
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 3 (2020), Article ID: JMHSB-134
https://doi.org/10.33790/jmhsb1100134Research Article
Part A of Anatomy at the Mall: A Multimodal Activity to Enhance Health Awareness and Identify Early Signs of Health-Related Issues in the General Public
Martin G. Rosario1*, Cassandra Woodson1, Michael G. George1,Victoria Junious1,Aleena Jose1 & Maryvi Gonzalez-Sola2
1 School of Physical Therapy, Texas Woman's University, Dallas TX, United States.
2 Department of Biology, Texas Woman’s University, Denton TX; United States.
Corresponding Author Details: Martin G. Rosario, PT, Ph.D., CSFI, ATRIC, Assistant Professor, School of Physical Therapy, Texas Woman's University, 5500 Southwestern, Medical Ave. Dallas,TX 75235-7299, United States. E-mail: mrosario1@twu.edu
Received date: 09th January, 2020
Accepted date: 04th March, 2021
Published date: 07th March, 2021
Citation: Rosario, M.G, Woodson, C., George, M.G, Junious, V., Jose, A., & Gonzalez-Sola, M. (2021). Part A of Anatomy at the Mall: A Multimodal Activity to Enhance Health Awareness and Identify Early Signs of Health-Related Issues in the General Public. J Ment Health Soc Behav 3(1):134.
Copyright: ©2019-21, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: There is a gap in the common knowledge of anatomy and its relationship to health in the community. Objective: We intend to obtain insight into community-dwelling adults' health status and promote health awareness using basic anatomy. Methods: Ninety-seven adults (average 32.6 years, 79.1 kg, 1.65 m) were participants at malls (MP) within the DFW area, and 36 healthy young adults performed as the control group (CP) (average 24.4 years, 67.7 kg, 1.65 m). MPs received a pretest/post-test to investigate their underlying knowledge and evaluate the knowledge of human anatomy and physiology before visiting six learning stations covering different anatomy systems. This research measured gait speed, isometric strength, balance, coordination, blood pressure, blood oxygenation, and heart rate to examine the health status and support the integration of the learned anatomy. Results: MPs displayed shifts from normative values with altered balance, lower leg strength, reduced gait speed, and high blood pressure. Conclusion and Clinical Relevance: The community-dwelling participants of this study revealed various health-related alterations link to poor quality of life. Regularly visit public areas such as malls, should incorporate free health screening educational booths or stations comparable to those in this research. Clinicians should recognize that the community-dwelling population requires knowledge of anatomyphysiology and health implications. Therefore, we encourage them to include educational items in the intervention strategies. Key Words: Community Health, Health Awareness, Anatomy, Outreach, Mall, Anatomy Tour
Introduction
Health in the United States proceeds to decrease, with heart disease being the contributing cause of death [1]. Diabetes, obesity, inadequate dieting, physical inactivity, and excessive alcohol use [1] are among the risk factors associated with heart disorders. In 2017, the prevalence of many cardiovascular illnesses in the United States was 7.9% [1]. Among Texans, there is a 7.7% prevalence of a significant cardiovascular disease among adults, along with 10.9% of the population having type 2 diabetes, 33% being obese, 36% considered overweight, and 83% not attaining the proposed amount of physical activity [1]. These determinants above are related to risk factors for heart disorders and other health conditions, a problem that afflicts the entire nation [1].
Several studies associate aspects of the human anatomy-body and function with risk factors of heart disease. For example, weakened hand grip musculature is linked to heart failure, sarcopenia, liver disease, walking performance/speed, functional disability, depression, Parkinson’s severity, longer hospital lengths of stay, and all-cause mortality [2-4] . The promising news is that various of these items mentioned above can be preventable.
Literature has established a connection among mobility/gait, lower body strength, hand-grip strength, balance, and single-limb stance time to avoid disability and premature death in both genders [5]. For the lower body, calf circumference has an inverse relationship with carotid plaques and stroke risk [6,7]. Step-length correlates with energy expenditure in people older than 65 with heart failure [8], and functional mobility is associated with health with gait speed related to all-cause mortality, pre-sarcopenia, osteoporosis, limited social involvement, and healthy aging [9-11]. In contrast, upper body muscular strength resulted in a reduced risk of all-cause mortality and death in both genders [6,7]. Additionally, hand-grip strength is connected with the bearing and duration of inflammation and loss of strength in rheumatoid arthritis and sarcopenia [12].
Many associations and healthcare providers' intentions are prevention and early diagnosis [13]. In short, rectify the situation before it develops into a problem. Various research established that using basic tools, tests, and measures could improve interventions to prevent disability and mortality in long-term care facilities. Information like muscular strength, balance, and functional mobility are predictors of all-cause mortality [1,5]. The question remains, how can healthcare providers reach out more effectively to the public, enhancing and promoting health?
One proposal to the above query is educational movements such as outreach-oriented activities. Health-related educational activities can diminish risk elements associated with heart disease and improve overall health [14], can promote healthy body weight [1], and lessen the occurrence of obesity, nutritional deficiency, and diabetes [15-17]. Further, health-related educational outreach activities can improve physical activity levels and have promising results when performed in real-world settings using a community-based participatory approach [18-20]. Specifically, health-educational outreach activities on the human body raise anatomical knowledge and understanding to all involved, thus underlining the value of health literacy, which can help diminish the risk factors identified with health conditions [21,[22].
Considering the above mentioned, the proposed study aims to enhance health awareness in the community through an anatomy outreach educational activity. We speculate that participants will exhibit alterations from the normative in various assessment protocols, increasing the risk of developing comorbidities and health issues.
Methods
In this study, we sent out emails to different malls in Texas and surrounding areas with information about the activity. We gathered qualitative and quantitative data from the Golden Triangle Mall in Denton, TX, and Music City Mall in Dallas, TX. Our sample was one of convenience, with participants being randomly selected as they entered the Mall or walked by the stations.In order to participate in this study, subjects had to meet the following criteria:
Inclusion criteria: be 18 years or older, any gender, with the ability to ambulate without an assistive device.
Exclusion criteria: were minors or those under 18 years old, women, and people that reported to be legally blind.
After meeting the criteria mentioned above, all participants signed informed consent before involvement in the activity. The Institutional Review Board approved the study at West Coast University Center for Graduate Studies in Los Angeles, CA.
Participants
Mall Participants (MPs). This study recruited 97 MPs, all subjects signed the informed consent however not all the MPs performer all tasks among the three different activities. The participants' age was 32.6 years, and the weight was 174.3 lbs, and height was 5'5" (Table 1). We recruited the subjects that visited the malls. A Graduate student stationed at the entrance of the activity location recruited participants. When partakers stopped to talk to the graduate scholar, a brief description of the activity was given. After participants agreed to partake in the outreach activity, they were brought to the entry table to read and sign the informed consent.
Control Participants (CP) [23]. To compare the public profile with CP, this study recruited healthy young adults from TWU Dallas. CPs' averaged profile was aged 24.4 years, weight of 149.2 lbs, and height of 5’5” (Table 1).
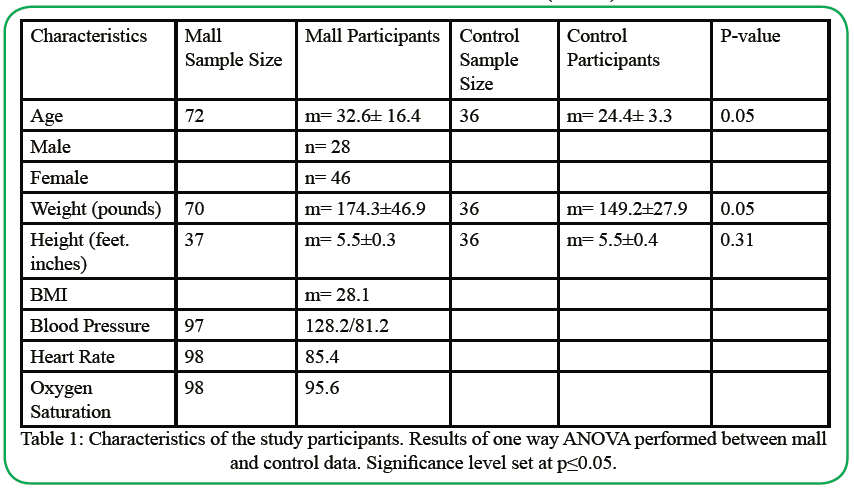
Table 1. Characteristics of the study participants. Results of one way ANOVA performed between mall and control data. Significance level set at p≤0.05.
Outreach activity
Each partaker was given the purpose and layout of the activity. Participants then went to each of the six primary stations (see Figure 1), comprising the nervous system, special senses, musculoskeletal system, organ area, cardiovascular system, and respiratory system.
Participants completed health-related tests at each station involving balance, coordination, strength, mobility, and vitals. Then, before continuing to the next station, a team member (trained nursing scholars and physical therapy students) gave health-related anatomybased information about each system.
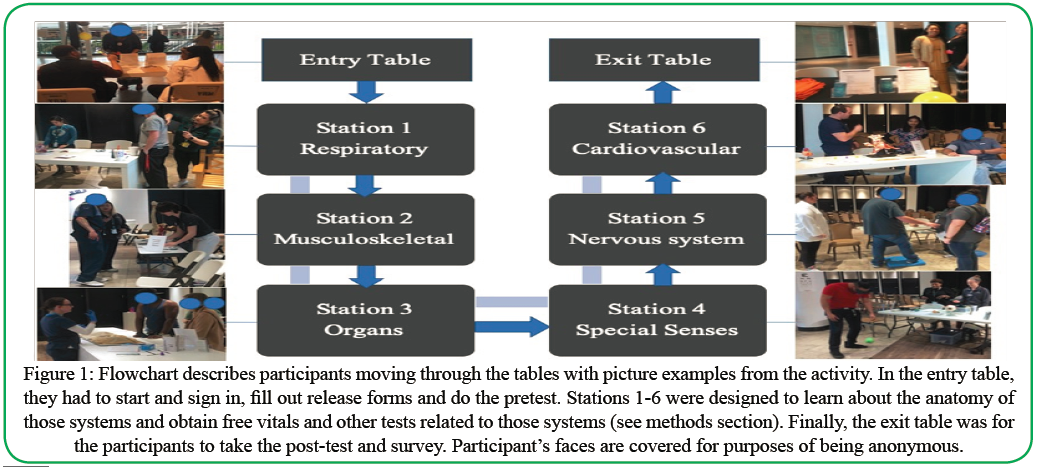
Figure 1: Flowchart describes participants moving through the tables with picture examples from the activity. In the entry table, they had to start and sign in, fill out release forms and do the pretest. Stations 1-6 were designed to learn about the anatomy of those systems and obtain free vitals and other tests related to those systems (see methods section). Finally, the exit table was for the participants to take the post-test and survey. Participant’s faces are covered for purposes of being anonymous.
Stations
Entry Table:
Each subject was instructed about the project and their role in participating. Subjects that signed the informed consent were given a pretest to determine their basic anatomy knowledge before engaging in the study. Figure 1 illustrates the organizational scheme of the activity.
1 Special Senses/Coordination Station:
A test was executed to evaluate the coordination of participants. (see Figure 1)
Coordination testing comprised several trials. One trial ball bouncing with no vision-altering goggles (baseline), two of drawing a smiley face on a piece of paper with and without goggles respectively, followed by a second trial of bouncing a ball while wearing the goggles. Every activity was conducted with two researchers given the instructions, gathering the results, and assisting each participant.
Part 1. We instructed the participant to bounce and catch a ball in their non-dominant hand five times. The researcher said, “bounce and catch the ball with one hand five times.” We started the timer once we said, “go” after asking the participant if they were ready. The researcher timed the participant using a stopwatch. Once the participant completed the round, they stepped to the table for the written portion.
Then, participants performed two drawings of a smiley face on their sheet. We explained to the participant to “draw a smiley face in the first box.” Once they finished the initial drawing, the participant put on the vision altering goggles. The goggles we designed altered the visual input. They drew the second smiley face with the goggles. The researcher informed the participant to “draw a smiley face in the second box.”
Part 2. Then, participants were again handed the ball to do the second round of the ball bouncing, hand-eye coordination. The second trial was run just like the first, with the addition of the goggles. If the participant dropped or missed the ball and traveled out of the participant's reach, the researcher handed it back to them to continue the round without stopping the time. The round concluded that once the participant caught the ball after the 5th bounce.
After completing this station, participants were educated about the importance of the visual, touch senses and the implication when both senses are lessened or impaired.
2 Nervous System/Balance Station:
During the balance and postural control component, we used the Single-Leg Stance (SLS). The test comprised the participant standing on one leg for 30 seconds while being timed. Trials were recorded in seconds. (see Figure 1)
Balance was assessed using SLS under four conditions; Ground (firm surface) without goggles (G-), foam (unstable surface) without goggles (F-), Ground with Goggles (G+), and Foam with Goggles (F+). We utilized a foam balance pad for G- and F- and modified goggles for G+ and F+. For safety, a spotter was used during the F+ condition. The participant was instructed to stand on one (either foot) foot for 30 seconds during each condition. Time was started when the participant lifted their foot and stopped when they touched the ground or reached 30 seconds.
After participants were finished, we explained the anatomy/ function of the different parts of the nervous system, the three major systems used for equilibrium (vestibular, proprioception, visual), and the implications of a reduced balance system to the risks of falls and injury.
3 Musculoskeletal Station:
At this station (see Figure 1), we asked participants to complete two tests measuring upper and lower extremities' strength and a walking component. Tests were done to measure grip strength, gastrocnemius and soleus strength, and gait parameters.
HHD. To assess the upper extremity force, we used a Camry EH101 electronic Hand-Held Dynamometry (HHD). We asked participants to sit in a standard armless chair with back support and their feet flat on the floor. Two successive measurements were collected on the dominant side and recorded. We then explained to the participant what the results mean, how they related to health, and average norms.
Activ5. To measure the lower extremity force, we utilized the Activ5 dynamometer [24] and tested the total isometric force in lbs or kg. We had participants sit on the chair in the position as previously mentioned with the HHD test. We asked each participant which foot was dominant before the examination and had them remove the shoe on that side. The participant’s knees were positioned at 90 degrees of flexion. The Activ5 device was placed with the top edge in line with the foot's metatarsals on the dominant side. We instructed the participant to hold the Activ5 device with their foot as hard as possible for 5 seconds while keeping their heel on the floor. A tablet with the Activ5 app was used to read the force produced on the Activ5 device. We performed the test 2 times and recorded the results. We explained to the patient their results and how lower body muscle strength related to health.
TUG. To measure gait parameters, we adopted the TUG test. The set-up and the instructions for the TUG test were retrieved from the Shirley Ryan Ability lab website [25]. A GoPro camera system was used to video record all the gait trials and record the time taken to finish each trial. We placed a visible tape on both legs' lateral and medial malleoli on each participant before testing. Two trials were performed with no assistive device.
Next, participants were instructed how to use a single point cane with their non-dominant hand while simultaneously performing a 2-point gait pattern. They conducted two trials of TUG with the cane in their non-dominant hand. The time, steps, cadence, and gait speed were recorded for each participant's four TUG trials.
After partaking in this station, participants were educated on the musculoskeletal system, the importance of strength, muscle weakness's implication to quality of life, and basic exercise recommendations.
4 Cardiovascular Station:
In the cardiovascular section (see Figure 1), participants had their blood pressure measured and described the heart's blood flow. Blood pressure was taken with the Omron HEM- 71DLX blood pressure cuff or an iHealth blood pressure cuff.
At the station's blood pressure section, participants were requested to take a seat to rest for a couple of minutes. Once the participant had rested, blood pressure was captured and recorded on the patient's form. Each participant was educated on their blood pressure reading compared to health standards (www.heart.org) [26] and reassured that this was not a diagnostic assessment for high blood pressure.
5 Respiratory Station:
In this location (see figure 1), we measured pulse oximetry to measure arterial oxygen saturation and performed auscultation of the lungs [27]. Pulse oximetry and lung auscultation were measured and assessed according to the guidelines of the American Lung Association 2020 [28] (Lung.org). Participants were formerly educated on the importance of a healthy respiratory system and normal oxygen saturation values' health implications.
6 Organ Station:
Here (see Figure 1), we provided the opportunity to view human organs from the Texas Woman's University Dallas Physical Therapy Department's cadavers. Participants observed and learned about the anatomy of healthy and pathological lungs, hearts, livers, gallbladders, kidneys, and spleens.
Because human organs were shown, this location was optional. Participants were allowed to partake of this station or proceed to the next part of the activity. However, if the participants took part in the organ station, they were taught about the organs' functions and diseases regarding health and wellness by physical therapy and nursing scholars. A trained graduate scholar, who completed human anatomy, performed the organs' demonstration and education in this station. If requested, participants were allowed to touch the organs after donning gloves. The students performed all handling, teaching, and demonstration.
Exit Table: (see Figure 1) Participants were given a survey to obtain insight into their perception of the activities and whether they found this outreach activity beneficial, as illustrated in Table 1.
Data Analysis:
A one-way ANOVA was conducted on participant characteristics and evaluation data of HHD, SLS, and Coordination. A paired t-test was conducted on mall participant gait results. A p-value of <0.05 was employed to establish significant differences in outcomes.
Results
Public profile:
Table 1 shows a significant difference between age and weight between the CP and MP, but height was similar. Age p-value was 0.05, weight p-value was 0.05, and height p-value was 0.31. The average BMI for the CP was 24.8 and for participants was 29.
Special Senses/Coordination:
As illustrated in Table 2, no notable difference was found (P=0.65). The average coordination result for the ball NO Goggles trial from 35 MPs was 4.3+/-1.5 seconds. The average coordination result for the ball NO Goggles trial from 36 CP was 4.7+/-1.1 seconds. The difference was not observed to be significant with a P-value of 0.25. The average coordination result for the ball WITH Goggles trial from 35 MPs was 7.6+/-5.4 seconds. The average coordination result for the ball WITH Goggles trial from 36 CP was 7.1+/-2.8 seconds.
Balance/ Nervous System:
Table 2 illustrates the average time for SLS with eyes open over ground was 25.9+/-7.8 seconds for 81 MPs and 29.6+/-13.0 seconds for 33 CP. There was no significant difference in time between the CP and MPs for SLS with eyes open over the ground (p=0.54). The average time for SLS with eyes closed over ground was 12.5+/-11.0 seconds for 81 MPand 24.5+/-10.0 seconds for 33 CP. There was a significant difference in time between the CP and MPs for SLS with eyes closed over ground (p=0.01). The average time for SLS with eyes open over foam was 14.5+/-10.6 seconds for 32 mall participants and 29.2+/-3.3 seconds for 36 CPs. There was a significant difference in time between the CPs and MPs for SLS with eyes open over foam (p=0.001). The average time for SLS with eyes closed over foam was 5.7+/-7.0 seconds for 32 MPs and 4.3+/- 1.3 seconds for 36 CPs. There was a significant difference in time between the CP and MPs for SLS with eyes closed over foam (p=0.05).
Muscle strength/ Musculoskeletal System:
HHD. Table 2 exemplifies the average HHD results of 71 MPswas 64.7 lbs +/- 28.5 lbs. The average HHD results of 33 CPs were 72.8 lbs +/- 27.5 lbs. The CP had higher results with a difference of 8.1 lbs between the groups and a p-value of 0.18.
Activ5. Table 2 depicts the average Activ5 results of 27 MPswas 27.0 +/- 13.2 lbs. The average Activ5 results of 33 CPs was 17.1 +/- 5.2. MPs had higher results with a difference of 9.9 lbs and a p-value of 0.001.
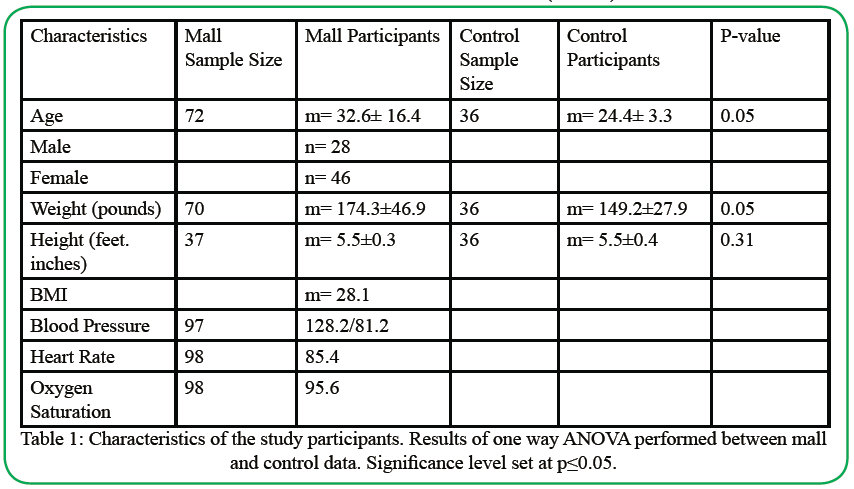
Table 2: Strength and balance test data. Results of one way ANOVA performed between mall and control data. Significance level set at p≤0.05.
TUG: Table 2 denotes the total of 15 mall participants who performed the TUG tests. The average time taken to complete the TUG with the cane was 13.1 seconds +/- 4.4 and without the cane 9.7 seconds +/- 2.2. The time taken to perform the TUG with the cane was 3.4 seconds higher, with a p-value of 0.001. The average number of steps taken with the cane was 13.6 steps +/- 2.3 and without the cane 12.1 steps +/- 9.7. The steps taken with the cane were 1.5 steps higher with a p-value of 0.001. The average cadence without the cane was 12 steps/min higher than with the cane, with a p-value of 0.001. The cane's average gait speed was 0.25 m/s +/- 0.8 and without the cane was 0.33 m/s +/- 0.12. TUG without the cane was 0.08 m/s higher with a p-value of 0.001.
Cardiorespiratory:
Table 1 illustrates the values for blood pressure, heart rate, and oxygen saturation of the MPs. According to the American heart association 2020 [29], all measurements are within normal limits except for blood pressure, which is slightly elevated with an average of 128.2/81.2 mmHg.
Discussion
Our research involved awareness outreach activities at various shopping malls (see Figure 1), forecasting to employ anatomy as a teaching tool to provide health understanding to the community while gathering the public’s health profile. This project was referred to Anatomy at the Mall because our study's primary intent was to educate the public about human anatomy and their health through anatomy while gaining a fundamental health profile on community people. In essence, this investigation segregated particular strategies into anatomy systems or components. Among the areas covered, we highlighted health and anatomy aspects of coordination (special senses), balance (nervous system), muscle strength (musculoskeletal), and blood pressure/heart rate cardiorespiratory.
Our initial assumption implied that partakers would exhibit deviations from the normative in the various assessment protocols, heightening the risk of developing comorbidities and health issues. Out of the four components discussed above, the MPs displayed alterations from the normative values in balance, lower leg strength, and blood pressure means; accordingly, we partly accept our previous hypothesis.
Special Sense, Coordination Station.
Our findings indicate similarities compared to coordination in MPs assessed at the Mall than in young, healthy adults. This research exemplifies that although other body systems might decline with maturing, hand-eye coordination remains unscathed in these participants. Previous studies reveal the deficiencies generated in coordination during different scenarios are related to neurological difficulties, musculoskeletal damage, and older age. One potential interpretation for this study's analogies could be related to how hand-eye coordination is a part of ordinary activities. Many routine tasks, such as key in the keyhole and fork in the mouth while eating, for instance, are part of the several ways people train, engage in, and maintain coordination accuracy [30,31]. Conversely, because of the simplicity of the ball bouncing task, we might have observed a ceiling-effect. A greater level of coordination task might have also been required to distinguish handeye coordination between the groups.
Another interpretation for the parallels in coordination is motor learning. We believe motor learning had a role during the hand-eye bouncing the ball coordination [32]. Since participants bounced the ball first with the visual system untouched, no goggles, motor learning was a component during the second part of the evaluation, when the examination required visual alteration with the goggles.
Although there was no statistical variation between the MPs and the CP, both groups increased their time from the NO GOGGLES task to the GOGGLES task. Participants were healthy; therefore, we were expecting similarities in the coordination component of the study. Previous researchers reported that profound impairment, such as visual field failure, is associated with longer reaction times and overall movement times [33]. Additionally, there are limited investigations on visual deterioration and its effect on coordination in community-dwelling people. Preliminary examinations have studied eye movement and behavior in coordination tasks [34,[34]. However, further research must be undertaken to determine how visual impairment affects eye movements in hand-eye coordination tasks in the community-dwelling population. Considering the outcomes above, prospective studies should focus on the reaction time of both upper extremities and lower extremists and visual impairment to further interpret and characterize the coordination aspects of distinct groups of participants.
Nervous system, balance station:
This study highlights that SLS balance is significantly impacted by the community group when visual and proprioceptive inputs are modified. Our results show a significant distinction in balance between the CP and the community group. Our findings suggest the factor provoking balance alteration is the relative inactivity of the public participants compared to the healthy individuals in the CP. Increased physical activity allows the body to train and improve the proprioceptive and vestibular systems, two critical components for balance [32].
Consequently, reduced physical activity culminates in diminished usage of both the proprioceptive and vestibular systems leading to increased reliance on the visual system to maintain balance [32]. SLS balance is also closely associated with dynamic stability during gait. Humans stand or bear weight on both feet during several movements, such as looking at a computer, standing in line, or cooking. Regardless, during gait, a single-leg stance is a fundamental component of the gait cycle. SLS time translates to dynamic balance, as longer SLS times will likely result in higher gait speeds [36].
Previous studies reveal the various pathologies and diagnoses that could alter the balance, such as diabetes and HIV [37,[38]. Nevertheless, our research substantiates that many seemingly healthy individuals in the community also demonstrate distorted balance. In our investigation, many MPs were astonished at the difficulty of maintaining SLS balance when vision and/or proprioception were modulated. Their decrease in balance had previously passed unnoticed due to compensation within the balance system's main components [39]. Once balance was challenged, the system could no longer compensate, requiring a stepping strategy to maintain standing balance.
It seems SLS has a steady decline in the community group. Losing the ability to balance in one limb will ultimately lead to increased fall risk, falls, and injuries. We suggest promoting and incorporating single limb activities in everyday tasks to slow down SLS time reduction. In the future, detailed testing procedures must be implemented to acquire more detailed data.
Muscle Strength / Musculoskeletal Station:
Our findings of this section revealed that, on average, the MPs scored less on handgrip values than the CP, but the distinction was not significant. However, on the plantar flexor, the CP scored less than the MPs with a considerable strength difference. Our results indicate that lower extremity strengths reduce or decline at a faster rate than the upper limb. A plausible explanation for our discoveries might be related to the rising trend of adolescents and adults who are not active. Therefore, this study could reveal an increasing tendency to reduce strength in the Dallas area and the associated increase in risk for health-related disorders (Data USA, 2018 & DSHS, 2014). We propose further examinations for Activ5 and HHD correlation and norms, providing activation of solely plantar flexors.
Most of the CPs were full-time students. As such, they spent most of the day sitting, making this previous statement a possible interpretation for the distinction in plantar flexor values and a limitation of this study. Early studies pointed to decreased physical activity reducing muscle strengths impacting balance and leg flexibility in older populations [40]. Notably, the present research discovered a potential trend involving pupils, lower limb weakness, and prolonged sitting. Further investigation should be conducted to recognize the impact of prolonged sitting with plantar flexor weakness. Additionally, we advise reviewing the ramifications of said weakness on gait and balance in full-time students.
Our examination indicated that the average cadence for the TUG was greater when performed without the cane. This cadence reduction while using the cane could be because participants were experiencing difficulty coordinating a 2-point gait pattern with the cane, leading to a slower cadence. The reason for integrating the cane during the TUG test was to determine the impact of this assistive device on gait in healthy subjects.
TUG.
Our examination indicated that the average cadence for the TUG was greater when performed without the cane. This cadence reduction while using the cane could be because participants were experiencing difficulty coordinating a 2-point gait pattern with the cane, leading to a slower cadence. The reason for integrating the cane during the TUG test was to determine the impact of this assistive device on gait in healthy subjects.
The ongoing research found out that gait speed for TUG with and without the cane was markedly lower than expected, notably since, from a clinical perspective, the community's normal gait speed is about 1.4 meters/second. The dilemma is that slower TUG times have been accompanied by more significant body mass index, comorbidities, and worsened perceived physical and mental health. [41]. Therefore, we interpret that introducing the cane to the standard gait patterns presents a more significant challenge to the community participating, provoking them to compensate with a slower cadence. Future inquiries should explore whether the demand for an assistance device could identify early manifestations of gait alterations, or the equipment typically will reduce cadence.
On the other hand, TUG's gait speed without a cane was higher than with the cane, implying that the cane decreased gait speed. The variation in gait speed using the cane could be due to an absence of familiarity with assistive devices and dual-tasking [42]. The discrepancy could also be due to the type of assistive device, whereas a particular assistive device such as a two-wheeled walker or using two canes could have increased gait speed [42].
One limitation to this station was that only 15 participants performed the TUG due to the station's location and the duration of time taken to accomplish the TUG trials. Many participants did not want to wait in line to perform this evaluation. These issues could have been achieved by adopting two camera systems to separately record two participants simultaneously and reduce the delay time.
Cardio and respiratory station:
BMI: Our findings show that the MPs were overweight according to the BMI calculator of the CDC 2020 compared to the CP. The CDC established that overweight and obese people are prone to suffer different issues and conditions such as hypertension, high cholesterol,and diabetes. Therefore, it was expected that our participants' average blood pressure was above normal levels, classifying them as hypertension stage 1, according to the American Heart Association 2020 [29].
Previous studies suggest that the obesity epidemic is in every population, including children. A study in 433 African American adolescents showed a prevalence of high blood pressure in this community. Furthermore, it showed how this group of students were unaware of their condition and did not see themselves as obese and exhibiting signs of hypertension [43]. However, some studies suggest that it decreases the sedentary lifestyle by examining exercise programs and improves sleep quality in obese adults [44]. Engaging in a moderate exercise of at least 30 minutes in the week was sufficient to start lowering high blood pressure [43].
Similar to both the CDC and the American Heart Association [29], we recommend to stop gaining weight and to lose a minimum of 10% of their weight. This small amount of weight loss can reduce health problems such as hypertension and high cholesterol. One of the constraints of this study was that some participants did not complete the entire program, and our database does not have the numbers of weight, HR, for instance, for all the 97 participants.
Sat O2 and HR:
The pulse oximeter enables us to understand how much oxygen our patients' red blood cells were obtained, hence the saturation (Sat02). Our findings revealed that both heart rate (85.4 bpm in average) and Sat02 (95.6% in average) were within the acceptable values. According to the American Lung Association, an acceptable result is from 90-92%. Thus, our participants were exceeding the expectations of a normal rate in terms of oxygenation. Usually, the SatO2 values are steady unless other underlying conditions affect the lungs' ability to exchange oxygen or hemoglobin for carrying oxygen, such as chronic obstructive pulmonary diseases [45]. There fore we were expecting these findings.
Regarding the heart rate, according to the American Heart Association, the normal values of the resting heart rate is from 60-100 bpm. Thus, the participants were within accepting average values of heart rate. However, the AHA recommends that a "lower bpm is better" for a resting heart rate, and it also correlates this to the physical activity of a person. So, the "higher the heart rate is, the lower the physical fitness," which could translate to develop "high blood pressure and more body weight."
We expected that numerous of our participants had a higher than normal blood pressure and weight due to many possible factors including sedentarism, and an unhealthy diet that is fostered and sponsored by different circumstances [46]. Because of the aforementioned average values, we showed our participants the results that they obtained. We explained the meaning of each value to raise the awareness of living a healthy lifestyle.
Weekly, a minimum of at least 150–300 minutes of moderateintensity activity is recommended to reduce the onset of chronic diseases such as high blood pressure in adults according to the WHO (www.WHO.INT) [47]. We speculate that inquiring information such as HR and BP in a public area (shopping mall) might encourage people to walk more. Further research should focus on promoting specific, doable physical activity goals for MP's when they attend public places. This physical activity objective could comprise simple modifications such as parking the car as far as possible from the entrance and starting on the opposite side of the establishment for extra steps.
Conclusion
Our study shows that the community-dwelling population around the DFW area lacks basic knowledge of anatomy and physiology. The study also demonstrated that individuals in the community exhibit significant differences in various assessment protocols than normative values. MPs displayed decreased lower leg strength, balance, and TUG time than the healthy CP, heightening their risk of developing comorbidities and health issues. The current study ushers in introducing human anatomical organs to MPs in a wellvisited area, the Mall. Additionally, we identified several aspects that point to early changes in normal human functions. These modifications described above were possibly going unnoticed before the participants partake in this activity.
Several shortfalls are worth pointing out; first, the lack of students to administer standardized testing procedures among participants across all events and data collection being taken from the same malls at different times of the year. These limitations led to incomplete data forms, which hindered our ability to analyze factors based on gender, age, weight, and other patient characteristics. The constraints also led to a lack of variance in mall locations across the DFW area, potentially resulting in skewed data. Various factors came into play for the previous limitations, including various malls declining to host our anatomy outreach activity, lack of coordination for checking information during the activity, short notice of events, and lack of standardized procedural training before the start of activities. These issues were corrected as the activity commenced. To further address these limitations, we recommend that a new station be included to ensure all data and tests are completed before the participant exiting the tour.
One final note, we hope the positive response, findings, and benefits of this activity encourages malls and other public facilities to be open to host these events in the future. Our study's results can be used to inform clinicians or health providers on the lack of knowledge concerning anatomy and physiology in the community-dwelling population and how information on anatomy systems can be applied to instruct their patients on the importance of health.
Acknowledgments
We would like to acknowledge the following people for helping in the Anatomy Tour at the Mall activities: Angela Agogo, Armida Belvill, Luning He, Dexter Hamilton, Sheila Wimberley, Anesa Hearst, Paul Davis, AditaGhney, LaMonica West, Sherri Smith-Keys, and Roshae Garner; your support and participation was instrumental for us. We would also like to give honorable mentions to the students Monica Mathis, Leslie Hadley, Tyler Reyes, Laura Tapia, and Rubi Aviles for your great responsibility and dedication to teach the participants. Finally, we would like to thank Chimdi Maduka, Anna Palacios, Komal Hemani, AneesahHyder and Damaris Hernandez for your participation and support.
Conflict of interests:
The authors declare no conflict of interest.
References
Centers for Disease Control and Prevention. (2019). Diseases & conditions: Heart disease. Retrieved 10/10/19 from: https:// www.cdc.gov/heartdisease/View
Bohannon, R. W. (2015). Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Current Opinion in Clinical Nutrition & Metabolic Care, 18(5), 465-470. DOI: 10.1097/MCO.0000000000000202View
Lee, L., Patel, T., Costa, A., Bryce, E., Hillier, L. M., Slonim, K., Molnar, F. (2017). Screening for frailty in primary care. Canadian Family Physician, 63(1), 51-57. DOI: 10.1111/ ggi.12508View
Rijk, J., Roos, P., Deckx, L., Akker, M., &Buntinx, F. (2016). Prognostic value of hand-grip strength in people aged 60 years and older: A systematic review and meta-analysis. Geriatrics Gerontology International, 16(1), 5-20. DOI: 10.1111/ggi.12508View
Agnieszka, W.S., Agnieszka, Ć.S., Natalia, W., Bernard, S., Anna, W.P. (2019). Association between Handgrip Strength, Mobility, Leg Strength, Flexibility, and Postural Balance in Older Adults under Long-Term Care Facilities. Biomed Res Int, 2019:1042834. DOI: 10.1155/2019/1042834View
Debette, S., Leone, N., Courbon, D., Gariepy, J., Tzourio, C., Dartigues, J., Ritchie, K., Alperovitch, A., Ducimetiere, P., Amouyel, P., &Zureik, M. (2008). Calf circumference is inversely associated with carotid plaques. Stroke, 39(11), 2958- 2965. DOI: 10.1161/STROKEAHA.108.520106View
García-Hermoso, A., Cavero-Redondo, I., Ramírez-Vélez, R., Ruiz, J. R., Ortega, F. B., Lee, D., & Martínez-Vizcaíno, V. (2018). Muscular strength as a predictor of all-cause mortality in an apparently healthy population: A systematic review and meta-analysis of data from approximately 2 million men and women. Archives of Physical Medicine and Rehabilitation, 99, 2100-13DOI: 10.1016/j.apmr.2018.01.008View
Yoshimura, K., Urabe, Y., Maeda, N., & Yoshida, T. (2019). Relationship between energy expenditure during walking and step length in patients with heart failure.Topics in Geriatric Rehabilitation, 35(2), 97-103. DOI: 10.1097/ TGR.0000000000000206View
Warren, M., Ganley, K. J., & Pohl, P. S. (2016). The association between social participation and lower extremity muscle strength, balance, and gait speed in US adults. Preventive Medicine Reports, 4, 142-147. DOI: 10.1016/j.pmedr.2016.06.005View
Bergland, A., Jørgensen, L., Emaus, N., & Strand, B. H. (2017). Mobility as a predictor of all-cause mortality in older men and women: 11.8 year follow-up in the tromsø study. BMC Health Services Research, 17(1), 22. doi:10.1186/s12913-016-1950-0View
Kim, W. B., Kim, B. R., Kim, S. R., Han, E. Y., Nam, K. W., Lee, S. Y., . . . Kim, J. H. (2019). Comorbidities in patients with end-stage knee OA: Prevalence and effect on physical function. Archives of Physical Medicine and Rehabilitation. DOI: 10.1016/j.apmr.2019.04.005View
Beenakker, K. G. M., Ling, C. H., Meskers, C. G. M., de Craen, Anton J. M., Stijnen, T., Westendorp, R. G. J., & Maier, A. B. (2010). Patterns of muscle strength loss with age in the general population and patients with a chronic inflammatory state. Ageing Research Reviews, 9(4), 431-436. doi:10.1016/j.arr.2010.05.005View
Scott, M.G., Ivor, J. B., Gregory, L. B., Alan, Chait., Robert, H. E., Barbara, V. H, William, M., Sidney, C. S., and James, R. S. (1999) . Diabetes and Cardiovascular Disease. https://doi. org/10.1161/01.CIR.100.10.1134View
Paeratakul, S., Lovejoy, J. C., Ryan, D. H., & Bray, G. A. (2002). The relation of gender, race, and socioeconomic status to obesity and obesity comorbidities in a sample of US adults. International Journal of Obesity, 26(9), 1205-1210. doi:10.1038/SJ.ijo.0802026View
Wallace, R., Lo, J., & Devine, A. (2016). Tailored nutrition education in the elderly can lead to sustained dietary behaviour change. The Journal of Nutrition, Health & Aging, 20(1), 8-15. doi:10.1007/s12603-016-0669-2View
Vieira, L. P., Nobre, M. R. C., & da Silveira, J.,Augusto Cardoso. (2016). Effects of nutrition education on recurrent coronary events after percutaneous coronary intervention: A randomized clinical trial. BMC Nutrition, 2(1), 72. doi:10.1186/ s40795-016-0111-5View
Tippens, K. M., Erlandsen, A., Hanes, D. A., Graybill, R., Jackson, C., Briley, J., &Zwickey, H. (2019). Impact of a short-term naturopathic whole-foods-based nutrition education intervention on dietary behavior and diabetes risk markers: A pilot study. The Journal of Alternative and Complementary Medicine, 25(2), 234-240. doi:10.1089/ACM.2018.0025View
Love, R., Adams, J., Sluijs, E., Foster, C., Humphreys, D. (2018). A cumulative meta-analysis of the effects of individual physical activity interventions targeting healthy adults. Obesity Reviews, 19(8), 1164-1172. DOI: 10.1111/or.12690View
Chase J. A. (2015). Interventions to Increase Physical Activity Among Older Adults: A Meta-Analysis. The Gerontologist, 55(4), 706–718. doi:10.1093/geront/gnu090View
Cohen, D. A., Han, B., Derose, K. P., Williamson, S., Marsh, T., & McKenzie, T. L. (2013). Physical activity in parks: A randomized controlled trial using community engagement. American journal of preventive medicine, 45(5), 590–597. doi:10.1016/j.amepre.2013.06.015View
Taylor, A., Diggle, P., & Wessels, Q. (2019). What do the public know about anatomy? Anatomy education to the public and the implications. Anatomical Sciences Education, 11(2), 117-123. DOI: 10.1002/ase.1746View
Mathis, M. ., Gonzalez-Sola, M., & Rosario, M. (2020). Anatomy Observational Outreach: A Multimodal Activity to Enhance Anatomical Education in Undergraduate Students. Journal of Student Research, 9(1). https://doi.org/10.47611/jsr. v9i1.869View
Centers for Disease Control and Prevention. (2020). Adult BMI Calculator. Retrieved 05/25/2020 from: https://www.cdc. gov/healthyweight/assessing/bmi/adult_bmi/english_bmi_ calculator/bmi_calculator.htmlView
Activbody. (2020). Activ5. Retrieved April 8, 2020 from: https://activ5.activbody.comView
Timed up and go. (2013). Shirley Ryan AbilityLab. Retrieved from: https://www.sralab.org/rehabilitation-measures/timed-and-goView
Heart. Understanding Blood Pressure Readings Retrieved January 5th, 2021. https://www.heart.org/en/health-topics/highblood- pressure/understanding-blood-pressure-readings
Valdez-Lowe, C., Ghareeb, S. A., & Artinian, N. T. (2009). Pulse oximetry in adults. AJN The American Journal of Nursing, 109(6), 52-59.View
American Lung Association. (2020) Pulse oximetry. Retrieved April 6, 2020 from: https://www.lung.org/lung-health-diseases/ lung-procedures-and-tests/pulse-oximetryView
American Heart Association (2020) Blood Pressure. Retrieved May 19, 2020 from: https://www.heart.org/en/health-topics/ high-blood-pressure/understanding-blood-pressure-readings
Soechting JF (2009) Eye-Hand Coordination – Timing and Reference Frames. In: Binder M.D., Hirokawa N., Windhorst U. (eds) Encyclopedia of Neuroscience. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-29678-2_3256View
J Randall Flanagan, Miles C Bowman, Roland S Johansson. Control strategies in object manipulation tasks, Current Opinion in Neurobiology. Volume 16, Issue 6, 2006, Pages 650-659. https://doi.org/10.1016/j.conb.2006.10.005.View
Shumway-Cook, A., & Woollacott, M. H. (2017). Motor control: Translating research into clinical practice. Philadelphia: Lippincott Williams & Wilkins. APA (6th ed.)View
Pardhan, S., Scarfe, A., Bourne, R., &Timmis, M. (2017). A comparison of reach-to-grasp and transport-to-place performance in participants with age-related macular degeneration and glaucoma. Investigative Ophthalmology & Visual Science, 58(3), 1560-1569.View
Land, M. F., & McLeod, P. (2000). From eye movements to actions: how batsmen hit the ball. Nature Neuroscience, 3(12), 1340-1345.View
Leigh, A.M. , John, F.S.(2007).Target interception: hand-eye coordination and strategies.View
Ji-Hye Junga, Si-EunKob, Seung-Won Leec (2014) Immediate effects of single-leg stance exercise on dynamic balance, weight-bearing and gait cycle in stroke patients. Physical Therapy Rehabilitation Science 3(1):49-54DOI: 10.14474/ ptrs.2014.3.1.49View
Rosario, M.G., Hyder, A., Orozco, E., VélezBartolomei, J. G., Quiñones, C. L., &Bayron, F. (2020)A. Evaluating static postural control in subjects with controlled-diabetes Mellitus II. Journal of Human Sport and Exercise, 15(2): 344-354. doi:10.14198/jhse.2020.152.09View
Rosario, M.G., Marshall, J., Herkert, A., Binoy, B., Windham, H., & Orozco, E. (2020)B. Lower Limb Neuromuscular Modification and Standing Postural Control Alteration in Apparent Asymptomatic People Living with HIV. J Rehab Pract Res, 1(1):102. https://doi.org/10.33790/jrpr1100102
Peterka, RJ. Sensorimotor integration in human posture control. J Neurophysiol 2002; 88:1097-1118.View
Gomez-Bruton A, Navarrete-Villanueva D, Pérez-Gómez J, Vila-Maldonado S, Gesteiro E, Gusi N, Villa-Vicente JG, Espino L, Gonzalez-Gross M, Casajus JA, Ara I, Gomez-Cabello A, Vicente-Rodríguez G. The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4312.View
Kear, B. M., Guck, T. P., & McGaha, A. L. (2017). Timed up and go (tug) test: normative reference values for ages 20 to 59 years and relationships with physical and mental health risk factors. Journal of primary care & community health. 8(1), 9–13. doi. org/10.1177/2150131916659282View
Peyton, E. L., Kirstie, A. F.(2017). Out with the Old?’ Why coarse spatial datasets are still useful for catchment-scale investigations of sediment (dis)connectivity . https://doi. org/10.1002/esp.4131View
White MS, Addison CC, Jenkins BW, Bland V, Clark A, LaVigne DA. Optimistic Bias, Risk Factors, and Development of High Blood Pressure and Obesity among African American Adolescents in Mississippi (USA). Int J Environ Res Public Health. 2017 Feb 20;14(2):209. DOI: 10.3390/ijerph14020209. PMID: 28230728; PMCID: PMC5334763.View
Martinez Aguirre-Betolaza A, Mujika I, Loprinzi P, Corres P, Gorostegi-Anduaga I, Maldonado-Martín S. Physical Activity, Sedentary Behavior, and Sleep Quality in Adults with Primary Hypertension and Obesity before and after an Aerobic Exercise Program: EXERDIET-HTA Study. Life (Basel). 2020 Aug 17;10(8):153. DOI: 10.3390/life10080153. PMID: 32824416; PMCID: PMC7460177.View
Soguel Schenkel N, Burdet L, de Muralt B, Fitting JW. Oxygen saturation during daily activities in chronic obstructive pulmonary disease. Eur Respir J. 1996 Dec;9(12):2584-9. DOI: 10.1183/09031936.96.09122584. PMID: 8980973.View
Chery,l D.F., Te-Ching, C., Xianfen, L.(2012).Prevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999-2010. NCHS Data Brief. Aug;(103):1-8.View
World Health Organization. (2020) Physical Activity. Retrieved 01/5/2021 from: https://www.who.int/news-room/fact-sheets/ detail/physical-activityView