
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-164
https://doi.org/10.33790/jmhsb1100164Research Article
Retracted: Interventions for Reducing the Effects of Adverse Childhood Experiences Among Black/African American Children and Adolescents: A Systematic Review
Tywan Ajani, LCSW, M.Ed.
Robert Stempel College of Public Health and Social Work, Florida International University, United States.
Corresponding Author Details: Tywan Ajani, LCSW, M.Ed., Robert Stempel College of Public Health and Social Work, Florida International University, United States. E-mail: tajan002@fiu.edu
Received date: 30th April, 2022
Accepted date: 23th June, 2022
Published date: 25th June, 2022
Citation: Ajani, T., (2022). Interventions for Reducing the Effects of Adverse Childhood Experiences Among Black/African American Children and Adolescents : A Systematic Review. J Ment Health Soc Behav 4(1):164.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: Research demonstrates tremendous harmful effects for children and adolescents that have experienced trauma of various forms before the age of eighteen. These effects are profound as not only are they linked to current detrimental effects such as increased rates of substance abuse, early sexual activity, higher rates of depression, and suicidal ideation, but they also have shown to be damaging in adulthood. This systematic review provides an examination of interventions that reduce the effects of Adverse Childhood Experiences (ACEs) for Black/African American children and adolescents.
Methods: This study used an intervention assessment tool to determine the methodological rigor derived from the American Psychological Association on assessing interventions as the risk of bias tool. The methodological rigor was used to assess the interventions that reduce the effects of ACEs. Effect sizes for controlled trials, pre-post effect sizes, and pilot studies were calculated.
Results: This search identified a total of 1,594 studies in which 617 were screened and five were selected. The five utilized harm reduction interventions to address the effects of ACEs. All of the study participants were Black/African American children and adolescents. The effect sizes that were available ranged from medium to large. The Strong African American Families Program (SAAF) intervention had the strongest methodological rigor with a medium effect size.
Conclusion: The review suggests that the combination of individual therapy, group therapy, and psychoeducational training techniques provided positive effects on the reduction of ACE related symptoms for Black/African American children and adolescents. The randomized control trials yielded the greatest improvements from the interventions. However, the findings were few and the need for interventions for this population continue to grow.
Keywords: Adverse Childhood Experiences, Childhood Trauma, Childhood Neglect, Childhood Poverty, ACEs, Intervention, Black/ African American Children, and Adolescents
Introduction/Social Problem
Colossal gaps in racial differences in terms of economic wealth, socioeconomic conditions, health disparities, and educational attainment have been pervasive throughout American history. Social science researchers have made extraordinary attempts to experiment, examine, and to uncover the root causes of these major disparities. Despite a myriad of government, religious, civic, and non-governmental agency attempts to intervene, vast differences in social mobility among racial/ethnic continue to be pervasive in the United States.
This paper will examine effective interventions to reduce the effects of Adverse Childhood Experiences symptoms among Black/ African American children and adolescents. Among the three largest minority ethnic groups in the United States, Hispanic, Black/African American, and Asian American Pacific Islander (AAPI), the Black/ African American community have the highest rates of Adverse Childhood Experiences (ACEs). The causes of ACEs are too vast to examine within the context of this paper. However, a review of effective interventions will be discussed.
Study outcomes in the past several years have unmasked stark impacts of ACEs on the many facets of social mobility. ACEs factors have now been established, with confidence, to have long term effects on physical and mental health, educational attainment, employment and labor rates, and more. This paper will delineate a portion of the latest studies on ACEs and examine why effective interventions are needed to mitigate further obstructions of ACEs among Black/ African American children and adolescents.
Overview of Adverse Childhood Experience
Adverse Childhood Experiences commonly referred to as ACEs is a concept that was introduced to the social scientific community from a study conducted by a partnership between the Kaiser Permanente Organization and the Center for Disease Control and Prevention (CDC) agency in the 1990s. Their major findings were that more than two thirds of the participants had at least one ACE score and more than a third had a score of five or more [1] (para. 8). Their results were so alarming that it led to dozens of subsequent experiments followed by hundreds of publications.
Watt et al., [2] discusses how ACE study was the first large scale study of childhood adversity as its subsequent adult impacts. Watt et al., [2] reported that the original study included 17,337 adult respondents to a survey revealing childhood adversity issues with “toxic-stress.” This stress has been linked to a myriad of adult functioning issues ranging to chronic health conditions, cognitive impairment, educational attainment, and low salary employment. Watt et al., [2] summarized this research by delineating that “neuroscientists have elaborated that toxic-stress, either from a single significant traumatic event, or even long-term stressors such as chronic poverty, can affect children’s nervous systems and stress hormones in a way that can contribute to problems with learning, health, and behavior (p. 2).”
The original study utilized four different surveys. They were entitled Family Health History Questionnaire (male and female versions) and Health Appraisal Questionnaire (male and female versions) [1] (para. 1). These survey questions have been made available for public use by the CDC on their website entitled About the CDC- Kaiser study.
The Effects of ACEs
The studies regarding the impacts of ACEs are great in number. At least 70 publications trailed the initial ACE experiment in the 1990s. The literature is colossal on the effects of ACEs not to mention the most recent findings from studies published in the past five years. According to Watt et al., [2]
research on adverse childhood experiences (ACEs) is extensive. The original ACE study produced 70 publications and spurred hundreds of other research students. The broad conclusion of the ACE study was that the seeds of adult disease and mental illness are planted in early life experiences and must be addressed in order to substantively impact adult physical and mental health (p. 2).
ACEs are critical to understanding adult human behavior especially when it comes to practitioners treating adults for both physical and mental health issues. In addition to mental health and physical issues, ACEs have also convinced researchers to have tremendous impacts on factors of social mobility including educational attainment, labor and employment, and cognition and learning. Whether you are a clinician, medical provider, or a patient, understanding ACEs helps people to understand the “why” questions as they relate to a person’s current socioeconomic status. Sterling et al., [3] reported that “ACEs are associated with several common, chronic medical and mental health conditions and earlier mortality in adults, with a strong, graded, dose response relationship between the number of ACEs and health problems” (p. 492).
An examination of dozens and dozens of ACE related studies and experiments over the past five years have revealed that they substantial effects on brain functioning and cognition, all aspects of physical and mental health conditions, mortality and morbidity rates, and even interpersonal relationship maintenance. Lorenti et al., [4], said
altogether, negative childhood circumstances combine to determine advantages and disadvantages during childhood, and their accumulation determines the extent to which the family is able to provide material and non-material forms of capital to children. In particular, low educational attainment is consistently associated with a number of childhood disadvantages. Adverse experiences during childhood set in motion a developmental process that may negatively affect individuals during their whole lives. That is, the disablement process and the ability to work are rooted in childhood within the family (p.3)
Black/African Americans and ACEs
The effects of ACEs can be observed in every racial/ethnic group of the United States but is particularly profound among the Black/ African American population. Research has uncovered that depending on the level of trauma, ACEs can affect the entire life trajectory of a child [5]. ACEs have been linked to a broad set of social and health issues such as early mortality rates, chronic depression, suicidality, high rates of parental incarceration, and more.
The APA reported that “Adverse Childhood Experiences or ACEs are potentially traumatic events that occur in childhood, including witnessing intimate partner violence, having an impaired caregiver due to substance or mental health problems, and experiencing abuse or neglect, bullying, racism, and community violence” [5](p. 1).
As anticipated, Black/African Americans have a disproportionate ACE level compared to white/Caucasian American populations. A study by the American Psychological Association published in 2001 reported that, “research has demonstrated African American youth experience disparities in the rates of exposure to ACEs, with reports of ACEs among African American children being 33% higher than rates for white children” [5] (p. 1).
ACEs have not only been related to barriers to educational attainment but are also barriers in securing gainful employment. These items are great factors that affect wealth building and social mobility. A study by Schurer et al., [6] reported that, “we find a statistically significant association between ACEs and all economic outcomes, independent of whether we control for confounding variables or not” [6](p. 10).
Researchers are finding higher ACE scores to be correlated with Black/African Americans living in or grew up in impoverished neighborhoods. People from these communities often experience a vicious cycle of poverty and ACEs that keeps them trapped or limited in opportunities to advance economically.
This cycle is often multi-generational. One of the first studies that quantifies the impact of ACEs on social mobility reported the following. “So far, we have shown that ACEs is significantly and robustly associated with earnings and increased welfare dependence as well as subjective material poverty. We have furthermore demonstrated that neglect experiences are the key contributing factor to the significant association between ACEs and later-life economic outcomes” [6] (p. 12).
A recent sample of Black/African American and Hispanic college students revealed a connection between the students’ academic performance and their ACE score. Watt et al., [2] reported from their research findings that “Model 3 reveals that race/ethnicity moderates the impact of childhood adversity on academic performance. Results reveal that having an ACE score of 4 or more significantly reduces GPAs, but only for Hispanic and Black students, and the nature of the effect is most profound” (p. 5).
Systematic Reviews
The impacts have been examined and the need for effective interventions are imminent. There are two recent systematic reviews conducted in the past few years regarding the impact of ACEs. The study findings were related to a general population and provided suggestions for interventions but did not identify any specific ones. However, there is no systematic review that examines interventions that focus on the reduction of the effects of Adverse Childhood Experiences specifically on Black/African American children and adolescents. This study intends to provide a review of interventions for this population.
A study by Petruccelli et al., [7] conducted a systematic review regarding Adverse Childhood Experiences as associated with health outcomes. Their study results were 507 records selected for review with 96 records included in their study. There findings were applied to a general population but not specifically for children. The results are consistent with this paper’s background overview of ACEs such as higher ACE scores are parallel with higher levels of medical and/ or mental health issues. “Psychosocial/behavioral outcomes had higher odds ratio than medical outcomes with increasing ACE scale scores” [7](p. 1).
The study by Liming et al., [8] identifies similar medical outcomes associated with ACEs with that of Petruccelli’s et al., [7] study. However, they focus specifically on children up to age six. This review is very limiting as most studies on ACEs focus on adolescents and adults. Liming et al., [8] said “this review did not include studies examining children in middle childhood, young teens, or teenagers” (p. 32). Liming et al., [8] also reporting that they searched only four databases and hand selected a few others. They included 132 articles in their review and identified five to examine.
This review has tremendous restrictions as there are more than nine reputable social sciences databases that could have been utilized. Next, Liming et al., [8] made use of only four key words in their search which is very restrictive considering there are dozens of key word possibilities linked to adverse childhood experiences. On the other hand, their results are consistent with the literature reported in this paper regarding the harmful effects of ACEs on children and adolescents. “Therefore, it is likely that young children exposed to multiple ACEs are at increased likelihood to have poor foundational skills, predisposing them to low adult literacy and future educational achievement, both of which have empirical evidence of being associated with poor health out-comes” [8] (p. 331).
Methodology
Search Strategy
This study was conducted through a literature review of seven social science databases between February 21 and February 28, 2022. They include the Social Work Abstracts (EBSCO), PubMed, PsychInfo (ProQuest), Medline First Search, Campbell Systematic Reviews and (ASSIA) Applied Social Sciences Index and Abstracts (ProQuest), and the Social Services Abstracts (ProQuest). The searches focused on finding interventions of Adverse Child Experiences for Black/ African American adolescents. Research terms were selected based on common synonyms found in the Sociological Abstracts (ProQuest). The following key words were searched both separately and in various combinations.
The following terms were searched within each database using the inclusion criteria identified below.
• For condition/experiences being examined, the terms included: “adverse childhood experiences” OR “childhood trauma*” OR “childhood adversity*” OR “child*divorce” OR “child* sex abuse” OR “adolescent trauma” OR “childhood neglect” OR “child*poverty”
• For racial/ethnic identity terms, the keywords searched included the following: “Black American*” OR “African American” OR “Black” OR “Black/African American”
• Intervention search terms included the following: “intervention*” OR “therap*” OR “treat*” OR “prevention*” OR “counsel* OR “psychotherap*” OR “group work” OR “family work” OR “direct practice” OR “program*” OR “service*” OR “strateg*” OR “technique*” OR “child social services*”
• The target population keyword search terms were “adolescent*” OR “youth*” OR “minor” OR “teenager” OR “young adult” OR “child*” OR “young adult” OR “youth”
Inclusion Criteria
The inclusion criteria for this analysis included the following: • The study had to be conducted within the United States of American.
• All of the study participants are of Black/African American ethnicity under age 18.
• The study had to be identified as an intervention directly applied to the identified population.
• The intervention must be a psychosocial or behavioral health intervention
• The study publications must be peer-reviewed.
Exclusion Criteria
Studies that were omitted from this analysis included the following:
• Literature or theoretical reviews
• Primarily adult populations
• Meta-analyses
• Non-psychosocial or behavioral health-based interventions
• Macro focused interventions
• Non-Black/African American racial groups
• Publications that are not peer-reviewed
• Adult populations
Risk of Bias
The assessment of study quality and rigor standards are based on a rating benchmark drawn from the American Psychological Association on assessing interventions [9]. These include six standards: (a) randomization of sample, (b) comparison with other treatments or standard services, (c) definition of a specific problem or population, (d) use of validated and reliable outcome measures, (e) use of treatment manuals or curriculum, and (f) large sample size (i.e., more than 25 per group) [9](p. 4).
Each of the five intervention findings will be assessed by the same standards above following Lateef’s tool referred to as Assessment of Methodical Rigor. “A point was given for each standard. Studies received a score between 0 and 6—higher scores indicated a higher level of methodological rigor” (p. 4). This scale was used for both randomized control trials and non-randomized pilot studies with no control groups.
Effect Size
This paper will examine the effect sizes of each of the study’s findings to assess the outcomes and to understanding the magnitude of the interventions impact of the experiment’s participants. Lakens [10] reported that “effect sizes are the most important outcome of empirical studies. Researchers want to know whether an intervention or experimental manipulation has an effect greater than zero, or (when it is obvious an effect exists) how big the effect is” (p. 862).
To address study outcomes, Cohen’s D was used in computing effect sizes of the post treatment and/or follow up group. The criteria in determining effect size are as follows:
small (η = 0.2), medium (η = 0.5), and large (η = 0.8) effects [10]. Cohen’s D effect size equation is below. Calculations were made through an online calculator Psychometrica [11].
Findings
Overall, this systematic review identified 1,594 studies that are related to the research topic. There were 977 duplicates studies removed from the search review. A full text review of 617 studies were screened for criteria eligibility with five studies remaining for review and data extraction. Studies that were primarily theoretical, literature reviews, case studies, secondary data or meta-analyses were excluded (Figure 1).
All five studies that are included in this review are actual experimental studies, not secondary data analyses, literature reviews, case studies, or meta-analyses. All the studies participants were Black/African American with one study also including some participant parents. However, the interventions focused on the affects directed towards children and adolescents.
The experiments were conducted between 2002 and 2018 and all were done within the past 20 years from the day of this report. The studies include both randomized control trials and quasi-experimental pilot study designs. The pilot studies had the weakest scores on the assessment of methodological rigor (Table 4). This is mostly due to small sample sizes, no randomization of the study participants, and no hypothesis testing. Leon et al., [12] said that
a pilot study is not a hypothesis testing study. Safety, efficacy, and effectiveness are not evaluated in a pilot. Contrary to tradition, a pilot study does not provide a meaningful effect size estimate for planning subsequent studies due to the imprecision inherent in data from small samples. Feasibility results do not necessarily generalize beyond the inclusion and exclusion criteria of the pilot design (p. 626).
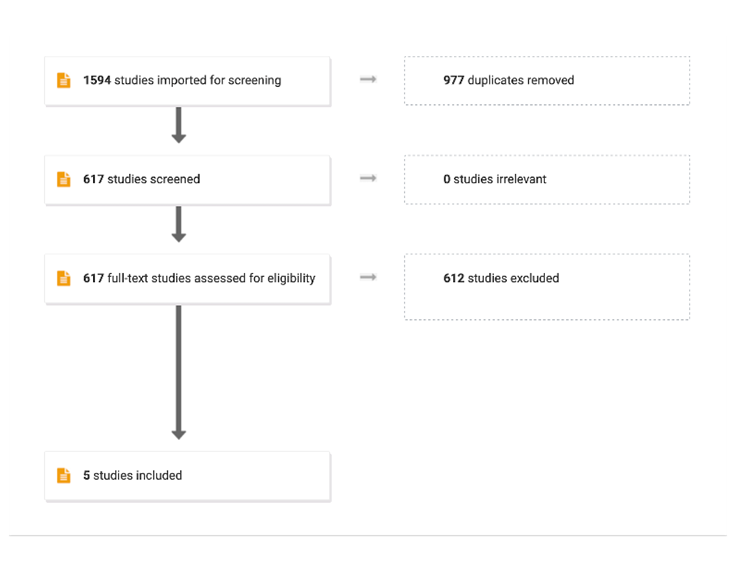
Figure 1: PRISMA Chart
The objective of this review was to identify interventions that focused on Black/African American children and adolescents. There were some findings of interventions that included Black/African American adults or interventions that addressed adolescents but with a small (less than 10%) Black/African American population. Ultimately, only five studies met the inclusion criteria.
Wrong study design means that the study was not an experiment such as a randomized control trial, a pilot study, or a quasi-experiment. Literature review means that the study was a secondary data analysis and not an actual experiment where an intervention is being tested. Wrong outcomes refer to a study that is focusing on issues that do not relate to Adverse Childhood Experiences.
The wrong patient population refers to study participants that do not meet the inclusion criteria. Theoretical studies refer to articles that focus on theoretical framework and are not actual experiments that are applying interventions. Adult populations are not part of the inclusion criteria. Wrong setting refers to a study conducted in a place of incarceration, hospital, or any other setting outside of the participant’s primary home, school, religious places of gathering, and school environments. Wrong intervention refers to an intervention that is not psychosocial or behaviorally based such as a medical intervention.
Edutainment
Allen et al., [14] conducted a pilot study with a unique intervention designed to address both cultural needs and to provide an impact on violence prevention as they relate to Adverse Childhood Experiences. They called the intervention Edutainment as a cross between education and entertainment. Edutainment included the incorporation of live theatrical plays about violence prevention followed by group therapy designed to keep the interests of these young adolescents and to make an impact on violence reduction rates. The intervention site was a community center in Philadelphia, Pennsylvania.
The study participants included 60 participants identified as Black African American between the ages of 9 and 15 with a mean age of 12.41 (Table 1). The live theatrical plays focused on violence prevention followed by subsequent group therapy facilitated by a MSW level social worker. The play ran for one hour followed by a 20-30 minute facilitated discussion [14].
This nonrandomized pilot study used a pre-posttest method in which over 80% of the participants reported exposure to violent behaviors in their communities such as “gun shots,” shootings, and stabbings. The study used several tools of measurement to measure anxiety and self-efficacy levels (Table 2). The study’s Risk of Bias is reported in Table 4. It shows that the study has a moderate to strong level of methodological of rigor (Table 4).

Table 1: Treatment and Intervention Variables
Table 2: Methodological Variables
The study participants completed a posttest nine days after the completion of the final discussion. Allen et al., [14] reported a large effect of the Edutainment intervention on the participant’s level of coping, stress, or anxiety. Additionally, the researchers reported a 23-point increase in self efficacy. The study was limited as they did not report rates of attrition nor was there a control group to provide comparisons.
Strong African American Families Program (SAAF)
Brody et al.,[15] this was a unique, collaborative experiment. This study applied the intervention called the Strong African American Families Program (SAAF). The objective of the intervention was to prevent early alcohol and substance abuse as well as early sexual activity using a multi-intervention approach. The SAAF intervention was designed with principles from the National Institute of Medicine and the Strengthening Families Program [15].
The study’s participants were 11-year-old children and their mothers or legal care givers. Participants engaged in seven consecutive weeks of meetings at community centers.
They were engaged in parent and youth skill building activities and other family training. Pre and post tests were conducted, and a control group was utilized.
The results showed that the intervention had a medium effect on the experimental group and higher levels of protective factors for the adolescents as reported in (Table 3). The overall assessment of methodological rigor was very strong with a perfect overall score (Table 4). This was the strongest study overall as it met all the inclusion criteria, was randomized, provided a control group, and met all the requirements in the rigor assessment scale in (Table 4).
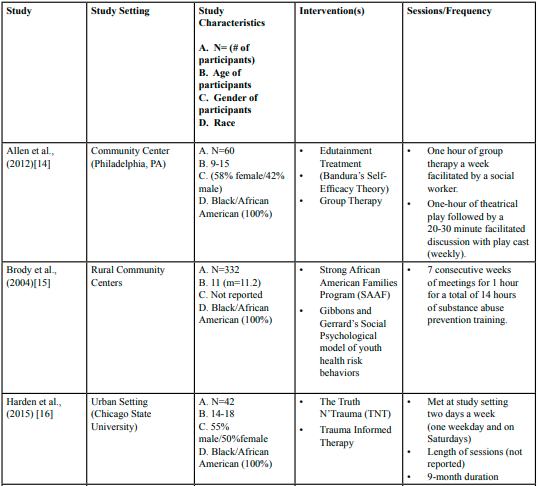
Table 3: Outcome Findings
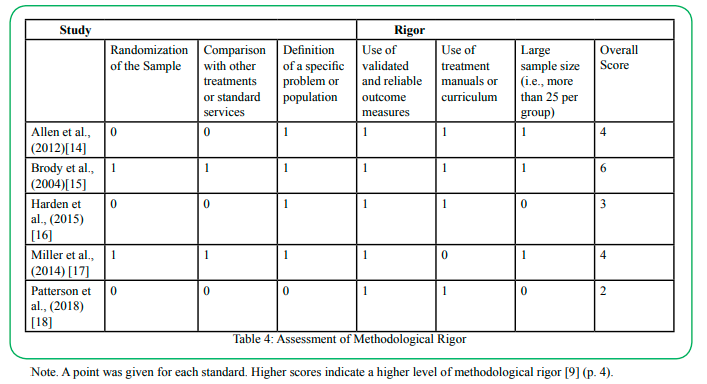
Table 4: Assessment of Methodological Rigor
The Truth N’ Trauma Project
Harden et al., [16] this was an experimental intervention applied to a Black/African American adolescents population on the South Side of Chicago. The experiment was administrated by staff from Chicago State University and the objective was to use a combined approach of Trauma Informed Therapy, Psyco Education, Theatrical Exposure, Media skills engagement, and youth research engagement called (Youth Participatory Action Research), to reduce the effects of violence and its involvement.
Forty-four adolescents participated. They were all between the ages of 14 and 18. This was a nonrandomized single subject experiment. The participants met twice a week on the campus of Chicago State University; (one weekday and on Saturdays). The participants length of sessions was not report during the program’s 9-month duration.
The results reported positive increases in multiple areas by the participants. They are identified as [16] (p. 72):
• Understanding of political issues affecting their communities
• Increased involvement in school (during the program intervention)
• Increased active involvement in community
• Increased reporting of the ability to handle future challenges of their communities.
Negative changes and/or increases from the intervention group were also identified as the following:
• Increased self-blame and critically self-evaluation
• Difficulty recognizing the good things about ones-self
• Increase in family disruption such as divorce, illness, and death
• Increase in community stressors such as gang pressure and (negative) racial experiences
Overall, the study scored three out of six on the rigor scale (Table 4). Findings were limited as there was no control group and no ability to calculate the effect size. This makes the intervention results difficult to generalize on larger population.
Family Therapy/Training
Miller et al., [17] was a randomized control trial that explored the effectiveness of family therapy and family training on children from low socioecomic status (SES). Based on the Cohen’s D effect size scale, the study intervention had a medium to large effect (Table 3) with a large sample size of 272 participant families.
The participants were between the ages of 11-19 and identified as Black/African American. The intervention was aimed at providing “nurturant-involved” parenting with less “harsh and inconsistent” parenting techniques [17]. This was executed through weekly family group sessions and individual sessions at participant’s local community center.
Post intervention follow ups were conducted both at three months and at eight years after completion of the program. Only 41% of the original participants completed the eight year follow up. The results of the last follow up were reported as the lowest among the participants that received the both the individual therapy and the nurturant-involved parenting training [17].
Overall, this was a moderate to strong level study due to it have score of four out of six on the methodological rigor scale (Table 4). The study had a large sample size, it was randomized, had a control group, and it provided two post intervention follow up tests. The intervention provided a medium to large effect on the experimental group.
Play Therapy
Patterson et al., [18] is a study that aimed at evaluating the effectiveness of applying both play and individual therapy to a child population that is currently living in poverty. The objective of the intervention was to reduce the effects of Adverse Childhood Experiences as identified as problematic behaviors, classroom performance, and reductions in anxiety [18]. All the participants identified as Black/African American and were between ages five and nine.
The intervention was a pilot study with no control group or randomization. It took place in a neighborhood after school program. The intervention was compromised of six weeks of individual therapy at one hour a week and six weeks of play therapy at one hour a week. Overall, the study reported a large effect of both interventions (play therapy) and (individual therapy) on the experimental group (Table 3). A major limitation to this study is the small sample size.
The respective study authors agree that for this experiment to be generalization to a larger population, a larger sample size with a control group will be needed. The overall rigor of the study was a two out of six. The study lacked in four categories of methodological rigor based on the American Psychological Association on assessing interventions (Table 4). This was the lowest scoring study out of the five examined.
Discussion
This study systematically reviewed psychosocial based interventions to reduce the effects of Adverse Childhood Experiences (ACEs) for children and adolescents withing the Black/African American community. Overall, this analysis is found that psychosocial based interventions had positive effects on the reported levels of ACEs. The three interventions that had the strongest methodological rigor in its study [14,15,17] were all executed through both individual and group therapy.
Three out of the five interventions were conducted through psychoeducation (Table 1 and Table 3). The participants responded well to preventative educational training regarding violence prevention, substance abuse awareness, and nurturing parenting techniques. Only two of the studies [15,17] had large enough sample sizes to provide generalizable data. Interestingly, these two studies had the highest scores on the intervention rigor scale (Table 4).
There was a good mix of settings among the studies. Two of them were in urban settings (Chicago, Illinois and Philadelphia, Pennsylvania), while the others were in rural communities providing a diverse viewpoint of the outcomes. On the other hand, there was a lack of data in four of the studies that would have provided stronger conclusions and validity. Harden et al., [16] and Patterson et al., [18] both lacked sufficient data to calculate the studies effect sizes. Harden et al., [16] and Allen et al., [14] lacked the experiment’s attrition data.
Overall, these interventions demonstrated varying levels of effectiveness in reducing symptoms of Adverse Childhood Experiences among Black/African children and adolescents. As discussed thoroughly in the Social Problem section of this paper, ACEs are at the root of most barriers to social mobility for the Black/African community. Five experimental interventions are not sufficient to provide the robust, evidenced-based data needed to equip practitioners with the tools needed to affect change on a larger scale. Future interventions experiments with complete data according to the American Psychological Association’s intervention assessment rigors described in Table 4 are needed to better treat this national plight.
Application to Social Work Practice
The harmful and negative impacts of Adverse Childhood Experiences have been discussed throughout this paper. The literature has also indicated that Black/African Americans have a disproportionally higher rate of ACEs than other U.S. based racial/ethnic groups. Ultimately, this is a social problem for many reasons, one being that the harmful effects of ACEs eventually cause tremendous negative effects in adult life such as predisposition to substance abuse, high rates of depression, high mortality, morbidity, and a host of other issues. Srivastav et al., [19] said
there is strong evidence to support the impact of ACEs across the life course as studies have found that ACEs are linked to risky health behaviors such as tobacco use, alcohol and substance misuse, and unprotected sex, which in turn increase risk for depression, h e a r t disease, cancer, substance use disorders, and ultimately, premature mortality ACEs can also affect life potential such as academic achievement, employment, and wealth, all of which are also linked to health outcomes (p. 525).
Social workers can play an instrumental role in mitigating these effects. First, social workers can continue actively searching, developing, testing, and eventually implementing interventions that reduce the harmful effects of Adverse Childhood Experiences. Social workers can also educate their client participants about ACEs and provide screening assessments to identify patients that may be at risk.
Ultimately, early detection is a key to lessening the impacts of ACEs and social workers can aid in this process. Social workers labor in a variety of settings ranging from community based mental health organizations, to hospitals, prisons, jail, schools, and more. Evans et al., [20] reports that “while the findings of the report show that the process of entering early intervention services is functioning well for most families, the results indicate that the process was not equally effective for all families, specifically for minority families” (p. 98).
Fundamentally, Black/African Americans carry a plethora of cultural differences that have shown to be a stumbling block in both seeking and receiving effective preventative treatment for ACEs. Clinical social workers and many social services agencies require training in culturally competency.
Therefore, providing culturally sensitive services to Black/ African American populations is within reach. Evans et al., [20] said “literature reviews of early intervention services suggest that services to minority families are often culturally inappropriate, resulting in a lack of suitable services for minority children” (p. 98). Social Workers often have cultural competency training that can be utilized in the development of culturally sensitive interventions for this population.
Limitations, Conclusions, and Future Research
The impact of Adverse Childhood Experiences has become an epidemic in American society as approximately 60% of the U.S. population is reporting as having at least one [6]. The rates are disproportionally higher for Black/African Americans ultimately affecting later life aspects of social mobility. Schurer et al., [6] said
digging deeper, the observed differences in net earnings by age 55 between those who experienced neglect and those who did not are almost entirely explained by differences in human capital – educational achievements and cognitive and noncognitive skills – accumulated by the beginning of mid-age (p. 2).
This problem of ACEs is affecting America’s entire societal and economic anatomy as ACEs directly impact physical and mental health, life expectancy, educational attainment, social mobility and more. These systems impact productivity rates, employment longevity, the ability to generate sustainable income which in turn affects America’s economic strength.
This systematic review has several limitations. First, the population studied is very narrow. It focused on children and adolescents of Black/African Americans. As reported earlier, ACEs has been shown to affect over one half of the United States population. The second limitation is that this review searched for interventions that were psychosocial and or behaviorally based. Adverse Childhood experiences maybe better treated as a “whole” such as from both a medical approach combined with psychosocial interventions. Srivastav et al., [19] discusses this aspect by mentioning the Socio-Ecological Model as an ideal theoretical intervention approach. “This model emphasizes the idea that health behaviors are influenced by social determinants, suggesting that public health prevention efforts are most effective when all these levels are addressed” (p. 527).
Out of 1,594 studies initially searched only five interventions were found in the past twenty years that were applied to the target population. That is very few experiments on interventions that reduce the impact of Adverse Childhood Experiences on Black/African American children. The majority of the literature reviewed in this study points to a greater need of more randomized control trials experiments to find more effective interventions that are cultural appropriate, replicable, and are generalizable. “Such notable racial disparities indicate a need to identify and develop culturally sensitive practice models to improve access and retain African American families and infants in the early intervention system” [19] (p. 98).
Another limitation to this study was that there were no samples from western United States regions. Three of the studies derived samples from rural communities in the southeastern United States, one is from the City of Philadelphia, one is from the City of Chicago. Additionally, it is worthwhile to consider cultural sensitivity regarding the ACE screening tools used to determine the ACEs level. ACEs related trauma are often linked to socioeconomic conditions. However, trauma, poverty, neglect, and what constitutes “abuse” is viewed differently across different cultures and racial/ethnic groups. This paper is limited in this context as it does not review the varying cultural aspects and views of Adverse Childhood Experiences.
Future research should include these varying cultural components. The ACEs screening tools and corresponding interventions would benefit from being culturally tailored to the racial/ethnic group that it seeks to serve. Eiser [21] said “the challenge of achieving culturally competent medical care in a multicultural society requires several different skill sets. Specific knowledge of minority communities’ culture and history is crucial to the cross-cultural clinical encounter” (p. 7).
Overall, an objective to this social problem is to intervene with the widespread and high rates of ACEs specifically within the Black/African community. This is significant as Adverse Childhood Experiences have been linked to a diverse array of factors that impede social mobility especially within the Black/African American community. Therefore, early intervention is key to reduction of these potentially long-term, harmful effects. Metzler et al., [22] said “the importance of preventing early adversity has never been clearer given the numerous studies demonstrating adverse associations with subsequent health and life opportunities that reverberate across generations” (p. 147).
Acknowledgements
This study acknowledges the instruction and guidance of Dr. Mark Macgowan, full professor and assistant Dean of the Robert Stempel School of Social Work at Florida International University.
Competing interests:
The authors declare that they have no competing interests.
References
Center for Disease Control and Prevention. (2021). Kaiser ACE Study.https://www.cdc.gov/violenceprevention/aces/about.htmlView
Watt, T. T., Hartfield, K., Kim, S., & Ceballos, N. (2021). Adverse childhood experiences contribute to race/ethnic differences in post-secondary academic performance among college students. Journal of American College Health, 1-9. https://doi.org/10.1080/07448481.2021.1947838View
Sterling, S., Chi, F., Lin, J., Padalkar, P., Vinayagasundaram, U., Iturralde, E., & Espinas, P. (2021). Physical, mental health and developmental conditions, and sociodemographic characteristics associated with adverse childhood experiences among young children in pediatric primary care. Journal of Pediatric Health Care, 35(5), 491-499.https://doi.org/10.1016/j. pedhc.2021.04.009View
Lorenti, A., Dudel, C., Hale, J. M., & Myrskylä, M. (2020). Working and disability expectancies at older ages: The role of childhood circumstances and education. Social Science Research, 91, 102447. https://doi.org/10.1016/j.ssresearch.2020.102447View
Woods-Jaeger, B. A., Hampton-Anderson, J., Christensen, K., Miller, T., O'Connor, P., & Berkley-Patton, J. (2021). School-based racial microaggressions: A barrier to resilience among African American adolescents exposed to trauma. Psychological trauma: theory, research, practice, and policy. https://doi. org/10.1037/tra0001091View
Schurer, S., Trajkovski, K., & Hariharan, T. (2019). Understanding the mechanisms through which adverse childhood experiences affect lifetime economic outcomes. Labour Economics, 61, 101743. https://doi.org/10.1016/j. labeco.2019.06.007View
Petruccelli, K., Davis, J., & Berman, T. (2019). Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis. Child abuse & neglect, 97, 104127. https://doi.org/10.1016/j.chiabu.2019.104127View
Liming, K. W., & Grube, W. A. (2018). Wellbeing outcomes for children exposed to multiple adverse experiences in early childhood: A systematic review. Child and Adolescent S o c i a l Work Journal, 35(4), 317-335. View
Lateef, H., Amoako, E. O., Nartey, P., Tan, J., & Joe, S. (2022). Black Youth and African-centered interventions: a systematic review. Research on Social Work Practice, 32(1), 3-12. https:// doi.org/10.1177/10497315211003322View
Lakens, D. (2013). Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Frontiers in psychology, 863. https://doi. org/10.3389/fpsyg.2013.00863View
Lenhard, W. & Lenhard, A. (2016). Computation of effect sizes. https://www.psychometrica.de/effect_size.html. Psychometrica. DOI: 10.13140/RG.2.2.17823.92329View
Leon, A. C., Davis, L. L., & Kraemer, H. C. (2011). The role and interpretation of pilot studies in clinical research. Journal of psychiatric research, 45(5), 626-629. https://doi.org/10.1016/j. jpsychires.2010.10.008View
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine, 151(4), 264-269.View
Allen, V. D., & Solomon, P. (2012). Educational entertainment as an intervention with Black adolescents exposed to community violence. Journal of prevention & intervention in the community, 40(4), 313-324. https://doi.org/10.1080/10852352.2012.707452View
Brody, G. H., Murry, V. M., Gerrard, M., Gibbons, F. X., Molgaard, V., McNair, L., & Neubaum-Carlan, E. (2004). The strong African American families program: Translating research into prevention programming. Child development, 75(3), 900- 917. https://doi.org/10.1111/j.1467-8624.2004.00713.xView
Harden, T., Kenemore, T., Mann, K., Edwards, M., List, C., & Martinson, K. J. (2015). The truth n’trauma project: Addressing community violence through a youth-led, trauma-informed and restorative framework. Child and Adolescent Social Work Journal, 32(1), 65-79View
Miller, G. E., Brody, G. H., Yu, T., & Chen, E. (2014). A family-oriented psychosocial intervention reduces inflammation in low-SES African American youth. Proceedings of the National Academy of Sciences, 111(31), 11287-11292.https://doi. org/10.1073/pnas.1406578111.View
Patterson, L., Stutey, D. M., & Dorsey, B. (2018). Play therapy with African American children exposed to adverse childhood experiences. International Journal of Play Therapy, 27(4), 215. https://doi.org/10.1037/pla0000080 View
Srivastav, A., Strompolis, M., Moseley, A., & Daniels, K. (2020). The empower action model: A framework for preventing adverse childhood experiences by promoting health, equity, and well-being across the life span. Health Promotion Practice, 21(4), 525-534.https://doi.org/10.1177/1524839919889355View
Evans, D. L., Feit, M. D., & Trent, T. (2016). African American parents and attitudes about child disability and early intervention services. Journal of social service research, 42(1), 96-112. https://doi.org/10.1080/01488376.2015.1081118View
Eiser, A. R., & Ellis, G. (2007). Cultural competence and the African American experience with health care: The case for specific content in cross-cultural education. Academic Medicine, 82(2), 176-183. https://doi: 10.1097/ACM.0b013e31802d92ea View
Metzler, M., Merrick, M. T., Klevens, J., Ports, K. A., & Ford, D. C. (2017). Adverse childhood experiences and life opportunities: Shifting the narrative. Children and youth services review, 72, 141-149. https://doi.org/10.1016/j.childyouth.2016.10.021 View