
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-172
https://doi.org/10.33790/jmhsb1100172Research Article
Stigma’s Influence on Mental Health Treatment in China
Kathryne B. Brewer1*, Robin E. Gearing2, Monit Cheung2, Patrick Leung2, Wanzhen Chen3, L. Christian Carr2, Arlene Bjugstad2, & Xuesong He3
1Department of Social Work, University of New Hampshire, 55 College Road, Durham, New Hampshire,United States.
2Graduate College of Social Work, University of Houston, 3511 Cullen Boulevard, Houston, TX 77204, United States.
3School of Social and Public Administration, East China University of Science & Technology, Shanghai, China.
Corresponding Author Details: Kathryne B. Brewer, PhD, LMSW, Assistant Professor of Social Work, The University of New Hampshire, 55 College Road, Durham, NH 03824, United States.
Received date: 18th October, 2022
Accepted date: 30th November, 2022
Published date: 02nd December, 2022
Citation: Brewer, B. K., Gearing, R. E., Cheung, M., Leung, P., Chen, W., Carr, L. C., Bjugstad, A., & He, X., (2022). Stigma's Influence on Mental Health Treatment in China. J Ment Health Soc Behav 4(2):172.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Mental health problems are one of the leading causes of disability in China. Stigma acts as a barrier to mental health treatment. This research explores the influence of self-stigma and public stigma toward mental health care among Chinese adults. The study investigated which participant characteristics affect stigma toward mental health treatment, and whether participant exposure to mental health problems moderates the relationship between participant characteristics and stigma toward mental health. Five hundred participants were recruited in public areas throughout Shanghai to participate in a community survey comprised of demographic questions and standardized instruments. Findings indicate that knowing someone with a mental health problem moderates the relationship between participant characteristics (e.g., age, gender, employment status) and stigma. Also, this study found that gender and knowing someone with a mental health problem influence public stigma. Results support the inclusion of family in the treatment of mental illness at a clinical practice level in China and informs anti-stigma interventions and public awareness campaigns at a policy level.
Keywords: Stigma, China, Public Stigma, Self-Stigma, Gender, Mental Health
Introduction
The largest country in the world with one-fifth of the world’s population [1], China has experienced drastic social and economic changes over the past 30 years [1]. Research has found that Asia overall has the second-highest prevalence rate of depression worldwide [2], and in China mental health disorders are considered to be among the leading causes of disability [3]. With a 16% lifetime prevalence, approximately 231 million Chinese experience a mental health disorder [4]. Yet in China, treatment-seeking behaviors among individuals with mental health problems are low with more than 90% of people untreated [5,6].
With a rising population and drastic socioeconomic changes, China in 2004 passed the ‘686 Programme’ into law to provide support for community-based mental health care but an implementation plan was not developed until 2015 [7,8]. With the increase in national recognition and need for support, research examining public beliefs and attitudes about mental health is pressing. Further, existing research demonstrates that recognition of mental health symptoms and mental health literacy is very low throughout China [4,9,10].
Two common explanations of mental health problems have been identified: ‘traditional beliefs’ and ‘biomedical beliefs’ [11]. Traditional beliefs posit that mental health disorders are symptoms of an individual’s deficiency due to lack of morals or religion, which need to be addressed through the person’s behaviors, including taking steps to become more moral or religious [11]. In contrast, biomedical beliefs assert that mental health disorders are symptoms of biological or medical problems that need to be addressed via medical treatment [11]. A study conducted by Jiang and colleagues [12] found that the majority of Chinese participants endorsed more traditional beliefs about depression, such as it not being a ‘real disorder’ and that depression symptoms are the fault of the individual.
Mental Health Stigma in China
Stigma has long been established as a barrier to mental health treatment [13]. This research study explores two types of stigma, self-stigma and public stigma, within the Chinese context. Self-stigma refers to a persons’ identification with negative stereotypes and the assimilation of those views into their own belief systems about themselves [14]. Individuals with mental health self-stigma have internalized socio-cultural negative connotations about mental health and may denigrate themselves, believe that they are inferior, and attempt to withdraw in social situations [15]. Research has found moderate to severe levels self-stigma is highly prevalent in China [16,17]. Lam and colleagues [18] describe that while not everyone experiences mental health-related self-stigma, it is common within the Chinese collectivist culture to internalize the ideologies of those around you. Nevertheless, self-stigma is concerning as it translates directly to increased symptomology due to the increased stress associated with internalized stigmatization and decreased recovery [15,19-22]. Self-stigma is initiated and promoted through public stigma and socio-cultural beliefs.
Public stigma refers to stereotypical beliefs and attitudes toward individuals of a specific group, which are then endorsed by the greater society [23]. Public stigma adversely impacts individuals with mental health issues, causing alienation, social stress, internalized stigma, increased mental health symptoms, and staunched recovery [24,25,26]. Among Chinese adults with mental health disorders, public stigma is associated with negative emotions, poor quality of life, limited social networks, and poor functioning [27,17]. Research reveals that public stigma surrounding mental health disorders is pervasive [18,28-31]. Studies have found inconsistent results related to differences in stigmatization based on group membership, such as age, hukou status, or other sociodemographic factors [28,10,32].
Public stigma influences whether affected individuals seek treatment or care for the mental health problems they are experiencing. In China, this is compounded with the widespread collectivist stigma associated with mental health symptoms [33]. Chinese adolescents with greater perceived public stigma were less likely to seek treatment, especially for internalizing disorders [34]. However, interventions that have been successful in other countries, such as exposure and education, have been attempted in some Chinese communities with promising results [35,36]. Exposure to or familiarity with mental health issues within communities is defined as (1) formal, by way of intentional education or exposure, or (2) informal, by way of knowing someone with a mental health issue. However, having a close relationship with someone, such as a family member or close friend who has a mental health disorder has not been found to decrease stigmatization, rather individuals with close family or friends with a mental health disorder are found to endorse greater stigma [35]. This is likely due to the public stigma and face associated with mental health issues in Chinese society [18].
This research examines the influence of characteristics of individuals and groups towards mental health treatment. The current study extends the knowledge base by examining self-stigma and public stigma toward mental health care among Chinese. Specifically, the study investigated the following questions:
1. Which participant characteristics affect stigma toward mental health treatment?
2. Does participant exposure to mental health problems moderate the relationship between participant characteristics and stigma toward mental health?
Methods
Participants and Procedures
This study uses cross-sectional data from a survey conducted in Shanghai, China in 2018 (N = 500). Convenience sampling was used to recruit participants in public spaces across the Shanghai metropolitan area, such as shopping malls, libraries, public parks, and commuter bus terminals. Eligible participants included all Chinese-speaking residents over the age of 18. Participants received an incentive of 50 RMB (US$7) for their participation. Following verbal consent, participants completed a survey that included questions on participant demographics and standardized measures related to attitudes and beliefs about mental health and mental health treatment (e.g., Devaluation of Consumers, Devaluation of Consumers’ Families). Interviews were conducted by local Mandarin-speaking research assistants who received comprehensive training on measures and study procedures. This study received Institutional Review Board approval in both the United States and China from (BLINDED Universities).
Measures
Participant Characteristics
Predictor variables for this study included the following participant characteristics: gender (male/female), education, full-time employment (yes/no), income, hukou status, and spirituality. Education was measured as the highest level of education completed using eight categories ranging from “No formal education” to “Post-graduate.” Monthly income was measured in 10 increments of 1,000 RMB starting at 0-999 RMB, with 10,000 or more RMB as the highest possible category. Due to a large number of categories, both education and income were treated as continuous variables in the analysis.
China’s hukou registration system consists of two broadly recognized residency statuses—urban (non-agricultural) and rural (agricultural)—which serve to regulate internal migration and labor distribution. Hukou status also regulates multiple aspects of an individual’s life including opportunities for employment, education, and access to resources, such as health care, housing, and entitlement programs [37,38,39]. Chinese citizens inherit their initial hukou status from their parents at birth; it is possible to change from a rural to urban hukou status with considerable policy requirements. For this study, hukou status was derived from two items asking the participant to indicate their hukou status at birth (urban or rural) and their current hukou status (urban, rural, or changing from rural to urban). Based on these items participants were grouped into three categories: rural status, always urban status, or transitioned to urban status (individuals with a rural status at birth and whose current status was either urban or transitioning to urban).
Spirituality was measured through six items from the Daily Spiritual Experiences Scale [40]. Items were rated on a 6-point Likert-type scale ranging from 0 = “Never or Almost never” to 5 = “Many times a day”. The total score of the six items was used to represent spirituality in this study, on a scale of 0–30, with higher scores indicative of higher levels of spirituality.
Stigma
Stigma was modeled across two domains: public stigma and self-stigma. Public stigma was measured using a combination of the Devaluation of Consumers (DCS) and the Devaluation of Consumer’s Families scales (DCFS [41]). The DCS consists of eight items measured on a four-point Likert scale, asking participants the extent to which they agree (1 = “Strongly disagree” to 4 = “Strongly agree”) with statements about individuals with mental illness (e.g., “Most people would accept a person who once had a serious mental illness as a close friend”). The DCFS consists of seven items measured on the same four-point Likert scale about statements about families that contain an individual with mental illness (e.g., “Most people would look down on families that have a member who is mentally ill living with them”). Study analyses included psychometric analysis of this measure which is detailed in the results section.
Self-stigma was measured using the Stigma Concerns about Mental Health Care scale (SCMHC [42]). The SCMHC provides a summative score based on three items asking participants whether they agreed or disagreed with statements that they would not want to receive treatment for depression due for the following reasons: (1) “being embarrassed to talk about personal matters with others”; (2) “being afraid of what others might think”; and (3) “family members might not approve.” Study analyses included psychometric analysis of this measure which is detailed in the results section.
Familiarity with Mental Health Problems
Participants were asked three dichotomous questions regarding whether they knew anyone with mental health problems, had any friends with mental health problems, or had any family members with mental health problems. Using these questions, two grouping variables were created to examine the potential moderating role of knowing someone with mental health problems. The first variable, mental health problem exposure (yes/no), captured whether the participant indicated knowing someone with mental health problems (endorsed anyone, a friend, and/or a family member). The second variable, mental health problem proximity (yes/no), was derived as the participant indicating that they had a relationship, either friend and/or family member, with mental health problems.
Statistical Analysis
Statistical analyses were performed using R 4.0.3, including the lavaan package [43] for modeling latent variables. For the Devaluation of Consumers (DC) and Devaluation of Consumer Families (DCF) scales (four-point Likert items), maximum likelihood estimation was used, with robust standard errors and chi-square tests. For the Stigma Concerns About Mental Health Care (SCMHC) instrument, a diagonally weighted least squares (DWLS) estimator was used that also provides robust standard errors and chi-square tests, which is more appropriate for binary indicators [44]. Although DWLS estimation is also generally preferred for ordered categorical data with fewer than five points, robust maximum likelihood is also appropriate [45] and is more flexible for testing measurement invariance across groups. Missingness for the DC and DCF scales was minimal (no more than 2% per variable) and was handled via full-information maximum likelihood. There were no missing data for the SCMHC instrument once the non-responses were collapsed into “yes” responses.
Prior to fitting structural regressions, measurement models for latent variables were checked using multiple group CFA, wherein measurement equivalence/invariance (ME/I) testing was performed to ascertain the degree to which the various questionnaires performed similarly across groups [46]. Briefly, this process involves initially estimating the measurement model separately in each group, then successively imposing additional constraints (e.g., factor loadings, item intercepts) to check the equivalence of parameter estimates across groups. The validity of cross-group comparisons (e.g., latent factor means) is influenced by the degree of measurement invariance achieved.
Results
As a first step in the analysis, we conducted a psychometric evaluation of the key scales for public stigma (Devaluation of Consumers Scale, Devaluation of Consumer Families Scale) and self-stigma (Stigma Concerns about Mental Health Care Scale).
Psychometric Evaluation: Devaluation of Consumers (DC) and Devaluation of Consumer Families (DCF)
Although the original authors of the Devaluation of Consumers (DC) and Devaluation of Consumer Families (DCF) scales [41] posited a multi-factor structure for each, it appears they retained too many factors, since some factors contained only one or two indicators. Conversely, Chang et al. [47] favored a single-factor solution for the DCF, with a correction for the effects of reverse-wording. We conducted a two-factor CFA model was fit separately for each group, with the items from the DC scale specified to load onto one factor and the DCF items loading onto the second factor, and further specifying residual correlations among the reverse-worded (RW) items on each factor. In both groups, the correlation between the latent variables represented by the DC and DCF scales, respectively, exceeded .85, indicating discriminant validity is questionable [46]. In addition, all of the factor loadings for the RW items as well as items two and three from the DC scale were non-significant and/or extremely low (i.e., <.32 [48]). Accordingly, these items were dropped from further analyses.
The base model for beginning the ME/I process featured the remaining items from the DC and DCF scales loading onto a single, latent common factor. The fit of this model was marginal but was much improved after freely estimating the residual correlation between DCF items four and seven, both of which pertain to visiting people with mental illness. Although the basic factor structure and factor loadings were found to be equivalent across groups, only partial scalar invariance was supported, which is a necessary condition for comparing mean levels across groups. All regression models were re-estimated under the assumption of scalar invariance and parameter estimates and p-values were not substantively changed.
Factor variances were invariant across groups, indicating variability of the underlying latent variable was similar. Finally, because some residual variances were not invariant, it is necessary to report reliability separately for each group [46], although the estimates were similar. A model-based reliability estimate was used (ρ ̂_SEM), which overcomes often unrealistic assumptions of more traditional approaches such as coefficient α [49]. For respondents who knew someone with mental health problems, ρ ̂_SEM = .820, 95% CI [.786, .849]. For respondents who did not know someone with mental health problems, ρ ̂_SEM = .806, 95% CI [.770, .837]. Fit of the final measurement model for DC/DCF was good: χYuan-Bentler^2(58) = 78.810, p = .036; CFI = .974; TLI = .975; RMSEA = .042, 90% CI [.012, .065]; SRMR = .055. As a reference point, Hu and Bentler [50] stated adequate fit is indicated if RMSEA ≤.06, CFI/TLI ≥ .95, and SRMR ≤ .09.
Psychometric Evaluation: Stigma Concerns about Mental Health Care (SCMHC) Scale
ME/I testing revealed the instrument performed differently within each group. Regarding reliability, a model-based estimate with weighted least squares estimation is not available, so Guttman’s lambdas [51] were computed separately for each group. In both groups, the greatest lambda was λ3, which is equivalent to Cronbach’s alpha. For respondents who did not know anyone with mental health problems, α = .79, with a 95% CI [.75, .83] based on 2,000 bootstrap samples. For respondents who did know someone with mental health problems, α = .69, with a 95% CI [.61, .75] based on 2,000 bootstrap samples.
Assessing model fit for the measurement model was not useful since it was identified with only three indicators; in this case, the specified model will always perfectly reproduce the observed covariance matrix. Finally, discriminant validity with the DC/DCF items was checked by estimating the correlation between the latent variable representing self-stigma and factor scores estimated from the DC/DCF measurement model discussed previously (both latent variables were not simultaneously fit in a CFA model since different estimators were used for each model). The correlation was .352 (p < .001) among respondents who did not know anyone with mental health problems and .273 (p = .004) for those who did. The difference between these estimates did not achieve significance: χ2(1) = 1.889, p = .17.
Modeling Stigma
This study conducted a series of regression models examining predictors of stigma. The first series of analyses focused on public stigma; the second series concentrated on self-stigma. For each series, three models were examined. The first model included the full sample and was grouped by participants exposure to someone with mental health problems. The second model was also grouped by participants’ exposure to mental health problems but excluded participants who had reported experiencing their own mental health problems. The third model used the same sample as the second model but grouped participants by their proximity to mental health problems (knowing a friend or family with mental health problems versus not).
Public Stigma Regression Models
The dependent variable for this model was the combined DC/DCF latent variable described previously, which was regressed on a series of demographic indicators and spirituality. Univariate descriptive statistics for these variables are detailed in Table 1, and results for regression models of public stigma are summarized in Tables 2 and 3.
In the initial model (left panel of Table 2), the grouping scheme consisted of respondents who knew someone with mental health problems versus those who did not. Among those who did not know anyone with mental health problems, none of the predictors achieved significance. For those who did know someone with mental health problems, the indicator for female respondents achieved significance. On average, females scored 0.385 SD units higher on the public stigma latent variable compared with males. Furthermore, a Wald test indicated group membership moderated this association, representing an interaction effect between group and gender: χ2(1) = 7.687, p = .006. Overall, the model accounted for about 8% of the variance in the public stigma latent variable within the know someone with mental health problems group.
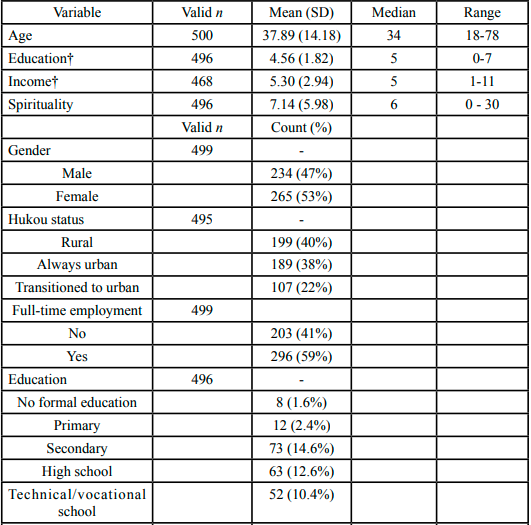
Table 1. Demographic Variables
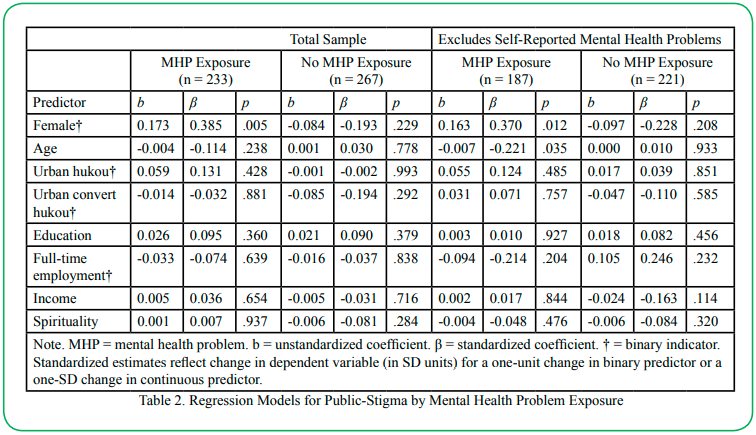
Table 2. Regression Models for Public-Stigma by Mental Health Problem Exposure
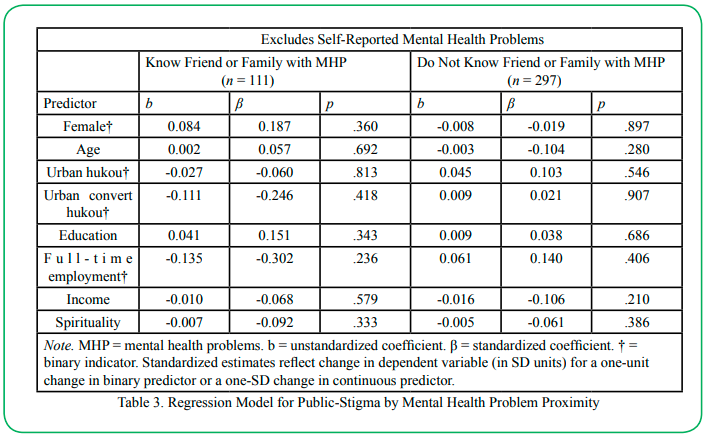
Table 3. Regression Model for Public-Stigma by Mental Health Problem Proximity
The regression was re-estimated using the same grouping scheme as above but excluded respondents who indicated they had experienced mental health problems themselves (n = 51) or who did not respond to the question (n = 41). The final measurement model described previously was verified to have an adequate fit with these cases excluded. The only change in the regression model (Table 2) was that age was significantly associated with the latent public stigma variable in the group of respondents who knew someone with mental health problems; when comparing two respondents who were one SD unit apart on age, the older respondent, on average, scored 0.221 SD units lower on public stigma. The indicator for gender remained significant in this model as well. A Wald test indicated group membershipmoderated the regression slopes for the female and age indicators: χ2(2) = 10.140, p = .006. Overall, the model explained about 11% of the variance in the latent public stigma variable within the know someone with mental health problems group.
The final regression model for public stigma involved assessing not just exposure to mental health problems, but also proximity (Table 3). The groups compared were those who had close proximity to someone with mental health problems (i.e., friend or family; n = 111) versus those respondents who did not have such a relationship (n = 297), once again excluding respondents who endorsed having mental health problems themselves. Again, the final measurement model for the latent dependent variable was checked for adequate fit prior to estimating the regression model. None of the predictors in either group achieved significance.
Self-Stigma Regression Models
A series of regression models were fit to the latent variable representing self-stigma. The modeling steps and grouping schemes proceeded as with the models for public stigma discussed previously, with the exception that income was excluded as an explanatory variable because of missing data and because it was not significant in bivariate analyses. For the first model (Table 4), none of the predictors achieved significance among respondents who knew someone with mental health problems, although the indicator for education level was close. There appears to be an inverse relationship between education and self-stigma, but this could be due to sampling error.
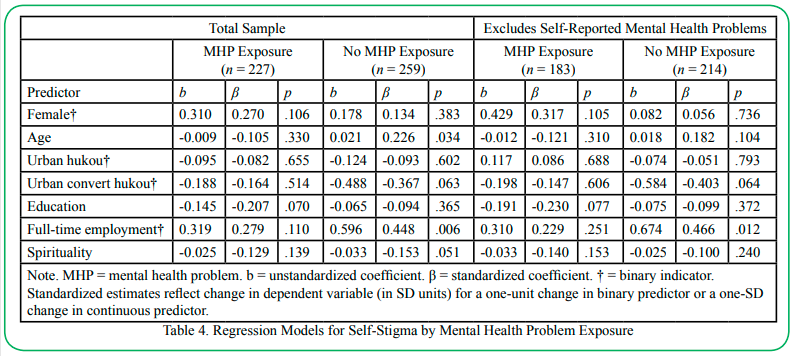
Table 4. Regression Models for Self-Stigma by Mental Health Problem Exposure
Within the group of respondents who did not know anyone with mental health problems, two predictors achieved significance and two more were close. Older respondents tended to express higher self-stigma, with a one SD unit difference in age relating to an average self-stigma score difference of 0.226 SD units. This is different from the pattern found with public stigma for the model excluding self-endorsed mental health problems, wherein older respondents who knew someone with mental health problems expressed lower public stigma. Additionally, respondents who were employed full-time tended to express higher self-stigma (about .448 SD units higher than non-full-time workers). Wald tests indicated group membership moderated the association of age and self-stigma, χ2(1) = 4.910, p = .027, but the difference in slopes for the full-time employment indicator was not significantly different across groups: χ2 (1) = 0.874, p = .350. Finally, there appears to be a trend of higher levels of spirituality being associated with lower self-stigma. Similarly, those who moved to urban areas from rural areas appear to express lower self-stigma than counterparts who remained in rural areas, but these effects could be due to sampling error. Overall, the model explained about 13% of the variance in the latent dependent variable representing self-stigma.
Results were very similar after respondents who self-reported mental health problems were excluded (right-hand panel of Table 4), with the only exceptions being age was no longer significant, and spirituality no longer approached significance. A Wald test indicated the grouping variable did not moderate the association between the full-time employment indicator and self-stigma since the difference in slopes was not significant: χ2(1) = 0.922, p = .337. For this model, the R2 in the “no exposure” group was approximately 11.4%. For the final model, comparing regression parameters based on proximity to mental health problems (see Table 5), the only predictor that achieved significance was the full-time employment indicator in the group who did not have close ties with a person with mental health problems. However, a Wald test indicated the grouping variable did not moderate this association: χ2(1) = 0.235, p = .628. The R2 was approximately 8% for respondents who did not know a friend or family member with mental health problems.
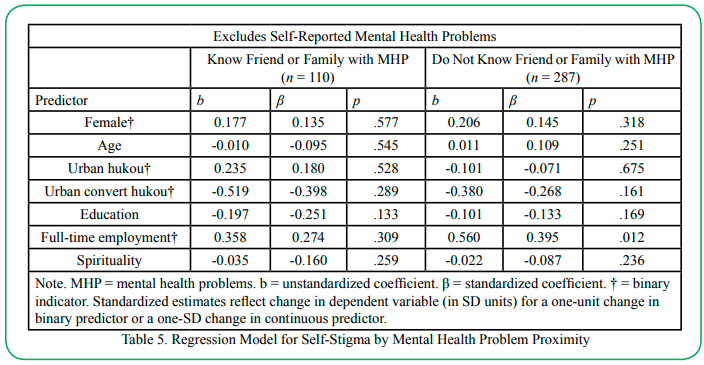
Table 5. Regression Model for Self-Stigma by Mental Health Problem Proximity
Discussion
Stigma toward mental illness remains high in China. Stigma often manifests itself at both the public level and individual level. Our study examined the role of participant characteristics on public stigma levels and self-stigma levels as well as the moderating effect of knowing someone with mental health problems on this relationship.
This research found differences in the relationship between participants’ characteristics and public stigma based on participants’ exposure to mental health problems. Specifically, participants’ exposure moderated the relationship between gender and public stigma, wherein females who knew someone with mental health problems reported higher public stigma toward mental illness. While other studies have found that gender generally does not predict public stigma [10,52], the finding from this study may indicate that gender and proximity together may influence public stigma. It is possible that females are aware of how those with a mental health disorder may be treated or perceived by the larger community. When we shifted the model to look at proximity (reporting a close relationship) rather than exposure (knowing anyone) the gender difference in public stigma levels was no longer present. This may be an indication that the closeness of the relationship rather than the presence of knowing someone is what drives this relationship. Further research is needed to clarify the role of proximity as opposed to familiarity in public stigma. The Chinese government recognized the importance of close engagement with individuals with mental illness is important for family members by passing legislation that provides subsidies to low-income families to provide direct care to their loved ones with a serious mental illness [33]. Emerging research on contact with individuals with mental illness and stigma suggests that the quality of contact may be an important target for anti-stigma interventions [53].
Corrigan and Nieweglowski [54] found a positive relationship between familiarity and public stigma. Similarly, our findings indicate that mental health proximity and awareness seem to influence stigma and stigma perceptions. Public awareness campaigns will often focus on raising awareness about mental health conditions, educating the public, and increasing contact with individuals with mental health conditions [22]. Awareness campaigns may be more effective if they focus on incorporating proximity. There may be a need to tailor such campaigns based on someone’s level of exposure to mental health problems. How the media portrays mental illness impacts how residents view people with mental illness and subsequent awareness campaigns as found in the study by Li and colleagues [10]. This is an important consideration, as recent research investigating the portrayals of mental health in Chinese mass media have found that these portrayals are overwhelmingly negative and stigmatizing [55,22]. The Chinese government has responded to mass media’s tendency to perpetuate the negative connotations associated with mental illness by creating The National Mental Health Work Plan (2015-2020 [22]). This work plan outlines requirements for media representations of mental illness to address concerns of stigma and discrimination [22].
Among those who did not self-report having mental health problems, age and gender became important for those who knew someone with mental health problems. As the age of participants increased, levels of public stigma decreased. These results add to mixed findings related to age and public stigma [29,30,52]. Li and colleagues [10] found that young adults endorsed significantly less public stigma than middle-aged adults but had similar rates of public stigma as older adults. As people who are exposed to someone with mental health problems get older, they endorse less public stigma. Whereas for people who do not know someone with a mental health problem, age does not appear to be associated with public stigma. This may reflect a perceived tolerance in the community by those who have more relational knowledge and exposure to individuals with mental health problems.
In the self-stigma models, the findings related to those who did not know someone with mental health problems. Age was related to self-stigma, with self-stigma levels increasing with older age. This relationship was moderated by knowing someone with mental health problems such that age was not related to self-stigma among those who reported knowing an individual with mental health problems. The finding that older age predicts greater mental health stigma is consistent with other research on mental health stigma in China [56,57].
Respondents who were employed full-time expressed higher self-stigma. This indicates that those with full-time employment are more likely to be concerned about being stigmatized for seeking mental health treatment. This may reflect a greater concern or fear among individuals who are employed that their employment may be negatively affected if other people knew about their mental health needs. Findings further indicate that this relationship between full-time employment and self-stigma stands on its own and is not moderated by either participants’ exposure or proximity to those with mental health problems. Consequently, further research is needed to understand the relationship between full-time employment and self-stigma.
Findings, although not statistically significant, indicate a trend of urbanity and higher levels of spirituality being associated with lower self-stigma among those who do not know someone with mental health problems. Participants who were born into a rural hukou status and changed their registration to an urban status reported lower self-stigma compared to those who remained rural. This perception may reflect that those who elect to convert to urban hukou perceive mental health needs in a more positive light. Alternatively, as the process of changing hukou status is complex and difficult this difference may indicate a combination of socio-economic factors, such as job, income, education, that may facilitate this change in status. This finding contributes to the research that hukou status is related to mental health stigma [36,58]; however, the direction of this relationship is mixed within the current literature [10,36]. It is likely that factors such as access, income, and education contribute to the differences among individuals of varying hukou statuses [59], thus continued research in this area is important for deconstructing these intersectional factors.
The relationship between spirituality and self-stigma was only found among those who did not know someone with mental health problems and when those who self-reported having mental health problems were present. While the research on spirituality and mental health in China remains scant, the studies that have been conducted have found that, unlike in many western societies, religiosity does not necessarily predict better mental health [60,61], rather religiosity in China has been associated with a higher prevalence of mental health conditions [62]; however, it is suggested that this link may be due to individuals with mental health conditions actively seeking out religion rather than religion causing mental health symptoms [62]. This is compounded with the fact that China is home to multiple ethnic groups with substantially different religious practices (i.e., Han, Hiu). Emerging research demonstrates significant variance in the link between mental health, stigma, and religiosity between these two ethnic groups based on their religious affiliations and governmental restrictions [58,61,62]. As China continues to experience a series of cultural changes regarding religion, further research is recommended in this area.
Study Limitations
Although participants were recruited across several public places across the greater Shanghai metropolitan area, this convenience sampling approach limits generalization. Overall, the study sample was comparable to the population on multiple characteristics, including average age, employment rates, hukou status, and extreme poverty. However, participants differ from the larger Chinese population in terms of gender balance (sample: 53% female; population: 49% female), Hukou status (sample: 62% urban; population: 60% urban) and level of education (sample: 42% college degree; population: 22% college degree), limiting generalizability. Finally, across the sample, 47% of participants reported knowing someone with mental health problems. This number may reflect under-reporting and is a point for future research. Participant demographics account for a portion of the variation in public stigma, but a notable portion is left unexplained by these models. Future studies should also examine other factors that may account for differences in stigma levels. Finally, it is recommended to expand research to examine stigma in rural areas.
Conclusion
Stigma is a barrier to engaging in treatment [34,54,63,64]. Building on the established association between stigma and help-seeking behaviors [28], this study examined the self-stigma and public stigma toward mental health care among Chinese individuals, and the moderating effect of knowing someone with a mental health problem. This study highlights that gender and proximity together influence public stigma, most notably the closeness of the relationship rather than the presence of knowing someone seems to be driving this relationship. Findings may support the inclusion of family in the treatment of mental illness at a clinical practice level in China, and also inform the targeting of anti-stigma interventions and public awareness campaigns at a policy level.
Interestingly, findings indicate that as the age of participants increased their public stigma decreased. While other research has found the association of age and stigma mixed [29,30,52], results may highlight that public stigma is a more nuanced phenomenon that may be influenced by experience and tolerance. Also, the study found that participants who were employed full-time expressed higher self-stigma. Consequently, interventions designed to address public stigma and self-stigma and to overcome the barrier to stigma to engaging and accessing mental health treatment may need to be more nuanced across demographics, such as age, gender, and employment.
Competing interest:
The author declares that they have no competing interests.
References
World Bank. (2019). Population total: China. https://data. worldbank.org/indicator/SP.POP.TOTL?locations=CNView
Lim, G. Y., Tam, W. W., Lu, Y., Ho, C. S., Zhang, M. W., & Ho, R. C. (2018). Prevalence of depression in the community from 30 countries between 1994 and 2014. Scientific reports, 8(1), 1-10. https://doi.org/https://doi.org/10.1038/s41598-018- 21243-x View
Phillips, M. R., Zhang, J., Shi, Q., Song, Z., Ding, Z., Pang, S., Li, X., Zhang, Y., & Wang, Z. (2009). Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–05: An epidemiological survey. The Lancet, 373(9680), 2041-2053. https://doi.org/https://doi.org/10.1016/ S0140-6736(09)60660-7View
Huang, D., Yang, L. H., & Pescosolido, B. A. (2019). Understanding the public’s profile of mental health literacy in China: A nationwide study. BMC psychiatry, 19(1), 1-12. https:// doi.org/https://doi.org/10.1186/s12888-018-1980-8View
Chen, J., Xu, D., & Wu, X. (2019). Seeking help for mental health problems in Hong Kong: The role of family. Administration and Policy in Mental Health and Mental Health Services Research, 46(2),220-237. https://doi.org/https://doiorg.ezproxy.lib. uh.edu/10.1007/s10488-018-0906-6View
Yin, H., Wardenaar, K. J., Xu, G., Tian, H., & Schoevers, R. A. (2019). Help-seeking behaviors among Chinese people with mental disorders: A cross-sectional study. BMC psychiatry, 19(1), 1-12. https://doi.org/https://doi.org/10.1186/s12888-019- 2316-z View
Good, B. J., & Good, M.-J. D. (2012). Significance of the 686 Program for China and for global mental health. Shanghai archives of psychiatry, 24(3), 175. https://doi.org/https://doi. org/10.3969/j.issn.1002-0829.2012.03.008View
Liang, D., Mays, V. M., & Hwang, W.-C. (2018). Integrated mental health services in China: Challenges and planning for the future. Health policy and planning, 33(1), 107-122. https:// doi.org/https://doi.org/10.1093/heapol/czx137 View
Li, J., Zhang, M.-m., Zhao, L., Li, W.-q., Mu, J.-l., & Zhang, Z.-h. (2018). Evaluation of attitudes and knowledge toward mental disorders in a sample of the Chinese population using a web-based approach. BMC psychiatry, 18(1), 1-8. https://doi. org/https://doi.org/10.1186/s12888-018-1949-7View
Loo, P. W., Wong, S., & Furnham, A. (2012). Mental health literacy: A crosscultural study from Britain, Hong Kong and Malaysia. AsiaPacific Psychiatry, 4(2), 113-125. https://doi. org/https://doi.org/10.1111/j.1758-5872.2012.00198.xView
Stefanovics, E., He, H., Ofori-Atta, A., Cavalcanti, M. T., Neto, H. R., Makanjuola, V., Ighodaro, A., Leddy, M., & Rosenheck, R. (2016). Cross-national analysis of beliefs and attitude toward mental illness among medical professionals from five countries. Psychiatric Quarterly, 87(1), 63-73. https://doi.org/https://doi. org/10.1007/s11126-015-9363-5View
Jiang, Y., Bogner, H. R., Wang, X., Wang, J., Zhu, T., Conwell, Y., & Chen, S. (2018). Primary care patient beliefs and help-seeking preferences regarding depression in China. Psychiatry Research, 269, 1-8. https://doi.org/https://doi.org/10.1016/j. psychres.2018.08.031 View
Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., Morgan, C., Rüsch, N., Brown, J. S., & Thornicroft, G. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychological medicine, 45(1), 11-27. https://doi.org/10.1017/S0033291714000129View
Corrigan, P. W., & Rao, D. (2012). On the self-stigma of mental illness: Stages, disclosure, and strategies for change. The Canadian Journal of Psychiatry, 57(8), 464-469.View
Livingston, J. D., & Boyd, J. E. (2010). Correlates and consequences of internalized stigma for people living with mental illness: A systematic review and meta-analysis. Social science & medicine, 71(12), 2150-2161. https://doi.org/https:// doi.org/10.1016/j.socscimed.2010.09.030View
Ran, M.-S., Zhang, T.-M., Wong, I. Y.-L., Yang, X., Liu, C.-C., Liu, B., Luo, W., Kuang, W.-H., Thornicroft, G., & Chan, C. L.-W. (2018). Internalized stigma in people with severe mental illness in rural China. International Journal of Social Psychiatry, 64(1), 9-16. https://doi.org/https://doi. org/10.1177/0020764017743999 View
Young, D. K.-W., & Ng, P. Y.-N. (2016). The prevalence and predictors of self-stigma of individuals with mental health illness in two Chinese cities. International Journal of Social Psychiatry, 62(2), 176-185. https://doi.org/https://doi. org/10.1177/0020764015614596View
Lam, T. P., & Sun, K. S. (2014). Stigmatizing opinions of Chinese toward different types of mental illnesses: A qualitative study in Hong Kong. The International Journal of Psychiatry in Medicine, 48(3), 217-228. https://doi.org/https://doi. org/10.2190/PM.48.3.fView
Chan, K. K. S., & Fung, W. T. W. (2019). The impact of experienced discrimination and self-stigma on sleep and health-related quality of life among individuals with mental disorders in Hong Kong. Quality of Life Research, 28(8), 2171-2182. https://doi.org/10.1007/s11136-019-02181-1View
Fung, K. M., Tsang, H. W., Corrigan, P. W., Lam, C. S., & Cheng, W.-m. (2007). Measuring self-stigma of mental illness in China and its implications for recovery. International Journal of Social Psychiatry, 53(5), 408-418. https://doi.org/https://doi. org/10.1177/0020764007078342View
Link, B. G., Struening, E. L., Neese-Todd, S., Asmussen, S., & Phelan, J. C. (2001). Stigma as a barrier to recovery: The consequences of stigma for the self-esteem of people with mental illnesses. Psychiatric Services, 52(12), 1621-1626. https://doi.org/https://doi.org/10.1176/appi.ps.52.12.1621View
Zhang, Z., Sun, K., Jatchavala, C., Koh, J., Chia, Y., Bose, J., Li, Z., Tan, W., Wang, S., & Chu, W. (2020). Overview of stigma against psychiatric illnesses and advancements of anti-stigma activities in six Asian societies. International Journal of Environmental Research and Public Health, 17(1), 280. https:// doi.org/https://doi.org/10.3390/ijerph17010280View
Corrigan, P. W., & Watson, A. C. (2002). Understanding the impact of stigma on people with mental illness. World psychiatry, 1(1), 16.View
Link, B. G., & Phelan, J. C. (2001). Conceptualizing stigma. Annual review of Sociology, 363-385. https://doi.org/https://doi. org/10.1146/annurev.soc.27.1.363View
Pescosolido, B. A. (2013). The public stigma of mental illness: What do we think? What do we know? What can we prove? Journal of Health and Social behavior, 54(1), 1-21. https://doi. org/https://doi.org/10.1177/0022146512471197View
Vogel, D. L., Bitman, R. L., Hammer, J. H., & Wade, N. G. (2013). Is stigma internalized? The longitudinal impact of public stigma on self-stigma. Journal of counseling psychology, 60(2), 311. https://doi.org/https://doi.org/10.1037/a0031889View
Chien, W.-T., Yeung, F. K., & Chan, A. H. (2014). Perceived stigma of patients with severe mental illness in Hong Kong: Relationships with patients’ psychosocial conditions and attitudes of family caregivers and health professionals. Administration and Policy in Mental Health and Mental Health Services Research, 41(2), 237-251. https://doi.org/https://doi. org/10.1007/s10488-012-0463-3View
Gearing, R. E., Chen, W., Brewer, K. B., Leung, P., Cheung, M., Carr, L. C., Gomez, G. R., Powell, K., & He, X. (2022). Examining public stigma of schizophrenia in China. China Journal of Social Work, 1-18. https://doi.org/10.1080/1752509 8.2022.2079164View
Liu, L., Chen, X.-l., Ni, C.-p., Yang, P., Huang, Y.-q., Liu, Z.-r., Wang, B., & Yan, Y.-p. (2018). Survey on the use of mental health services and help-seeking behaviors in a community population in Northwestern China. Psychiatry Research, 262, 135-140. https://doi.org/https://doi.org/10.1016/j.psychres.2018.02.010View
Yang, F., Yang, B. X., Stone, T. E., Wang, X. Q., Zhou, Y., Zhang, J., & Jiao, S. F. (2020). Stigma towards depression in a community-based sample in China. Comprehensive Psychiatry, 97, 152152. https://doi.org/https://doi.org/10.1016/j. comppsych.2019.152152View
Yang, L. H., & Kleinman, A. (2008). ‘Face’and the embodiment of stigma in China: The cases of schizophrenia and AIDS. Social science & medicine, 67(3), 398-408. https://doi.org/https://doi. org/10.1016/j.socscimed.2008.03.011View
ShiJie, F., HongMei, G., Li, W., BinHong, W., YiRu, F., Gang, W., & TianMei, S. (2017). Perceptions of stigma and its correlates among patients with major depressive disorder: A multicenter survey from China. AsiaPacific Psychiatry, 9(3), e12260. https://doi.org/https://doi.org/10.1111/appy.12260View
Yu, Y., Zhou, W., & Xiao, S. (2018). China’s reward policy for family care of persons with serious mental illness. Psychiatric Services, 69(12), 1210-1211. https://doi.org/https://doi. org/10.1176/appi.ps.201800114View
Chen, H., Fang, X., Liu, C., Hu, W., Lan, J., & Deng, L. (2014). Associations among the number of mental health problems, stigma, and seeking help from psychological services: A path analysis model among Chinese adolescents. Children and Youth Services Review, 44, 356-362. https://doi.org/https://doi. org/10.1016/j.childyouth.2014.07.003View
Xu, X., Li, X.-M., Zhang, J., & Wang, W. (2018). Mental health-related stigma in China. Issues in Mental Health Nursing, 39(2), 126-134. https://doi.org/https://doi.org/10.1080/01612840.2017 .1368749 View
Xu, Z., Rüsch, N., Huang, F., & Koesters, M. (2017). Challenging mental health related stigma in China: Systematic review and meta-analysis. I. Interventions among the general public. Psychiatry Research, 255, 449-456. https://doi.org/ https://doi.org/10.1016/j.psychres.2017.01.008View
Boffy-Ramirez, E., & Moon, S. (2018). The role of China’s household registration system in the urban-rural income differential. China Economic Journal, 11(2), 108-125. https:// doi.org/https://doi.org/10.1080/17538963.2018.1453103View
Zhou, S., & Cheung, M. (2017). Hukou system effects on migrant children’s education in China: Learning from past disparities. International social work, 60(6), 1327-1342. https:// doi.org/https://doi.org/10.1177/0020872817725134 View
Zhu, Y., & Österle, A. (2017). Rural-urban disparities in unmet long-term care needs in China: The role of the hukou status. Social science & medicine, 191, 30-37. https://doi.org/https:// doi.org/10.1016/j.socscimed.2017.08.025View
Underwood, L. G., & Teresi, J. A. (2002). The Daily Spiritual Experience Scale: Development, theoretical description, reliability, exploratory factor analysis, and preliminary construct validity using health-related data. Annals of behavioral medicine, 24(1), 22-33. https://doi.org/https://doi.org/10.1207/ S15324796ABM2401_04 View
Struening, E. L., Perlick, D. A., Link, B. G., Hellman, F., Herman, D., & Sirey, J. A. (2001). Stigma as a barrier to recovery: The extent to which caregivers believe most people devalue consumers and their families. Psychiatric Services, 52(12), 1633-1638. https://doi.org/https://doi.org/10.1176/appi. ps.52.12.1633 View
Interian, A., Ang, A., Gara, M. A., Link, B. G., Rodriguez, M. A., & Vega, W. A. (2010). Stigma and depression treatment utilization among Latinos: Utility of four stigma measures. Psychiatric Services, 61(4), 373-379. https://doi.org/10.1176/ ps.2010.61.4.373 View
Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of statistical software, 48, 1-36. http://www. jstatsoft.org/v48/i02/View
Beauducel, A., & Herzberg, P. Y. (2006). On the performance of maximum likelihood versus means and variance adjusted weighted least squares estimation in CFA. Structural Equation Modeling, 13(2), 186-203. https://doi.org/https://doi. org/10.1207/s15328007sem1302_2View
Bandalos, D. L. (2014). Relative performance of categorical diagonally weighted least squares and robust maximum likelihood estimation. Structural Equation Modeling, 21(1), 102-116. https://doi.org/https://doi.org/10.1080/10705511.201 4.859510View
Brown, T. A. (2015). Confirmatory factor analysis for applied research. Guilford publications.View
Chang, C.-C., Su, J.-A., Chang, K.-C., Lin, C.-Y., Koschorke, M., & Thornicroft, G. (2018). Perceived stigma of caregivers: Psychometric evaluation for Devaluation of Consumer Families Scale. International journal of clinical and health psychology, 18(2), 170-178. https://doi.org/https://doi.org/10.1016/j. ijchp.2017.12.003View
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (Sixth ed.). Pearson Education.View
Raykov, T., & Marcoulides, G. A. (2011). Introduction to psychometric theory. Routledge.View
Hu, L. t., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1-55. https://doi.org/https://doi.org/10.1080/10705519909540118View
Sijtsma, K. (2009). On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. psychometrika, 74(1), 107-120. https://doi.org/https://doi.org/10.1007/s11336-008-9101-0View
Yin, H., Wardenaar, K. J., Xu, G., Tian, H., & Schoevers, R. A. (2020). Mental health stigma and mental health knowledge in Chinese population: A cross-sectional study. BMC psychiatry, 20(1), 1-10. https://doi.org/https://doi.org/10.1186/s12888-020- 02705-xView
Ran, M.-S., Peng, M.-M., Yau, Y. Y., Zhang, T.-M., Li, X.- H., Wong, I. Y. L., Ng, S., Thornicroft, G., Chan, C. L.-W., & Lu, L. (2022). Knowledge, contact and stigma of mental illness: Comparing three stakeholder groups in Hong Kong. International Journal of Social Psychiatry, 68(2), 365-375. https://doi.org/https://doi.org/10.1177/0020764021997479View
Corrigan, P. W., & Nieweglowski, K. (2019). How does familiarity impact the stigma of mental illness? Clinical Psychology Review, 70, 40-50. https://doi.org/10.1016/j. cpr.2019.02.001View
Duan, X. J. (2018). Research on media images of mental patients in internet media analysis of related reports based on People's Daily Online and Tencent Network.
Wang, X. Q., Petrini, M. A., & Morisky, D. E. (2017). Predictors of quality of life among Chinese people with schizophrenia. Nursing & health sciences, 19(2), 142-148. https://doi.org/ https://doi.org/10.1111/nhs.12286View
Yen, C.-F., Chen, C.-C., Lee, Y., Tang, T.-C., Yen, J.-Y., & Ko, C.-H. (2005). Self-stigma and its correlates among outpatients with depressive disorders. Psychiatric Services, 56(5), 599-601. https://doi.org/https://doi.org/10.1176/appi.ps.56.5.599View
Cheang, S. I., & Davis, J. M. (2014). Influences of face, stigma, and psychological symptoms on helpseeking attitudes in Macao. PsyCh journal, 3(3), 222-230. https://doi.org/https:// doi.org/10.1002/pchj.61 View
Chen, J., & Zhu, S. (2016). Online information searches and help seeking for mental health problems in urban China. Administration and Policy in Mental Health and Mental Health Services Research, 43(4), 535-545. https://doi.org/https://doi. org/10.1007/s10488-015-0657-6View
Hayward, R. D., & Elliott, M. (2014). Cross-national analysis of the influence of cultural norms and government restrictions on the relationship between religion and well-being. Review of Religious Research, 56(1), 23-43. https://doi.org/https://doi. org/10.1007/s13644-013-0135-0View
Wang, Z., Chen, H., Koenig, H., & Phillips, M. R. (2019). Relationship of religiosity to mental health literacy, stigma, social distance, and occupational restrictiveness in Ningxia Province, China. Mental health, religion & culture, 22(4), 400- 415. https://doi.org/https://doi.org/10.1080/13674676.2019.159 3338 View
Wang, Z., Koenig, H. G., Zhang, Y., Ma, W., & Huang, Y. (2015). Religious involvement and mental disorders in mainland China. PLoS One, 10(6), e0128800. https://doi.org/https://doi. org/10.1371/journal.pone.0128800View
Gearing, R. E., Brewer, K. B., Cheung, M., Leung, P., Chen, W., & He, X. (2021). Suicide in China: community attitudes and stigma. OMEGA-Journal of Death and Dying, 0030222821991313. https://doi.org/10.1177/0030222821991313View
Gearing, R. E., Schwalbe, C. S., & Short, K. D. (2012). Adolescent adherence to psychosocial treatment: Mental health clinicians' perspectives on barriers and promoters. Psychotherapy Research, 22(3), 317-326. https://doi.org/10.10 80/10503307.2011.653996 View