
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-163
https://doi.org/10.33790/jmhsb1100163Research Article
How Anxiety Our Adult Patients Before Venepuncture Procedure: A Study in UiTM Medical Centre Sungai Buloh (UiTMMC)
Izzaty Dalawi1,2, Mohamad Rodi Isa1*, Khasnur Abd Malik 3, Faizul Haris Mohd Hatta1,2, & Muhammad Fairuz Rahmat1
1 Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi Mara (UiTM) Sungai Buloh Campus, 47000, Selangor, Malaysia.
2 Training Management Division, Ministry of Health, Level 6, Menara PRISMA, Presint 3, 62675, Putrajaya, Malaysia.
3 Department of Primary Care Medicine, Faculty of Medicine, Universiti Teknologi Mara (UiTM) Sungai Buloh Campus, 47000, Selangor, Malaysia.
Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA Jalan Hospital, 47000 Sungai Buloh, Malaysia.
Received date: 20th April, 2021
Accepted date: 04th June, 2022
Published date: 07th June, 2022
Citation: Dalawi, I., Isa, M. R., Abd Malik, K., Mohd Hatta, F.H., & Rahmat, M.F., (2022). How Anxiety Our Adult Patients Before Venepuncture Procedure: A Study in UiTM Medical Centre Sungai Buloh (UiTMMC).
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Venepuncture is one of the commonest stressful invasive procedures in the health care setting. Unfortunately, to date, there was a lack of locally published studies that studied anxiety, especially before the procedure among adult patients. Hence, this study was conducted to determine the factors associated with the state and trait-anxiety among adult patients before the venepuncture procedure in UiTMMC.
Methods: A cross-sectional pilot study was conducted among patients while waiting for a venepuncture procedure in March 2020. Patients aged 18 years old and above, Malaysian, able to understand English or Malay and had experienced venepuncture in UiTMMC were recruited. Malay validated version of the State-Trait-Anxiety-Inventory (STAI) Questionnaire was used to assess the anxiety level. Data were analysed using IBM SPSS Version 26.0, and multiple linear regression was used to determine the associated factors for state and trait-anxiety before the venepuncture procedure.
Results: A total of 330 patients with a mean age of 46.34 ± 14.34 years participated in this study. The mean of the state-anxiety score was 38.02 ± 14.25 and the mean trait-anxiety score was 36.46 ± 11.47. The correlation between state-anxiety and trait-anxiety scores was highly significant (r=0.870, p<0.001). Factors associated with state-anxiety and trait-anxiety contributed with 72.6% and 58.5% variances, respectively.
Conclusions: Adult patients who waiting for venepuncture in were average low state and trait anxiety scores. Although the associated factors were majority non-modifiable, this finding still can instil awareness to the health care workers who are dealing with needle procedurals.
Keywords: State-anxiety, Trait-anxiety, Venepuncture.
Introduction
Venepuncture or also known as phlebotomy is one of the most frequent medical procedures whereby the vein is punctured with the needle to withdraw the blood or for intravenous medication purposes. Despite its common, there is approximately 10% of individuals in medical settings report an excessive fear of the needle which subsequently may lead to significant avoidance, distress and problems in managing and treating the patients [1]. Research also has established that waiting for surgery or any invasive procedures is stressful, and anxiety may aggravate the situation [2].
Anxiety can be defined as an emotion characterised by feelings of tension, worried thoughts and physical changes [3]. Anxiety can be a normal and expected feeling in life. However, when it causes disproportions and interferences to the daily activities, job performance and relationship of the individual, it is called an anxiety disorder. Generally, an anxiety reaction may be developed due to acute or chronic pain [4]. Spielberger CD [5] have classified anxiety into two types which is state-anxiety and trait-anxiety. State-anxiety can also be called "right-now anxiety" which reflects a transitory emotional state or a condition that is characterised by subjective, consciously perceived feelings of tension and apprehension, and heightened autonomic nervous system activity. It may fluctuate and can vary in intensity. In contrast, trait-anxiety refers to a general tendency to respond with anxiety to perceived threats in the environment and is a relatively stable characteristic of an individual. An individual with higher trait-anxiety feels more threats in many situations than someone with low trait-anxiety. Hence, it is best to study both kinds of anxieties at the same time [6].
Several researchers have investigated the anxiety and pain of venipuncture and cannulations procedures in recent years. However, the studies were more focused on the children and young adult populations [7]. There was also a wide range of prevalence of anxiety towards venipuncture found among young adults and adults. Some studies reported the prevalence could be as low as 3 to 5% [8] to 20 to 50% [7] or as high as 73.3% [9]. Looking at the prevalence of venipuncture-related anxiety mentioned, it gives an idea that the adult population is also facing the same issues as children when it comes to anxiety on needle procedural or venepuncture. There is a necessity to explore further from the study on factors that may be associated with it.
Distress to needle procedural such as venepuncture poses the patients with psychological stress, anxiety and needle phobia, which can have deleterious consequences to the patients. For example, anxiety has negatively affected thoughts and behaviour such as avoidance of health care and rehabilitation [4] and avoidance of influenza vaccination [7]. Besides, the needle fear also may extend to another procedure such as blood donation and may affect those with chronic conditions that requiring injection such as diabetes mellitus [7].
The anxiety toward venepuncture can be associated with several factors such as underlying chronic illnesses [10], age and gender, level of pain, marital status, income status, body mass index, level of pain [11] and presence of accompanying [12]. Other than that, venipuncture services and patient's satisfaction also showed to be related to venipuncture-related anxiety symptoms [13].
However, most of the literature found were from international studies. It implied the topic of anxiety towards venepuncture services in our local setting yet is still under-published. There is no similar study found measuring the anxiety on venepuncture while the patient is waiting for the procedure in the outpatient phlebotomy setting. Hence, it opens the necessity to explore further the extent of anxiety symptoms experienced in our local adult populations and the factors that may be associated with their anxiety before the venepuncture procedure is done. Therefore, the objective of this study was to determine the state and trait-anxiety levels and its associated factors among patients while waiting for venepuncture procedure in UiTM Medical Centre Sungai Buloh (UiTMMC).
Material and Methods
Study design
The cross-sectional study design was conducted at the Phlebotomy Unit, UiTM Medical Centre Sungai Buloh (UiTMMC). The phlebotomy services are operating on weekdays from 7.30 am to 4.00 pm. All patients who attended the Phlebotomy Unit for blood taking procedure between March 2020 until May 2020 was set as the target population.
Study population, Inclusion and Exclusion criteria
The study population consisted of all patients who attended the Phlebotomy Unit UiTMMC for blood taking procedure between March 2020 until May 2020 who fulfilled the inclusion and exclusion criteria for the study.
The inclusion criteria for the study were patients aged 18 years old and above, Malaysian citizens, able to speak and understand in Malay and had at least experienced one venepuncture procedure in UiTMMC before. On the other hand, a patient who has been diagnosed with any psychiatry problems and under psychiatry clinic active follow up, a patient who is on any psychotropic drugs such as antidepressants, sedatives (anxiolytics, hypnotics) or antipsychotics medications or patient who are not consented to participate in the research has been excluded from the study. The systematic random sampling was used to select the patients whereby every alternate two patients who were available and eligible for the study during the data collection session were approached. Patients who had provided a written informed consent would be recruited for the study.
Data collection methods and instruments
This study was only able to conduct the data collection process in March 2020 due to the unprecedented pandemic Covid-19 infection that happened in the early year 2020. During the study recruitment, all patients who attended the outpatient Phlebotomy unit, UiTMMC were screened through the registration number of the patients. From the patient’s registration number, their medical record was retrieved to ensure the patients with underlying psychiatry illnesses or on psychotropic medications have been excluded. Every two alternate patients were approached and informed about the study. A patient information sheet that consisted of brief information about the study was given to the approached patient. Once the patient agreed to participate, informed consent was signed by the patient, and a copy will be kept each by the patient and researcher for record-keeping.
Subsequently, the patient was given a set of questionnaires that consisted of two parts. Part 1 consisted of the sociodemographic details of the patient (age, gender, ethnicity, religion, marital status, occupation, education level, household income per month, body mass index (BMI), smoking status and living arrangement), past venepuncture history (frequency of venepuncture per year, history of complications upon venepuncture in the past, venepuncture service rating based on the patient had in UiTMMC and the presence of accompanying for venepuncture procedure during the data collection day.
Part 2 of the questionnaire made up the outcome for the study which consisted of the translated Malay version of the State-Trait-Anxiety Inventory (STAI) Form Y for Adults that able to measure state-anxiety and trait-anxiety of the patient [14]. The State-anxiety scale (STAI Form Y-1) consisted of 20 statements that evaluate how the patient feels "right now, at this moment, before the venepuncture procedure takes place". There is a four-points-Likert scale for the patient to choose the number that best describes the intensity of their feelings at that particular moment. The scales were: 1 = not at all, 2 = somewhat, 3 = moderately, and 4 = very much. The trait-anxiety scale (STAI Form Y-2), consisted of 20 statements that evaluate how the patient feels "generally". The patient needs to choose and rate their feelings on the following four-points-Likert scale. There scales were: 1 = almost never, 2 = sometimes, 3 = often and 4 = almost always. The sum of the scores on all items remarks the individual patient score. The scores for both state-anxiety and trait-anxiety can be varied from a minimum of 20 to a maximum of 80.
The translated and validated Malay version of STAI Form Y by Hashim, Wan-Hasyila [14] used has very high reliability as the Cronbach alpha form STAI Form Y1 (STAI-S) and STAI Form Y2 (STAI-T) was 0.94 and 0.84 respectively. The structured face-to-face interview was done whereby every patient who has consented to participate in the study was interviewed using the questionnaire. It took about 10 to 15 minutes to complete the interview per patient.
Ethics approval
The study was conducted in compliance with the ethical principles outlined in the Declaration of Helsinki and Malaysia Good Clinical Practice Guideline. Research ethical approval was obtained from the UiTM Research Ethics Committee with the approval code REC/05/2020(MR/103) and also granted permission to conduct the data collection from the Deputy Dean of Clinical Service, UiTM Sungai Buloh Campus. All study participants have signed written informed consent before their study participation.
Statistical analysis
Data were analysed using statistical software IBM SPSS Version 26.0. For descriptive statistics, data were presented with the absolute number (n) and percentage (%) for categorical data. For numerical data, it was presented by the mean and standard deviation for normally distributed data. For non-normal distributed data, it was presented by the median and interquartile range (IQR). Normality of the distribution of the continuous variables was evaluated using skewness and kurtosis as well as the Kolmogorov-Smirnov normality test.
The dependent variable in this study was the State-anxiety and Trait-anxiety scores. The distribution of these scores must be normally distributed. If the normality was not fulfilled, transformation using reciprocal transformation method, which was determined through the trial-and-error approach to fulfil the assumption for the parametric method.
One-Way analysis of variance (ANOVA) was performed to compare the state and trait-anxiety score with all the categorical independent variables. For the determination of factors associated with state-anxiety and trait-anxiety, data was analysed using multiple linear regression (MLR). Before the analysis was done using MLR, simple linear regression (enter method) was used to examine the relationship between state and trait-anxiety score and all the independent variables. The significant variables in simple linear analysis were further analyzed using multiple linear regression to adjust for the confounding factors to determine the factors associated with State-anxiety and Trait-anxiety
The linear regression models were created using backwards-step selection methods. The assumptions of linear regression were evaluated using a variety of tests. The scatter plot on residual values was plotted to assess the linearity and homoscedasticity when the dots were scattered without showing any figure. The outliers were checked by plotting the scatter plot of the residual where the dots were scattered within -3 to +3. Autocorrelation of the independent variables was examined using the Durbin-Watson test and showed the value closed to two, which means no autocorrelation was detected. The multicollinearity was checked using the variance inflation factor (VIF) and showed less than five for both state and trait-anxiety score, which means no multicollinearity. There were also no interactions between the independent variables considered in the analysis. A value of p < 0.05 was considered statistically significant.
Data management
The questionnaire was checked by the researcher at the end of each interview session and before the compilation of the data to ensure its completeness. All data were entered and coded into the personal researcher's computer with a password protected. All data will be kept for a minimum of 5 years.
Results
The overall response rate for our study was 89.5%. The sociodemographic and characteristics of the respondents are presented in Table 1. A total of 330 patients participated in the study with a mean age of 46.34 ± 14.34 years old and gender were equally distributed. The majority of the patients were Malay (61.2%), Muslim (65.5%) and married (79.1%). More than half of the patients have had their education until upper secondary level (58.2%) and currently still working (54.7%) with a median of household income RM 4,500 (IQR: 4422.00). 54.7% were working at the government staff and 61.9% working at the non-healthcare sector. The majority of patients were underweight & normal BMI (67.6%), non-smoker (61.2%) and 94.5% were staying with their family or partner.
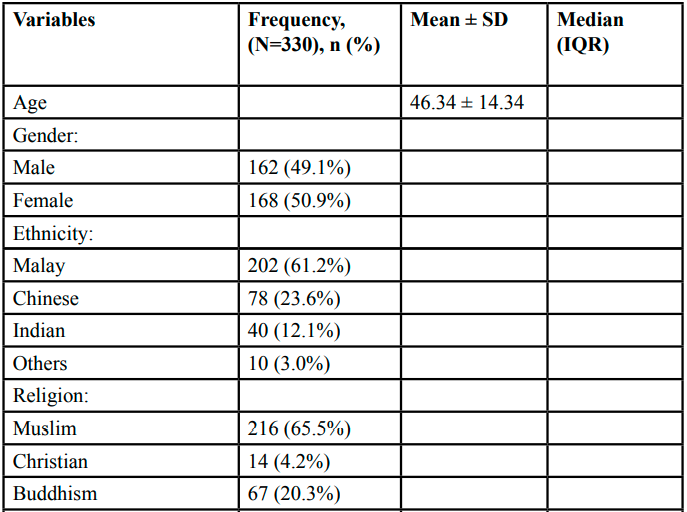
Table 1: Sociodemographic of the respondents (N=330)
The venepuncture history of the respondents is shown in Table 2. 50.6% came accompanied and 59.7% of the patients came to the unit quite frequent with at least every 3-monthly. The majority of the patient had no history of venepuncture complications in the past (86.7%) with 22.7% gave complications of swelling and 70.5% of bruising. Overall gave a good rating on their perceived venepuncture service rate and their venepuncture experience in UiTMMC.
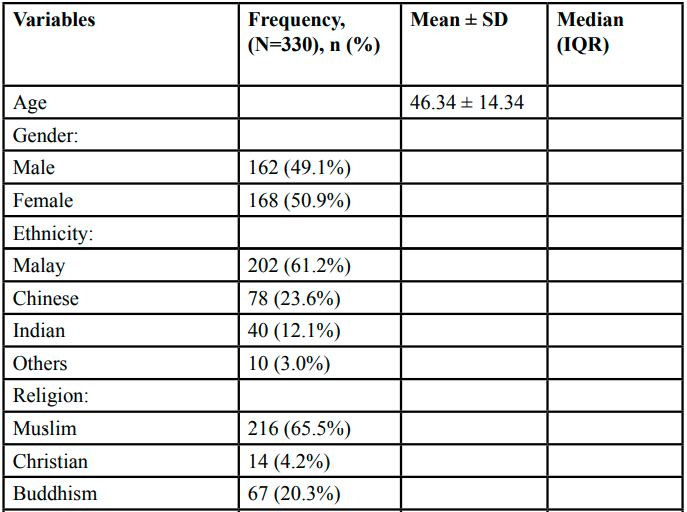
Table 2: Venepuncture history of the respondents (N=330)
The mean of the state-anxiety score was 38.02 ± 14.25 and the mean trait-anxiety score was 36.46 ± 11.47. Both of the scores were normally distributed (Kolmogorov Smirnov test: p = 0.200 and p = 0.200, respectively). The minimum score for state-anxiety and trait-anxiety was 20. However, the maximum score for state-anxiety was 67 and the maximum score for trait-anxiety was 65. The correlation between state-anxiety and trait-anxiety was positive linear (Pearson correlation coefficient, r = 0.870, p < 0.001).
Table 3 shows the comparison of the state and trait-anxiety scores with all the categorical independent variables. For the State-anxiety score, there were differences in the mean score in gender (p=0,002), educational level (p=0.023), occupational status (p<0.001), BMI classification (p<0.001), smoking status (p<0.001), presence of accompanying (p<0.001), frequency of venepuncture (p<0.001) and history of complication (p<0.001). For the Trait-anxiety score, there were differences in gender (p=0.004), educational level (p=0.011), occupational status (p<0.001), BMI classification (p<0.001), smoking status (p<0.001), presence of accompany (p<0.001), frequency of venepuncture (p<0.001) and history of complication (p<0.001).
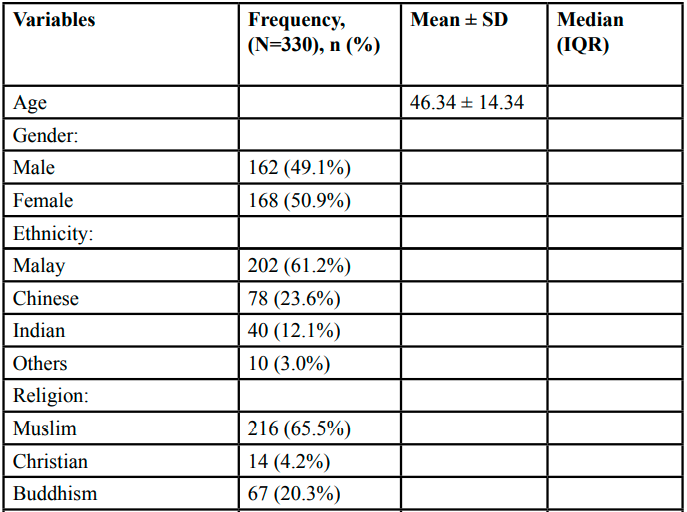
Table 3: The comparison of the State-anxiety and Trait-anxiety scores between variable interest (N=330)
Table 4 shows the factor associated with State-anxiety. There were seven factors found to be significant: age, gender, BMI classification, smoking status, presence of accompany and frequency of venepuncture in a year. The state-anxiety score increases by 0.084 (95%CI: 0.014, 0.154) state-anxiety score by the one-unit increase in and female has higher 5.506 (95%CI: 2.554, 8.845) state-anxiety score compared to male. University educational level has 2.479 (95%CI: 0.497, 4.462) higher in state-anxiety score compared to the primary level of education. Obese patients had a higher 18.442 (95%CI: 14.533, 22.221) and overweight had a higher 17.929 (95%CI: 15.117, 20.741) state-anxiety score compared to the underweight & normal BMI group. Those ex-smokers had less 10.156 (95%CI: (-13.574, -6.737) state-anxiety score compared to the current smoker and those without the presence of accompanying had 3.111(95%CI: 1.096, 5.126) higher state-trait score compared to those with the presence of accompanying. Patients who had at least once in a year frequency of venepuncture had 12.662 (95%CI: 0.685, 1.459) and those with at least once in 6 months frequency of venepuncture had 2.457 (95%CI: 0.685, 1.459) higher in state-anxiety score compared to who had at least once in a month. All these factors contributed to 72.6% variances of the state-anxiety score.
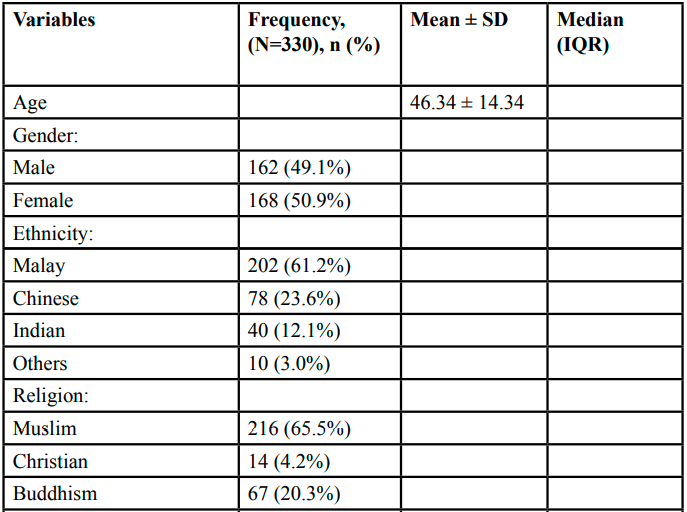
Table 4: Factor associated with State-Anxiety
On the other hand, for Trait-anxiety, six factors were found to be significant: age, gender, BMI classification, smoking status, presence of accompany and the frequency of venepuncture (Table 5). The trait-anxiety score increases by 0.093 (95%CI: 0.027, 0.160) with the one-year increase in age and female has higher trait-anxiety score compared to male by 1.225 (95%CI: 0.676, 5.506). Obese patients had higher 18.442 (95%CI: 14.533, 22.221) and overweight had higher 17.929 (95%CI: 15.117, 20.741) in trait-anxiety scores compared to the underweight & normal BMI group. Those ex-smokers had less than 5.747 (95%CI: 2.843, 8.651) state-anxiety score compared to the current smoker and those without the presence of accompanying had 3.111 (95%CI: 0.418, 4.248) higher state-trait score compared to those with the presence of an accompanying. Patients who had at least once in a year frequency of venepuncture had 12.662 (95%CI: 0.685, 1.459) higher in state-anxiety score compared to those who had at least once in a month. All these factors contributed to 58.5% variances of the state-anxiety score.
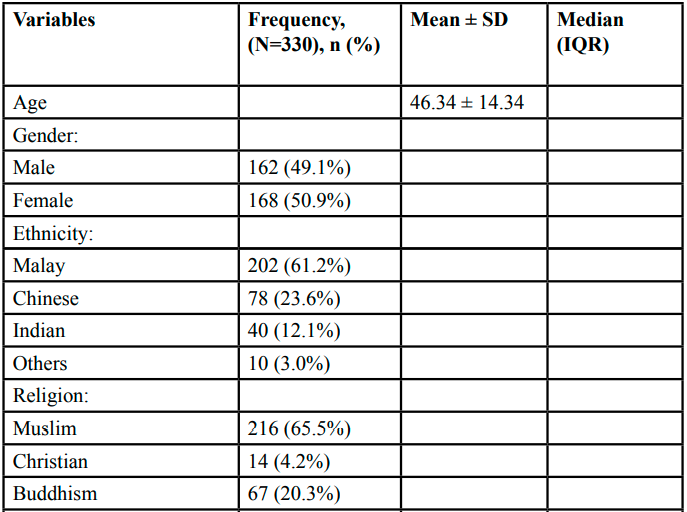
Table 5: Factor associated with Trait-Anxiety
Discussion
This study was done to determine the state and trait-anxiety of patients before the venepuncture procedure takes place among adult patient. As shown in the literature, distress to any needle procedurals can happen not only in the children group but also in the adult group of population which ranging from none, very little or severe. This may expose the patients to some psychological stress and deleterious consequences such as avoidance in seeking health care services. In the literature, there is a variation of the mean or median score for anxiety toward venepuncture studied. Our study showed that adult patients who are waiting for venepuncture procedure in phlebotomy unit had a lower anxiety score compared to other studies that measure the anxiety score for venepuncture using the same STAI Questionnaire [15]. On the other hand, our finding also is not far from the study findings from Turkey [16] on the effect of vibration on pain and anxiety during venipuncture. The control group who only had a standard venipuncture procedure without any intervention applied were reported to have the mean (SD) for state-anxiety score 23.79 ± 4.75, and there was no statistically significant difference in mean compared to the intervention group.
These average score of state and trait-anxiety in our study population may reflect the good quality of phlebotomy services provided by the phlebotomy unit to the patients. The outpatient phlebotomy unit in UiTMMC has outlined a good standard of practice to be followed to cater for patient for venepuncture. Apart from having a well-managed flow for the patients to follow, the conducive air-conditioned room as well as patients are attended by the well-trained and friendly phlebotomists who are qualified for the venepuncture added the good quality of services here. This can be supported by other studies which found that good phlebotomy experience and satisfaction will lead to low anxiety score of the patients [17]. In addition, well-managed needle procedures may reduce the venepuncture distress significantly [18].
If we compared the trait-anxiety score and state-anxiety score of our study population, the state-anxiety score was slightly higher compared to trait-anxiety score with 38.02 ± 14.25 and 36.46 ± 11.47, respectively. This is possibly contributed by patients’ worry on their exposure to pandemic Covid-19 infection during the study duration in line with Malaysia has reported the first case of Covid-19 on 25th January 2020 and up to 31st March 2020, Malaysia has faced three waves of Covid-19 infection [19].
The current study found seven factors to be significantly associated with state-anxiety score among adult patients who are waiting for venepuncture procedure in this study which are age, gender, BMI classification, educational level, smoking status, presence of accompany and frequency of venepuncture in one year. The older the patients, the higher score in state and trait-anxiety score (adj. B: 0.084 and 0.093, respectively). However, a study from United States that found age is a predictor for anxiety among young and older adults whereby young adults reported higher levels of overall health anxiety compared to older adults [20]. This is in line with other Furthermore, he also stated that older adults have a higher level of coping skills, less intolerance with uncertainty and less anxiety sensitivity which possibly explain the present study finding as well [20].
In terms of gender, our study finding was in line with other studies that reported the woman to have higher anxiety than man both in state and trait-anxiety due to the hormonal fluctuation throughout the life span. This could be exacerbated during a stressful situation [21] which can include the situation in waiting for venipuncture procedure [2]. Besides, being female has more amplification of somatic senses than the male, which makes them perceive more disturbing and intense in perceiving a somatic sensation from the venipuncture [11]. Although this study did not assess the anxiety during the procedure, however, all patients included has experienced at least once venipuncture procedure in the same setting in the past. Other than that, the relationship between gender and state-anxiety also could be due to the difference between man and woman in admitting and reporting their anxiety, rather than due to natural factor which makes the man had a lower anxiety score [22].
The current study also found that the better the past venipuncture experience rating by the patients, the lower the state and trait-anxiety scores. However, the result were not significant. This finding may reflect a good venipuncture service that phlebotomy unit has provided for the patients, which leads to a higher patient’s satisfaction. This is also supported by a few other studies which reported the significant association between patients satisfaction and lower anxiety level, which can explain our study finding [17,23]
In terms of the smoking status, ex-smoker group found to have a significantly lower state and trait-anxiety score compared to the current smoker group (adj. beta: 10.156 and 5.747, respectively). However, there were no significant difference when compared with non-smoker to smoker group. It could be due to the high-grade nicotine addiction that the current smoker has which make them have higher somatization, anxiety, depression and paranoid symptoms [24]. This study found that those patients who came accompanied has a lower state and trait-anxiety scores compared to those patients who weren’t accompanied. This is in line with some other study [25] that reported the presence of accompany should be able to provide the psychological support to the patient in a stressful situation especially in the health care setting and significantly lower the anxiety level.
This study was unable to show the significant association between history of venipuncture complication with the state-anxiety score before the venipuncture procedure. A study by McMurtry CM, Taddio [18] found the poorly managed needle procedures more likely to develop high painful memories that can lead to significant distress to the patients. Hence, it is possibly due to the well-managed needle procedures and venipuncture experience in the past masking the effect of history of venipuncture complication that patient had in our study. Furthermore, we can see that only one-third of the patients experienced minor complications in their past venipuncture such as bruises.
This study was able to show a significant relationship between the frequency of venipuncture and the state and trait-anxiety scores. This finding was consistent with a study that reported patients with frequent exposure to invasive procedures and venipuncture significantly higher pain score and distress, although their study population was among children [10]. This can be speculated as the more patient is exposed to the painful procedure, the more they can anticipate the needle stick pain, which can cause anxiety [26].
Obesity and overweight patients were found to have higher state and trait-anxiety score compare to underweight and normal patients in this study. Obesity was significantly increase the difficulty to manage patients in the emergency department [27]. Therefore, handling obese patients while venepuncture need to be done in carefully to avoid any complication such as bruises and swelling. Indirectly, these can cause more anxiety to the patients.
Some literature found a significant association between marital status and anxiety [28]; however, our study found no significant association in line with some other literature [11]. Same goes to religion factor as studies have shown that anxiety was associated with religion in which religious belief has significantly reduced anxiety or patient's stress and reduced the avoidance coping thus support in reducing stress [29]. However, our study showed other than Muslim had increased risk of state and trait-anxiety compared to Muslim, but the result was not significant. This is probably can be further studied in the future in terms of how the differences of coping mechanism between religions may affect the anxiety status of our patients since Malaysia is known for its multicultural and multireligious population.
The implication in public health
As mentioned earlier, no similar study was found primarily in Malaysia setting. Research on anxiety towards venepuncture during and after the procedure, especially among the children group, has been well established in the literature. However, it was always forgotten that anxiety could be experienced in a lifetime regardless of the time as long as there is a stressful event that may stimulate it. Therefore, having this study can be the baseline reference to the venepuncture services in every health care setting in Malaysia, particularly to give an idea of the patient's anxiety status before the venepuncture. Although our population has low anxiety status when it comes to waiting for venepuncture, it does not mean that as a health care worker, we don't have to think about it. Knowing the factors and characteristics of the patients that have a higher risk for anxiety to venepuncture can signal the phlebotomists or health care workers who deal with needle procedural that a pharmacological or pharmacological intervention can be prepared and offered to patients when needed [18]. Apart from to alleviate the fear and distress, it also may increase patient satisfaction and services in our health care setting [23]
This study has filled the research gap in terms on providing baseline information on the anxiety among adult patients who are waiting for venepuncture in the local setting. Furthermore, there were no similar studies that studied in Malaysia region. The study used a probabilistic sampling in recruiting the samples which able to eliminate the bias in samples selection. The research tool used also has a very good reliability and suitable enough to be used among the study population.
There were several limitations to this study. It was conducted in only one health care facility. Therefore, caution should be given in interpreting and applying the study findings to other health care facility in different geographic locations which may have slight differences in a phlebotomy service setting. Other than that, concerning the rating of the venepuncture services experienced and perceived by the patients in the past, there were only two questions made without using validated tools that able to measure the perception of patients on venepuncture services and experience in details. This might expose some bias to the respondents in determining their perception. Future research in qualitative study design would be beneficial to explore in detail on the perception of the patients regarding the anxiety towards venepuncture. In the current study, we did not capture the sociodemographic details and reason for not participating among the non-respondents, which may expose the study findings to respondent bias. Therefore, caution should be considered when giving interpretation for the study findings.
Conclusions
This study showed the adult patients who are waiting for venipuncture procedures in UiTMMC had a low state and trait-anxiety level. Although most of the associated found in this study were non-modifiable, perhaps, this study could instill awareness to the phlebotomists or health care workers who are dealing with needle procedurals such as venipuncture of the patients who might have a higher risk of anxiety. Any pharmacological (such as local anaesthetic) or counselling session may be applied in the service to reduce the anxiety level further among patient as this may reflect a better phlebotomy service and maintain good satisfaction among the patients.
Competing interests:
The authors declare that they have no competing interests.
List of Abbreviation
ANOVA: Analysis of Variance; BMI: Body Mass Index; IQR: Interquartile range; MLR: Multiple Linear Regression; STAI: State-Trait-Anxiety-Inventory: VIF: Variance inflation factor; UiTMMC: Universiti Teknologi MARA Medical Centre;
Acknowledgements
We would like to thank to all patients who involved in this study.
Funding:
This study was supported by self-funding.
References
Hamilton, J.G., (1995). Needle Phobia: A Neglected Diagnosis. Journal of Family Practice, 41: p. 167-169.View
Chutima R, S.T., Aurasa C, (2012). Preoperative anxiety among patients who were about to receive uterine dilatation and curettage. J Med Assoc Thai, 95: p. 1344-1395.View
Kazdin, A.E. (2019). Encyclopedia of Psychology. 30 September 2019]; Available from: https://www.apa.org/topics/anxiety/.View
Woo, A.K., (2010). Depression and Anxiety in Pain. Reviews in pain, 4(1): p. 8-12.View
Spielberger, C.D., (1966). Anxiety and Behavior: New York: Academic Press.View
Spielberger, C.D., Gorsuch, R.L., Lushene, R., Vagg, P.R., & Jacobs, G.A., (1983). State-trait anxiety inventory for adults (Malay Version): Manual, instrument, and scoring guide. Mind Garden, Incorporated.View
McLenon, J. and M.A.M. Rogers, (2019). The fear of needles: A systematic review and meta-analysis. J Adv Nurs, 75(1): p. 30-42.View
McMurtry, C.M., et al., (2016). Exposure-based Interventions for the management of individuals with high levels of needle fear across the lifespan: a clinical practice guideline and call for further research. Cogn Behav Ther, 45(3): p. 217-35.View
Tee, F.Y., C.S.L. Low, and P. Matizha, (2015). Patient Perceptions and Experience of Pain, Anxiety and Comfort during Peripheral Intravenous Cannulation in Medical Wards: Topical Anaesthesia, Effective Communication, and Empowerment. International Journal of Nursing, 5: p. 41-46.View
Bisogni S, D.C., Olivini N, Ciofi D, Giusti F, Caprilli S, Gonzalez Lopez JR, Festini F, (2014). Perception of venipuncture pain in children suffering from chronic diseases. BMC Res Notes, 7: p. 735.View
Kivrak, Y., et al., (2016). Pain perception: predictive value of sex, depression, anxiety, somatosensory amplification, obesity, and age. Neuropsychiatr Dis Treat, 12(1913-1918).View
Alireza ZF, A.A., Tayebeh NB., (2019). Comparison the effect of trained and untrained family presence on their anxiety during invasive procedures in an emergency department: A randomized controlled trial. Turk J Emerg Med, 19: p. 100-105.View
Kantartjis, M., et al., (2017). Increased Patient Satisfaction and a Reduction in Pre-Analytical Errors Following Implementation of an Electronic Specimen Collection Module in Outpatient Phlebotomy. Lab Med, 48(3): p. 282-289.View
Hashim, E., et al., (2018). Psychometric Properties of the Malay Translated Spielberger State-Trait Anxiety Inventory in Exploring Parental Anxiety. Med & Health, 13: p. 106-116.View
Valeri, B.O., et al., (2016). Neonatal Invasive Procedures Predict Pain Intensity at School Age in Children Born Very Preterm. The Clinical journal of pain., 32(12): p. 1086-1093.View
Duztepeliler, S. and Arslan, G.G., (2020). The Effect of Vibration on Pain and Anxiety During Intravenous Blood Sampling in Adults. HEAD, 17(Ek sayı): p. 10-17.View
Al-Radha, A.S.D., (2017). Impact of Anxiety on the Satisfaction of Dental Implant Patients. Journal of Prosthodontics, 28(7): p. 1-6.View
McMurtry, C.M., et al., (2016). Exposure-based Interventions for the management of individuals with high levels of needle fear across the lifespan: a clinical practice guideline and call for further research. Cogn Behav Ther, 45(3): p. 217-235.View
Shave, K., et al., (2018). Procedural pain in children: a qualitative study of caregiver experiences and information needs. BMC Pediatr, 18(324).View
Gerolimatos, L. and B. Edelstein, (2012). Predictors of health anxiety among older and young adults. International psychogeriatrics / IPA, 24: p. 1998-2008.View
Jalnapurkar, I., M. Allen, and T. Pigott, Sex Differences in Anxiety Disorders: A Review. 2018.View
Kumar, A., P.K. Dubey, and A. Ranjan, (2019). Assessment of Anxiety in Surgical Patients: An Observational Study. Anesthesia, essays and researches, 13(3): p. 503-508. View
Ibarra, A. and S. Villanueva, (2019). Evaluation of Phlebotomy-Related Anxiety, Pain and Safety in A Mexican General Hospital Using Winged Blood Collection Sets. Biomedical Journal of Scientific & Technical Research, 13(5): p. 10219-10221. View
Gülsen, A. and B. Uygur, (2018). Psychological Features of Smokers. Respiratory Care, 63(12): p. 1492.View
Gheshlaghi, P., et al., (2020). Effect of Family Presence on Pain and Anxiety Levels among Patients during Invasive Nursing Procedures in an Emergency Department. View
Raypole, C., (2020). Meet Anticipatory Anxiety, The Reason You Worry About Things That Haven't Happened Yet, in Healthline Newsletter, Healthline Media. View
Kam J and Taylor DMD, (2010). Obesity significantly increase the difficulty in patient management in the emergency department. Emerg Med Asutralas, 22(4): p. 316-323. View
Spiker, R.L., (2014). Mental Health and Marital Status. The Wiley Blackwell Encyclopedia of Health, Illness, Behavior, and Society.View
Stewart, W.C., et al., (2019). Review of the Effect of Religion on Anxiety. Int J Depress Anxiety., 2: p. 016. View