
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 3 (2021), Article ID: JMHSB-150
https://doi.org/10.33790/jmhsb1100150Review Article
Suicide among South Asians in the United States: Perspectives, Causes, and Implications for Prevention and Treatment
Susheelabai R. Srinivasa, Ph.D.1, Sudershan Pasupuleti, Ph.D.2*, Rani Dronamraju, LMSW, QIDP 3, Denise Longoria, Ph.D.4
1,4Department of Social Work, University of Texas Rio Grande Valley, United States.
2* Professor, Department of Social Work, University of Texas Rio Grande Valley, United States.
3Clinical Social Work, University of Michigan, County Community Mental Healthcare, United States
Corresponding Author Details: Sudershan Pasupuleti, Ph.D., Professor, Department of Social Work, University of Texas Rio Grande Valley, United States. E-mail: sudershan.pasupuleti@utrgv.edu
Received date: 23rd September, 2021
Accepted date: 21st October, 2021
Published date: 28th October, 2021
Citation: Srinivasa, S. R., Pasupuleti, S., Dronamraju, R., & Longoria, D. (2021). Suicide among South Asians in the United States: Perspectives, Causes, and Implications for Prevention and Treatment. J Ment Health Soc Behav 3(2):150.
Copyright: ©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Introduction
Suicide and suicide related behaviors have been a global phenomenon. Suicide is a major social problem with more than one million deaths and 25 million attempted suicides [1] and 140 million who reported ideation [2]. Specifically in the US, it is the tenth leading cause of death with a staggering 47,173 Americans who committed suicide and 1,400,000 who attempted suicide. Nearly 575,000 Americans visited a hospital with self-inflicted injuries [3]. Astonishingly, the number of suicidal deaths is greater than the total number of deaths from homicide, AIDS, car accidents combined [4]. The cost of suicide and self-injury was over $ 70 billion in medical as well as work loss expenses in the United States [5]. The highest suicide rate (20.2) percent is prevalent among middle-aged adults in the age group of 45 to 54 years old; followed by older adults 85 years of age and older with (20.1) percent. Among young adults and adolescents in 15-24 years, it was 14.46 percent in 2017. According to the Center for Disease Control and Prevention [6], suicide rates were 6.59% among Asian & Pacific Islanders, 6.61% among African Americans and 13.42% among American Indians and Alaskan natives in 2019. It was highest (15.85%) among the Caucasian population. White males account for nearly 70 percent of all suicides occurred in the United States though females make twice the number of suicidal attempts. Firearms was the number one means used since 50.57 percent of those who committed suicide used this method [7].
The US Census doesn’t provide specific sub-groups of Asian Americans in collecting the data and so suicide data for South Asians and other subgroups is never available. A compilation of the incidences of suicide of South Asians are included among all Asian Americans. Research literature cited high suicidal rates among South Asians, especially women, contrary to the trend found in the larger American population [3]. SAALT (2019) reported that nearly 5.4 million South Asian origin live in the United States of America and 472,000 or 10 percent of them approximately live in poverty. Poverty has many ramifications that affect their health and mental well-being and access to services. Table 1 presents suicide rates among different racial groups in the United States.
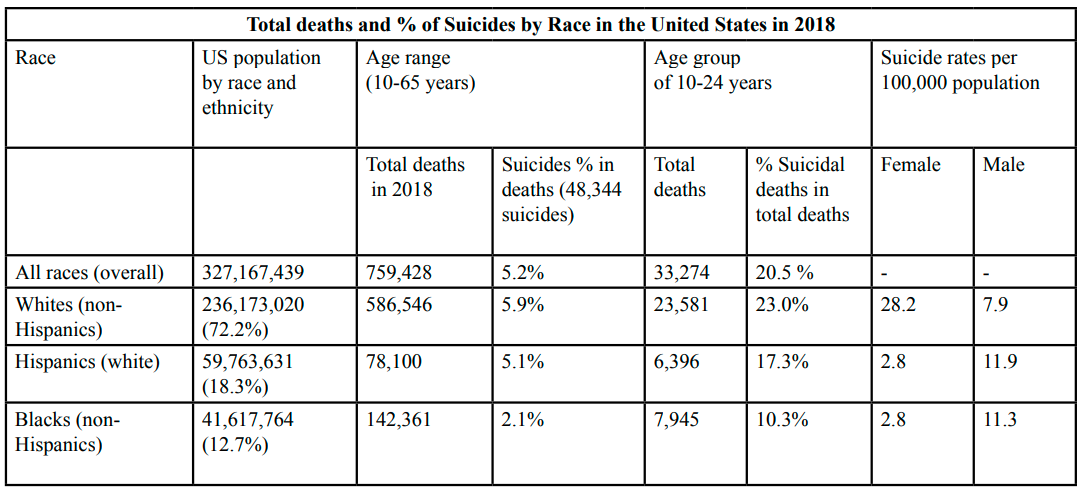
Table 1.Suicide incidence by age groups and race/ethnicity (48,344 suicides) 2018
Literature on Suicide in the U.S. and among the South Asians
There is limited literature on suicide among Asian Americans. The study by Leong et al. [8] reported, “Suicide is not actively deterred in Hinduism.” In fact, Hindu Dharma categorically prohibits suicide. Followers of Hinduism believe souls are eternal and death doesn’t destroy it. Hindu Dharma, rooted in four Vedas and its elaborations in the forms of Aranyakas and Upinishads, comprises complex and sophisticated belief system. This belief system recognizes one universal God, Brahman, Parameshara, and Iswara. The goal of human life is to lead a righteous karma that liberates human from the cycle of birth and rebirth. ‘Karma’ includes both good and bad actions. Leading Dharmic life and performing good deeds per the scriptures would earn credits for liberation from this cycle, while bad Karmas prolong it. Without going through Karmas, one can’t attain moksha (a state like salvation). As per Hindu scriptures and beliefs, a person does not have right to end one’s life. Suicide is not allowed in Hindu Dharma. The soul will be born many times, and this is called reincarnation. The life and death cycle will continue until an individual completes one’s ‘Karmas’, both good and bad acts (Bhagavad Gita, n.d.).
A 'model minority image’ of the South Asians as in Asian Americans creates subtle pressure which places high expectations on individuals. Sometimes this burden of high expectations is unbearable and might lead suicidal ideation resulting from feelings of unworthiness and depression. Leong, Leach, Yeh, & Chou [8] study reported higher suicide rates among Hindu men compared to Hindu women in the United States. Karma theory is based on the cause and effect and the moral life, but it is incorrectly assumed to encourage self-harm and suicide. The authors’ interpretations of the Hindu beliefs on suicide are not consistent with the Hindu scriptures and beliefs of followers. The authors highlighted that the reasons for suicide were not uniform and consistent within the literature.
Among different causes of adolescents’ deaths, suicide is third highest killer. Psychopathology, stressors, alcohol, and substance use are major factors associated with suicide [9]. Alcohol consumption is significant predictor of suicidal attempts among adolescents, 17 times higher likely in males and 3 (three) times in females. Suicide and suicide rates differ among different ethnic groups, it is higher among Asians in the United States. Depression is four times likely to prompt suicidal behavior among Asian youths compared to other ethnic groups. Parental conflict is a major factor (17 times higher) for suicidal attempts and suicide in Asian origin adolescents [9]. In another research study on Indian immigrants, it was reported that children 15 or older had higher incidences of suicide after they migrated to other countries than when they lived in India [10]. In a study by Lane, Cheref, & Miranda [11], hopelessness, depressive symptoms, and suicidal ideation were identified as factors affecting 204 South Asian undergraduate students.
Case Narrative 1
Mr. X was a 28-year-old young man who came to the United States of America when he was 26 years old. He had completed his engineering degree and worked in India for a couple of years. He came to complete his master’s degree in engineering and got a job in a fortune 500 company. He lived in an apartment and was in constant communication with a couple of his distant family members who lived in the state where he worked.
He always wanted to be a cricket player and was also selected for a local team for Ranji Trophy and played very well. He came from an orthodox South Indian family. His family insisted that he would not be a cricket player, continue to complete his education, and work in the field of engineering.
It seemed to his family and close friends that he was not a happy person, but he did not seem to let that dampen the spirit of get togethers. He seldom talked to others and was considered a ‘strong, silent man’. In March 2016, his friends and local family were concerned as they had not heard from him for the past 10 days. They called him and he did not respond. They called him at work, and they were told that he was not at work for the past three days. One of the family members decided to go by his apartment and found that there were police cars around his apartment area. The apartment management was called by the neighbors as they smelt something foul from the apartment. The apartment authorities opened the door, they saw the dead body in a chair in the living room. He was clutching a picture of his Guru in his hand. He wrote a suicide note taking complete ownership of this decision. He emphasized that his family, friends, or anyone at work was responsible for his suicide. He was tired of not being able to complete his dream. He was not happy with the goals he was pursuing and wanted to end his life (Case notes, Interview with a family member, 2019).
Case Narrative 2
This was an 18-year-old girl, senior in high school. Her mother was a psychiatrist and a single mom. She lived in her parental home with her brother and sister. She was in general calm, composed, and gentle person. Her family didn’t have any issues with her. She was also helpful to her mother and siblings. She was an average student in school and did not participate in too many extra-curricular activities. She was planning to go to the local community college and did not attempt to do the SAT or other exams. Y dealt with some health issues and was dealing with seizure disorder. She did everything to stay healthy but struggled to stay on top of it and seizure free. She felt that this health problem impacted her capability of living a complete life. She could not drive and was constantly dependent on her mother and siblings to transport her.
On the day of her suicide, she was in communication with her mother to go to a doctor’s appointment in the evening after her mother’s work. She told her siblings that she was going to finish her laundry in the basement as she was busy in the weekend. Her siblings were busy with their schoolwork and did not register it as an important statement to respond to. She went to the basement and decided to commit suicide by hanging herself. Her mother came to look for her and was devastated that she took her life. (Case notes, Interview with family member, 2019).
Case Narrative 3
Mrs. Z was a 48-year-old woman who was a scientist herself and the wife of a professor at a major university. She had two children who were 14 years and 16 years at the time of her death. Mrs. Z was dealing with schizophrenia and tried to get treatment. She did not follow her treatment well and was dealing with trauma related to family micro-aggressions, family taboo, and prestige issues. Many individuals that she knew tried to support her and direct her to find solutions, but Mrs. Z chose options that were ultimately detrimental to her well-being and extremely stressful for her family. Though Mrs. Z was an educated woman with a master’s degree, she couldn’t maintain her job because she was frequently suspicious that others were tampering with her computer and things. She would quarrel with everyone and that led to her being fired. She had a trail of jobs that she was fired from because of her attitude, inability to work, and struggling to complete her assignments. This situation became more difficult for her, and events spiraled downward.
Her domestic life was also going south. She started suspecting her husband of having an affair and created more havoc in their already turbulent life. She left the house one evening after an argument stemming from a false suspicion about her husband. She stopped taking her medications and kept going from place to place. Her friends stopped allowing her to stay with them. She had no place to go and no job. She stayed in the homeless shelter for a couple of days. She left the shelter after she was ridiculed and insulted (in her perception) by the other homeless inmates. She imagined that the TV was talking to her, and the fan was going in several directions. She was afraid that the fan would fall on her. She didn’t seek any help. She was noticed by the shelter officials who tried to get her a psychiatric appointment in order to put her back on medications. She started feeling restless and walked away from the shelter. She was found dead the next day in a small ledge behind the bank, where she had overdosed on her mental health medication.
Suicide from Durkheim’s Perspective and Relevance to South Asian situation in the United States
A 19th century sociologist, Durkheim, published “Le Suicide” book in 1897, which provided sociological perspective on suicide. He identified social factors responsible for suicidal behaviors, besides psychological and emotional factors. He pointed out that individuals who are isolated and not in close relationships, tend to commit suicide in the absence of social support and social connectedness. Durkheim believed and attributed those reasons for higher rates of suicide among the soldiers than in civilians. He classified suicides into three categories such as anomic, altruistic, and egoistic suicides. According to Durkheim, social disconnection, excessive regulation of individual behavior, loss of self-respect, social status, and oppressive conditions were identified as major causes for suicidal behavior.
Although the Durkheim theory is a century old, some causes and aspects of suicide theory overlap some that have been identified in the latest literature on suicide. There has been an increase in suicide rates in the past decade. The United States Census data specifically pertaining to South Asians is not available, but information is included as Asian American as whole without information about ethnic subgroups within. South Asians have a lower suicide rate compared to the national suicide rate is misleading and doesn’t capture hidden reality [12]. However, data presented in research studies [11] revealed nearly 1 (one) percent of South Asians reported suicidal ideation; 4.13 percent reported feelings of hopelessness; and 12.35 percent identified depressive symptoms. It is important to note that 1.34 percent of Indian Americans, the largest ethnic group among the South Asian population, reported high rate of suicidal ideation, attempts and suicides. The issues of South Asian Americans is shadowed by racial categories used by the United States Census.
Stressors and Pressures of South Asians in the US that Push them to Suicide
The first-generation South Asian immigrants encounter complex situations such as staying away from family [13,14,15] acculturative stress; and language barrier issues [16]. The homeostasis of these individuals may be disturbed because of sociocultural challenges and psychological issues faced in the new environment. In another important study on South Asians students, the authors summarized that transition of adolescence to adulthood was identified as a period of high risk for suicide, making it the second leading cause of death among individuals in ages 15 to 24 [17]. Gater et al., [18] supportive evidence revealed that mental health concerns were not addressed among South Asian students who participated in their study.
Causes of Suicide for the South Asians in the US and its intersectionality Familial and Cultural Factors
Some individuals have genetic predispositions to mental health conditions such as bipolar disorder or schizophrenia. Family conflict in South Asian families contribute to women’s unhappiness, depression, and domestic violence. South Asians do not feel comfortable sharing their personal information or family problems with their health care providers in order to protect family dignity [19]. South Asians do not tell providers about any suicidal thoughts because they don’t trust them. There is also a negative stigma about seeking help from providers. Cultural non-acceptance, stigmatization of mental health services, and a lack of cultural sensitivity in the existing mental health services all contributed for underutilization of mental health services. South Asian younger women in the age group of 15-34 years committed high rates of suicide.
The cultural conflict (low acculturation) of the two cultures can be highly stressful and may impact the mental health of South Asians in the United States [20]. Parental conflict is also arising out identity crisis that youth go through due to the choice between their own ethnic group culture and mainstream culture. Middle and high school students of South Asian and Southeast Asian origin experienced higher rates of suicide attempts and suicide [21]. Studies reported that shame/disgrace triggered suicide in a few cases of suicide by Asian American youths [22]. Individuals in vulnerable situations do not know how and from whom to seek guidance and help. The family perceives it as a burden and disgrace to have a family member who is suffering from mental illness. In addition, there is the inability to afford professional help, the stigma, shame, and hesitation to share mental health problems with family, friends, or society [23,24]. Cultural model of suicide has was developed that integrated four cultural factors after extensive secondary research of published articles that linked culture and suicide. These four factors included cultural sanctions, idioms of distress, minority stress, and social discord [24].
Socioeconomic Factors
Tummala-Narra [16] reported that the immigrants from South Asia experienced a lot of problems with assimilation in the United States as competing with the mainstream population becomes challenging. Average people failing in the competition, they might be rendered unemployed or underemployed and get pushed into poverty. This may also lead to homeless that condition results in a spectrum of issues such as mental health, substance use and suicidal ideation. Many young South Asians including teens perceive underperforming in high schools is the end of road for them and regard themselves unworthy. Such thoughts of hopelessness and depression affected 3 percent of the population below the age of 18 years who tend to have suicidal ideation.
Fuller [25] says that individuals dealing with mental health issues at times become aggressive to overcome their failing functionality. Such illnesses cause them to lose employment, friends, and families, thus, the negative effect of hopelessness and depression continues. Comorbidity for a few, was a major factor for suicide amongst South Asians.
Health Beliefs and Help-seeking Behaviors
There are dormant widespread concerns about mental health among South Asians, but they are not acknowledged, and people don’t seek help. Many South Asians do not even think they have to address. Career and work-related issues cause a lot of anxiety, stress, and depression. Some studies conducted in the United Sates (Lane, Cheref, & Miranda [11] have examined predictors of depression and concluded that physical factors such as old age and poor health in combination with perceptions of illness. Feelings of isolation, lack of help-seeking, and lack of adherence to mental health treatment regimens, are the cause of many fatal decisions taken by individuals.
Intersectionality Model for Suicide
Based on the real case narratives and the available literature, the researchers have developed a model of intersectionality of factors which contributed to suicide. The socioeconomic factors included family expectations, economic hardships, lack of health insurance, gender, ethnicity, and cultural beliefs, cognitive impairment, and mental health conditions.
The intersectionality of socioeconomic factors, along with the mental health issues compel and determine the course of action. Below is a pie diagram depicting the intersectionality model. Recent literature indicated a wide range of causes for suicide. The first set of factors include life stresses, break ups, legal problems, academic failures, and loss of close relatives/ family members, and friends [26]. A second set of factors involves mental health conditions such as depression, bipolar disorder, schizophrenia, borderline, or anti-social personality disorders, conduct disorders, substance use disorders, chronic health conditions, exposure to suicide, access lethal weapons, childhood abuse [27], violence and incarceration (National Institute for Mental Health, 2015). Family history of suicide or childhood maltreatment, cultural and religious beliefs, social isolation, and lack of access to mental health services, and unwillingness to seek help, are other reasons behind suicide [28].
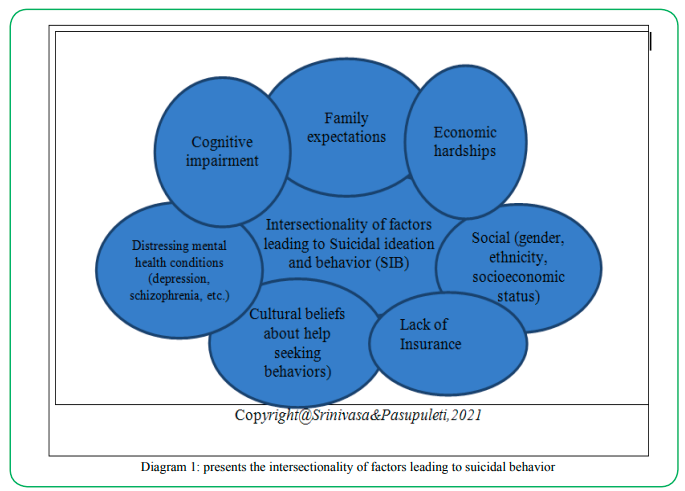
Diagram 1:presents the intersectionality of factors leading to suicidal behavior
The Bhutanese Refugees: Situational Analysis of South Asian Community
The Bhutanese refugees have dealt with a huge crisis which was spurred by systematic oppression. This is one of the reasons why refugees have experienced torture, poor living conditions, and general trauma exposure before and after fleeing from their country and in refugee camps too. These traumatic experiences pose a higher risk factor for eventual medical and health related problems, such as post-traumatic stress disorder (PTSD) [29]. Some of the stressors are family conflict, anxiety related to family who are in refugee camps; difficulty in obtaining employment for unskilled workforce; lack of health services; lack of culturally sensitive trained professionals who can understand the mental health problems which affect the Bhutanese ethnic group; and lack of language translators.
These post-migration stressors correlate with the elements of the Interpersonal- Psychological Theory of Suicidal Behavior (IPTS) including thwarted belongingness and perceived burdensomeness. These factors act as barriers in seeking treatment for mental health issues [30]. Factors beyond their control include separation from family, and inability to manage or control their choices in life. The disconnect was enhanced by the difficulty to maintain cultural and religious traditions. This causes emotional drain without lack of support to maintain good mental health [31]. Elevated social alienation, which includes a perception that their existence is a burden to the world. Increased acquired capacity for suicide, which is evident in the increased pain tolerance due to their trauma, and personal experiences of frightening stimuli. Presence of perceived burdensomeness and social alienation causes the individuals to have a ‘concrete or abstract’ desire for suicidal ideation, intention, and suicidal death [32,33].
The current suicide epidemic in the Bhutanese refugee community can be reduced by having more refugee outreach and education to assist with prevention [34] Cultural sanctions are noted to be a good evidence-based practice in the Bhutanese culture. Many Bhutanese, who are Hindus or Buddhists, understand that it is clearly in their religious doctrine that suicide is condemned. These cultural sanctions protect and may assist an individual to refrain from taking the extreme steps. Establishing religious or cultural centers assist individuals to assimilate and be in touch with their religion amongst Bhutanese [35]. Religious involvement, Buddhism specifically, was shown to be protective against anxiety and depression [36]. Religious beliefs and ceremonies for spiritual fulfillment, may provide social support and spiritual coping. Temples act as centers for social gathering where there is networking, support, resources, and food distribution. These services alleviate some of the stressors that may be linked to suicide [36]. The model of cognitive behavioral therapy (CBT) has shown to assist individuals in reframing their trauma and stress to moderate the triggering events and not respond to the stress [29]. Acceptance and commitment therapy (ACT) combines mindfulness with CBT (Cognitive Behavior Therapy) has shown a lot of promise in assisting individuals who are dealing with suicidal ideation or intention [37].
In response to the high rate of suicidal behaviors among Bhutanese refugees resettled in Vermont, the co-authors (PI: J.M.) began a suicide risk detection study in Burlington, aiming to deliver better risk detection and elucidation of culturally responsive risk factors. This study threw light on methods of providing support and removed some of the blind spots to reduce the rate of suicide. The National Center for Injury Studies reflected on the suicide problem of the Bhutanese. The practice of Buddhists’ prayers and meditation helps them maintain calmness [24]. This has also assisted them spiritually, to balance stress and maintain well-being [24]. Most effective techniques with this population are mindfulness-based methods such as meditation, breathing, MBSR (Mindful Based Stress Reduction). As the Interpersonal- Psychological Theory of Suicidal Behavior (IPTS) specifies, the suicidal behavior in Bhutanese was due to the combination of three factors.
Gaps in the Literature in subset of Asian population in the United States
The CDC has no recorded data specifically pertaining to Asian American sub-groups and with regards to South Asians. The data classification is very broad and titled as Asian Americans. Jha, Ahuja, Wani & Bavikatte [38] identified huge gaps in the literature. At present, there is lack of available literature on associated risk factors, suicidal attempts, or incidence of suicides. The factors were from the study indicated financial problems, lack of social support, and marital problems were factors responsible for the risk of suicide. The factors that were identified as themes and are presented in the diagram 1. Furthermore, most research studies are conducted in English and can’t cover the non-English speakers, so the viewpoints of non-English speakers are not captured. These are the gaps in research on South Asians. Fernando [39] reported that there is a dearth of literature on the status of the mental health of South Asians and only 10 percent of this subset of population have a place in the literature. Lack of knowledge among mental health professionals on this ethnic group’s values, cultural traditions, and religious beliefs were identified.
One vital finding was that the Western model of treatment was not meeting the needs of the South Asian group. Culture-bound restrictions in help-seeking contributed to perceptions about mental health of this ethnic group. Ahmad-Stout et. al. [40] investigated beliefs and highlighted help-seeking behaviors among South Asians in the United States. Limited research has been done on South Asians in the United States. Although the rate of prevalence of suicide among South Asians is higher than other ethnic groups, the risk factors among Asian and Non-Asian cultures are widely different and in-depth literature is lot more desired.
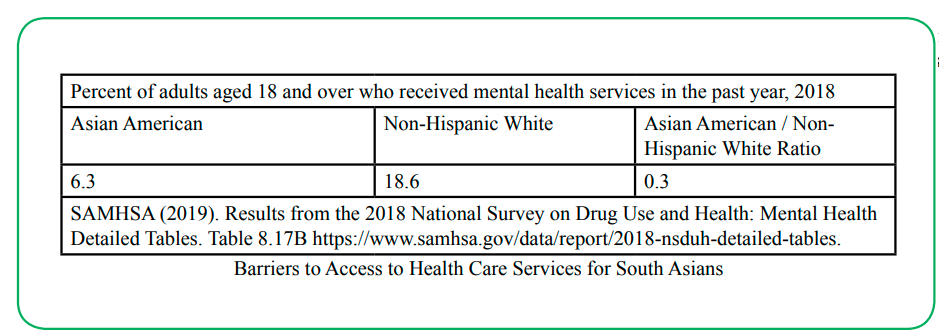
Barriers to Access to Health Care Services for South Asians
The feeling of dejection and shame caused by social, environmental, and other reasons closes all options of finding a solution for their problems and resort to taking their lives. Males are at higher risk for suicides across the ethnic groups ranging from 9.9 percent in Asian Americans to 33.8 percent in Native Americans. Females witnessed lower rates of suicide though ethnic minority females, especially Asian and Native Americans barring Whites, are at higher risk compared to whites. In terms of average suicide rates per 100,000 population is highest (6.9 percent for Asian American, 7.1 percent for African Americans, 6.9 percent in Hispanic and 22.4 percent in Native Americans) among ethnic minorities. These highlights need for comprehensive approach to suicide among ethnic minorities.
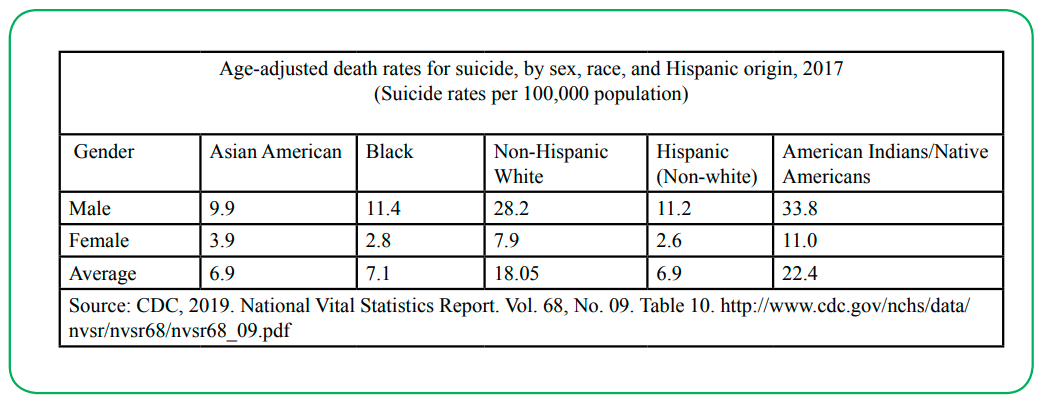
Source: CDC, 2019. National Vital Statistics Report. Vol. 68, No. 09. Table 10. http://www.cdc.gov/nchs/data/ nvsr/nvsr68/nvsr68_09.pdf
There is scant literature about these barriers here in the United States. The barriers are the same when it comes to accessing services among other ethnic groups, too. In a study in Hong Kong, on South Asians Vandan et. al., [41] identified language and culture as common barriers. Like South Asians, the Latinos, who have migrated to the United States, experience similar challenges and barriers [42].
Bhutanese refugees living in the U.S. have a significantly elevated rate of suicide [43] than the general U.S. population [44]. This data highlighted that risk assessments predicted on the presence of suicidal ideation would result in under-identification of these refugees at risk for suicide. Some of the barriers include not seeking therapy and taboos relating to not seeking mental health treatments. It is believed that a majority of 11,000 refugees settled in United States [45]. They may not display clinical risk factors within the first six months or not be able to communicate it well during the screening process. Some of the other factors include improper identification of suicidal behaviors and subsequent intervention [46]. In the absence specific statistics on South Asian population, data compilation inaccurate and are not available [6].
Another barrier to treatment or prevention of suicide is the trauma and torture that the Bhutanese endured. These are risk factors for general psychopathology and suicide among the Bhutanese refugees [47,48,49]. Suicidal ideation is also stigmatized within Bhutanese culture. Hence, relying on traditional suicide indicators of suicidal ideation may not be ideal [24].
Implications for suicide prevention and treatment services for South Asians in the United States
This has important implications for treating individuals belonging to different racial, ethnic, and cultural groups in the United States, as discussed in detail in the Surgeon General’s Report, Mental Health: Culture, Race, and Ethnicity (US DHHS, 2001). Lately, the patient data is electronically available, and it will be easy to exchange the data and do the data transfer. Data from all healthcare providers such as clinicians’ offices, county hospitals, and other healthcare departments and facilities, should be collected and reported - including information on suicides, attempted suicides, and suicide ideation to update the specific data sets.
Important lessons learnt from Nath, Van Leer & Ahmad-Stout [50] research are beliefs and help-seeking behaviors. Aspects to guide people to accept help for mental health treatments and services. This acceptance of help-seeking can maximize health, mental, and wellness. Culture can promote or prevent acceptance. Not attaching stigma can prevent people from being affected and victimized by the risk factors for suicide. Culture-specific and community-based education about mental health needs to be developed and implemented with inputs from respective communities. The study was modeled on the United Kingdom’s study in which seventy South Asians participated in an internet survey on “Reasons for Living” (RFL).
A lower score on RFL indicated a higher risk for suicide. South Asian ethnic groups had higher rates of suicide, especially younger women (15-34 years). High suicide rates among Hindus, compared to Muslims, was attributed to Hindu beliefs, even though the beliefs (as per Hindu scriptures) prohibit and condemn suicides. Limited research was available on South Asians living in the United States. South Asians struggles with disconnect from family and lack of supportive ‘social networks.’ This causes despair in social and cultural situations, wherein both the integration, love, comfort, caring, feeling of belonging, regulation, obligations, duties, responsibilities, and oversight are either non-existent or minimal. In this state, individuals’ resort to suicide as a solution (Society and Culture, 2002, p.195).
Suicide as a public health problem as well as a social problem that requires public attention. Stigmatizing it will prevent or withhold people from reporting and help-seeking. Health education to the public and public health messages will desensitize people and make it acceptable for people to report suicidal incidences. Attention to public insensitiveness and dissonance towards their family members and their close friends is of prime importance and approaching suicide should be given more consideration. These steps should help sensitization and should promote awareness about mental health and result in more reporting. Societal and local community support and empathy should replace stigmatization. Even bystanders should take the responsibility to report. Suicide reporting should be encouraged and appreciated. Community-based support systems and crisis-responders should be available to provide support to at-risk individuals. Mental Health First Aid program is great initiative in this direction. It should be widespread across different stakeholders in the United States.
Conclusion
South Asians come to North America and make the United States their home having high hopes of improving their quality of life for themselves and their family. They also hope to improve their lives by meeting the expectations of their extended family members in their countries of origin. After arriving in the United States, they find a discrepancy between their imagination and reality. The road and process to success is long and time consuming. Hence, stress arising out of this discrepancy, causes imbalance in their life’s homeostasis. The after effects of migration and the transitional problems and issues arising from cultural adaptation may sometimes end up at a point of crisis, or breakdown, resulting in suicide.
The psychopathological, psychosocial, economic, and cultural issues intersect with the sad concoction of socio-economic problems, along with the mental health issues, social issues like violence, poverty, and unemployment, can create a ruinous situation in a person’s life. This may sadly conclude in individuals ultimately resorting to closure of their lives.
Conflict of interests:
The authors declare no conflict of interest.
References
Franklin, J. C., Ribeiro, J. D., Fox, K. R., Bentley, K. H., Kleiman, E. M., Huang, X., Musacchio, K. M., Jaroszewski, A. C., Chang, B. P., & Nock, M. K. (2017). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143(2), 187–232. https://doi. org/10.1037/bul0000084View
Borges, G., Angst, J., Nock, M. K., Ruscio, A. M., & Kessler, R. C. (2008). Risk factors for the incidence and persistence of suicide-related outcomes: a 10-year follow-up study using the National Comorbidity Surveys. Journal of Affective Disorders, 105 (1-3), 25–33. https://doi.org/10.1016/j.jad.2007.01.036View
South Asians Americans Leading Together (SAALT, 2015). A Demographic Snapshot of South Asians in the United States (Fact Sheet). http://saalt.org/wp-content/uploads/2016/01.
Centre for Disease Control and Prevention. (2014, June 12th). Health, United States, 2014 with Special Feature on Adult Aged 55-64. https://www.cdc.gov/nchs/data/hus/hus14.pdfView
Center for Disease Control and Prevention (2020). Web-based Injury Statistics Query and Reporting System (WISQARS). (2020) Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control.View
Centre for Disease Control and Prevention (2019, June 12th). Summary Health Statistics: National Health Interview Survey: 2017. Table http://www.cdc.gov/nchs/nhis/shs/tables.html View
Center for Disease Control (2017). National Center for Health Statistics. https:www.cdc.gov/nchs/data/hestat/suicide/ rates_1999_2017.htmView
Leong, F. T., Leach, M. M., Yeh, C., & Chou, E. (2007). Suicide among Asian Americans: what do we know? What do we need to know? Death studies, 31(5), 417–434. https://doi. org/10.1080/07481180701244561View
Groves, S. A., Stanley, B. H., Sher, L. (2007). Ethnicity and the relationship between adolescent alcohol use and suicidal behavior. International Journal of Adolescent Medical Health. 19(1):19-25. doi:10.1515/ijamh.2007.19.1.19. PMID: 17458320.View
Patel, S. P., & Gaw, A. C. (1996). Suicide among immigrants from the Indian subcontinent: A review. Psychiatric Services, 47(5), 517–521. https://doi.org/10.1176/ps.47.5.517View
Lane, R., Cheref, S., & Miranda, R. (2016). Ethnic Differences in Suicidal Ideation and its Correlates among South Asian American Emerging Adults. Asian American Journal of Psychology, 7 (2), 120–128. https://doi.org/10.1037/ aap0000039.View
Curtin, S. C., Warner, M., & Hedegaard, H. (2016). Increase in Suicide in the United States, 1999-2014. National Center for Health Statistics Data Brief, (241), 1–8.View
Das, A. K., & Kemp, S. F. (1997). Between two worlds: Counseling South Asian Americans. Journal of Multicultural Counseling and Development, 25(1), 23–33. Against Women, 5(6), 591-618.View
Dupree, W.J., Bhakta, K.A., Patel, P.S., & Dupree, D.G. (2013). Developing Culturally Competent Marriage and Family Therapists: Guidelines for Working with Asian Indian American Couples. The American Journal of Family Therapy, 41 (4), 311-329.View
Rastogi, M. (2007). Coping with transitions in Asian Indian families: Systemic clinical interventions with immigrants. Journal of Systemic Therapies, 26(2), 55–67.View
Tummala-Narra, P. (2013). Psychotherapy with South Asian women: Dilemmas of the immigrant and first generations. Women & Therapy, 36(3-4), 176-197. doi:10.1080/02703149.2 013.797853.View
Kessler, R.C., Berglund, P., Borges, G., Nock, M., Wang, P.S. (2005). Trends in Suicide Ideation, Plans, Gestures, and Attempts in the United States, 1990-1992 to 2001-2003. Journal of American Medical Association, 293 (20):2487–2495. doi:10.1001/jama.293.20.2487View
Gater, Richard & Waheed, Waquas & Husain, Nusrat & Tomenson, Barbara & Aseem, Saadia & Creed,Francis. (2010). Social intervention for British Pakistani women with depression: Randomized controlled trial. The British journal of Psychiatry: The Journal of Mental Science, 197. 227-33. 10.1192/bjp. bp.109.066845.View
Pratomthong, S. J., & Baker, S. B. (1983). Overcoming obstacles to the growth and development of guidance and counseling in Thailand. Personnel & Guidance Journal, 61(8), 466–469. https://doi.org/10.1111/j.2164-4918.1983.tb00073.xView
Lau, A. S., Jernewall, N. M., Zane, N., & Myers, H. F. (2002). Correlates of suicidal behaviors among Asian American outpatient youths. Cultural Diversity and Ethnic Minority Psychology, 8(3), 199–213. https://doi.org/10.1037/1099- 9809.8.3.199View
Supple, A. J., Graves, K., Daniel, S., Kiang, L., Su, J., & Cavanaugh, A. M. (2014). Ethnic, gender, and age differences in adolescent nonfatal suicidal behaviors. Death Studies, 37, 830–847. doi:10.1080/07481187. 2012.699909View
Blinn, R. E. (1997). Asian-American and Chinese American suicide in San Francisco. Doctoral dissertation. Retrieved from ProQuest Dissertations and Theses (Accession Order No. 9639830).
Lester, D. & Rogers, J. R. (2013). Suicide: A Global Issue [2 volumes]: A Global Issue. Santa Barbara, CL: Preager.
Chu, J.P., Goldblum, P., Floyd, R., & Bongar, B. (2010). The cultural theory and model of suicide. Applied and Preventive Psychology, 14(1–4), 25–40. 10.1016/j.appsy.2011.11.001View
Fuller, J. R. (1988). Martial arts and psychological health. The British journal of medical psychology, 61 (Pt 4), 317–328. https://doi.org/10.1111/j.2044-8341.1988.tb02794.xView
American Association of Suicidology (2006). Facts and Statistics. https://suicidology.org/facts-and-statistics/View
American Foundation for Suicide Prevention. (2015). Frequently asked questions: What should I do if someone tells me they are thinking about suicide? Retrieved from https://www.afsp.org/ preventing-suicide/frequently-asked-questions
Centre for Disease Control and Prevention. (2014, June 12th). Health, United States, 2014 with Special Feature on Adult Aged 55-64. https://www.cdc.gov/nchs/data/hus/hus14.pdfView
Vonnahme, L.A., Lankau, E.W., Ao, T., Shetty, S., Cardozo, B.L. (2015). Factors associated with symptoms of depression among Bhutanese Refugees in the United States. Journal of Immigration Minor Health, 17(6):1705–1714.View
Ellis, B.H., Lankau, E.W., Ao, T., Benson, M.A., Miller, A.B., Shetty, S., & Cochran, J. (2015). Understanding Bhutanese refugee suicide through the interpersonal-psychological theory of suicidal behavior. American Journal of Orthopsychiatry, 85(1), 43–55. 10.1037/ort0000028.View
Ao, T., Shetty, S., Sivilli, T, Blanton, C, Ellis, H, Geltman, P.L., Cochran, J., Taylor, E., Lankau, E.W., Lopes Cardozo, B. (2016). Suicidal ideation and mental health of Bhutanese refugees in the United States. Journal of Immigrant and Minority Health, 18, 828–835.View
Klonsky, E. D., & May, A. M. (2014). Differentiating suicide attempters from suicide idolators: a critical frontier for suicidology research. Suicide & Life-threatening Behavior, 44(1), 1–5. https://doi.org/10.1111/sltb.12068.View
Nock, M.K., Borges, G., Bromet, E. J., et al. (2008). Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. British Journal of Psychiatry: Journal of Mental Science, 192: 98–105.View
Ellis, B.H., Lankau, E.W., Ao, T., Benson, M.A., Miller, A.B., Shetty, S., Cardozo, B.L., Geltman, P.L., Cochran, J. (2015). Understanding Bhutanese refugee suicide through the interpersonal-psychological theory of suicidal behavior. American Journal of Orthopsychiatry,85, 43–55.View
Schininà, G., Sharma, S., Gorbacheva, O., Mishra, A.K. (2011). Who Am I? Assessment of psychosocial needs and suicide risk factors among Bhutanese refugees in Nepal and after the third country resettlement. International Organization for Migration. https://www.iom.int/files/live/sites/iom/files/What-We-Do/ docs/Mental-Health-Assessment-Nepal_Final_11March.pdf.
Shrestha, N.M., Sharma, B., Van Ommeren, M., Regmi, S., Makaju, R., Komproe, I., de Jong, J.T. (1998). Impact of torture on refugees displaced within the developing world: Symptomatology among Bhutanese refugees in Nepal. Journal of American Medical Association, 280(5), 443–448. https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC6980157/View
Luitel, N.P., Jordans, M., Murphy, A., Roberts, B., Cambridge, J. (2013). Prevalence and patterns of hazardous and harmful alcohol consumption assessed using the AUDIT among Bhutanese refugees in Nepal. Alcohol. 2013; 48:349–55.View
Jha, A., Ahuja, M., Wani, R., Bavikatte, S. (2019). (Jan. 16-20) Suicide in South Asian Americans: An Emerging Public Health Problem Society for Social Work and Research 23rd Annual Conference session. (Ending Gender Based, Family and Community Violence conference, San Francisco, United States. https://sswr.confex.com/sswr/2019/webprogram/Paper35816. htmlView
Fernando, G.A. (2015). Attempting to bridge the 10/90 divide: special issue on South Asian mental health, International Review of Psychiatry, 27:3, 176-179. DOI: 10.3109/09540261.2015.1065079View
Ahmad-Stout, Farah & Nath, Sanjay & Khoury, Nayla & Huang, Hsiang (2018). Experiences of Intimate Partner Violence: Findings from Interviews with South Asian Women in the United States. Journal of Interpersonal Violence, 36 (1). 088626051775385. 10.1177/0886260517753850.View
Vandan, Nimisha & Wong, Janet & Fong, Daniel. (2018). Accessing healthcare: Experiences of South Asian ethnic minority women in Hong Kong. Nursing & Health Sciences. 21. 10.1111/nhs.12564.View
Barrera, I., & Longoria, D. (2018). Examining Cultural Mental Health Care Barriers Among Latinos. Journal for Leadership, Equity, and Research, 4(1). Retrieved from https://journals.sfu. ca/cvj/index.php/cvj/article/view/35.View
Ao, T., Taylor, E., Lankau, E., Sivilli, T., Blanton, C., Shetty, S., & Lopes-Cardozo, B. (2012). An investigation into suicides among Bhutanese refugees in the US. (Stakeholders Report). Atlanta, GA: Centers for Disease Control and Prevention. [Google Scholar]
National Center for Injury Prevention and Control Division of violence Prevention (2015). https://www.cdc.gov/ violenceprevention/about/index.htmlView
United Nations High Commission for Refugees (2018). United Nations News. Global Perspectives Human Stories. https:// news.un.org/en/tags/bhutan?page
Vandan, Nimisha & Wong, Janet & Fong, Daniel. (2018). Accessing healthcare: Experiences of South Asian ethnic minority women in Hong Kong. Nursing & Health Sciences. 21. 10.1111/nhs.12564.View
Ferrada-Noli, M., Asberg, M., & Ormstad, K. (1998). Suicidal behavior after severe trauma. Part 2: The association between methods of torture and of suicidal ideation in posttraumatic stress disorder. Journal of Traumatic Stress, 11(1), 113–124. 10.1023/A:1024413301064. View
Ferrada-Noli, M., Asberg, M., Ormstad, K., Lundin, T., & Sundbom, E. (1998). Suicidal behavior after severe trauma. Part 1: PTSD diagnoses, psychiatric comorbidity, and assessments of suicidal behavior. Journal of traumatic stress, 11(1), 103–112. https://doi.org/10.1023/A:1024461216994View
Hovey, J. D. (2000). Acculturative stress, depression, and suicidal ideation among Central American immigrants. Suicide & Life—Threatening Behavior, 30(2), 125–139.View
Nath, S. R., VanLeer, S., & Ahmad-Stout, F. (2018). South Asians and suicide: Beliefs about suicide in a U.S. community sample. Asian American Journal of Psychology, 9(4), 334– 343. https://doi.org/10.1037/aap0000145.View