
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Retraction
https://doi.org/10.33790/jmhsb1100165Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-157
https://doi.org/10.33790/jmhsb1100157Research Article
A Systematic Review of Program Outcomes for the National Family Caregiver Support Program Using a Theoretical Approach
Dorothea L. Ivey, PhD, MSW, MPA
Assistant Professor, School of Social Work, University of Southern Maine, United States.
Corresponding Author Details: Dorothea L. Ivey, PhD, MSW, MPA, Assistant Professor, School of Social Work, University of Southern Maine, United States. E-mail: dorothea.ivey@maine.edu
Received date: 22th November, 2022
Accepted date: 22th January, 2022
Published date: 25th January, 2022
Citation: Ivey, D.L. (2022). A Systematic Review of Program Outcomes for the National Family Caregiver Support Program Using a Theoretical Approach. J Ment Health Soc Behav 4(1):157.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The National Family Caregiver Support Program provides grants to states with large populations of citizens ages 70 and older that are formal and informal caregivers to fund support for various services. The Child Welfare Information Gateway (2016) defined kinship caregiving as the full-time care and protection of children by relatives. The purpose of this study is to identify outcomes of state and community level programs initiated by the National Family Caregiver Support Program (NFCSP) that serves informal grandparent caregivers. Micro and macro frameworks of rational decision making, symbolic interaction, and agency theories were used in this study when determining program outcomes. Outcomes reported in this study were: (1) reduced isolation, (2) increased connection to resources, (3) increased independence/empowerment, (4) reduced stress, (5) lower levels of burden, (6) increased well-being, and (7) intergenerational reciprocity. The NFCSP is a significant first step in assisting this population and is an important federal program that provides much needed funding to Area Agencies on Aging (AAA) in support of grandparent raising grandchildren.
Keywords: National Family Caregiver Support Program, Informal Grandparent Caregivers
Introduction
Grandparents assume guardianship roles to grandchildren when the middle generation is unavailable due to death, illness, divorce, unemployment, incarceration, and adolescent childbearing [1-4]. Additionally, grandparents become caregivers to children due to maltreatment and abandonment. Child maltreatment and abandonment can lead to complex negotiations between courts and families to find permanent living arrangements for children when they are no longer able to live with parents. Such living arrangements are formal or informal. Grandparents will continue to play significant roles in raising children for many generations. As a result, common problems encountered by grandparent caregivers are physical/emotional health, role loss, social isolation, and financial strain [2,5-7]. This study elaborates on the various definitions used when referring to relatives raising children as kinship caregivers and kinship foster caregivers to highlight the increase of demographics for informal grandparent caregivers. “Demarcating the boundaries of informal and formal kinship care and establishing the appropriate policies and programs for regulating, supporting, and sustaining these alternative care systems remain as enduring challenges for state and national programs and practice” [8] (P. 350). The purpose of this study is to identify outcomes of state and community level programs initiated by the National Family Caregiver Support Program (NFCSP) that serves informal grandparent caregivers.
National Family Caregiving Support Program
The NFCSP is a federal law enacted in 2000 as part of the Older Americans Act. The law provides funding for community and state level programs serving two types of caregivers – family caregivers of individuals ages 60 and older; and grandparents (over age 60) raising children. The NFCSP has established five categories of support for the two types of caregivers. Those five categories of support are:
1. Information to caregivers about available services.
2. Assistance to caregivers in gaining access to services.
3. Individual counseling, organization of support groups, and training caregivers to assist them in making decisions and solving problems related to their caregiving roles.
4. Respite care to enable caregivers to be temporarily relieved from their caregiving responsibilities.
5. Supplemental services to complement the care provided by caregivers.
NFCSP Program Requirements and Funding
The NFCSP initially required that grandparent caregivers live with grandchild (ren) on a full-time basis without the help of parents and that these living arrangements were formally appointed by the foster care or child welfare system. Congress appropriates more than $150 million/year in funding for the NFCSP. The money is distributed to states to allocate funds to the Area Agencies on Aging (AAAs). The AAAs provide the support services either directly to caregivers or to programs that assist these caregivers. Ten percent of the funds appropriated for the NFCSP is used to provide support services to relative caregivers raising children within the five categories.
Amendment to NFCSP for Including Informal Grandparent Caregivers
In 2003, Generations United (GU)[6] played a significant role in amending the NFCSP. GU of Washington, DC is a nonprofit organization with a mission to promote intergenerational public policies, strategies, and programs. Founded in 1986 through collaboration efforts of the Child Welfare League of America, the National Council on Aging, the Children’s Defense Fund, and AARP, one of its initiatives is the National Center on Grandparents and Other Relatives Raising Children. The center is one of the eleven national organizations that receives grant funds from Administration on Aging (AoA) as a project to support the implementation of the NFCSP. In 2003, GU conducted surveys with the support of AoA, the National Association of Area Agencies on Aging (n4a), the Brookdale Foundation, and the National Association of State Units on Aging (NASUA) to determine training and technical assistance needs of programs serving relatives raising children. GU used the survey results to help organizations tailor training and technical assistance they provide to relatives raising children. Emerging from the results was reports of increase of grandparents informally raising grandchildren that organizations were not trained to assist. GU submitted recommendations along with new definitions to include relative caregivers who are informally raising children. The NFCSP responded by including informal caregivers among those eligible for the five categories of supportive services and lowering the age to 55 in 2006.
Program Initiatives for Informal Grandparent Caregivers
Although funding is limited, the NFCSP is a critical first step in assisting informal grandparent caregivers. While all states use the NFCSP to assist the two types of family caregivers (relatives ages 55 and older caring for the elderly and relatives ages 55 and older caring for children), only few known programs serving informal grandparent caregivers have emerged across the U.S. Those states, funded by the NFCSP, where specific services are provided to informal grandparent caregivers reported are Delaware, Illinois, Kansas, Michigan, Tennessee, Washington, Virginia, Oklahoma, Oregon, California, Connecticut, Maryland, Wisconsin, and Florida (Generations United, 2014). It is difficult to list every program in these states due to services being offered in multiple hospitals, mental health facilities, public facilities, and nonprofit organizations without specific program names. This also makes it difficult for researchers to identify states that offer services to informal grandparent caregivers but are not listed above. Known programs funded by the NFCSP serving informal grandparent caregivers under the five categories of support services are:
1. Information: Washington State Unit on Aging, Grandparents Raising Grandchildren Program of East Central Illinois AAA, Relatives as Parents Program (RAPP), Grandparents Raising and Nurturing Dependent Children (GRAND), Grandparents Raising Grandchildren (GRG), and Tribal Kinship Care Programs.
2. Assistance: RAPP, GRG, Ohio Department of Aging, KinCare, AAA Big Stone Gap, and Mountain Empire Older Citizens (MEOC).
3. Counseling, Support Groups, and Training: Grandparents as Parents (GAP), Children and Family First, and MEOC.
4. Respite Care: YMCA of Delaware, Catholic Charities, Senior Volunteer Programs, Oklahoma Respite Research Network, and Washington Aging and Long Term Care.
5. Supplemental Services: Prairie State Legal Services, Grandparents Parenting Again, Senior Volunteer Programs, Mid-Willia mette Valley Senior Services Agencies, Upper Cumberland Relative Caregiver Program, MEOC, and Tribal Kinship Care Programs.
The programs listed above range from national, state, and community levels. Some of these programs are considered as multi-component programs that provide innovative services to meet the interrelated needs of informal grandparent caregivers. The multi-component programs are those that are repeated throughout the five categories of support services.
Background and Significance of Grandparents Raising Grandchildren
Nearly 5.8 million grandparents are living in households with grandchildren ages 18 and younger. More than 2.5 million of these grandparents are the primary caregivers for these children, with the responsibility of meeting their basic needs (US Census Bureau, 2000). Grandparent caregivers over the age of 55 are usually raising children informally. This means that they are more likely to encounter difficulty accessing services on behalf of grandchildren without formal documents. Services may include: health insurance, housing, support services, and school enrollment. Moreover, grandparents possess their own share of stressors such as physical/emotional health, role loss, social isolation, and financial strain [2,5-7].
Informal vs. Formal Kinship Caregivers
A myriad of definitions are used when referring to informal and formal kinship caregivers. This can create confusion between stakeholders, researchers, and practitioners when planning and implementing programs. “Demarcating the boundaries of informal and formal kinship care and establishing the appropriate policies and programs for regulating, supporting, and sustaining these alternative care systems remain as enduring challenges for state and national programs and practice” [8](P. 350). When considering relatives raising children as kinship caregivers and kinship foster caregivers, understanding the various use of definitions may help social workers and decision-makers advance policies and programs to meet specific needs of informal and formal kinship caregivers [3]. As an attempt to help clarify the differences of definitions used for informal and formal caregivers, Kinship Caregiver Definitions Table 1 was created.
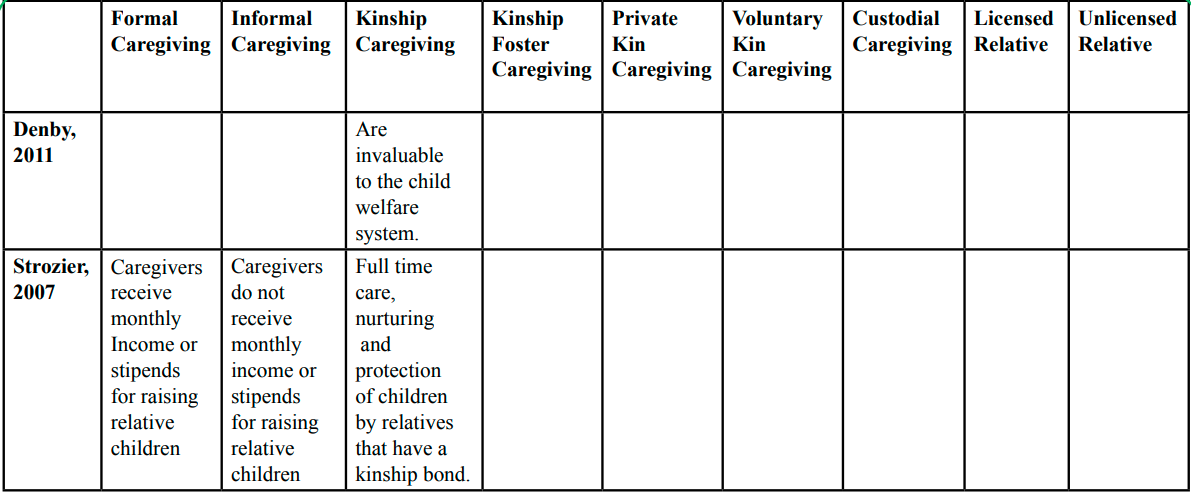
Table 1 : Kinship Caregiver Definitions
Informal Caregivers
Kinship caregiving is defined as the informal care of children (usually grandparents and other relatives) due to parental hardship or absence [9]. Although the number of children in kinship care has increased dramatically over the past few decades, research suggested that kinship caregivers receive less support, resources, and training versus kinship foster caregivers [10-13]. Strozier [14] and Dorch, et. al., [15] defined informal caregivers as those raising children with no financial support, no legal representation, and no involvement with the child welfare system. The Child Welfare Information Gateway [16] defined kinship caregiving as the full-time care and protection of children by relatives. Kinship care is also defined as the full-time nurturing of children who are separated from their parents by relatives, member of their tribes, step-parents, god-parents or other adults who have a kinship bond with a child [8,17]. The NFSCP defined informal kinship caregivers as grandparents related by blood or marriage, who are 55 years of age and older, and care for a child on a full-time basis. More specifically, the NFSCP defined that informal grandparent caregivers are eligible for services if he or she lives with a grandchild and is the primary caregiver of the child because the biological parents are unable to serve as primary caregivers [6].
Grandparents may be unwilling to take measures with the child welfare system that might result in conflict between family members. Measures may include confronting or suing their children and/or formally adopting or becoming legal guardians of their grandchildren [6]. Such avoidance can lead to needs unmet personal needs without formal support. With the ongoing demands of rearing children, grandparent caregivers reported feeling socially isolated and financially burdened [18]. Additionally, they reported the lack of information and access regarding support services, programs, benefits, and policies [19].
While grandparent caregivers are also of younger age, those that are ages 55 and older tend to have specific barriers when raising children on limited resources [20]. In previous studies, older relatives assuming the role of caregiving for children reported a variety of stressors. Common stressors among older grandparent caregivers include fatigue, limited social outlets, guilt, lack of time and privacy, limited community support, and legal issues [21]. For the older grandparent caregivers, having a child in the home can create strain on family resources and place immense demands on grandparents’ time [5]. More than two-thirds of older grandparent caregivers also experience chronic health conditions and, as a result are likely to have high depression levels [5,22].
Formal Caregivers
Kinship foster care is often referred to as formal when training and licensure processes are involved for the caregivers. Monthly payments assist in defraying the cost of caring for the child, and formal support services are provided [16]. Formal arrangements occur when the federal government provides payments from Title IV-E funds to foster parents and licensed relatives who care for abused and neglected children [15]. Fuentes, et. al [23] defined kinship foster caregivers as those that receive social support for raising relative children in foster care placements. Other forms of kinship foster care, or formal kinship care, are defined by relatives that obtain legal guardianship or custody of a child.
Theoretical Perspectives
Human service programs are essentially created to solve specific social problems. Social problems should be clearly stated in a way that does not predetermine how the problem will be solved [24]. To help mediate this process, outcomes are usually predicted when planning programs to determine a means to an end. Outcomes are desired changes in clients or communities associated with program activities [25]. Changes are usually the result of what a program has achieved [26]. At some point, agencies should conduct a program evaluation to show accountability through the process of measurement to stakeholders involved. This means that program evaluation results should highlight actual outcomes vs. predicted outcomes of clients to show the overall impact of the program. McDavid & Hawthorne [26] defined program evaluation as a systematic process for gathering and interpreting information to answer questions about a program. The problem with previous programs serving grandparent caregivers is the limited reports of outcomes for clients. Due to the complex needs of grandparent caregivers, agencies should consider using macro and micro lenses to predict and measure program outcomes. This study uses micro and macro perspectives of rational decision making, symbolic interaction, and the agency theory when determining program outcomes.
Rational Decision-Making Model
From a macro perspective, the rational model is a decision-making process that is helpful in planning, implementing, and evaluating programs [27]. The theory is one that uses a step-by-step analysis to achieve a means to an end. The rational decision-making model suggests the determination, clarification, weighting, and specification of goals, objectives, and values [28]. The model also suggests the importance of considering how decision-makers within these community and state-level programs measure success, gather feedback, and evaluate grandparent caregiver programs. Vining and Weimer [29] explained that the theory consists of two important factors: (1) analysis of the problem and (2) analysis of the solution. An analysis of the problem includes understanding the problem, explaining relevant goals, and choosing a solution method. The solution analysis consists of selecting impact categories for goals, generating policy alternatives, predicting the impact of each alternative, assigning a value to the predicted impacts by using qualitative or quantitative measures, and making recommendations. When planning programs for informal grandparent caregivers, decision-makers should have a plan in place to meet their specific needs. This perspective is helpful in identifying the increase in numbers of informal grandparents and making clear program goals to meet their needs.
The rational approach of decision-making has its share of flaws in theory and practice [28]. It can be viewed as a “one size fits all” model when grandparent caregivers have different needs based such variables as geographical locations, and age groups. More specifically, the model is criticized intellectually, politically, and philosophically. This “one size fits all” limitation is characterized by human errors and the lack of future projections. Humans are not always rational and are limited only by what they experience or learn. Choices are often made in conflict with the environment between those with levels of power within organizations and the government. Therefore, when using this model, one person of power can make the decisions for all within a community, state, or a nation. This can result in producing cookie cutter or irrelevant services for informal grandparent caregivers which can clearly have different needs.
Symbolic Interaction
To consider the specific and various needs of grandparent caregivers while making future projections, a micro perspective should be used. Symbolic interaction was developed between philosophical, psychological, and sociological disciplines in the late 1800s by George Herbert Mead. The term, symbolic interaction, was coined by Mead’s student, Herbert Blumer [30]. The theory uses a micro lens to speculate on society by focusing on a small-scale viewpoint of interaction of individuals [31]. Symbolic interaction helps practitioners to understand a phenomenon by examining a population to create a connection with others in society for change and social order. Symbolic interaction assumes that nature and change of human development concludes: (1) that people are social beings that interact with one another based on shared meanings and symbols; (2) that human interaction is symbolic interaction; (3) that the ability to think is impossible without language; and (4) that an individual’s personality is derived from the social structure and social processes by which he or she develops a self-conception [31]. When using symbolic interactionism in the context of grandparent caregivers, decision-makers can extract data from case studies and focus groups usually administered by practitioners to determine specific needs based on geographical locations, age groups, and other criteria. Furthermore, the theory can help decision-makers predict the future by exploring specific meanings of needs from grandparent caregivers and by understanding that these needs are likely to change. Symbolic interactionism has been utilized in both qualitative and quantitative methods. One limitation of the theory is that it is often considered as scientifically insufficient and judged as inadequate in providing a subjective description of a phenomenon.
Agency Theory
While the rational decision-making model considers all kinship caregivers and symbolic interaction breaks down the specific population of grandparent caregivers based on demographics, the agency theory examines more closely how one party (grandparent) acts on behalf of another (grandchild) [32]. The agency theory provides a deeper examination of the population in promotion of a gift relationship [33]. The gift relationship, in benefit to grandparent caregivers and grandchildren, is known as reciprocity [33,34]. The gift relationship is compared to the agency relationship as guided by the agency theory. The framework of the agency theory suggests that the grandparent caregiver (the agent) is delegated the discretion to act on behalf of the interest of the grandchildren (principal). A dilemma in agency relationships is whether agents will continue to act on the best interest of their principal or defects from these expectations at the principal’s expense [8]. Within the social science context, a common set of organizational principals to minimize agency risks and to resolve the social dilemma as stated above are classified into four general types of alternative care for children: (1) affine principal, caregiving responsibilities are delegated to a child’s extended family; (2) hierarchical principal, caregivers are granted authority over the person and property of the child to whom they owe duties of support, care, and education; (3) fiduciary principal, caregiving responsibilities are delegated to agents that can be counted on to look after children with the utmost integrity; and (4) contractual principal, where agents are screened, selected, licensed, and compensated for caregiving.
Specifically, this study focuses on the affine principle of the agency theory. Affine relationships are cultivated when family members volunteer or are appointed by the family as caregivers when parents can no longer care for their children. Resources are shared in a communal manner within the family in which members give to and take freely without accounting of how much one contributes or consumes [8]. Moreover, affine relationships are informal caregiving relationships that excludes the involvement of the child welfare system. Affine relationships consist of intergenerational households (with grandparent/grandchild) or multigenerational households (with grandparent, parent, and grandchild). The affine principal suggests that the parent may or may not be involved with the child in kinship care. The phenomenon of informal kinship caregiving will continue to expand in the U.S resulting in the need for social service researchers to delve more deeply into affine foundations of the resilience of extended family networks.
Research Questions
The purpose of this study is to identify reported outcomes of state and community level programs initiated by the National Family Caregiver Support Program (NFCSP) that support informal grandparent caregivers. Using the concepts as generated from the rational decision-making model, symbolic interaction, and agency theory, research questions consist of the following:
1. Rational Decision-Making Model: What needs of all informal grandparent caregivers should programs address? What are the outcomes of these program services?
2. Symbolic Interaction: How are programs meeting the needs of informal grandparent caregivers from a cultural perspective?
3. Agency Theory: Does the placement of grandchildren with grandparent caregivers create better outcomes with or without the parent present in the household?
Methods
Systematic reviews represent a scientific synthesis of research articles and should have inclusion and exclusion criteria that are rigorously and transparently reported a priori [35]. This systematic review is designed on the standards as established by the PRISMA group [36]. The reviewer evaluated research that described outcomes for programs serving informal grandparent caregivers under the NFCSP. Multiple electronic databases (Google Scholar, Social Services Abstracts, Age Line, EBSCO Host, Social Work Abstracts, and ProQuest Dissertations and Theses) were searched for published, peer reviewed articles and dissertations evaluating services/ interventions for informal grandparent caregivers. The intentional search strategy was conducted using the following keywords and connected phrases to yield research reports on programs specifically related to all grandparent caregivers: programs for grandparents raising grandchildren; national family caregiver support program AND “grandparent”; grandparent programs; grandparent caregiver programs; and National Family Caregiver Support Program AND “informal grandparent”. This process yielded more than one million studies (exact results can be provided by the reviewer) due to the multitude of results from google scholar. To help mediate the high number of results in google scholar, the first ten pages of each search result were manually reviewed and evaluated for duplicates in the six other databases. The manual review consisted of the use of the search tool using authors’ names. Duplicates of articles in google scholar which were also found in other databases were omitted in the overall totals. Database Results Table 2 1 provide specifics in the number of articles found in each database. A detailed list of duplicate articles can be provided by the reviewer if needed.

Table 2 : Database Results
Title Evaluation
Although the evaluation of titles was not the sole strategy for this study, a review of titles assisted in narrowing down selected articles. The rationale for this methodology of evaluation assisted in the identification of interest and to conduct a preliminary evaluation before and after reading the articles [37]. The specific criteria used when evaluating titles for this study were based on the following questions: (1) does the title identify grandparent caregivers? (2) if there were variables, were the variables referred to in the title? (3) does the title contain jargon or acronyms (NFCSP)? (4) is the title sufficiently specific?
Abstract Evaluation
Evaluation of abstracts also assisted in the identification of articles of interest. A preliminary evaluation of each abstract was conducted to make subjective decisions about how much weight to each element would include. When reviewing abstracts, several characteristics were evaluated: (1) was the purpose of the study clearly implied? (2) were there highlights of the research methodology? (3) were highlights of the results described? and (4) were references made for future implications?
Other Evaluation Strategies
Intervention strategies and methodologies were also evaluated and critiqued in the process. When reviewing articles for this study, a challenge with extracting data on outcomes of the NFCSP was the high volume of publications outside of empirical research such as program reports and resource guides. Due to high volume of program reports and resource guides for the NFCSP, these were also evaluated for inclusion. The evaluation process consisted of a review of whether outcomes of services were reported. Lastly, reference lists of reviewed studies were also evaluated when needed for possible inclusion.
Inclusion Criteria
With the idea in mind of the inception of the NFCSP in 2000, the reviewer searched for articles dated 2000 to 2017. Inclusion criteria consisted of peer-reviewed publications and dissertations/theses dated from 2000 to 2017. When reviewing articles for this study, a challenge with extracting data on outcomes of the NFCSP was the high volume of publications outside of empirical research such as program reports and resource guides. These types of publications were more descriptive of the program and most did not provide much information on grandparent outcomes. However, those that fit the inclusion criteria were evaluated.
A total of 12,800 were found in initial searches resulting in 7 studies meeting the final inclusion criteria after evaluation. Four of the included publications are empirical articles, one study was retrieved from dissertations and theses database, one was a literature review, and the final study was a program guide. See PRISMA Standard Flow Chart Figure 1 for a detailed description of the retrieval process using the PRISMA format.
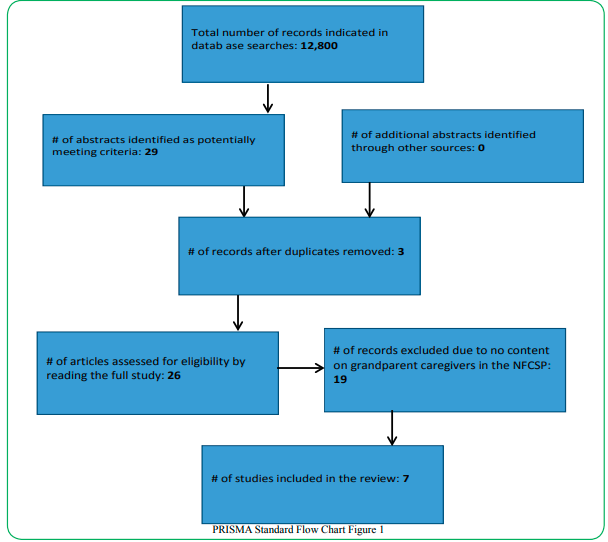
Figure 1: PRISMA Standard Flow Chart
Results
Study Selection
A total of 29 studies were considered for this review based on the evaluation criteria as mentioned in the methods section. Only 26 of those studies were evaluated after three duplications were removed. Of the 26 studies considered for this review, 12 were program guides, 4 were resource guides, and 8 were empirical studies, and 2 were dissertations. Of the 26 studies identified for the review, 19 did not meet the inclusion criteria due to the lack of reports of outcomes for grandparent caregivers. Therefore, 7 studies were selected for this systematic review. Outcomes reported in this systematic review are:
• Reduced isolation
• Increased connection to resources
• Independence/empowerment
• Reduced stress
• Lower levels of burden
• Increased well-being
• Intergenerational reciprocity
Table 4 provides an overview of the included articles:
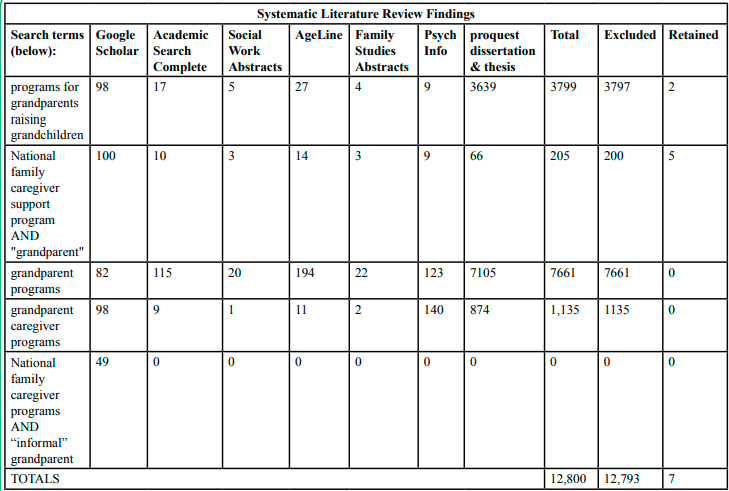
Table 4 : Included Articles
Description of Included Studies
Littlewood [38] conducted an exploratory study on the Grandfamilies Outcome Workgroup (GrOW) to examine concepts, goals, outcomes, and measures of the program. “For grandparents raising grandchildren, support groups continue to be the most widely available service but there is no best practice or recommended approach to evaluating this intervention” [38] (p. 32). The purpose of this study was in response to need of best practices and attempts to make recommendations for support groups. Participants of the study included members of GrOW representing five states (CA, NY, FL, CN, and AZ). The data collection process took place over several months where each group leader took several hours to complete and inventory survey. Results of the inventory revealed several outcomes for grandparent caregivers. Outcomes included reduced stress, increased connection to resources and social support, and reduced stress. It is questionable as to how the validity of these outcomes were measured since no specific data was reported. The study revealed several areas examined within support groups such as structure, facilitation, and funding but failed to provide results from inventory surveys. Littlewood listed promising measures for each outcome but failed to detailed meanings of the promising measures.
Conway, et. al. [39] conducted a secondary analysis of a cross-sectional survey to report the uses of resources and services for grandparent caregivers. The study also examined levels of burdens and factors that mediate their relationships. The study was conducted at the National Resource Center for Native American Aging in the North Dakota Data Center where NFCSP services are provided. The overall outcome reported for grandparent caregivers as results of services offered is lower levels of burden. However, the levels of burden varied by reasons of caring for a child. Reasons included, family violence, having a grandchild with a disability, having a stressed relationship with the parent, and the use of governmental services. It is not clear in the study on how the use of governmental services increase or decrease burden. However, it is speculated that governmental resources may help to defray the cost of everyday living expenses, thus, may help to decrease caregiver burden. It was reported that grandparents were asked if they use TANF and/ or other community resources. Level of burden was measured using the Zarit Burden Scale. The study builds on current research using established data collection instruments from the NFCSP to address two questions:
1. What is the relationship between grandparent caregivers use of resources and services and their levels of burden?
2. How do other factors (characteristics of the child and grandparent) influence level of burden and use of resources and services?
A convenience sample of 247 grandparent caregivers were used. Grandparent caregivers were younger than 65 years old and 57% were American Indians. Fifty-two percent were married or living with a partner, and 49% had an annual household income of $20k or less before taxes. Outcomes included lower levels of burden if they used financial or other resources. The study failed to provide a control group or lack of pretest/posttest to compare results of caregiver burden, thus, raising questions as to how caregiver burden was decreased. There is also confusion on the ages of grandparent caregivers in this study due to the methods and discussion sections indicating different age numbers. Finally, with the sample being a convenience sample, it may not have been representative of the population of grandparent caregivers in rural regions.
Whittier, et. al. [40] examined the range of existing sources for family caregivers from the perspective of the AAAs. In scope, the study examined the extent and adequacy of resources available in California corresponding to each of the five categories of service of the NFCSP. Several research methods were used to identify existing services and service gaps consisting of survey questionnaires to 33 AAAs. Of the 33 surveys sent to administrators and program directors, 24 (73%) responses were received. One of the biggest difficulties that caregivers encounter is the lack of time to do what he or she wants or needs. A reported outcome of this study stems from respite care services. Family caregivers experienced reduced amounts of stress due to opportunities of free time for personal activities and self-care. However, this study included the two types of caregivers (family caregivers of individuals (ages 60 and older); and grandparents (over age 60) raising grandchildren) as a whole and did not differentiate outcomes between the two. Therefore, no specific outcomes for grandparent caregivers were reported.
Kaplan & Perez-Porter [41] conducted a descriptive study of web programs, support systems, organizational structures, and social policies that can help households with grandparents and grandchildren thrive. The authors use the term “grand families” in reference to households with grandparents and grandchildren. The study revealed that support groups is most used of grandfamilies as compared to the other 4 categories of services. Support services for grandparent caregivers help reduce emotional stress by providing instrumental support. The study provides more detail of specific support groups that other included studies did not provide. With this study focusing on grand families, it reports increase of intergenerational reciprocity. One support group discussed is the Kinship Family Retreats which promotes intergenerational reciprocity. Kinship Family Retreats, created by Penn State’s Cooperative Extension provide stress-free settings for grandfamilies to enjoy quality family time. The retreat setting takes place outside of the social service settings. Grand families report the appreciation of not having to worry about treatment, therapy, or referrals. They are simply participating in these retreats to spend quality time with family. Planning for intergenerational reciprocity does not necessarily require structured planning. It creates a time set aside to bring the entire family together for joint activities involving cooking, storytelling, art, and travel. The study also provided detail on agency collaboration initiatives for building capacity of human service agencies. Some of these interagency collaboration initiatives fill service delivery gaps across children welfare and aging service system. These initiatives also stand as positive outcomes for grandparent caregivers. Kaplan and Perez-Porter [41] used a strengths-based approach to establish a continuum of support for grand families.
A common trend when systematically reviewing literature on programs serving grandparent caregivers within the NFCSP is the repeated reports of successful programs in the state of California. Minkler & Odierna [7] conducted a study on model programs within the NFCSP that serve grandparent caregivers. The study initially provided characteristics of grandparent caregivers which consisted of the increase of the population and special challenges they encounter. When providing characteristics, the authors noted statewide diversity as suggested by the symbolic interaction theory. Because of the diversity between grandparent caregivers among the state, the authors highlighted special challenges and provided model program details that meet their needs. Special challenges are cohesive with the challenges previously mentioned in this review. Those challenges are physical/emotional health, role loss, social isolation, and financial strain [2,5-7]. The study concluded with implications for recommendations for the aging network:
• Start where the people are before deciding on a new program or activity: Grandparent caregivers are articulate spokesperson of their own needs regarding themselves, the children, and extended families.
• Identify and address the special cultural, linguistic, and other needs and concerns of diverse groups of grandparent caregivers: The phenomenon of grandparent caregiving spans across all ethnicities, it is highest among African Americans and Hispanics. Special attention to these cultures is important so that programs can be tailored to their specific needs.
• Search out and develop creative partnerships: It is important for organizations to seek opportunities of agency collaboration to increase services to grandparent caregivers.
Additionally, a breakdown of formal statewide programs was provided with summaries and contact information.
Description of Outcomes Within the Five Categories of Service
When reviewing articles for this study, a challenge with extracting data on outcomes of the NFCSP was the high volume of publications outside of empirical research such as program reports, literature reviews, and resource guides. However, those that fit the inclusion criteria were evaluated for use in this study. In result, two non-empirical reports were used. Without the use of methodology and interventions, the two non-empirical are discussed in terms of the five categories of services. Generations United [6] is a program guide that describes the NFSCP in detail. It highlights specific problems encountered by grandparent caregivers and provides recommendations for program improvement. The most common problems encountered by grandparent caregivers are physical/emotional health, role loss, social isolation, and financial strain [5,6,2,7]. Further elaboration on these common problems are provided in the discussion section. The Hayslip & Kaminski [2] article is a review of literature with recommendations for improving services offered to grandparent caregivers. Outcomes from this article are also reported within the five categories of services.
Information: This category of service connects grandparent caregivers to available community resources. The intended outcome of providing information to grandparent caregivers is the increased likelihood to utilize more services available to them. GU [6] revealed several outcomes related to spreading information to grandparent caregivers. From the use of physical resource manuals and handbooks, older caregivers feel more comfortable and empowered versus using electronic methods. Manuals provide valuable information on parenting, budgeting, referring to local support groups, and other valuable resources. This method allows grandparent caregivers to feel safe and provides a clearer understanding of the resources available to them. The Connecticut State Department on Aging [42] use this approach to allow elderly caregivers to help themselves. The Maryland State Department on Aging provides a 108-page manual with contacts for various community services.
Assistance: Grandparent caregivers experience barriers that may prevent the access of appropriate and suitable services. This category offers a level of independence by providing caregivers with social capital that can help make the caregiving process more bearable. GU [6] reported resources such as community support groups and professional liaisons to help provide technical support for basic computer skills and other needed assistance when caring for children. GU also reported the benefits that grandchildren can offer to grandparents especially with technological assistance. Training programs offered by the NFCSP often use a reciprocal approach when assisting grandparent caregivers with technology. Other provisions are transportation, legal help, and access to recreational clubs for personal improvement. Haysilp & Kiminski [2] noted an increase in well-being for informal grandparent caregivers when such assistance is made available.
Support Services: Supportive services promote outcomes of alleviated stress and improved health for caregivers [2]. Examples of support services as provided by the NFCSP are counseling, parenting classes, budgeting classes, and other trainings to assist grandparent caregivers. GU [6] reported various state and community efforts that provide support. One program offered at the state level is Family Circles that provide education and support groups to build reciprocity among grandparents and grandchildren.
Respite Care: Respite care include services that provides caregivers with temporary relief from caring for children. These services are provided in recreation centers like the YMCA where children can be left to participate in various activities. Respite care for grandparents are also available through volunteer and in-home programs. AAAs in various states collaborate with local parks and recreation providers, and other organizations such as Easter Seals and Camp Fire to pay for day camps for children who live with grandparents ages 55 and older. Outcomes from respite services provide an increase of well-being for grandparent caregivers allowing them the free time for self-care [2].
Supplemental Services: Supplemental services complement the care provided by caregivers. Supplemental services also help to promote intergenerational reciprocity where both grandparents and grandparents are strengthened to work more in harmony with one another. These services can range from federal programs to state and community programs. The services are provided for all members of the household and include healthcare, legal services, financial assistance from federal and state programs, and basic needs assistance from community programs.
Intergenerational Reciprocity
The exchange of reciprocal support promotes well-being of those involved in households headed by grandparents when needs are met for grandparent caregivers [43,44]. Simply stated, intergenerational reciprocity is the extent to which generations can strengthen one another, especially when living in the same household. Intergenerational reciprocity is also defined as a pattern of social behaviors which create a motive for generations to exchange support [43,45]. In some special cases, grandparent caregivers can look to grandchildren for help. Using the theoretical perspectives of decision-making, symbolic interaction, and agency theory; an overarching theme that all studies presented in this review was the outcome of intergenerational reciprocity for both grandparents and grandchildren.
Discussion
The purpose of this study was to identify outcomes of state and community level programs initiated by the National Family Caregiver Support Program (NFCSP) that serves informal grandparent caregivers. This study provided information on community and state level programs for informal grandparent caregivers, ages 55 and older as defined by the NFSCP. In reviewing literature, the reviewer used macro and micro perspectives of the rational decision-making model, symbolic interaction, and agency model to identify specific needs of informal grandparent caregivers, to identify program outcomes for this population, and to make recommendations for future research and practice. The rational decision-making model consisted of a clear-cut method of diagnosing, selecting an action plan, and implementing the plan [27]. When diagnosing problems for grandparent caregivers, the decision-maker should evaluate its most salient features and avoid using a conditioned response based on past experiences. In other words, when a researcher or practitioner collects data on informal grandparent caregivers in one state or community, decision-makers should consider that the needs can be different from those in other states and communities. The second step in decision-making was to choose an action plan that works best for the population served. For informal grandparent caregivers, the concept was applied in the various forms of programs offered in different states and communities. However, the decision-making process stopped at evaluation and did not fully consider future projections. Symbolic interaction was applied to help take things a step farther in making future projections by analyzing populations within society by addressing subjective meanings that people impose on objects, events, and behaviors. Symbolic interaction helped decision-makers notice gaps in services and trends in needs. When using the context of symbolic interaction in kinship care, the increase of unmet needs for informal grandparent caregivers were noted. The agency model examined more closely how one party (grandparent) acts on behalf of another (grandchild) [32]. The model defined the grandparent as the agent and the grandchild as the principal. The agency model prompted that intergenerational reciprocity where generations can work together to strengthen one another was promoted when the affine principal was applied. However, the question remains: does placement of grandchildren with grandparent caregivers create better outcomes with or without the parent in the household? None of the studies reviewed for this project fulfilled this question. The purpose of this study was to identify outcomes of state and community level programs initiated by the National Family Caregiver Support Program (NFCSP) that serve informal grandparent caregivers. Outcomes reported in this systematic review were:
• Reduced isolation
• Increased connection to resources
• Independence/empowerment
• Reduced stress
• Lower levels of burden
• Increased well-being
• Intergenerational reciprocity
NFCSP programs for informal grandparent caregivers are currently implemented in the states of Delaware, Illinois, Kansas, Michigan, Tennessee, Washington, Virginia, Oklahoma, Oregon, California, Connecticut, Maryland, Wisconsin, and Florida (Generations United, 2014). These programs are tailored to serve the specific needs of informal grandparent caregivers with the context of the five categories of support as defined by the NFCSP. When determining specific needs of informal grandparent caregivers, the stressors they encounter should be considered. Research reported several stressors such as physical/emotional health, role loss, social isolation, and financial strain [2,5-7]. When these stressors are addressed then reciprocity can be established.
Limitations
There were several limitations of this study. One limitation was the minimal number of reports revealing funding sources of programs serving informal grandparent caregivers. It was difficult to fully identify all NFCSP programs serving informal grandparent caregivers due to unmarked programs providing bundle services in hospitals, mental health facilities, recreation facilities, and other agencies. Because these types of programs served more than one type of caregiver, they do not fully report outcomes of services for informal grandparent caregivers. Another limitation is that there is a 13-year gap of time with sparse empirical research evaluating specific NFCSP programs serving informal grandparent caregivers.
Implications for Social Work Practice
This study implies that more outcome evaluation reports should be published on NFCSP programs serving informal caregivers which might provide stronger evidence for future practice. An updated comprehensive study that considers the diverse needs of informal grandparent caregivers would be helpful in tailoring future program services that will serve this population. Empirical and evaluative research should also be conducted on a regular basis to make future projections regarding the needs of grandparent caregivers.
Conclusion
The NFCSP is a significant first step in assisting this population and is an important federal program that provides much needed funding to AAAs in support of grandparent raising grandchildren. Currently, about $150 million is allocated toward the federal program with ten percent of those funds appropriated to grandparents informally raising grandchildren.
Conflict of interest:
The authors declare no conflict of interest.
References
Hayslip, B. Jr., Fruhauf, C.A., Dolbin-MacNab, M.L. (2019). Grandparents Raising Grandchildren: What Have We Learned Over the Past Decade?. Gerontologist.17;59(3):e152-e163. doi: 10.1093/geront/gnx106.View
Hayslip, B. Jr., Kaminski, P.L. (2005). Grandparents raising their grandchildren: a review of the literature and suggestions for practice. Gerontologist. 45(2):262-9. doi: 10.1093/ geront/45.2.262.View
Ivey, D. L. (2018). an exploration of national family caregiver support programs serving informal grandparent caregivers: A descriptive phenomenology approach. ProquestView
Montoro-Rodriguez, J., Hayslip, B., Ramsey, J., & Jooste, J. L. (2021). The utility of solution-oriented strategies to support grandparents raising grandchildren. Journal of Aging and Health, 33(9), 647-660. https://doi.org/10.1177/08982643211004817View
Butler, F., & Zakari, N. (2005). Grandparents parenting grandchildren: assessing health status, parental stress, and social supports. Journal of Gerontological Nursing, 31(3), 43-54.View
Generations United. (2003). A guide to the national family caregiver support program and its inclusion of grandparents and other relatives raising children.View
Minkler, M. & Odierna, D. (2001). California’s grandparents raising grandchildren: What the aging network needs to know as it implements the national family caregiver support program. The center for the advanced study of aging services. University of California, Berkley.
Testa, B. (2013). ChemInform Abstract: Organic Stereochemistry. Part 3. Other Stereogenic Elements: Axes of Chirality, Planes of Chirality, Helicity, and (E,Z)- Diastereoisomerism, ChemInform, 10.1002/chin.201330225View
Lane, G. W., Podgorski, C. A., Noronha, D. O., & King, D. (2012). "the hidden caregiver": Kinship caregivers and lessons learned from dementia family caregiving. Clinical Gerontologist, 35(2),195-203.doi:10.1080/07317115.2011.641708View
Berrick, J. D., Barth, R. P., & Needell, B. (1994). A comparison of kinship foster homes and foster family homes: implications for kinship foster care as family preservation. Children and Youth Services Review, 16(1–2), 33–63.View
Gebel, T. J. (1996). Kinship care and nonrelative family foster care: a comparison of caregiver attributes and attitudes. Child Welfare, 75(1), 5–18.View
Scannapieco, M., Hegar, R. L., & McAlpine, C. (1997). Kinship care and foster care: A comparison of characteristics and outcomes. Families in Society, 78(5), 480-488. doi:10.1606/1044-3894.817.View
Brooks, D., & Barth, R. P. (1998). Characteristics and outcomes of drug-exposed and non-drug-exposed children in kinship and non-relative foster care. Children and Youth Services Review, 20(6), 475– 501.View
Strozier, A., Kerry, K. (2007). Capturing caregiver data: An examination of kinship care custodial arrangements. Children and Youth Services Review, 29(2), 226 – 246.View
Dorch, E., Mumpower, J., & Jochnowitz, L. (2008). The cost and benefits of cash and services to kinship caregivers. Social Work in Public Health, 23(6), 55-73. doi:10.1080/19371910802059601.View
Child Welfare Information Gateway. (2016). About kinship care. Retrieved from https://www.childwelfare.gov/topics/ outofhome/kinship/about/.
Child Welfare League of America. (1994). Kindship care: A natural bridge. Washington, DC: CWLA Press.View
Kelley, S., Sipe, T., & Whitley, D. (2001). Grandparents raising grandchildren: Are they at increased risk of health problems? Health and Social Work Journal, 26(2), p.105
Campos, P., Kelley, S., & Whitley, D. (2010). Grandmothers raising grandchildren: Results of an intervention to improve health outcomes. Journal of Nursing Scholarship, 42, 379–386. doi: 10.1111/j.1547-5069.2010.01371.x.View
Geen, R. (2004). The evolution of kinship care policy and practice. Children, Family, and Foster Care, 14(10), 130 – 149.View
Madden, L. (2006). Taking It All In. Children & Libraries: The Journal of The Association For Library Service To Children, 4(1), 15-16.
Minkler, M., Roe, K., Robertson-Beckley, R. (1994). Raising grandchildren from crackcocaine households: Effects on family and friendship ties of African American women. American Journal of Orthopsychiatry, 64(1), 20-29. doi:10.1037/ h0079493.View
Fuentes-Palaez., Balsells, A., Fernandez, J., Vaquero, E., and Amoros, P. (2016). The social support in kinship foster care: A way to enhance resilience. Child and Family Social Work, 21(5), 581 – 590.View
Watson, L. & Hoefer, R. (2014). Developing nonprofit and human service leaders. Sage Publications. Thousand Oaks, CA.View
Newcomer, K., Hatry, H., & Wholey, J. (2015). Handbook of practical program evaluation. John Wiley & Sons. Hoboken, NJ.View
McDavid, J., & Hawthore, L. (2006). Program evaluation and performance measure: An introduction to practice. Sage Publications. Thousand Oaks, CA.View
Beach, L. R., & Connolly, T. (2005). The psychology of decision making: People in organizations. SAGE Publications Inc. https://doi.org/10.4135/9781452204406View
Clemons, R. S. & McBeth, M. K. (2009). Public policy praxis: A case approach for understanding policy and analysis. New York: Pearson / Longman.View
Vining, A., & Weimer, D. (2010). Foundations of public administration: policy analysis. Public Administration Review, pp. 1 – 17.
Mead, G. (1934). Mind, self, and society. University of Chicago Press. Chicago, IL.View
Robbins, S.P., Chatterjee, P., & Canda, E.R. (2012). Contemporary human behavior theory: A critical perspective for social work. Boston: Allyn and Bacon.
Shapiro, S. (2005). Agency theory. Annual review of sociology 31(1), 263-284. doi:10.1146/annurev.soc.31.041304.122159View
Testa, M.F., & Shook Slack, K. (2002). The gift of kinship foster care. Children and Youth Services Review, 24, (1/2), 79-108.View
Titmus, R. (1971). The gift relationship: From human blood to social policy. Pantheon Books. New York, NY
Torgerson, D.J., Torgerson, C.J.(2003).Avoiding Bias in Randomised Controlled Trials in Educational Research. British Journal of Educational Studies,51(1) https://doi. org/10.1111/1467-8527.t01-2-00223View
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Medicine, 6(7), e1000097. doi:10.1371/journal.pmed.1000097.View
Pyrczak, F. (2013). Evaluating research in academic journals: A practical guide to realistic evaluation. Pyrczak Publishing. Gendale, CA.View
Littlewood, K. (2014). Granfamilies Outcome Workgroup’s review of grandfamily support groups: An examination of concepts, goals, outcomes, and measures. The contemporary journal of research, practice, and policy, 1(1), 32 – 55.View
Conway, P., Boeckel, J., Shuster, L., & Wages, J. (2010). Grandparent caregivers’ use of resources and services, level of burden, and factors that mediate their relationships. Journal of intergenerational relationship, 8(2), 128 – 477, doi. 10.1080/15350771003741931.View
Whittier, S., Scharlack, A., Dal Santo, T. (2008). Availability of caregiver support services. Journal of aging and social policy. 17(1), 45 – 62. Doi 10.1300/J031v17n01_03.View
Kaplan, M., & Perez-Porter, M. (2014). Support for grandfamilies: A mosaic of intervention strategies. Journal of intergenerational relationship. 12(2), 99 – 112. View
Connecticut State Department on Aging (2016). The national family caregiving support program. Retrieved from: http:// www.ct.gov/agingservices/cwp/view.asp?a=2513&q=313064.View
Zhang, J. (2014). Elderly Chinese immigrants, intergenerational reciprocity, and quality of life. New Zealand Sociology, 29(2): 11-30.View
Antonucci, T. (1985). Social support: Theoretical advances, recent findings, and pressing issues. Social support: Theory, research, and applications. Boston, MA: Martinus Nijhoff Publishers.View
Schwarz, B., Trommsdorff, G., Zheng, G., Shi, S. (2010). Reciprocity in intergenerational support. A comparison of Chinese and German adult daughters. Journal of Family Issues, 31(2): 234-256.View