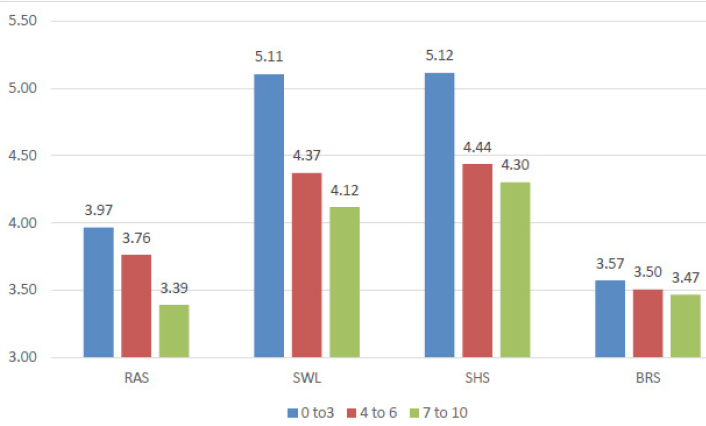
Figure 3.ACE Score Level across RAS, SWL, SHS, and BRS
Discussion and Conclusions
The results of the current investigation suggest a number of interesting outcomes. First, those who associate faith and/or spirituality as helping them to navigate difficult challenges in life are demonstrating significantly better life outcomes, as measured by the RAS, BRS, SWL, and SHS (as seen in Figure 1).
So, why does identifying with faith/spirituality in trauma associate with better life outcomes;
As individuals reframe their early hardships into divine purposes, they see opportunities for personal and spiritual growth, they ward off the detrimental effects of childhood adversity, they benefit from a strong feeling of connection with a perceived divine other, and they experience feelings of dignity and worth [17]. The data supports that spirituality and religion help to reframe life’s adversities and provide a hopeful lens to view distress and a way to intergrate their tragedy into their future story.
Likewise, the better reported health outcomes are associated with significantly better life outcomes (as seen in Figure 2). Research indicates that childhood adversity is associated with poor psychological and emotional health [17]. Figure 2 demonstrates that the less exposure to adversity predicts greater health. Greater health predicts better life outcomes.
Lastly, lower ACE scores were associated with significantly better reported life outcomes (as seen in Figure 3). All of these outcomes are consistent with what has been suggested in the extant research. The impacts of ACEs can be detrimental and deterministic of the long-term outlook of overall health and wellness [13]. Research also indicates that childhood adversity is associated with poor psychological and emotional health [17]. The data outcome illustrated in Figure 3 supports the theory that the less adversity (the lower ACES score) one experiences, the more probability of positive life outcomes.
As counselors, utilizing spirituality as a strength-based approach to trauma-recovery provides hope for a brighter future and increases protective factors against future stressors. We can implement the knowledge of the effects of spirituality on building resilience in trauma recovery to positively impact the trauma survivor’s perception of psychological and physical health. The complement of counseling and spiritual growth can free those burdened by childhood trauma so that they use those experiences to help others and ultimately experience better life outcomes themselves.
Conflict of interest:
The authors have declared no conflict of interest.
References
Centers for Disease Control and Prevention. Adverse childhood experiences reported by adults—five states, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(49):1609–1613.View
American Academy of Pediatrics, 2014.View
National Council for Behavioral Health (2019). Traumainformed Care.View
Data Resources Center for Children and Adolescents in Health, 2019.
Levenson, J. & Socia, K. (2016). Adverse childhood experiences and arrest patterns in a sample of sexual offenders. Journal of Interpersonal Violence 31, 1883-1911. https://doi. org/10.1177/0886260515570751.View
Felitti V.J., Anda, R.F., Nordenberg D., Williamson, D.E., Spitz A.M., Edwards, V., Koss M.P., Marks, J.S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE) study. American Journal of Preventative Medicine 14, 245-258. https://doi.org/10.1016/ s0749-3797(98)00017-8 View
Gilbert, L.K, Breiding, M.J., Merrick, M.T., Thompson, W.W., Ford, D.C., Dhingra, S.S, Parks, S.E. (2014). American Journal of Preventative Medicine. https://doi.org/10.1016/j. amepre.2014.09.006 View
Zastrow, C., Kirst-Ashman, K., & Hessenauer, L., (2019). Understanding the human behavior and the social environment. Cengage Learning.View
Strine, T., Dube, S., Edwards, V., Witt Prehn, A. (2012). Associations between adverse childhood experiences, psychological distress, and adult alcohol problems. American Journal of health Behavior 36(3), 408-423. https://doi. org/10.5993/ajhb.36.3.11 View
Hughes, K., Bellis, M., Hardcastle, K., Sethi, D., Butchart, A., Mikton, C., Jones, L., Dunne, M. (2017). The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health 2, 356-366. https://doi. org/10.1016/s2468-2667(17)30118-4.View
Mandelli L, Petrelli, C., Serretti, A., (2015). The role of specific early trauma in adult depressin: A meta-analysis of published literature. Childhood trauma and adult depression. European Psychiatry 30, 665-680. https:// doi.org/10.1016/j. eurpsy.2015.04.007.View
Cluver L., Orkin, M., Boyes, M., Sherr, L. (2015). Child and adolescent suicide attempts, suicidal behavior, and adverse childhood experiences in South Africa: a prospective study. Journal of Adolescent Health 1-8.
Van Der Kolk, B. (2014). The Body keeps the score: brain, mind, and body in the healing of the trauma. New York, NY: Penguin Books.
Van Hook, Mary P. (2016). Spirituality as a resource for coping with trauma. Social Work & Christianity 43(1), 7-25.
Hatala, A. R. (2013). Towards a biopsychosocial–spiritual approach in health psychology: exploring theoretical orientations and future directions. Journal of Spirituality in Mental Health, 15(4), 256-276. https:// doi.org/10.1080/19349 637.2013.776448 View
Huntington, N., Moses, D.J., Veysey, B.M. (2005). Developing and implementing a comprehensive approach to serving women with co-occurring disorders and histories of trauma. Journal of Community Psychology, 33(4), 395-410. https://doi. org/10.1002/jcop.20059 View
Jung, Jong H. (2018). Childhood adversity, religion, and change in adult mental health. Research on Aging, 40(2): 155-179. https://doi.org/10.1177/0164027516686662View
Hellis, S., Anda, R., Felitti, V., Marchbanks (2001). Adverse childhood experiences and sexual risk behaviors in women: a retrospective cohort study. Family Planning Perspectives 33, 206-211. https://doi.org/10.2307/2673783View
Ashford, J. B., LeCroy,L., & Williams, L. (2018). Human behavior in the social environment. Boston, MA: Cengage Learning.View
Engel, G. L. (1978). The biopsychosocial model and the education of health professionals. Annals of the New York Academy of Sciences, 310(1), 169-181. https://doi.org/10.1111/j.1749-6632. tb22070.x.
King, D. E. (2000). Faith, spirituality, and medicine: Toward the making of the healing practitioner. Psychology Press, https:// doi.org/10.4324/9780203047958.
Creasey, G. (2002). Psychological distress in college-aged women: Links with unresolved/preoccupied attachment status and the mediating role of negative mood regulation expectancies. Attachment and Human Development, 4(3), 261–277. http:// dx.doi.org/10.1080/14616730210167249 View
Miller, G. E., Chen, E., & Parker, K. J. (2011). Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychological Bulletin, 137, 959–997. https://doi. org/10.1037/a0024768 View
Dagan, O., Asok, A., Steele, H., Steele, M., & Bernard, K. (2017). Attachment security moderates the link between childhood experiences and cellular aging. Development and Psychopathology, 30, 1211-1223. https://doi.org/10.1017/ s0954579417001705 View
Scales, T. Laine, Scales, April T. (2016). After trauma: family relationships and the roads to healing. Social Work and Christianity, 43(1), 26-39. https://doi.org/10.1093/ acrefore/9780199975839.013.349
Hendrick, S. S., Dicke, A., & Hendrick, C. (1998). The relationship assessment scale. Journal of Social and Personal Relationships, 15, 137-142. https://doi.org/10.1177/0265407598151009 View
Lyubomirsky, S., & Lepper, H. S. (1999). A measure of subjective happiness: Preliminary reliability and. Social Indicators Research, 46, 137-155. Htttps://doi. org/10.1023/a:1006824100041 View
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The Satisfaction with Life Scale. Journal of Personality Assessment, 49, 71-75. https://doi.org/10.1207/s15327752jpa4901_13 View
Smith, L.A., Lenz, A.S., & Strohmer, D. (2016). Differential prediction of resilience among individuals with and without a history of abuse. Counseling and Values 62, 106-122. https:// doi.org/10.1002/cvj.12052 View
Andrews, F. M., & Withey, S. B. (1976). Social indicators of well-being : Americans' perceptions of life quality. New York: Plenum Press. https://doi.org/10.1007/978-1-4684-2253-5_8View
Eid, M., & Diener, E. (2006). Handbook of multimethod measurement in psychology. Washington, DC: American Psychological Association. https://doi.org/10.1037/11383-000View
Krueger, A. B., & Schkade, D. A. (2008). The reliability of subjective well-being measures. Journal of Public Economics, 92, 1833-1845. https://doi.org/10.1016/J.JPUBECO.2007.12.015 View
Margolis, S., Schwitzgebel, E., Ozer, D. J., & Lyubomirsky, S. (2018). A new measure of life satisfaction: The riverside life satisfaction scale. Journal of Personality Assessment, 1-10. https://doi.org/10.1080/00223891.2018.1464457.View
Lyubomirsky, S. (2008). The how of happiness : A new approach to getting the life you want. New York, N.Y.: Penguin Books.
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: assessing the ability to bounce back. International journal of behavioral medicine, 15(3), 194-200. https://doi.org/10.1080/10705500802222972View
Badran, M. A., & Youssef-Morgan, C. M. (2015). Psychological capital and job satisfaction in Egypt. Journal of Managerial Psychology. https://doi.org/10.1108/jmp-06-2013-0176View
Robbins, J. M., Ford, M. T., & Tetrick, L. E. (2011). Perceived unfairness and employee health. Journal of Applied Psychology, 97, 235-272. https://doi.org/10.1037/A0025408 View
Achour, M., & Nor, M. R. M. (2014). The effects of social and resilience on life satisfaction of secondary school students. Journal of Academic and Applied Studies, 4, 12-20.
Sagone, E., & Caroli, M. E. D. (2014). Relationships between psychological well-being and resilience in middle and late adolescent. Procedia - Social and Behavioral Sciences, 141, 881-887. https://doi.org/10.1016/J.SBSPRO.2014.05.154View
Souri, H., & Hasanirad, T. (2011). Relationship between resilience, optimism and psychological well-being in students of medicin. Procedia - Social and Behavioral Sciences, 30, 1541-1544. https://doi.org/10.1016/J.SBSPRO.2011.10.299View
Tansey, T. N., Kaya, C., Moser, E., Eagle, D., Dutta, A., & Chan, F. (2016). Psychometric validation of the brief resilience scale in a sample of vocational rehabilitation consumer. Rehabilitation Counseling Bulletin, 59, 108-111. https://doi. org/10.1177/0034355215573539 View
Renshaw, K. D., McKnight, P., Caska, C. M., & Blais, R. K. (2011). The utility of the relationship assessment scale in multiple types of relationship. Journal of Social and Personal Relationships, 28, 435-447. https://doi.org/10.1177/0265407510377850 View