
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-170
https://doi.org/10.33790/jmhsb1100170Research Article
Relieving Pandemic-Related Psychological Distress: Key Protective Factors Against Mental Health Impairment
Dana Alonzo, Ph.D.
Associate Professor, Fordham University, Graduate School of Social Service Director, Suicide Prevention Research Program, 400 Westchester Avenue, West Harrison, NY 10604, United States.
Corresponding Author Details: Dana Alonzo, Ph.D., Associate Professor, Fordham University, Graduate School of Social Service Director, Suicide Prevention Research Program, 400 Westchester Avenue, West Harrison, NY 10604, United States.
Received date: 07th September, 2022
Accepted date: 11st October, 2022
Published date: 13th October, 2022
Citation: Alonzo, D., (2022). Relieving Pandemic-Related Psychological Distress: Key Protective Factors Against Mental Health Impairment. J Ment Health Soc Behav 4(2):170.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Over the two past years, mental health professionals have warned about the negative mental health consequences related to the covid pandemic. Most commonly reported are increased rates of depression, anxiety disorders, post-traumatic stress symptoms, sleep and appetite disturbance, contagion fears, frustration, burden, boredom, and suicidal behavior [1-5]. Previous resreach by our group has found that in low-resourced, high-risk communities characterized by pre-existing condition of extreme poverty, violence, and limited educational and occupational opportunities, there is a high prevalence of Persistent Pandemic-Related Distress Syndrome (Authors, in press), a condition representing on-going mental health impairment consisting of psychological distress and physical symptomatology persisting for an extended period of at least 6-months after mitigation efforts such as lockdown and social distancing restrictions were lifted and unrelated to contagion and infection fears.
However, not everyone experiences negative mental health consequences to the same degree in response to a crisis like the current global pandemic. In fact, research indicates that the majority of people show some degree of resilience in the face of adversity [6]. Resilience has been defined as a dynamic process of adaptation in the face of challenging life stressors that embodies a range of personal resources that help individuals to cope with stressful experiences and serves to reduce the negative mental health impact of exposure to traumatic life events [7,8]. Resilience may present as ‘immunity’ or stable and unaffected mental health when facing a prolonged period of adversity [9]. It may also reflect aspects of either “bouncing back”- returning to a former level of mental stability following an adverse period; or, ‘growth’- achieving a post-adversity higher level of mental functioning than experienced prior to the onset of the stressor [9].
Individual level trait factors have received the greatest attention in research to date as contributing to resilience and influencing how people react in times of adversity. For example, optimism, or the tendency to expect positive outcomes in uncertain situations has consistently been shown to contribute to adaptive outcomes, including improved psychological well-being, physical health, and coping with uncontrollable life events [10-12]. Mindfulness, or the ability to bring one's attention and awareness to present experiences along with accepting negative thoughts and feelings without judgement, is related to lower psychological distress during stressful life events [13-18]. Temperament, defined as individual differences in emotional reactivity, with strong biological underpinnings [19], has also been shown to influence resilience and/or mediate its effects on the development of psychiatric symptomatology via promotion of better or worse coping mechanisms when confronting stressors [20]. Lastly, motivation, interests, humor, talents and skills have also been shown to protect against life stressors.
However, for cultures that are not driven by Western values of individualism, such as low- and middle-income countries, relational and community level factors may play a more crucial role in contributing to resilience. In particular, the influence of family, extended family, friend, and community relationships are especially important to consider. Limited research related to relational/ community factors provides evidence for the proposition that they may serve a critical role in low-resource settings.
Social support is the most extensively researched interpersonal factor that has been explored as a protective factor against mental health distress during times of crises. Social support has been conceptualized as either emotional (reflecting a sense of affection, belonging, confidence), or instrumental (reflecting the practical help or advice one receives from others) [21]. Social support has been found to directly contribute to mental well-being and to indirectly safeguard against adverse circumstances [21-24].
Further, emotional social support, has been established as a protective factor against negative mental health consequences during previous disasters and crisis periods [25]. Some have suggested that perceived social support may be especially relevant during the current pandemic due to the prolonged shelter-in-place periods and social distancing requirements that served to increase social isolation at the onset of the pandemic [15,26-29].
Instrumental support is usually not considered a contributing factor to emotion-focused coping. However, in the context of a global pandemic associated with great uncertainty and a lack of understanding, it is likely that people may have responses and ideas similar to their peers. In such situations, turning to others might provide emotional relief [30]. Additionally, for low-resourced settings where the pandemic has been experienced as a complex emergency, practical knowledge regarding how to access scarce and limited resources may serve a critical role in coping.
Despite these studies pointing to the important role of relational and community factors in influencing mental health during times of crises such as the current pandemic, little research has examined protective factors at the relational/community level that serve as buffers to experiencing adverse mental health consequences during the current pandemic. Even more limited are studies regarding protective factors relevant for low-resource settings that can inform prevention efforts during times of future crises. This study aims to address this gap and specifically examines protective factors against mental health impairment related to the pandemic at the relational and community levels among individuals residing in high-risk marginalized low-resourced settings in Guatemala one and a half years post onset of the pandemic.
Methods
Sample and Study Design
The Covid Care Calls Program (CCC) was designed to respond to the pandemic and its complex consequences in high-risk communities in and around Guatemala City, Guatemala. The goal of the CCC was to address developing community needs including to: 1) identify main challenges related to the COVID-19 pandemic for these communities; 2) provide emotional support for people either suffering from symptoms of COVID-19 or showing psychological distress related to living through the pandemic; 3) make referrals for medical and mental health care; and, 4) prevent the spread of COVID-19 by providing education on evidence-based protective measures such as social distancing, regular hand-washing, and mask-wearing (for details see)[31].
With the approval of the appropriate Institutional Review Board and in collaboration with Hunger Relief International and International Social Work Solutions, a total of 330 individuals from 11 districts in and around Guatemala City participated in the baseline Covid Care Calls study (CCC). The study PIs designed the semi-structured interview, trained callers, and provided support and supervision to in-country staff. The calls are made by HRI-based social workers and psychology interns. Baseline surveys were conducted between June 2020 and September 2020. For the current study, the same procedure of telephone surveying was used and a random sample of 100 baseline participants were included. Calls were administered between June 2021 and July 2021.
Measures
The follow-up survey was designed by the study PIs. It was informed by qualitative feedback and quantitative data obtained during the baseline study [31-34] as well as grounded in relevant research focused on the impact of previous epidemics, such as SARS, and swine flu.
Sociodemographic Variables
Participants provided information regarding their sex, age, number of children, number of individuals in the household and their ages, and having a family member diagnosed with covid-19 during the pandemic.
Clinical variables
We assessed for 4 areas of mental health functioning including anxiety, stress, depression, and burnout that were operationalized according to evidence-based, culturally-relevant conceptualizations of illness and idioms of distress informed by prior research. All mental health items were rated on a scale of 0 to 5, where 0=none and 5=high. An overall score for each domain was derived by summing the scores on the individual items in the respective domain, with a higher score representing greater impairment.
The depression measure consisted of 6 items assessing mood including, feeling sad; thinking about not wanting to be alive; feeling hopeless; difficulty sleeping; difficulty eating; and difficulty concentrating/paying attention. The anxiety measure consisted of 4 items targeting feeling anxious; difficulty managing nerves; feeling worried about the future; and feeling worried about income. The stress measure consisted of 4 items targeting feeling overwhelmed; feeling stressed by children; feeling stressed by spouse/partner; and difficulty focusing on work/household responsibilities. The burnout measure consisted of 4 items targeting feeling burned-out/fatigued; having difficulty completing work/schoolwork; having difficulty helping children with homework; and feeling bored.
Protective Factors
Four primary areas of protection were assessed in the follow-up assessment including, interpersonal support; psychoeducation; community resources; adaptive coping. The four areas were assessed by a total of 25 items rated on a scale from 1 (not at all) to 5 (very much). A score was generated for each of the four areas by summing the scores of the individual items for that area of protection.
Interpersonal support
Participants were asked to rate the degree to which the following 6 sources social support served as protection against psychosocial distress during the pandemic: children; spouse/partner; extended family; frequent communication with family; frequent communication with friends; and, God/prayers. A higher score on this subscale reflects greater protection derived from perceived social support.
Psychoeducation
Participants were asked to rate the degree to which the following 4 types of psychoeducation served as protection against psychosocial distress during the pandemic: access to useful information on health/ health care; access to useful information on mental health/mental health care; access to useful information on financial support; and, access to useful information on employment. A higher score on this subscale reflects greater protection derived from psychoeducation.
Community Resources
Participants were asked to rate the degree to which the following 4 community-level sources of support served as protection against psychosocial distress during the pandemic: community-based service providers; schools/teachers; church; and, neighbors. A higher score on this subscale reflects greater protection derived from community resources.
Adaptive Coping
Participants were asked to rate the degree to which the following 4 sources of adaptive coping served as protection against psychosocial distress during the pandemic: participating in new activities; developing meaningful new relationships; developing new interests; and, finding new employment opportunities. A higher score on this subscale reflects greater protection derived from adaptive coping.
Data Analysis
The statistical analyses were performed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., USA). All the tests were two-tailed, with a significance level of p<0.05.
Descriptive statistics (means, standard deviations, and percentages) were used to describe the sociodemographic and clinical characteristics of the sample. bivariate analysis included correlation for continuous predictors and independent sample t-test for binary predictors.
Multivariate analyses were performed using multiple linear regressions. Main and interaction effects (unstandardized Beta coefficients) and p-values of each predictor and adjusted squares of each model are reported. All regression analyses complied with assumptions regarding variable distribution and there was no evidence for collinearity. Level of significance was set to p=.05.
We took several steps to examine protection against psychosocial distress. First, bivariate analyses using correlation for continuous predictors and independent sample t-test for binary predictors were conducted to identify variables that had significant associations with the four domains of protective factors (interpersonal support, psychoeducation, community resources, and adaptive coping). Second, we conducted separate multiple regressions models examining the four protective factor domains for their protective affect against experiencing anxiety, depression, stress, or burnout at one and a half years post onset of the pandemic, while controlling for age and gender (Model 1). A second model for each outcome was then estimated that only included variables found to be significant (p < .05) in Model 1 (Model 2). Lastly, we included interaction terms in a final model (Model 3) when significant variables in Model 2 indicated relevance in exploring effects by age, having. A sick family member, and/or gender.
Results
Participants were largely female (70%), with an average age of 35(±11.88). The majority of participants lived with family (73%). Just under 40% reported having children under the age of 18 living in the home and 21% reported having family members over 60 years old living in the home. Participants reported moderate to high levels of impairment in anxiety (average score 12.54(±5.02) out of 20) and depression (average score of 15.73(±7.99) out of 30), and low to moderate levels of stress (average score of 8.30(±4.56) out of 20) and burnout (average score of 9.17(±4.17) out of 20).
Tables 1 and 2 present the results of the bivariate analyses. No significant differences were found between groups by sex. Significant differences were found between those reporting having a family member diagnosed with Covid-19 during the pandemic and those who did not for interpersonal support, psychoeducation and adaptive coping. Individuals who reported having a family contract Covid-19 during the pandemic were more significantly more likely to report less protection in these three areas than those without a sick family member (see table 1).

Table 1. Results of T-Tests Examining Interpersonal Relationships by Sociodemographic and Clinical Characteristics
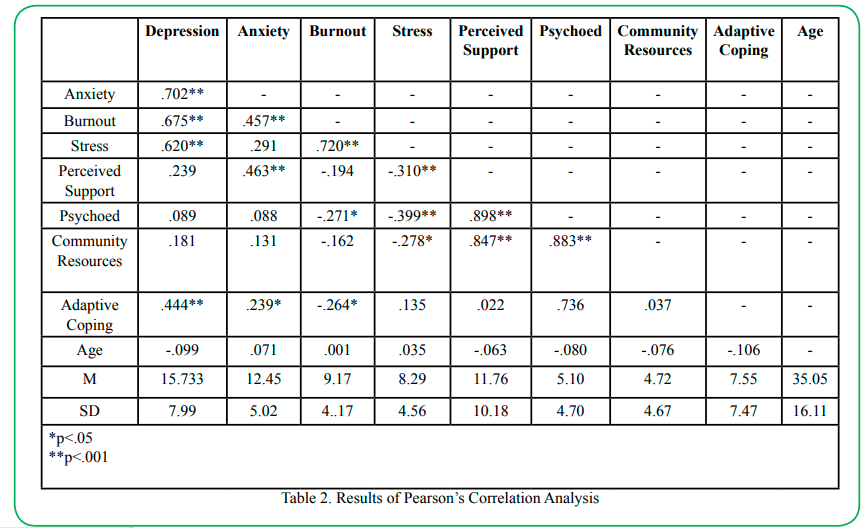
Table 2. Results of Pearson’s Correlation Analysis
Results of the correlation analysis revealed significant associations among protective factors. More specifically, strong positive associations were found between interpersonal support and psychoeducation (r=.899, p<.001), interpersonal support and community resources (r=.847, p<.001), and psychoeducation and community resources (r=.883, p<.001). Moderate positive associations were also found among the mental health variables (see table 2). No significant associations were found for age with any of the protective factors of mental health variables.
In terms of associations between the protective factors and the mental health variables, weak positive associations were found between depression and adaptive coping (r=.444, p<.001). Low to moderate associations were found between anxiety and adaptive coping (r=.239, p<.05), and anxiety and interpersonal support (r=.463, p<.001). Weak negative associations were found between burnout and adaptive coping (r=-.264, p<.05) and burn-out and psychoeducation (r=-.271, p<.001). Weak negative associations were also found between stress and interpersonal support (r=-.310, p<.001), stress and psychoeducation (r=-.399, p<.001), and stress and community resources (-.278, p<.001).
Tables 3-6 presents report on the results of the multivariate analyses examining protective factors against experiences psychosocial distress in response to the pandemic. The core sociodemographic characteristics were retained in all of the models based on their association with mental health functioning as established in previous research providing a strong rationale to include them in the analyses. As such, all models included sex, age, and having a family member diagnosed with Covid-19 during the pandemic in addition to the four domains of protective factors.
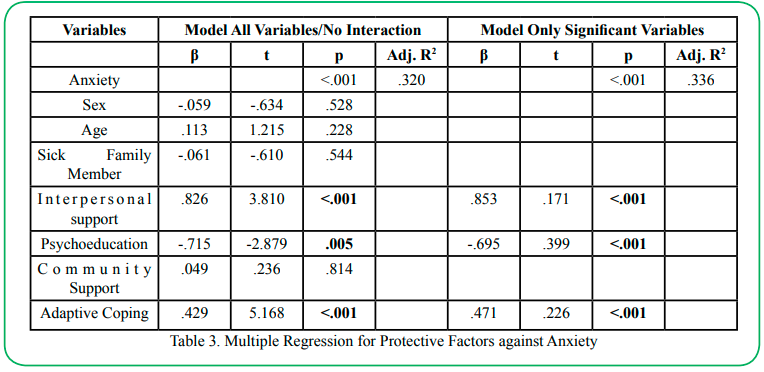
Table 3. Multiple Regression for Protective Factors against Anxiety
Table 3 reports on the results of the multiple linear regression examining interpersonal support, psychoeducation, community resources and adaptive coping protective as predictors of anxiety at one and a half years post onset of the pandemic. Results indicate that the Model 1 (including all variables) was significant (p<.001) and the model explained 32% of the variance in anxiety. Three significant main effects were found. A significant main effect was found for interpersonal support (OR=.826; p<.001) and for adaptive coping (OR=.429, p<.001), greater levels of both predicting increased anxiety, contrary to anticipated results. Only psychoeducation (OR=-.715; p.050) reflected a significant protective effect, indicating that individuals reporting greater degrees of protection from psychoeducation were 72% less likely to report anxiety. Model 2 was then estimating including only the three significant variables from Model 1. Results indicate that, overall, Model 2 was significant (p<.001) and explained 36% of the variance in anxiety. All three remained significant however once again, only psychoeducation (OR=.-695, p<.001) represented a significant protective effect, with individuals reporting greater protection from psychoeducation being approximately 70% less likely to report anxiety.
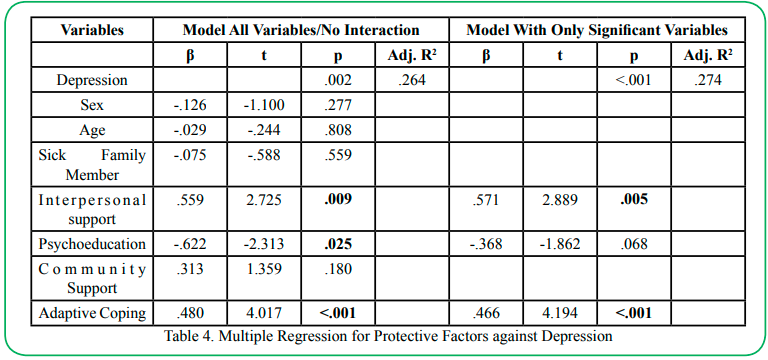
Table 4. Multiple Regression for Protective Factors against Depression
Table 4 reports on the results of the multiple linear regression examining interpersonal support, psychoeducation, community resources and adaptive coping as predictors of depression at one and a half years post onset of the pandemic. Results indicate that the Model 1 (including all variables) was significant (p=.002) and the model explained 35% of the variance in depression. A significant main effect was found for interpersonal support (OR=.559; p=.009) and for adaptive coping (OR=.480, p<.001), again reflecting risk rather than protection. Lastly, a significant main effect was found for psychoeducation (OR=-.622, p.025), which was the only variable to have a protective effect, indicating that individuals reporting greater degrees of psychoeducation were 62% less likely to report depression. Model 2 was then estimated including only the three significant variables from Model 1. Results indicate that, overall, Model 2 was significant (p<.001) and explained 31% of the variance in depression. Only interpersonal support (OR=.571, p=.005) and adaptive coping (OR=.466, p<.001) remained significant. Contrary to expectations, both indicated that greater protection in these areas predicted greater levels of depression.
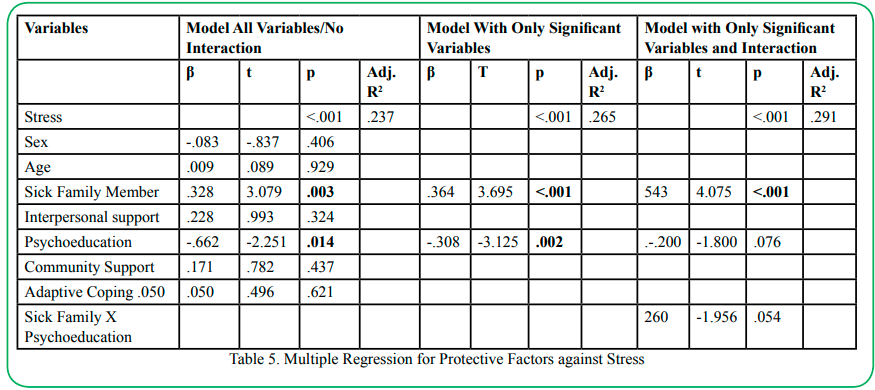
Table 5. Multiple Regression for Protective Factors against Stress
Table 5 reports on the results of the multiple linear regression examining interpersonal support, psychoeducation, community resources and adaptive coping as predictors of stress at one and a half years post onset of the pandemic. Results indicate that the Model 1 (including all variables) was significant (p<.001) and the model explained 30% of the variance in stress. A significant main protective effect was found for psychoeducation (OR=-.662; p=.014), indicating that individuals reporting a greater degree of psychoeducation were 66% less likely to report depression. Additionally, a significant main effect was found for having a family member diagnosed with Covid-19 (OR=.328, p=.003), indicating that individuals who did not have a family member contract Covid-19 were approximately 77% less likely to report stress. Model 2 was then estimated including only the two significant variables from Model 1. Results indicate that, overall, Model 2 was significant (p<.001) and explained 28% of the variance in stress. Both psychoeducation (OR=.-.308, p=.002) and having a sick family member (OR=.364, p<.001) remained significant in Model 2 and reflected protective effects against stress. Model 3 was then estimated to examine the interaction effect of having a family member diagnosed with Covid-19 and psychoeducation. Model 3 was significant (p=.003) and explained 32% of the variance in stress. However, results demonstrated no significant interaction effect and only a significant main effect for having a family member diagnosed with covid-19 (OR=.543, p<.001), indicating that those individuals who did not have a family member contract Covid-19 were 46% less likely to report stress.

Table 6. Multiple Regression for Protective Factors against Burnout
Table 6 reports on the results of the multiple linear regression examining interpersonal support, psychoeducation, community resources and adaptive coping protective as predictors of burnout at one and a half years post onset of the pandemic. Results indicate that the Model 1 (including all variables) was significant (p=.005) and the model explained 23% of the variance in burnout. A significant main effect was found for sex (OR=-.238, p=.023), indicating that females were more likely to report burnout than males. Additionally, once again, a significant main effect was found for psychoeducation (OR=-.695; p=.014), indicating that individuals reporting a greater degree of psychoeducation were more approximately 70% less likely to report burnout; and for adaptive coping (OR=.265, p=.014), indicating increased risk associated with increased adaptive coping. Model 2 was then estimated including only the three significant variables from Model 1. Results indicate that, overall, Model 2 was significant (p<.001) and explained 20% of the variance in burnout. Sex (OR=-.246, p=.019), psychoeducation (OR=.-.249, p=.017) and adaptive coping (OR=.255, p=.014) remained significant, with psychoeducation again reflecting the only protective effect. Model 3 was then estimated to examine the interaction effect of sex with psychoeducation and adaptive coping. Model 3 was significant (p=.003) and explained 15% of the variance in burnout. However, results demonstrated no significant main effects or interaction effects.
Discussion
This study aimed to examine protective factors against Covid-19 pandemic’s impact on mental health, namely anxiety, depression, stress and burnout. We explored the roles of key domains of protection (interpersonal support, psychoeducation, community resources and adaptive coping) for their effect against psychological distress one and a half years post onset of the pandemic in under-resourced communities where the pandemic has been experienced as a complex emergency. We hypothesized that higher self-reported protection across the four domains would be associated with less severe anxiety, depression, stress, and burnout. Our findings demonstrate that only psychoeducation serves a protective factor against psychological distress. To our knowledge, this is the first study to examine protective factors against mental health impairment related to the Covid-19 pandemic in low-income under-resourced settings.
The protective effect of psychoeducation has long been recognized. Research has found that appropriate communication to the general population and health and allied professionals improves awareness and understanding, and reduces distress associated with uncertainty [35]. Psychoeducation is a highly attractive form of intervention in low-income, under-resourced settings given its cost-effectiveness, ease of dissemination, and flexibility on delivery (i.e., individual, family, group; in-person and virtual; etc.). However, to date, findings regarding the efficacy of psychoeducation-based interventions hare inconsistent. Findings about the efficacy of psychoeducation are conflicting. Some studies demonstrate that psychoeducation leads better outcomes including better self-efficacy while others have documented no significant benefits related to psychoeducation (for review see) [36,37]. Our finding suggests that in the context of under-resourced highly marginalized communities where formal services are lacking or are severely diminished, psychoeducation may play a key protective role against psychological distress.
Additionally, instrumental support (reflecting practical help and/or advice), although not generally considered a core contributing factor to emotion-focused coping in non-crisis periods, may play a more important role in the context of a global pandemic characterized by great uncertainty and a lack of understanding. That is, during global crises like the current the pandemic, it is likely that individuals may have responses and ideas for managing fears, distress and uncertainty similar to their peers. In such situations, turning to others might provide emotional relief [30]. Additionally, for low-resourced settings where the pandemic has been experienced as a complex emergency, practical knowledge regarding how to access scarce and limited resources may serve a critical role in coping. Indeed, prior research has found that in low-income countries, health communications are critical for providing invaluable health and mental health information to targeted communities where formal services are not available [38,39] and for spreading word in areas where outreach in the community is lacking [39,40].
Our findings show no statistically significant relationship between community resources and protection against psychological distress. It may be that the on-going social distancing, while no longer required or strictly reinforced, may still be serving to minimize the degree of contact and interception individuals choose to have with those outside of their immediate household or extended family circle. In this context, interactions with school personnel, neighbors, and others from the wider community may not be as valued, easily accessible, and/or as helpful as they may be under other circumstances. Rather, digital technology that can deliver public mental health interventions, reduce social isolation, and promote help-seeking even while social distancing and or quarantining, may be more effective [35]. However, in under-resourced, low-income settings issues of access to stable internet and digital devices needs to be considered when implementing public health measures grounded in technology.
Further, contrary to expectations, interpersonal support was found to predict increased levels of anxiety and depression and adaptive coping was found to predict increased levels of anxiety, depression, and burnout. What might explain these counterintuitive findings? Several key issues must be considered.
First, interpersonal support, as conceptualized in the current study, reflects factors associated with emotional social support, such as a sense of affection, belonging, and or confidence, specifically in relation to children; spouse/partner; extended family; friends; and, God. We anticipated that higher levels of interpersonal support would predict less psychological distress based on prior research demonstrating perceived support as a protective factor against depression and anxiety during stressful situations [41-43]. However, it is important to consider the cultural context. It has been noted that the degree of stigma towards mental illness in Guatemala is so high that individuals are victimized and abused for simply expressing a mental health need [44,45]. Further, mental health care systems in Guatemala are inadequate and underfunded; human rights abuses often go unchallenged; and psychiatric education for physicians is insufficient, conveying the message that individuals struggling with mental health issues are not worthy of support, further perpetuating stigma. Compounding this structural stigma is the common belief in Guatemala that mental illness results from weakness and/ or immorality rather than a biological basis, leading individuals struggling with mental illness to try to hide their symptoms rather than to seek treatment [44,46]. Therefore, it may be that those individuals willing to report symptoms of anxiety and depression are those who feel secure in their support systems and therefore would be more likely to endorse symptoms of mental distress despite having interpersonal supports. As such, our findings suggest that cultural attitudes and beliefs may play an important mediating role in the relationship between perceived support and mental health outcomes.
Additionally, previous research has emphasized that social support is only protective to the degree that the recipient perceives it, and that one’s well-being in the face of a stressful event is determined by whether or not the recipient perceives the support given as sufficient [47,48] as well as the frequency of the supportive behavior [49]. As such, perceived social support is generally beneficial only when people believe their families and/or friends can provide adequate and frequent/consistent support [42,48]. Our findings may reflect that the support provided by family and friends was either insufficient for managing anxiety and depression given degree of uncertainty related to the Covid-19 pandemic or that such support was inconsistent based on ever-changing needs in response to new variants and changes to mitigation policies for managing the spread of the virus.
Next, adaptive coping as defined in this study, reflects a growth mindset in terms of participating in new activities; developing meaningful new relationships; identifying new interests; and, identifying opportunities for new types of employment. Prior research examining this type of coping, referred to it as approach coping [50,51]. Approach coping represents efforts to change the quality or perception of the stressor (in the current study, changing the pandemic from a period of loss and crisis to an opportunity to develop new interests, relationships and opportunities). This generally involves strategies such as acceptance, planning, positive reframing, and active coping (or taking steps to relieve the effects of the crisis situation) [50]. Approach coping, and the strategies associated with it, has been found to predict better mental health outcome under certain stressors (i.e., SARS) [52], but not others (i.e., natural disasters) [53], which might be extremely relevant in the context of complex emergencies, that erode the ability of individuals and communities to have hope for the future and reframe crises as opportunities. Similar to our findings, Shamblaw et al., [51] found that adaptive coping was associated with lower depression and better quality of life at the onset of the pandemic, but that the protective effects do not persist over time [51]. Further, results indicated that planning (such as identifying opportunities for new employment and new hobbies in the current study), was associated with more severe anxiety symptoms, despite being considered an adaptive strategy in pre-pandemic contexts [51]. Our findings apply the important relationship between coping strategies and mental health impairment to low-income settings. This suggests that in such settings, the impact of psychoeducation efforts could be maximized by providing information on effective long-term coping strategies for managing the current pandemic. Mindfulness skills, guided imagery, and relaxation/breathing techniques for managing symptoms of depression and anxiety may be particularly helpful in this context.
Limitations
Several methodological limitations warrant consideration. First, we focused on individuals residing in high-risk communities in a low-income country. As such, findings may not generalize the findings to individuals residing in high income countries or within high risk, low-income communities within high-income countries as their mental health profile may differ. Next, we examined mental health functioning at one and a half years post onset of the pandemic. To better understand on-going mental health impairment, additional prospective studies with longer term follow-up periods are required. Third, data was collected via participant self-report and therefore subject to recall bias. Notably, however, it is generally acknowledged that bias in the recall of adverse experiences is not a sufficient issue to invalidate studies that employ this data collection method [54].
Conclusion
The Covid-19 pandemic has resulted in disruptions in every area of life. Identifying protective factors against developing mental health impairment in the face of widespread unpredictability and uncertainty is essential for decreasing severity of anxiety, depression, stress and burnout, and for promoting mental well-being. For under-resourced settings, psychoeducation regarding how to access care and support is a key protective factor against mental health impairment. Furthermore, in the context of complex emergencies that have an immediate effect on already scarce resources at personal, community, and institutional levels, psychoeducation has the advantage of a low-cost intervention, easily transferable between communities, providing immediate support as well as sustainability over time. Further research focusing on the effectiveness of psychoeducation as well as other coping mechanisms in mitigating the negative impact of complex emergencies on mental health in low-income communities over time is needed to inform not only practice, but also mental and community healthcare policy changes and governmental funding allocation. Public mental health efforts should capitalize on the effectiveness of psychoeducation to promote strategies for managing symptoms of psychological distress and providing information regarding resources and services.
Conflict of interest:
The authors declare no conflict of interest.
References
Brooks S.K., Webster R.K., Smith L.E., Woodland L., Wessely S., Greenberg N., Rubin G.J. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet, 395(10227):912–920. doi: 10.1016/s0140- 6736(20)30460-8.View
Holmes, E. A., O'Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., ... & Bullmore, E. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry, 7(6), 547-560.View
Mazza, M. G., De Lorenzo, R., Conte, C., Poletti, S., Vai, B., Bollettini, I., ... & COVID-19 BioB Outpatient Clinic Study Group. (2020). Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain, behavior, and immunity, 89, 594-600.View
Mertens, G., Gerritsen, L., Duijndam, S., Salemink, E., & Engelhard, I. M. (2020). Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. Journal of anxiety disorders, 74, 102258View
Taylor, S., Landry, C. A., Paluszek, M. M., & Asmundson, G. J. (2020). Reactions to COVID-19: Differential predictors of distress, avoidance, and disregard for social distancing. Journal of affective disorders, 277, 94-98.View
Bonanno, G. A. (2004). Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events?. American psychologist, 59(1), 20View
Hu, T., Zhang, D., & Wang, J. (2015). A meta-analysis of the trait resilience and mental health. Personality and Individual differences, 76, 18-27.View
Kim-Cohen, J. (2007). Resilience and developmental psychopathology. Child and adolescent psychiatric clinics of North America, 16(2), 271-283.View
Ayed, N., Toner, S., & Priebe, S. (2019). Conceptualizing resilience in adult mental health literature: A systematic review and narrative synthesis. Psychology and Psychotherapy: Theory, Research and Practice, 92(3), 299-341.View
Carver, C. S., Scheier, M. F., & Segerstrom, S. C. (2010). Optimism. Clinical psychology review, 30(7), 879-889.View
Gallagher, M. W., & Lopez, S. J. (2009). Positive expectancies and mental health: Identifying the unique contributions of hope and optimism. The Journal of Positive Psychology, 4(6), 548-556.View
Gallagher, M. W., Lopez, S. J., & Pressman, S. D. (2013). Optimism is universal: Exploring the presence and benefits of optimism in a representative sample of the world. Journal of Personality, 81(5), 429-440.View
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., ... & Williams, J. M. G. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15(3), 329-342.View
Bergomi, C., Ströhle, G., Michalak, J., Funke, F., & Berking, M. (2013). Facing the dreaded: Does mindfulness facilitate coping with distressing experiences? A moderator analysis. Cognitive behaviour therapy, 42(1), 21-30.View
Conversano, C., Di Giuseppe, M., Miccoli, M., Ciacchini, R., Gemignani, A., & Orrù, G. (2020). Mindfulness, age and gender as protective factors against psychological distress during COVID-19 pandemic. Frontiers in psychology, 1900.View
Lindsay, E. K., & Creswell, J. D. (2017). Mechanisms of mindfulness training: Monitor and Acceptance Theory (MAT). Clinical psychology review, 51, 48-59.View
Nyklíček, I., & Irrmischer, M. (2017). For whom does mindfulness-based stress reduction work? Moderating effects of personality. Mindfulness, 8(4), 1106-1116.View
van Son, J., Nyklíček, I., Nefs, G., Speight, J., Pop, V. J., & Pouwer, F. (2015). The association between mindfulness and emotional distress in adults with diabetes: Could mindfulness serve as a buffer? Results from Diabetes MILES: The Netherlands. Journal of Behavioral Medicine, 38(2), 251-260.View
Moccia, L., Janiri, D., Pepe, M., Dattoli, L., Molinaro, M., De Martin, V., ... & Di Nicola, M. (2020). Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: an early report on the Italian general population. Brain, behavior, and immunity, 87, 75-79.View
Akiskal, K. K., & Akiskal, H. S. (2005). The theoretical underpinnings of affective temperaments: implications for evolutionary foundations of bipolar disorder and human nature. Journal of affective disorders, 85(1-2), 231-239.View
Grav, S., Hellzèn, O., Romild, U., & Stordal, E. (2012). Association between social support and depression in the general population: the HUNT study, a cross-sectional survey. Journal of clinical nursing, 21(1-2), 111-120.View
Gariepy, G., Honkaniemi, H., & Quesnel-Vallee, A. (2016). Social support and protection from depression: systematic review of current findings in Western countries. The British Journal of Psychiatry, 209(4), 284-293.View
McGuire, A. P., Gauthier, J. M., Anderson, L. M., Hollingsworth, D. W., Tracy, M., Galea, S., & Coffey, S. F. (2018). Social support moderates effects of natural disaster exposure on depression and posttraumatic stress disorder symptoms: Effects for displaced and nondisplaced residents. Journal of traumatic stress, 31(2), 223-233.View
Viseu, J., Leal, R., de Jesus, S. N., Pinto, P., Pechorro, P., & Greenglass, E. (2018). Relationship between economic stress factors and stress, anxiety, and depression: Moderating role of social support. Psychiatry research, 268, 102-107.View
Fuller-Iglesias, H., Sellars, B., & Antonucci, T. C. (2008). Resilience in old age: Social relations as a protective factor. Research in Human Development, 5(3), 181-193.View
Bhattacharjee, B., & Acharya, T. (2020). The COVID-19 pandemic and its effect on mental health in USA–A review with some coping strategies. Psychiatric Quarterly, 91(4), 1135-1145;View
Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. (2021). Mental Health During the First Weeks of the COVID-19 Pandemic in the United States. Front. Psychiatry, 12, 1898;View
Schug, C., Morawa, E., Geiser, F., Hiebel, N., Beschoner, P., Jerg-Bretzke, L., ... & Erim, Y. (2021). Social support and optimism as protective factors for mental health among 7765 healthcare workers in Germany during the COVID-19 pandemic: results of the VOICE study. International Journal of Environmental Research and Public Health, 18(7), 3827.View
Son, C., Hegde, S., Smith, A., Wang, X., & Sasangohar, F. (2020). Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. Journal of medical internet research, 22(9), e21279.View
Oryan, Z., Avinir, A., Levy, S., Kodesh, E., & Elkana, O. (2021). Risk and protective factors for psychological distress during COVID-19 in Israel. Current Psychology, 1-12.View
Alonzo, D., Popescu, M., Zubaroglu, P (2021). Qualitative Examination of the Mental Health Impact of Quarantine During the Covid-19 Pandemic. International Journal of Social Psychiatry, 00207640211028612.View
Alonzo, D., Popescu, M., Zubaroglu, P. (2021) The Current pandemic, a complex emergency? Mental health impacts of the COVID-19 pandemic and extended quarantine periods on highly vulnerable communities in Guatemala. International Journal of Social Psychiatry, 00207640211027212.View
Alonzo, D., Popescu, M., Zubaroglu, P. (2021). Mental Health Impact of the Covid 19 Pandemic on Parents in High Risk, Low Income Communities, International Journal of Social Psychiatry, 0020764021991896.View
Alonzo, D., Popescu, M., Zubaroglu, P. (2021). Back to ‘normal’? Mental health functioning after extended lockdown during the COVID 19 Pandemic. International Journal of Emergency Mental Health and Human Resilience, 23(8): 488.View
Campion, J. (2019). Public mental health: evidence practice and commissioning. Royal Society for Public Health.View
Rodrigues, F., Bartolo, A., Pacheco, E., Pereira, A., Silva, C. F., & Oliveira, C. (2018). Psycho-education for anxiety disorders in adults: A systematic review of its effectiveness. Journal of Forensic Psychology, 3(2), 1-5.View
Zhao, S., Sampson, S., Xia, J., & Jayaram, M. B. (2015). Psychoeducation (brief) for people with serious mental illness. Cochrane Database of Systematic Reviews, (4).View
Corley, C. D., Cook, D. J., Mikler, A. R., & Singh, K. P. (2010). Text and structural data mining of influenza mentions in web and social media. International journal of environmental research and public health, 7(2), 596-615.View
Moorhead, S. A., Hazlett, D. E., Harrison, L., Carroll, J. K., Irwin, A., & Hoving, C. (2013). A new dimension of health care: systematic review of the uses, benefits, and limitations of social media for health communication. Journal of medical Internet research, 15(4), e85.View
Adams, S. A. (2010). Revisiting the online health information reliability debate in the wake of “web 2.0”: an inter-disciplinary literature and website review. International journal of medical informatics, 79(6), 391-400.View
Lakey, B., & Orehek, E. (2011). Relational regulation theory: A new approach to explain the link between perceived social support and mental health. Psychological Review, 118(3), 482– 496.View
Panayiotou, G., & Karekla, M. (2013). Perceived social support helps, but does not buffer the negative impact of anxiety disorders on quality of life and perceived stress. Social Psychiatry and Psychiatric Epidemiology, 48(2), 283–294.View
Roohafza, H. R., Afshar, H., Keshteli, A. H., Mohammadi, N., Feizi, A., Taslimi, M., & Adibi, P. (2014). What’s the role of perceived social support and coping styles in depression and anxiety? Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences, 19(10), 944–949.View
Figueroa, C. (2014). State of Terror, States of Mind: Ladinas, Mental Health and Systems of Care, in Guatemala City. Retrieved from the University of Minnesota Digital Conservancy, https:// hdl.handle.net/11299/185181. Accessed June 1, 2021.View
Figueroa, C., Zheng, Y., & Adams, J. (2020). Beliefs About Psychological Services Among Guatemalan College Students. Journal of Multicultural Counseling and Development, 48(1), 44-57. 10.1002/jmcd.12163View
Thornicroft, G. (2006). Tackling discrimination against people with mental illness. Mental Health Foundation, London.View
Gurung, R., Sarason, B., & Sarason, I. (1997). Close personal relationships and health outcomes: A key to the role of social support. Handbook of personal relationships: Theory, research and interventions (2nd ed) Chichester, UK: Wiley, 547-573View
Özmete, E., & Pak, M. (2020). The relationship between anxiety levels and perceived social support during the pandemic of COVID-19 in Turkey. Social Work in Public Health, 35(7), 603- 616.View
Winefield CS, et al. (1992). Cloning and characterization of a cDNA encoding aspartate aminotransferase-P1 from Lupinus angustifolius root tips. Plant Physiol, 104(2):417-23. doi: 10.1104/pp.104.2.417.View
Langford et al., (2020). Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect, 26(12):1622-1629. doi: 10.1016/j.cmi.2020.07.016.View
Shamblaw, A. L., Rumas, R. L., & Best, M. W. (2021). Coping during the COVID-19 pandemic: Relations with mental health and quality of life. Canadian Psychology/Psychologie canadienne, 62(1), 92.View
Cheung, C., Chan, G. and Limayem, M. (2005) A Critical Review of Online Consumer Behavior: Empirical Research. Journal of Electronic Commerce in Organizations, 3, 1-18. https://doi.org/10.4018/jeco.2005100101 View
Glass et al., (2009). Norovirus gastroenteritis. N Engl J Med, 361(18):1776-85. doi: 10.1056/NEJMra0804575.View
Hardt, J. and Rutter, M. (2004) Validity of Adult Retrospective Reports of Adverse Childhood Experiences: Review of the Evidence. Journal of Child Psychology and Psychiatry, 45, 260- 273. http://dx.doi.org/10.1111/j.1469-7610.2004.00218.xView