
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-158
https://doi.org/10.33790/jmhsb1100158Research Article
Suicide among South Asian Americans: A Systematic Review of Causal and Risk Factors
Susheelabai R. Srinivasa, Ph.D.1*, Sudershan Pasupuleti, Ph.D.2, & Rani Dornamraju, MSW, LMSW,QIDP3,
1*Assistant Professor, School of Social Work, The University of Texas Rio Grande Valley, United States
2Professor, School of Social Work, The University of Texas Rio Grande Valley, United States.
3Health Services Supervisor, Washtenaw County Community Mental Healthcare, MI, United States.
Corresponding Author Details: Susheelabai R. Srinivasa, Ph.D., Assistant Professor, School of Social Work, The University of Texas Rio Grande Valley, United States. E-mail: susheelabai.srinivasa@utrgv.edu
Received date: 02nd March, 2022
Accepted date: 29th March, 2022
Published date: 31th March, 2022
Citation: Srinivasa, S.R., Pasupuleti, S., & Dornamraju, R. (2022). Suicide among South Asian Americans: A Systematic Review of Causal and Risk Factors. J Ment Health Soc Behav 4(1):158.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This paper will provide an overview of suicide prevalence among South Asian Americans who constitute nearly one-third of Asian Americans and 1.7 percent of the United States population. South Asians, late 20th century immigrants, are a numerally small percentage of the population in the United States. As a distinct ethnic population despite significant diversity within, South Asians encounter unique challenges with myriad sub-cultures and struggles that make them vulnerable and underrepresented in policy and service utilization in mental health and health care due to various barriers. These conditions create vulnerability among first and subsequent generations as they go through social pressures of acculturation and integration into American society. Suicide, as a rising social concern related to health disparities research, is described with the aid of common theoretical perspectives along with causal/risk factors. Suicide rate is the highest among South Asians even among Asian-origin Americans which has higher suicide among all minority populations – Asian, African and Hispanic Americans. Success of South Asians is associated with certain hidden or unrecognized costs. Making the American dream a reality which is a strenuous journey for South Asians predisposes them at higher risk for health, mental health, substance abuse, suicidal ideation, and behavior. Systematic review of articles from three databases with focus and content on South Asian Americans was conducted and the results are presented in this article. Identified concerns and issues are addressed in the light of theoretical perspectives and evidence gathered from the systematic review and critical analysis.
Keywords: Suicide, South Asians, South Asian Americans, Suicide Risks, Disproportionality, Health Disparities, Acculturation stress, and Prevention of suicide
Introduction
Suicide is major public health concern since 12.2 million individuals entertain suicidal ideation, 3.2 million plan to commit suicide and 1.2 million attempt suicide and that result in nearly 46,000 deaths every year in the United States (Center for Disease Control [CDC], 2020). This menace has multidimensional negative impact on individuals, families, and society with staggering economic loss of $60 Billion. Except a small decline during 2019 and 2020, suicide rates increased at 30% between 2000 and 2018. It is 9th leading cause of death among 10-64 age- group and 2nd leading cause of death among 10-14- and 25-34-year age groups. According to National Institute of Mental Health [1], “suicide is defined as death caused by self-directed injurious behavior with intent to die because of the behavior. A suicide attempt is a non-fatal, self-directed, potentially injurious behavior with intent to die because of the behavior. A suicide attempt might not result in injury. Suicidal ideation refers to thinking about, considering, or planning suicide.” Franklin et.al [2] investigated suicide risk factors with metanalysis of 50 years of research.
Nearly 6.27 million people in the United States trace their ancestry and heritage to current South Asian countries. The United States Census Bureau does not include South Asians as a distinct ethnic group for the Census it lumped all Asian Americans together as one racial/ethnic group. Major ethnic groups that make up South Asian population include Asian Indians (79%), Bangladesh (3.74%), Bhutanese (.56%), Burmese (3.32%), Nepalese (3.06%), Pakistanese (9.24%) and Sri Lankans (1.07%). They constitute 1.9 per cent in the U.S. population with an aggregate population of 6,268,769 which is one-third of Asian Americans (Wikipedia, 2020). South Asian Americans represent vast diversity as they speak many different linguistic and cultural backgrounds that included but limited to Assamese, Bengali, Gujarati, Hindi, Kannada, Malayalam, Marathi, Nepali, Maldivian, Punjabi, Rajasthani, Sindhi, Simhala, Tamil, Telugu, and Urdu. Their faith traditions include many of world religions such as Buddhism, Hinduism, Jainism, Sikhism, Christianity, and Islam.
People of Indian origin is the largest group with 4,506,308 (1.3 percent of U.S. population) in 5,507,437 South Asian population. According to American Association of Suicide Prevention [3] about 46,000 people die by suicide every year in the U.S. More distressing fact is that it is the second leading of death among young people in the age range of 14-34 years, while it is the fourth leading of death for individuals between 35 and 80 years. The overall suicide rate for Asian Americans is half of the non-Hispanic white population. Though the large data indicate less concerns of suicide about South Asian population than their western counterparts, it is a recognized problem in the research studies. Suicide was the leading cause of death among South Asian Americans in the age-group of 15 to 24 years [4]. Asian American females in the grades 9-12 were 20 percent more likely to attempt suicide as compared to non-Hispanic white female students [5]. South Asian Americans Advocacy Group [6] reports about 10% of the South Asian population, constituting approximately 6 million, lives in poverty in the United States as per the Federal Guidelines for Poverty. This is contrary to population stereotype of model minority. Suicide in United States has become a reflection of the fragile and fragmented emotional state of immigrants from South Asia since they are not fully qualified as minority population. Some of the factors that affect immigrants include cultural, socioeconomic, health, and mental health [7,8].
The Census data did not specifically present statistics on the suicides among South Asians. Research literature cited high suicidal rates among South Asians. There is contradictory evidence about suicide rates in people of South Asian Americans. Most studies reported suicide rates are higher among South Asian (SA) men and women among minority ethnic groups, barring non-Hispanic whites and American Indian (Native Americans), which is contrary to the population of model minority in American population [9]. According to South Asian American Leading Together [9], highest suicide rate (20.2%) is prevalent among middle-aged adults in the age group of 45 to 54 years old; it is followed by older adults with 20.1 percent in the age group of 85 years and older. Among young adults and adolescents (15-24 years), it was 14.46 percent in 2017. South Asian women attempt suicides twice as often as males [10]. Asian refugees are identified as high-risk group for post-traumatic stress disorder (PTSD) associated with trauma experienced before, during and after immigration to the United States. One study found that 70% of Southeast Asian refugees receiving mental health care were diagnosed with PTSD. However, these PTSD rates for South Asians Americans were not clear.
Suicide: A Social Menace and Disproportionality
Suicide is a major social problem not only in American society but also world-wide where one million people die by suicide every year, that accounts for .0245 percent in the world population. In the United States, suicide accounts for 1.5 percent of aggregate deaths from all causes [11] that translates into 25 million suicidal attempts and one million deaths every year [2]. Suicide, at the rate of 14.2 per 100,000 population, took 48,344 lives in 2018 becoming the 10th leading cause of deaths among all age groups in the United States (see table 1). Suicide and self-injury attempted by 1,400,000 people costs whopping $69 Billion to society. Deaths due to suicide, along with Alzheimer's disease, remained high as leading causes of untimely premature deaths which costs heavily for society [12]. Heart disease, stroke, and deaths attributed to motor-vehicle injuries demonstrated notable declines since 2005. It is a public health problem representing mental health dimension. In addition to 575,000 Americans caused harm to themselves and were rushed to the hospitals nation-wide [9]. It is shocking to note that suicidal deaths are greater in numbers compared to deaths due to homicide, AIDS, car accidents [13]. O’Brien [14, p.15] strongly recommended that words like “kill oneself” or “die by suicide” [15] are not to be used and usage of “the word commit is more is punitive” and “successful” and “unsuccessful” are to be avoided. It is also global menace with 140 million people had suicidal ideation world-wide [15]. Table 1 presents leading causes of deaths in 2017 and 2018, in which suicide emerges as 10th leading cause.

Table 1: Age adjusted death rates of top 10 leading causes of deaths in 2017 and 2018.
From critical examination of suicide rates among different racial/ ethnic groups reveal a sublime problem of disproportionality Table 2 presents suicidal rates by age groups and racial and ethnic groups.

Table 2: Suicide incidence by age groups and race/ethnicity (48,344 suicides) 2018
From the above table Asian Americans experienced highest 6.7 percent suicides rate in 10-65 years age group and 32.5 percent in 10-24 years age group, compared to other ethnic groups. However, there are no statistics specifically for South Asian American groups. Among all racial/ethnic groups, African American ethnic group has lowest rate. According to the Center for Disease Control and Prevention [13], suicide rates were 6.59% among Asian and Pacific Islanders, 6.61% among African Americans and 13.42% among American Indians and Alaskan natives; it was highest (15.85%) among Caucasian population. White males account for 70 percent of all suicides in the United States.
Research Questions and Method
In this article, authors investigated suicide among South Asian Americans by undertaking systematic and critical review of data resources and literature with the content about this subset of U.S. population. In this investigation, the high rate of suicide in South Asian American population, in relation to other ethnic groups, was examined by exploring the linkages between disproportionality, under-representation in utilization of mental health services, lack of cultural sensitivity in providers and the factors associated adverse life events, culture, and tradition. Through this undertaking authors gained more insights into these issues and there is a dearth of scholarship focusing these ethnic groups. The results may draw the attention of scholars, policy makers, and healthcare providers in addressing the issues discussed in this article.
Search was completed involving three major databases to locate peer-reviewed articles published in English journals in the past ten years. The databases included Google Scholar, PubMed and EBSCOST. The search terms used for finding appropriate articles in these databases were “Suicide among South Asians” and “United States.” Google scholar’s initial search yielded 1,260,000 results. The search was narrowed by setting the timeframe from 2010 to 2020. The narrowed (advanced) search resulted in 1,070,000. Then the titles and abstracts were screened. Only 12 abstracts met the inclusion and exclusion criteria. All the abstracts which met the criteria were selected for full text review. Secondly, SocIndex was searched for relevant articles. This directed to EBSCOST with same search terms which generated 3,563 articles. Finally, advanced search generated around 100 articles and these titles and abstracts were screened further. From which only two articles were found meeting criteria. The full text was reviewed for the abstracts which met the criteria. Thirdly, in PubMed, only twenty-two resources were retrieved, and advanced search provided only one relevant article. The full text was reviewed for this abstract. Overall, fifteen peer-reviewed articles with content on South Asians have been clearly identified, reviewed and results are presented in this article. There is dire need for more research in area. It is an under-researched and published topical area.
Suicide among South Asians: Results of Systematic Review
South Asian immigrants after coming to the United States acculturate to the new and challenging environment. Most South Asian ethnic groups who migrated to the United States are successful as students, as employees, and as residents of their adopted home, United States, after going through a stringent immigration process [16]. South Asians come as students, non-immigrant (H1-B) workers and family and employment-based visas. This entire process of immigration is lengthy taking many years which turns out a highly stressful life event for most people. Nevertheless, the transition, acculturating themselves in the United States, is not smooth either. Immigrants during the acculturation process adjust by inculcating and assimilating many aspects of the mainstream culture. Scholars, on one hand, view immigrants based on a unidimensional approach and believe that immigrants acculturate at the cost of sacrificing their culture [17]. Furthermore, in this process, individuals experience high psychological distress and trauma if they are less acculturated to the dominant culture. For instance, immigrant students from South Asian origin expressed concerns and reported to have faced a lot of prejudice like their Asian American and Hispanics counterparts in social, educational, and occupational realms in the United States [18]. On the other hand, scholars who view with a multidimensional approach believe immigrants do not give up on their culture of origin, but they retain their culture and assimilate the components of the mainstream culture. In other words, the immigrants imbibe the dominant culture and blend the aspects of both cultures without negatively affecting themselves and having no impact on their mental health [19].
Overview of Results from the Systematic Review
Analysis of 15 articles that focused on suicides among South Asians was made from the framework of Durkheim’s ‘Le suicide [20], from excerpts by (Jones, 1897). A select review of literature is presented in table 3.
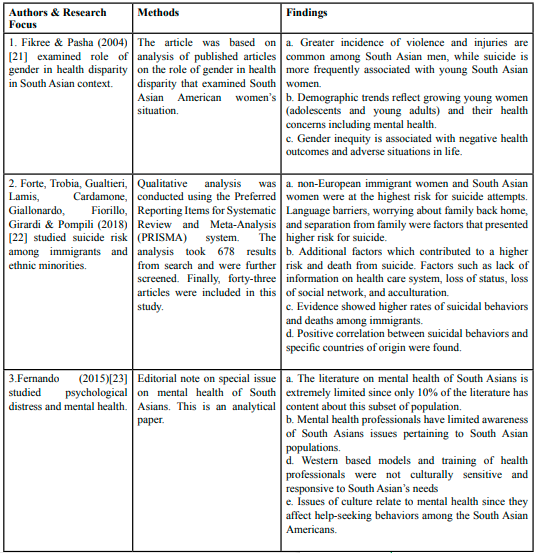
Table 3: Select research studies and findings
Emerging Themes from the Review and Risk Factors for Suicide
In this section, various causes of suicide will be discussed which include ethnic, socioeconomic, cultural, religious, legal, and mental health perspectives and the intersectionality.
The literature underscores numerous factors that are responsible for suicide. These factors include sociocultural, immigration and legal issues, economic distress, lack of family and community support, childhood adversity, personality, and cognitive issues, anticipated or real-life stresses or romantic failures, legal loss, and academic failures. In addition, health and mental health factors associated with suicide which include depression/bipolar, antisocial, conduct disorder and substance use, physical health reasons, and chronic physical health conditions, access to lethal means. Stressful life events, childhood abuse and family history are antecedents and they contribute to suicidal ideation and behaviors. Other factors are cultural and religious beliefs which play a role influencing thoughts and behaviors. Negative interpersonal relationships and social isolation were found to be significant predictors of suicide. Hopelessness and unwillingness to seek help are related to one’s cultural beliefs and values. A person’s exceptional circumstances such as being refugee or migrant in new and challenging environment could also precipitate situations leading to frustration and despair. Further, being a member of marginalized group such as prisoner and LGBTQ may also create distressing situations that form suicidal ideations and behaviors [29]. At both the individual and population levels, the suicide rate is found to correlate with cultural, social, political, and economic forces. The perceived notions or real aspects of different issues in a person’s life in the cultural, social, mental/ physical health and economic domains create pressure and distress to a person that may result in suicide [35]. In this section a review of the scope of this problem in terms of immigrants in the United States from South Asia is presented.
Cultural factors affecting help seeking behavior
Society and culture play a significant role in dictating how people respond to and view mental health and suicide. Culture influences the way in which we define and experience mental health and mental illness, our behavior to access care, help, quality of the interaction with provider in the health care system, and our response to treatment [29]. This has implication for how individuals belonging to different racial, ethnic, and cultural groups in the United States, as discussed in detail in the Surgeon General’s Report, Mental Health: Culture, Race, and Ethnicity [36]. Individuals living with mental health symptoms and suicidal ideations do not seek help that may aggravate situation. Research shows that depression, if not treated, would place individuals at risk for hurting themselves and others. Help-seeking behavior is affected by cultural factors because mental health is associated with stigma within cultures of South Asian communities [30]. In addition, lack of qualified and culturally sensitive practitioners is a challenge in healthcare system. Many providers, psychiatrists, counselors, social workers are trained in dominant cultures and society that shapes the patters of communications between providers and clients which are not compatible to South Asian cultures. This is a barrier which is correlated with the underutilization of mental health services by the South Asians [30]. Since this is a numerally small group, the systems are not geared up to provide culturally sensitive services. There is a huge need for workforce with South Asian background to provide the services because these groups have low/no confidence in regular workforce [29]. This is obvious in the discussions of health disparities often we get to hear about African Americans and Hispanic Americans but not much about South Asians. This subset of population is numerically small but distinct within Asian population in the United States [29]. Among South Asian Americans there is a strong emphasis on enculturation to preserve their culture during acculturation in American society [29].
Religious and social factors
In the literature, a few authors commented linking Hindu tradition to suicide. According to Hindu sacred texts like the Brahma Purana, ‘deha-tyaga’ is allowed for elevated and self-actualized people who believed to have accomplished the purpose of their life in this ‘mruthyalok’ (world where people will eventually die). This world is ‘mrutylok’ where people come here by birth and are bound to die after performing Karma in this birth. The western thinkers and scholars those who do not have in-depth knowledge of Hindu scriptures have interpreted and equated this with suicide. This is a striking difference between suicide and ‘deha-tyag’ (renouncing body). Those who are suffering from the feelings of loneliness, alienation, frustration, depression, hopelessness, and other mental health issues in life commit suicide, according to Western literature [27,29]. Whereas realized souls (satisfied with the life and fulfilled the deeds in this birth) decide to leave body (deha-tyag) to attain re-union with God (Moksha) through rigorous spiritual and meditational practices. Such individuals are rare and very tiny (fractional) proportion of world population.
According to Hindu beliefs there is no death to “Atman” (soul) which transcends into next phase after completing the term here on this earth. It is the body which is made up of five elements (air, water, earthly matter, fire, and space) which is returned to nature upon death. So, the physical form (body) ceases to exist, but soul transcends. In fact, according to Karma theory, a person born on this earth is required to go through one’s Karma and perform charitable deeds (consistent with Dharma [duties], as prescribed in Vedic literature, to liberate oneself from the cycles of birth and re-birth. Hindu scriptures do not allow anyone to sacrifice life by suicide which is treated as a ‘bad karma or sin’ that warrants a person’s re-birth and required good karma upon re-birth. And this cycle continues until a person attains positive balance of good acts (Karma consistent with Dharma). Ultimate goal of life is attainment of ‘moksha’ which is similar (not equivalent) to salvation in Christian tradition [29]. So, suicide is prohibited as per Karma theory. Another example of suicide, ‘Sati,’ is often cited as a practice promoted by Hindu religion. In fact, it has no place for such practice in original scriptures [27,29]. A social practice that originated to escape from political prosecution, torture, sexual subjugation, and slavery which surviving spouse(s) of a King (defeated or killed) and the servant women in the palace ended their life during medieval times. This is different from suicide which the previous studies described as a practice promoted or tolerated by Hindu religion. Authors lacking in-depth understanding of Hindu religious scriptures made misinterpretation by linking suicide to Hindu beliefs [29]. When a woman becomes a widow and decides to terminate her life to protect dignity to depart to the other world but not out of disappointment or hopelessness. Individuals who are from South Asia come from rich cultural backgrounds where the traditions and values are strong that influence family bonds and individual behavior [27]. Cultural and religious values create certain practices followed by the individuals.
Buddhist Religious Beliefs on Suicide
Literature and scholars have ignored the fact that Buddhist tradition is rooted in Hindu Sanatana Dharma. Hence tenets of Buddhist religion have deep meanings and explanations which is often ignored and/or misunderstood by the western scholars and others who learned scriptures under not so qualified masters. Like Hindu religion, Buddhist also strongly supports the idea of thinking about death and dying [26]. The underlying reasons for this are for people to be aware of the consequences of death and journey thereafter. Awareness of Karma consistent with Dharma is essential to live without desires and attachment that can take one on the path of enlightenment and fulfilment. The values and morals for living are emphasized and are embarked upon for Buddhist believers to be conscious and self-aware of their acts and their living based on ahimsa (non-violence). Violence to self and to others is actively prohibited. Non-violence is strongly rooted in the Vedic literature.
Family and community impact
The structure of the family unit is strong in most South Asian countries. Most of the families are patriarchal. There is evidence of how this structural unit is both a boon and bane to the individual. It is a boon when the family unit acts as a safety net to assist and support the individual. It becomes a bane when family inhibits a member from seeking professional help when needed. The impact and influence of the family on the individual is evident even when the individual sticks to country-of-origin culture [27]. This could be a factor that inhibits assimilation and leads to maintaining unique identity even after immigration. The cultural clash/conflict of the two cultures along with the added stress impacts the mental health of South Asian immigrants [33].
Model minority image also serves as a bane and creates pressure to succeed in school and career. When they fail to meet the expectations and feel shame and guilt that may lead them to suicidal ideation. The need for achievement is a major factor to maintain self-esteem in South Asians [33]. Many individuals who are of the age 18 years or younger tend to be pressured to do well in school/college education and later on in career. Such pressures cause them to have suicidal ideation and behavior [27]. Suicide rate among South Asian people is projected to be higher in Asian Americans, compared to all racial/ ethnic groups, who experience highest suicide rates (6.7% and 22.5% respectively) in both categories, 10-24 years, and 10-64 years in 2018 [28,34].
Socioeconomic Issues
South Asians, particularly Indians, come to the North Americas to establish a good life for themselves. Many who come to North America are overqualified and underemployed. They seek to try to move ahead and may sometimes end up in a point of no return. Immigrants from South Asian decent are seen to have a lot of problems with assimilation in the society and their inability to acculturate. There may be times that they are not able to compete with the local citizens and tend to do several different things that led them from one stress to another. They may be working several jobs, living in cramped shared quarters, doing jobs below their experience or educational level. This accumulated stress tends to manifest in different forms. This further inhibits their motivation and their potential to become stronger and reach their goals. They may in turn become unemployed, homeless, and poor (on welfare sometimes). Blakely, Collings, and Atkinson [37] reported an increase in the rate of suicide due to unemployment and half of these numbers are attributed to mental illness.
The immigration status may affect potential health benefits because undocumented immigrants do not get help to avail healthcare. These factors in addition to the regular stress of work and not being able to balance their finances with their needs. This creates an emotional turmoil and pulls them further into a negative spiral. This negative spiral leads to mental health issues including depression and anxiety. Some individuals due to genetic predispositions may become victims of some other major mental illnesses such as bipolar disorder or schizophrenia. Individuals dealing with mental health issues sometimes become aggressive when timely help is not offered. They also are defiant and do not want to seek help for their illnesses. The illnesses cause them to lose employment, friends and families thus causing depression and hopelessness. Additional socioeconomic stress occurs in trying to keep with the Joneses. Individuals try to deal with family pressures, but it becomes difficult, and it encourages individuals to use negative methods such as violence, alcoholism, and drugs to cope with their problems. These habits make their problems more complicated. Getting out of situations seems to become impossible and causes individuals to seek more dangerous ways of trying to escape the situation.
Legal issues and immigration Status
South Asians came to the United States either legally with visas, a green card, or as refugees. They sometimes come from countries afflicted by violence, political, and economic strife. They come in with stress related to their lives from their country of origin and expect to find immediate relief. The societal pressures cause further struggle which eventually pushes them towards suicide. It is seen that even if they come to US sponsored by their company or workplace, they deal with a lot of stress that causes them to become depressed, anxious, and sometimes even resort to violence within the family. Individuals at times use all their life savings to ‘pursue their dreams’ in the United States in the hope that they would be wealthy and prosperous in a quick time. The reality of their struggles and lack of supportive ‘social network’ [20] and family support tends to pull the person further into their misery. Individuals in these cases often find themselves in social and cultural situations where both the integration (love, comfort, caring, and feeling of belonging) and regulation (obligations, duties, responsibilities, and oversight) are either non-existent or minimal. This is one of the reasons why individuals resort to suicide as a solution [38]. Since there are not well documented numbers in terms of individuals who are subjected to human trafficking, it difficult to estimate suicide among these survivors. There is evidence of post-traumatic stress disorder (PTSD) about these immigrants. Southeast Asian refugees are at risk for PTSD associated with trauma experienced before and after immigration to the United States. One study found that 70% of Southeast Asian refugees receiving mental health care were diagnosed with PTSD.
Mental Health Issues, Access to Healthcare and impact on Suicide
Another aspect of culture is the taboo associated with the issues related to mental health. Mental illness is a further ignored area in this culture due to the taboo surrounding it. This leads individuals to resorting non-traditional methods and refraining from seeking help for the issues they are dealing with. Individuals may not take medications and in their depressed or manic states resort to taking their lives as opposed to getting treatment. The stress of cultural assimilation in combination with the stress of achievement and competition causes this social anomaly. The individuals who come in from countries that are overpopulated tend to constantly be in a struggle to better themselves economically. Their personal values and goals sometimes become secondary to their personal achievement. This cultural clash impacts the individual psyche causing them to crash and seek suicide.
Suicide stems from the depth of the depressed mind of an individual that see no hope or positive outcomes for oneself. Suicide is a very poignant but preventable tragedy. Individuals who succumb to their hopelessness are often those who project that they are strong and able to manage their lives well, while hiding their pain and suffering [30]. Suicide is the action taken by individuals who deal with depression and feel hopeless toward their life and life situations. Due to the cultural and socioeconomic situations, individuals seem to deal with a lot of stress and tend to pressure them to take drastic decisions such as suicide. Below are some numbers that show that almost 3 percent of the population below 18 years of age tend to have thoughts of hopelessness, sadness, and in general deal with depression. They may have comorbid factors that also cause them to deal with serious psychological distress. The details are presented in table 4.
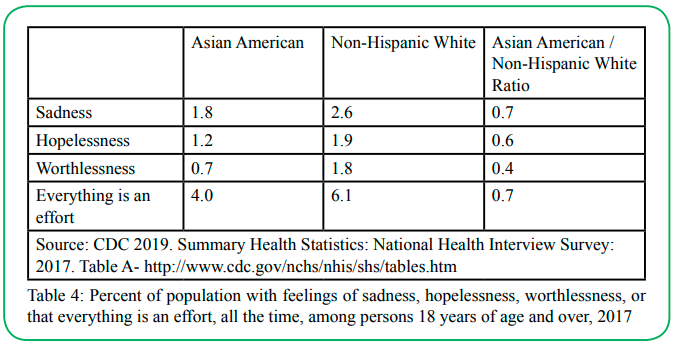
Table 4: Percent of population with feelings of sadness, hopelessness, worthlessness, or that everything is an effort, all the time, among persons 18 years of age and over, 2017
Individuals who are Asian American tend to still hold traditional values such respecting elders or family values. The acculturation may be moderate sometimes that causes individuals to deal with situations that are causing a cultural conflict. Cultural conflict leads to disagreement in the families. Individuals have differences with their elders and family members which causes micro-and macroaggressions in the family. This leads to more emotional turmoil and at times leads to depression, anxiety, and hopelessness. These feelings of hopelessness may be within the family and outside the family also. However, due to the difference in the ways different regions express cultural and social value systems, there is evidence of how they assimilate and absorb the culture they migrate to. The impressions of their values and culture are evident in the way they perceive and understand mental health issues and depression. It has been observed that there is cultural variability in the expression and manifestation of depression [39]. This may be the reason it is assumed that South Asians may not resort to suicide as an option when they are in their native countries.
The pressures of immigration and socio-economic issues cause them to react in drastic ways due to the emotional pressures they face outside their ‘safety net’ or place of comfort. Serious mental illnesses including depression and bipolar, along with the socio-economic circumstances are seen to be the cause of deaths caused by suicide. There has been an increase in suicide rates in the past decade. The issues related to employment, lack of employment, sense of achievement and being successful, seem to be the causes of more Asian American males committing suicide compared to females. The percentage of suicide is lesser that non-Hispanic white males and females, but that may be attributed to the overall numbers. Another crucial factor that impedes their well-being is the availability of their access to health care. Immigrants who may not be citizens or green card holders have health insurances that cover partially or none of the care that a person needs to deal with their mental health issues. They tend to let the issue be ignored which exacerbates the problem creating a crisis in the person’s life which may include the option of a suicide. That is the reason for a lower proportion of individuals seeking help for their mental health needs in relation to the general population, details can be seen table 5.
Access to health care
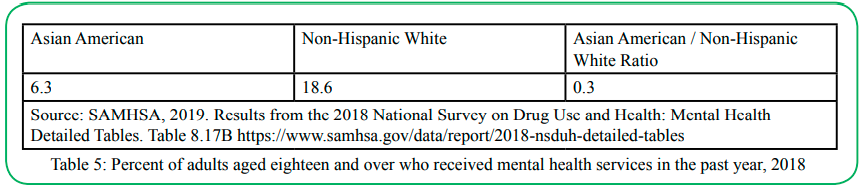
Table 5: Percent of adults aged eighteen and over who received mental health services in the past year, 2018
Some mental illnesses cause a lot of delusions, hallucinations, and suspicion, and at times, that cause individuals to believe that they must take their lives for varied reasons. The feeling of dejection and shame caused by social, environmental, and other reasons in turn closes all options to find or finding a solution for their problem. They resort to taking their lives instead. It is seen that the cultural and religious values which are the basis of many Asian value systems may be the reason for reduced suicide rates for Asian males and females compared to individuals who non-Hispanic white. South Asian males experienced higher percentage of suicides, though women have lower rate.
The same reasons could also present issues from enculturation perspective as discussed earlier. The details are presented in table 6.

Table 6: Age-adjusted death rates for suicide, by sex, race, and Hispanic origin, 2017
Identify Gaps in the Literature in subset of Asian population in the United States
Center for Disease Control [40] has no specific informational on South Asians. This is a gap in compilation of data. To represent data on South Asians, it is imperative that data from all clinician’s office, County hospitals and other health care facility should be collected and report data on suicides, attempted suicide, and as well as suicide ideation. Furthermore, people must be educated about suicide as a public health problem and no stigma should be attached so that people will not feel threatened to express and report any such incidents voluntarily.
Jha, Ahuja, Wani & Bavikatte [41] pointed out there are huge gaps in literature on South Asians. There is no literature suicide on thoughts and behavior, prevalence, and risk factors. They further mentioned their thematic analysis was on financial problems, lack of social support and marital problems as common themes were discussed. Research studies conducted in English automatically eliminate non-English speakers or participants and miss on this groups’ input. This is a huge gap, and this group cannot access literature in English and most of the literature is in English.
Analysis of Findings
Research on suicide among South Asians immigrants after migrating to the United States are exposed to life events, social disconnect with familiar environment, interpersonal losses, conflict within the family, intergenerational conflict, unemployment or under-employment, lack of financial resources and a host of other psychosocial and cultural and economic factors plays an crucial role in leading to depression and suicidal behaviors [22].
For South Asian population, though it constitutes 1.7 percent in the United States, higher rates of suicides are projected since Asian American population was found to have higher rates of suicides in both age groups, 10-24 years (youth) and 10-64 years (children, adolescents, and adults). This is remarkably striking facet of model minority ethnic groups. This revelation is supported by under-utilization of mental health services and substance use in this population. In the age of 10–24-year age group of Asian Americans, it is 22.5 percent of deaths are due to suicide. Most of them choose suffocation as means to end their lives.
Immigrants who may not be citizens or green card holders may or not have health insurances and those who have full or partial coverage for mental health issues they don't utilize the services. They tend to let the issue be ignored which exacerbates the problem creating a crisis in the person’s life which may include the option of a suicide [22]. That is the reason for a lower number of individuals seeking help for their mental health in relation to the general population [23]. Individuals experience high psychological distress if they are less acculturated to the dominant culture [23]. For instance, immigrant students from South Asian origin expressed concerns and reported to have faced a lot of prejudice like their Asian American and Hispanics counterparts in social, educational, and occupational realms of life [18]. Cohen [42] mentioned, the interaction of South Asian American ethnicity, hopelessness and suicidal ideations have significant effects and hence, it is important to pay caution while interpreting the effects of interaction of these factors.
Heredity is one of the major risk factors for people with thoughts on suicide leading to psychiatric disorder [43]. Suicide is a multifaceted problem. Cultural, social, mental, and physical health and economic domains are determinants which pressurized a person. Cultural clash impacts a person individual psyche and cause them suicide. South Asians seek refuge in religion than help seeking behaviors. South Asians are socialized to believe suicide as a sin and hence do not share their thoughts. And they do not seek help, they are defiant. Immigrants feel stuck and difficult to get out of the situation. Depression and bipolar are seen as a cause of death caused by suicide. Immigrant and South Asians issues cause them to react in drastic ways due to the emotional pressures [23]. Research evidence also suggests age and gender differences in the association between life events and suicidal behavior, with younger subjects are likely to have more adverse life events than older subjects, and males likely to experience more life events than females which is clearly reflected in the statistics presented earlier. School environment, for South Asians, contributed to their plight, vulnerability, stress, and suicide. In older adults, health impairments, somatic illnesses and declining physical capacity play a role in precipitating suicidal behavior, with some evidence that physical health problems play an increasingly influential role with increasing age, particularly for males. A further set of factors associated with suicidal behavior in adults relates to various forms of social interaction. Those making serious suicide attempts are likely to be characterized by high rates of social isolation, feelings of loneliness, poor social support, and lack of a close, confiding relationship. These findings call for further research on South Asian Americans and for policy attention [24].
Discussion
It is evident from this research that a host of factors are responsible for higher rates of suicide amongst South Asians and Asian Americans in general. It is a public health as well as a psychosocial problem. This is an effort to delve deeper into health, mental health, and well-being of South Asian and Americans immigrants and their under-representation in the utilization of mental health and social services. Social conditions or social problems may change but the response and the human reactions to vulnerable situations and adverse social conditions remain the same. The means of committing suicide have changed though. It is evident from the above literature the factors that are causes of suicide among South Asians are, more than genetic factors, acculturation, enculturation, stress, mental health, and model minority image. Suicide is a social problem as one million deaths and twenty-five million suicidal attempts are accounted or undertaken [2]. Medically, suicide and self-injury costs $69 billion. It is a public health problem that represents the mental health dimension of the individual’s health. The loss of humans due to suicide are greater than homicide and suicide is not based on one single factor but an outcome of multidimensional environmental factors, personal, economic, and socio-cultural factors.
Future research should focus on social and cultural dimensions of South Asians Americans [21]. Limited number of studies on South Asian Americans signals the gaps in research [24]. Future research should focus on the gaps, different South Asian ethnic groups, and interventions on how to stop this inter-generational suicide [44]. Longitudinal studies were recommended to examine the issues concerning South Asian population. Under-reporting of suicide prevails in Asian Americans since there is stigma associated with it. Future studies should examine multidimensional aspects of Asian American suicidal behavior along with acculturation and enculturation variables. Current measures of suicide could not capture spectrum of suicidal ideation and behavior [27]. Future research should focus presented on suicide among different South Asian ethnic groups since studies contradictory findings about South Asians. Public mortality data research recommended for future researchers [25]. Future research should pay attention and assess the needs of the Asian Americans as recommended by Chambers et al. [45]. More rigorous studies are needed to investigate cultural and religious influences on suicidal ideation and behavior [29]. More research needed on impact of gender and cultural issues on Asian American women [34].
Suicide prevention and interventions strategies
There is a great need for comprehensive approach to suicide trends among South Asians and Asian Americans in general. Policy needs to recognize unique challenges and issues of this population. It is important for clinicians and service providers to look for signs and symptoms. It is likely that individuals who have suicidal thoughts can cause harm to themselves within one hour. It is imperative that prevention or intervention must be provided in a very narrow timeframe of one hour to reach and protect the individual from the risk of suicide. O’Brien [14, p.15] strongly recommended that words like “kill yourself” or “die by suicide” are not to be used and usage of “the word commit is more is punitive” and “successful” and “unsuccessful” are to be avoided. Individuals at-risk for suicide can be identified by observing for their behavioral patterns. As suicide results from a combination of factors rather than one single factor. More importantly, the factors that affect each age-group are different. O’ Brien points out the stressors for suicide for adolescents and adults are different. For example, scary medical diagnosis might lead to suicide in adults and reasons like bullying can lead to suicide among young adolescents. Reed [44, p.16] mentioned, “usually, people don’t want to die by suicide, they just want to end their pain.” “We want to catch people and alleviate that pain, so they don’t turn to lethal means and make the decision to end their life.” Reed further mentions youth more often engages in impulsive suicide. Furthermore, teens expressed the need for empathetic listening.
It is important that individuals are encouraged to help themselves by creating a list of people and resources available for readily for help to access when they feel suicidal thoughts take over them O’Brien [14]. O’Brien, [14] said the individuals should focus on interesting things that makes individuals want to live. If individuals are at -risk of involving in self-harm and possess firearms, then they must keep it away from their homes and lock in a place to prevent easy access. Twelve aspirational goals of the research prioritization process of the National Action Alliance for Suicide Prevention are prescribed. Although stakeholders indicated that predicting who is at imminent risk was an aspirational research goal. And expert consultants recommended that assessments focused on finding treatable conditions or symptoms were more actionable than prediction per se. Therefore, this goal has been reworded.
Conclusion
South Asians, particularly Indians come to the North Americas to establish a good life for themselves. The struggles of trying to find that balance in their lives and not be overwhelmed by the stress causes them to go to places where they do not want to go to many who come to North America are overqualified and underemployed. Individuals as seen in the above scenarios have a lot of problems with assimilation in the society and their inability to acculturate. They may be working several jobs, living in cramped shared quarters, doing jobs below their experience or educational level. This accumulated stress tends to manifest in different forms. This further inhibits their motivation and their potential to become stronger and reach their goals.
Conflict of interest:
The authors declare no conflict of interest.
References
National Institute of Mental Health. (2019, January 18th). Suicide Prevention. https://www.nimh.nih.gov/health/topics/ suicide-prevention/index.shtml View
Franklin, J. C., Ribeiro, J. D., Fox, K. R., Bentley, K. H., Kleiman, E. M., Huang, X., Musacchio, K. M., Jaroszewski, A. C., Chang, B. P., & Nock, M. K. (2017). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143(2), 187–232. https://doi. org/10.1037/bul0000084View
American Association of Suicidology (2020, August 1st). Facts & Statistics. https://suicidology.org/2020facts-and-statistics/View
Hijioka S, Wong J. (2012). Suicide among Asian Americans. [Fact Sheet]. Retrieved June 21,2020, from http://www. apa.org/pi/oema/resources/ethnicity-health/asian-american/ suicide-fact-sheet.pdf. In Psychiatric Treatment, 8(6), 418-423. doi:10.1192/apt.8.6.418.View
American Psychological Association (2017, August 1st). Statistics on Asian Americans’ Suicide-Related Outcomes. https://www.apa.org/pi/oema/resources/ethnicity-health/asian-american/suicide-fact-sheet.pdfView
South Asians Americans Living Together (SAALT, 2018). Resources and Fact Sheets. https://saalt.org/wp-content/ uploads/2019/04/SAALT-Demographic-Snapshot-2019.pdfView
Khuwaja, S. A., Selwyn, B. J., Mgbere, O., Khuwaja, A., Kapadia, A., McCurdy, S., & Hsu, C.E. (2013). Factors associated with the process of adaptation among Pakistani adolescent females living in United States. Journal of immigrant and minority health, 15(2), 315–325. https://doi.org/10.1007/s10903-012- 9703-6View
Miranda, R., Polanco-Roman, L., Tsypes, A., & Valderrama, J. (2013). Perceived discrimination, ruminative subtypes, and risk for depressive symptoms in emerging adulthood. Cultural Diversity and Ethnic Minority Psychology, 19 (4),395-403. https://doi.org/10.1037/a0033504View
South Asians Americans Leading Together (SAALT, 2015). A Demographic Snapshot of South Asians in the United States (Fact Sheet). http://saalt.org/wp-content/uploads/2016/01View
Hameed, S., Sadiq, A., & Din, A. U. (2018). The Increased Vulnerability of Refugee Population to Mental Health Disorders. Kansas Journal of Medicine, 11(1), 1–12.View
Hawton, K., & Van Heeringen, K. (2009). Suicide. Lancet (London, England), 373 (9672), 1372–1381.https://doi. org/10.1016/S0140-6736 (09) 60372-X.View
Johnson, M. W., Garcia-Romeu, A., Cosimano, M. P., & Griffiths, R. R. (2014). Pilot study of the 5-HT2AR agonist psilocybin in the treatment of tobacco addiction. Journal of psychopharmacology (Oxford, England), 28 (11), 983–992. https://doi.org/10.1177/0269881114548296 View
Centre for Disease Control and Prevention. (2014, June 12th). Health, United States, 2014 with Special Feature on Adult Aged 55-64. https://www.cdc.gov/nchs/data/hus/hus14.pdfView
McManama O’Brien, H.K. (2018). Suicide Rates on The Rise. Social Work Advocates. National Association of Social Workers,) Oct.-Nov. , pp. 12-21, Social Workers.org https:// www.socialworkers.org/News/Social-Work-Advocates/2018- Oct-Nov-Issue/Suicide-Rates-on-the-Rise
Borges, G., Angst, J., Nock, M. K., Ruscio, A. M., & Kessler, R. C. (2008). Risk factors for the incidence and persistence of suicide-related outcomes: a 10-year follow-up study using the National Comorbidity Surveys. Journal of affective disorders, 105 (1-3), 25–33. https://doi.org/10.1016/j.jad.2007.01.036View
Seth, M. (1995). Asian Indian Americans. In P.G. Min (Ed.). Asian Americans: Contemporary trends and issues. Thousand Oaks, USA: Sage. Google Scholar
Szapocznik J., Kurtines W.M., Fernandez T. (1980). Bicultural involvement and adjustment in Hispanic-American youths. International Journal of Intercultural Relations, 4 (3-4), pp. 353-365.View
Sodowsky, G.R., Lai, E. W. & Plake, B. S. (1991). Moderating effects of sociocultural variables on acculturation attitudes of Hispanics and Asian Americans. Journal of Counseling and Development,70,194-204.
LaFromboise, T. & Coleman, H & Gerton, J. (1993). Psychological Impact of Biculturalism: Evidence and Theory. Psychological Bulletin, 114. 395-412. 10.1037/0033- 2909.114.3.395.View
Durkheim, E. 1897 (1951). Suicide: A study in sociology. Translated by JA Spaulding, G Simpson. New York: Free Press. View
Fikree, F. F., & Pasha, O. (2004). Role of gender in health disparity: the South Asian context. BMJ (Clinical research ed.), 328(7443), 823–826. https://doi.org/10.1136/bmj.328.7443.823.View
Forte A, Trobia F, Gualtieri F, Lamis DA, Cardamone G, Giallonardo V, Fiorillo A, Girardi P, Pompili M. (2018). Suicide Risk among Immigrants and Ethnic Minorities: A Literature Overview. International Journal of Environmental Research and Public Health, 15(7): 1438.View
Fernando. G.A. (2015). Attempting to bridge the 10/90 divide: special issue on South Asian mental health, International Review of Psychiatry, 27:3, 176-179. DOI: 10.3109/09540261.2015.1065079View
Nath, S. R., VanLeer, S., & Ahmad-Stout, F. (2018). South Asians and suicide: Beliefs about suicide in a U.S. community sample. Asian American Journal of Psychology, 9(4), 334– 343. https://doi.org/10.1037/aap0000145View
Kuroki Y. (2018). Comparison of Suicide Rates Among Asian Americans in 2000 and 2010. Omega, 77(4), 404–411. https:// doi.org/10.1177/0030222816678425.View
Leong, F. T., Leach, M. M., Yeh, C., & Chou, E. (2007). Suicide among Asian Americans: what do we know? What do we need to know? Death studies, 31(5), 417–434. https://doi. org/10.1080/07481180701244561View
Wong, J., Uhm, Y., & Li, P. (2012). Asian Americans' family cohesion and suicide ideation:Moderating and mediating effects. American Journal of Orthopsychiatry, 82(3), 309–318. https://doi.org/10.1111/j.1939-0025.2012.01170.xView
Duldulao, A. A., Takeuchi, D.T. & Hong, S. (2009). Correlates of Suicidal Behaviors among Asian Americans, Archives of Suicide Research, 13:3, 277-290. https://doi. org/10.1080/13811110903044567.View
Thapa, P., Sung, Y., Klingbeil, D. A., Lee, C. Y., & Klimes-Dougan, B. (2015). Attitudes and Perceptions of Suicide and Suicide Prevention Messages for Asian Americans. Behavioral Sciences (Basel, Switzerland), 5(4), 547–564. https://doi. org/10.3390/bs5040547.View
Conrad, M.M., & Pacquiao, D.F. (2005). Manifestation, attribution, and coping with depression among Asian Indians from the perspectives of health care practitioners. Journal of Transcultural Nursing.16 (1):32-40.View
Lane, R., Cheref, S., & Miranda, R. (2016). Ethnic differences in suicidal ideation and its correlates among South Asian American emerging adults. Asian American Journal of Psychology, 7 (2), 120-128.View
Dupree, W.J., Bhakta, K.A., Patel, P.S., & Dupree, D.G. (2013). Developing Culturally Competent Marriage and Family Therapists: Guidelines for Working with Asian Indian American Couples. The American Journal of Family Therapy, 41 (4), 311-329. View
Renzi-Callaghan, P. (2018) Healing from the loss of a loved one to suicide, Qualitative Research in Psychology, 15:2-3, 367- 374, DOI: 10.1080/14780887.2018.1430731.View
Noh, E. (2007) Asian American Women and Suicide, Women & Therapy, 30:3-4, 87-107, DOI: 10.1300/J015v30n03_08. https://doi.org/10.1300/J015v30n03_08.View
Giddens. A. (1964). Notes on the Concepts of Play and Leisure. Sociological Review. SAGE Publications.View
Department of Health & Human Services (2001). Mental Health Services in Primary Care Settings for Racial and Ethnic Minority Populations. Rockville, MD: U.S. Department of Health and Human Services, Office of Minority Health, September 2004. 26p.View
Blakely, T., Collings, S., and Atkinson, J., (2003). Unemployment and suicide. Evidence for a causal association? Journal of Epidemiology Community Health, 57 (8): 594–600.View
"Society and Culture." Institute of Medicine. 2002. Reducing Suicide: A National Imperative. Washington, DC: The National Academies Press. doi: 10.17226/10398.View
Marsella, A.J., Sartorius, N., Jablensky, A., & Fenton, F.R (1985). Cross-cultural studies of depressive disorders: an overview. Culture and Depression. Berkeley, Calif, USA: University of California. View
Centre for Disease Control and Prevention (2019, June 12th). National Vital Statistics Report. Vol.68, No. 09. Table 10. https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf View
Jha, A., Ahuja, M., Wani, R., Bavikatte, S. (2019). (Jan. 16- 20) Suicide in South Asian Americans: An Emerging Public Health Problem Society for Social Work and Research 23rd Annual Conference session. (Ending Gender Based, Family and Community Violence conference, San Francisco, United States. https://sswr.confex.com/sswr/2019/webprogram/Paper35816. html View
Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Lawrence Erlbaum; 1988. [Google Scholar] View
Beautrais, A. (2003). Suicide and Serious Suicide Attempts in Youth: A Multiple-Group Comparison Study. The American journal of psychiatry. 160.109310.1176/appi.ajp.160.6.1093.View
Reed, J., (2018). Suicide Rates on The Rise. Social Work Advocates. National Association of Social Workers,) Oct.-Nov., pp. 12-21, Social Workers.org https://www.socialworkers.org/ News/Social-Work-Advocates/2018-Oct-Nov-Issue/Suicide-Rates-on-the-RisView
Chambers, D.A.; Pearson, J.L.; Lubell, K.; Brandon, S.; O’Brien, K.; Zinn, J. (2005). The science of public messages for suicide prevention: A workshop summary. Suicide Life Threat. Behav., 35, 134–145. [Google Scholar] [Cross Ref] [PubMed]View