
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 5 (2023), Article ID: JMHSB-174
https://doi.org/10.33790/jmhsb1100174Special Issue
Perspectives of American Indian/Alaska Native Mental Health Practitioners on Psychological Distress, Social Support, and Wellness
Mark Standing Eagle Baez, Ph.D., LSP, LCDC, CCBT, MS/MA
Assistant Professor of Clinical and Counseling Psychology, Department of Psychology, Bemidji State University, United States.
Corresponding Author Details: Mark Standing Eagle Baez, Ph.D., LSP, LCDC, CCBT, MS/MA, Assistant Professor of Clinical and Counseling Psychology, Department of Psychology,Bemidji State University, United States.
Received date: 28th November, 2022
Accepted date: 03rd January, 2023
Published date: 05th January, 2023
Citation: Baez, M. S. E., (2023). Perspectives of American Indian/Alaska Native Mental Health Practitioners on Psychological Distress, Social Support, and Wellness. J Ment Health Soc Behav 5(1):174.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objective: This quantitative research study employed a correlational design to determine if there is an association between social support, psychological distress, and wellness among American Indian and Alaska Native mental health practitioners (AI/ANMHPs).
Methods: A quantitative correlational approach examined to what extent a relationship exists between social support, psychological distress, and wellness among mental health practitioners who are Native American. The variable of psychological distress was measured by the Outcome Questionnaire 45 (OQ-45.2), the variable of social support was measured by the Multidimensional Scale of Social Support (MSPSS), the variable and the variable of wellness was measured using the Five Factor Wellness Inventory (5F-WEL).
Results: The sample comprised 95 AI/ANMHPs in the United States. A Spearman’s rank-order correlation was used to explore the relationship between social support and psychological distress (RQ1) and social support and wellness (RQ2) among AI/ANMHPs. The results of the study indicate a statistically significant negative correlation between social support and psychological distress (rs= -0.386, p < .001) and a statistically significant positive correlation between social support and wellness (rs = 0.439, p < .001).
Conclusions: The current study found two statistically significant correlations. Social support was statistically significantly negatively correlated with psychological distress, and social support was statistically significantly positively correlated with overall wellness. These findings suggest that as the NAMHPs perceive more social support, their psychological distress decreases; so, NAMHPs need more culturally responsive support if they want to manage distress.
Keywords: AI/ANMHPs, Social Support, Psychological Distress, Wellness, Correlational Design, Quantitative, Spirituality.
Introduction
Mental health service providers (mental health practitioners) are trained to work with individuals, families, and groups in treating mental, behavioral, and emotional problems and disorders [1]. Still, they often experience a range of emotional and personal demands that can impact their quality of life and clinical efficacy [2]. Counselors are highly susceptible to psychological distress due to their feelings of responsibility for clients' well-being, which can lead to deficits in patient care [3]. When mental health practitioners deal with their difficulties with mental health and other challenges by addressing significant issues, such as fulfillment and being healthy psychologically, the endeavor can be very gratifying and sustaining [4]. Bearse and colleagues [5] proposed that practitioners’ work predisposes them to experience specific problems, such as burnout, vicarious traumatization, compassion fatigue, and countertransference, thus creating a solid potential toll on those practicing in the field of mental health. Working as a mental health professional can lead to satisfaction [6]. Still, evidence suggests that mental health professionals are more vulnerable to increased stress levels than other occupational groups [7]. Mental health practitioners who are American Indian/Alaska Native (AI/ANMHP) may be at particular risk for psychological distress. Compared with all other racial groups, non-Hispanic American Indian/Alaska Native adults are at greater risk of experiencing psychological distress and are more likely to have lower overall mental health and unmet psychological needs [8].
In recent decades, many studies have been conducted on the impact of social support on mental health [9,10], with current research suggesting that social support is a strong influence that can affect mental health [11]. Social support is a factor that has the potential to reduce the psychological distress caused by burnout [12]. AI/ ANMHPs who may be dealing with previous traumas in their lives find that social support activities may reduce their psychological stressors and improve their level of wellness [13]. Bradley et al. [2] stated that counselors could not be effective if they do not engage in a healthy level of self-care. Just as research posited that social support improves one’s mental health, wellness is another underlying factor. Research has also demonstrated the link between social relationships and many different aspects of health and wellness [14]. Self-care is a priority to maintain the ability to work effectively for mental health practitioners. A critical need to care for yourself first and allow others to manage for you to be able to do your best work in caring for others [15].
A model that has shown promise in assessing wellness among counselors is the Wheel of Wellness, a model introduced by Witmer and Sweeney [16]. The model holds fast to the principle of using wellness-based counseling [17]. The Wheel of Wellness is the first model based on counseling and is a theoretical model “which emerged from reviews of cross-disciplinary studies” [17]. The Five Factor Wellness Inventory (5F-WEL) was developed through structural equation modeling analysis of the database for the instrument, its precursor, the Wellness Evaluation of Lifestyle [18,19]. The 5F-WEL, an evidence-based tool, is used to assess wellness characteristics, such as social, familial, stress, spiritual, and cultural, as a basis for helping individuals make choices for a healthier living (social, psychological, and wellness). The 5F-WEL [17] and the Wheel of Wellness [16] correlate the quality of life, health, spirituality, and endurance while employing Adlerian individual psychology, the organizing principle of the wheel.
Social support provided by family members, peers, and others may not be fully appreciated; however, prior research suggested that this support may represent an essential asset for maintaining and preserving wellness [20]. According to Gone [21], the fact that AI/ANMHPs subscribe to Western methods of health suggests that they also subscribe to culturally specific techniques, such as spiritual, ceremonial, and healing practices towards wellness (i.e., sweat-lodge, Native American Church ceremony, healing circles, formal dances, etc.). Using culture and tradition as a roadmap may provide healing and healthy lifeways for AI/ANMHPs and possible opportunities to develop behaviors to actively engage with others to promote wellness [22]. Thus, integrating weekly social support activities for AI/ANMHPs, such as spiritual, ceremonial, and healing practices, may increase the optimum level of wellness [23].
The relationship between social support, psychological distress, and wellness among AI/ANMHPs has not been examined. This study sought to understand wellness’s role among AI/ANMHPs while recognizing that their effectiveness and value as mental health counselors depend on their own psychological and physical well-being [24]. Identifying the association between each of the variables for developing wellness-oriented program procedures for mental health practitioners while identifying ways to prevent and reduce impairment among practitioners is vital.
The author of this research examined the disclosure of psychological distress, social support, and wellness among AI/ANMHPs. Using ethnography and qualitative analysis, the author proposed that these methods can enhance AI/ANMHPs research conducted with multicultural communities and provide better avenues toward a proper understanding of diversity as it relates to professional inquiry.
The two research questions and two hypotheses to examine and measure the extent to which relationships exist between social support, psychological distress, and wellness are as follows:
Research Question 1
Is there a relationship between social support and psychological distress among AI/ANMHPs in the United States?
Research Question 2
Is there a relationship between social support and wellness among AI/ANMHPs in the United States?
Methods
Research Design
The design selected for the study was correlational, as the researcher sought to examine the extent to which relationships exist between social support, psychological distress, and wellness of AI/ ANMHPs in the United States. The researcher used validated survey instruments to collect quantitative data that could be analyzed using statistical analysis to assess the relationships among the variables of interest. A correlational design was most suitable for this study as correlation is a statistical method that evaluates and defines the strength and direction of linear associations between variables [25].
Participants
This study's targeted population of interest included AI/ANMHPs. They were licensed professional counselors, licensed social workers, psychologists, licensed mental health counselors, and licensed substance abuse counselors providing services in the community setting/mental health programs. The study population was comprised of licensed and credentialed AI/ANMHPs from throughout the United States who are members of the listserv of the Society of Indian Psychologists (SIP), a professional association of psychologists and counselors who work with AI/AN clients and non-Native clients off the reservation.
Sampling Strategy
Participants were recruited through a non-probability sampling process employing a convenience sampling strategy because this allowed the researcher to maximize the sample size with limited resources [25]. The inclusion criteria for the sample were that the participants must self-identify as AI/AN and be licensed/credentialed mental health professionals. Exclusion criteria were participants residing outside the United States and those who did not self-identify as of Indigenous ancestry.
Sample Size
The minimum sample size for this study was computed using the G*Power software package (version 3.1.9.4) for the planned correlation analyses. Parameters for the power analysis included a two-tail test with a power of 0.80 and a significance level of .05 [26]. A minimum of 97 AI/ANMHP individuals were needed for Pearson’s correlations. If one accounts for a contingency of non-parametric analysis due to a failure of one or more assumptions, an additional 15% was added to the sample size, thus resulting in a minimum sample size of 97 (N = 84 + 13 = 97) AI/ANMHPs in the United States.
Recruitment
Of the 250 potential participants identified from the SIP listserv (e.g., those subscribed to the listserv that self-identified as AI/AN and licensed/credentialed MHPs), 115 people clicked on the link that took them to an informed consent form. Of those, 114 agreed to participate in the study. The 114 participants were then directed to the survey content. Of the 114 who agreed to participate, 16 (14%) failed to complete the survey. Removing these 19 participants resulted in a total sample size of 95 respondents.
IRB Approval
Before collecting data, the researcher sought permission from the SIP to use their members as the study subjects. Upon receiving permission from SIP, the researcher asked SIP to sign a site authorization form for the GCU Institutional Review Board (IRB) verification purposes. After getting approval from the IRB, the researcher sent written invitations to the SIP organization members. Participants were informed that participation in the study was completely voluntary and confidential.
Procedure
Participants were asked to complete a 10-minute questionnaire administered through an online survey application (i.e., Survey Monkey). Participant codes were assigned to the instruments to ensure the matching of responses to participants. The researcher collected the various forms as they were completed, and efforts were made to correct any errors in the data collection process.
Variables
Demographics
Demographic variables of interest included participant age, marital status, employment, current educational status, highest degree obtained, and gender. These data are represented in Table 1.
The MSPSS [27] is a 12-item instrument that measures the perceived adequacy of social support from three sources: family members, friends, and other significant people. Ratings of these items were scored from a 7-point Likert-type scale ranging from very strongly disagree (1) to agree (7) very strongly

Table 1. Demographic Information from Study Sample
Outcome Questionaire-45.2 (OQ-45.2)
OQ-45.2 is a normed, referenced, 45-item self-report instrument that attempts to measure the subjective experience of participants, as well as the way they function in the world [28]. Specifically, it attempts to measure how a person is feeling (depressed or anxious), getting along with others (friends and family), and functioning in important life tasks (school and work). The inventory uses a Likert scale that ranges from 0 (never) to 4 (always).
Five-Factor Wellness Evaluation of Lifestyle (5F-WEL)
The 5F-WEL is an evidence-based tool developed by Sweeney and Witmer in 1992 [29] and designed to assess wellness characteristics and provide data for the variables in this research. The inventory measures a person’s overall degree of wellness and how a person scores on the five subscales: the Creative Self, the Coping Self, the Social Self, the Essential Self, and the Physical Self. Each statement on the 5F-WEL inventory was scored on a 4-point Likert-type scale ranging from strongly agree (4) to strongly disagree [17]. The Five The MSPSS, OQ-45.2, and 5F-WEL attempt to measure perceptions of social support, psychological distress, and wellness by focusing on how wellness decisions are processed. After the MSPSS, OQ-45.2, and 5F-WEL, the AI/ANMHPs were also asked questions that provided personal and professional information for the sample studied, descriptive purposes, and demographic data.
Analysis
Upon receiving the assessments, the data were scored per the protocols of each assessment manual. Per protocol, the data for the MSPSS, OQ-45.2, and 5F-WEL were inputted into an online scoring database system. The data were then entered with verification from a second party for each participant on an Excel spreadsheet and finally uploaded into an SPSS data file for statistical analyses. Specifically, each AI/ANMHP was examined to determine if the sample size requirements (84 + 13 = 97) as per the G*Power analyses were adequate. Only the surveys that were fully completed were used in this study.
For both research questions, the researcher used a Pearson bivariate correlation for the analyses because both variables are measured on continuous scales.
The researcher administered three inventories to compare responses between AI/ANMHP levels of social support, psychological distress, and wellness. The inventories were used to compare responses between the patterns of relationships in overall totals on the MSPSS, the OQ-45.2, and the 5F-WEL factors. The researcher used a bivariate correlational approach to assess correlations between social support, psychological distress, and wellness. This was more appropriate due to the nature of correlations, two variables, and large samples describing associations between two variables.
Results
Research Question 1
Is there a relationship between social support and psychological distress among AI/ANMHPs? Pearson Correlation was used to assess the extent and direction of relationships between variables. To conduct this analysis, several assumptions were met first—variables must be continuous, variables must be paired, there should be no significant outliers, there needs to be a linear relationship between variables, and the data need to be close to customarily distributed [30]. The following sections describe each of these assumptions and the related analysis. In the current study, the researcher visually inspected the scatterplot generated by plotting total MSPSS scores against OQ-45.2. This visual inspection aimed to determine if there was a linear relationship between the two variables. As depicted in Figure 1, a visual inspection of this scatterplot indicated a linear relationship between the variables [30].

Figure 1. Scatterplot of MSPSS against OQ-45.2.
Approximately Normal Distribution
To assess the normality of the data, a Shapiro-Wilk test and a visual inspection of a histogram were used. If the assumption of normality has been violated, the “Sig.” value will be less than .05 (i.e., the test is significant at the p < .05 level). As evident in Figure 1 above, the MSPSS and OQ.45.2 scores have significance values of less than .05; therefore, the normality assumption has been violated in each case. Visual inspection of Figures 2 and 3 shows the distribution of scores to be skewed as well.
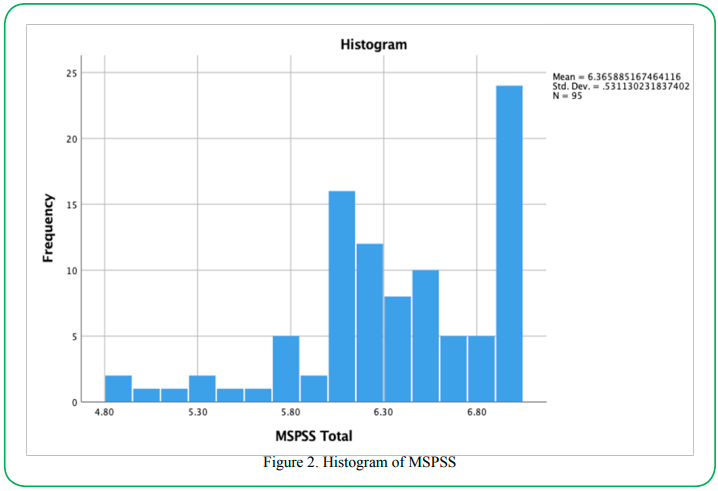
Figure 2. Histogram of MSPSS

Figure 3. Histogram of OQ-45.2.
For Research Question 1, Spearman’s rank-order correlation indicates a statistically significant, negative correlation between social support and psychological distress, rs= -.386, p < .001. The results of the current study indicate a rejection of the null hypothesis that there is a statistically significant negative correlation between social support and psychological distress.
Research Question 2
Is there a relationship between social support and wellness among AI/ANMHPs in the United States? Like Research Question 1, a Pearson Correlation was initially intended.
Linear Relationship Between the Variables
In the current study, the researcher visually inspected the scatterplot generated by plotting total MSPSS scores against 5F-WEL scores. This visual inspection aimed to determine if there was a linear relationship between the two variables. Visual inspection of this scatterplot, as depicted in Figure 4 (below), indicated a linear relationship between the variables [30].
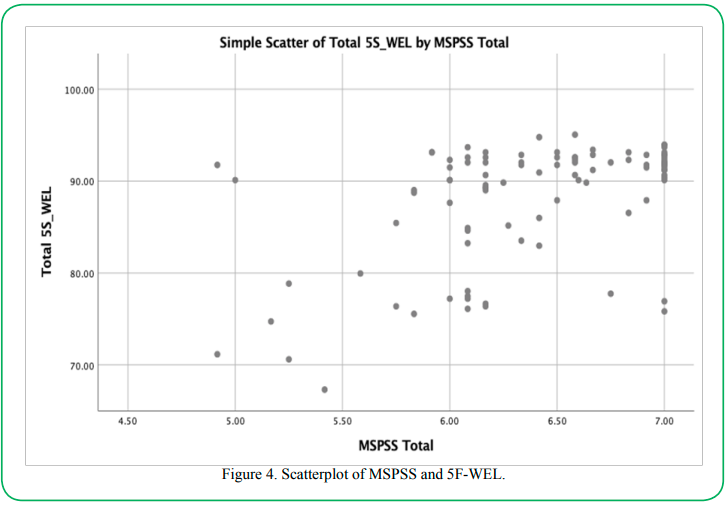
Figure 4. Scatterplot of MSPSS and 5F-WEL.
Approximately Normal Distribution
To assess the normality of the data, a Shapiro-Wilk test and a visual inspection of a histogram were used. If the assumption of normality has been violated, p values will be less than .05 (i.e., the test is significant at the p < .05 level). As is evident in Table 2, the MSPSS and 5F-WEL scores have p-values of less than .05; therefore, the normality assumption has been violated in each case. Visual inspection of Figures 5 and 6 shows (below) the distribution of scores to be skewed as well.
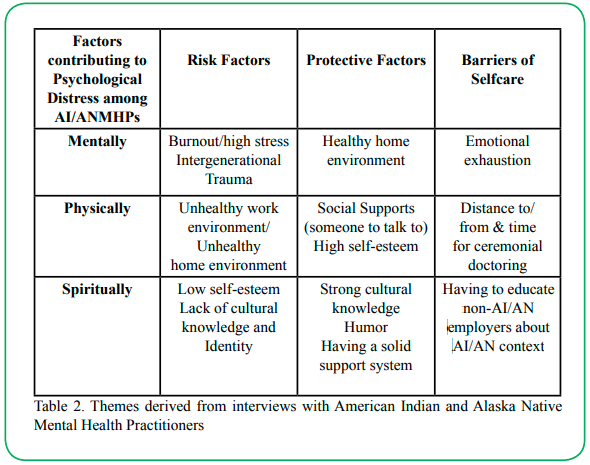
Table 2. Themes derived from interviews with American Indian and Alaska Native Mental Health Practitioners
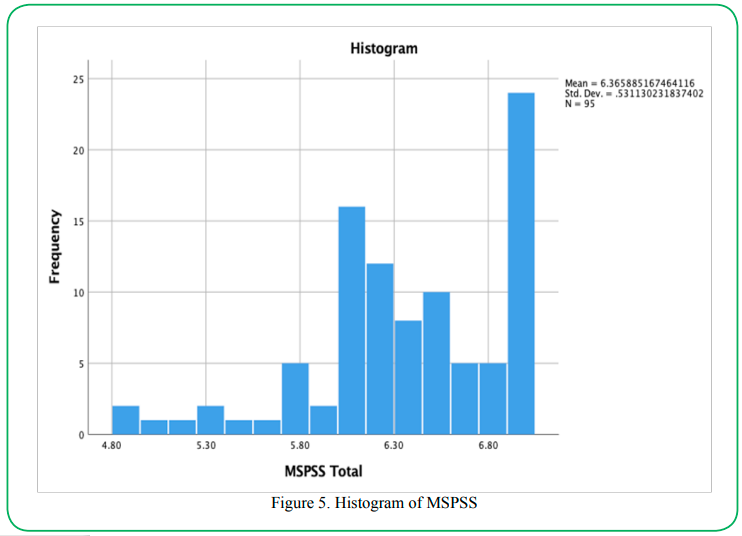
Figure 5. Histogram of MSPSS
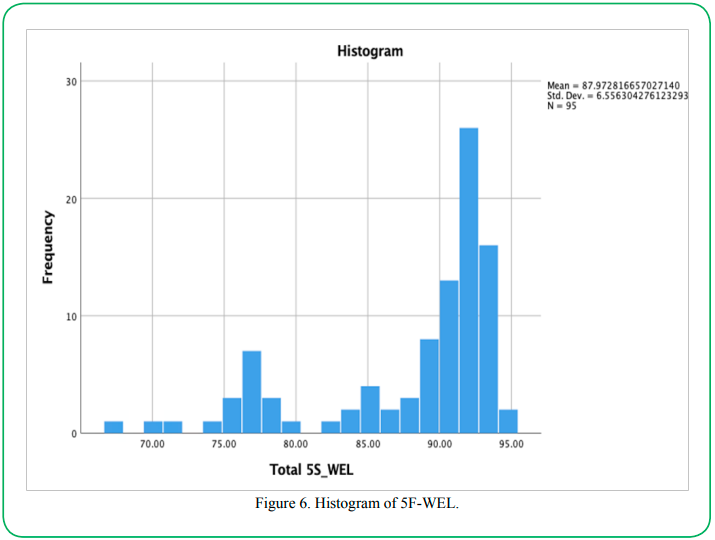
Figure 6. Histogram of 5F-WEL.
As mentioned above, because the assumption of normality was violated, the researcher had to conduct a Spearman’s rank-order correlation instead of a Pearson’s correlation. Three assumptions must be met to perform a Spearman rank-order correlation: variables must be continuous, variables must be paired, and there needs to be a monotonic relationship between variables [30]. The first two assumptions were met based on the study design. The third assumption was verified using the scatterplot generated in Figure 4. All hypotheses were met to conduct a Spearman’s correlation appropriately. Research Question 2: A Spearman’s rank-order correlation showed a statistically significant, positive correlation between social support and wellness, rs= .439, p < .001. The results of the current study support the rejection of the null hypothesis that there is not a statistically significant correlation between social support and wellness among AI/ANMHPs in the United States.
Themes derived from interviews with American Indian and Alaska Native Mental Health Practitioners
The themes from the questionnaire featured the participants' accounts characterizing particular perceptions and experiences that the researcher saw relevant to the research question. This method allowed the researcher to describe the data and interpret the themes. The analysis produced three factors contributing to psychological distress among AI/ANMHPs Mental, Physical and Spiritual. Mentally. Some risk factors were high burnout/high stress levels and intergenerational traumas. Some of the protective factors were a healthy home environment and familial support. Barriers to self-care were emotional exhaustion. Physically. Some risk factors were an unhealthy work environment and an unhealthy home environment. Some protective factors were social support (someone to talk to) and high self-esteem. Barriers to self-care were distance to/from participating in ceremonial services. Spiritually. Some risk factors were Low self-esteem and lack of cultural knowledge and identity. Some protective factors were strong cultural knowledge, humor, and a solid support system. Barriers to self-care included educating non-AI/AN employers about the AI/AN context of wellness support in lowering levels of distress. Almost all participants reported the importance of mental, physical, emotional, and spiritual in the practice they provide. Illustrative examples appear below (Table 2).
Strengths and Weaknesses of the Study
The current study has several strengths. One strength of the study is that the instrumentation was previously created and validated in various situations with several samples. In addition, the 5F-WEL is culturally sensitive and appropriate for this study's population. Another strength is the overall research design. Given that the researcher applied a correlational study, the extent to which relationships exist between social support, psychological distress, and wellness of AI/ANMHPs in the United States could be examined. The final strength of the study is that the researcher obtained more (95) responses than needed. Initially, the G Power analysis showed that the researcher required 84 participants to conclude appropriately.
Given that the researcher could solicit 95 participants, the results are more robust. One advantage of convenience sampling is that data can be collected quickly and cheaply. Because cultural medicine is essential to AI/AN and AI/ANMHPs, cultural encapsulation has deterred the acknowledgment of AI/AN medicinal practices as a precursor to folk medicine and many herbal remedies, which have greatly influenced modern medicine. Understanding AI/AN healing practices requires helping professionals know about AI/AN cultural belief systems regarding health and wellness, with the many influences that create change in the mind, body, spirit, and natural environment [31]. The study also has several weaknesses. One of the weaknesses in this study was in response to the practice concerns and a sample study using a convenience sample. One disadvantage of convenience sampling is that the model may not represent the population the researcher is interested in studying. Another weakness is that participants’ work experiences and ethnicity may influence their responses and approaches to the instruments. For example, two random questions were asked of AI/ANMHPs providing services off the reservation, were ‘Are you supported and provided with appropriate time off (i.e., ceremonial support/having a ceremony done for you as a practitioner)’ and ‘Does your place of employment encourage cultural supports for self-care?’
Recommendations for Future Research
The first recommendation is to conduct a similar line of study with AI/ANMHPs working on an Indian reservation. The request for further research is to explore the same population of AI/ANMHPs working on an Indian reservation over time or longitudinally to determine if their wellness and distress differ across time. Further research into these approaches, as well as other environmental factors, should be considered.
The second would be, given that 61% of the total sample scored above the clinical cutoff score for the severity of Total Symptom Distress, that future research might address the specific study of this population. Mental health practitioners who are Native American and may be dealing with previous traumas [13] find that social support activities may reduce their psychological stressors and improve their level of wellness. Given that social support is only one measure of AI/ANMHP wellness, this study helps to provide a holistic picture of the wellness profile of an AI/ANMHP and past traumas.
The third is to explore other Indigenous populations which serve in the mental health field globally. One of the reasons the counselors gave for their engagement in self-practice was that they live and work in their communities where their clients might be people they know, including friends, relatives, or friends of a friend [32]. Further research into First Nations, Aboriginals, and Indigenous AI/ ANMHPs, and their levels of social support, psychological distress, and wellness should be considered.
The fourth is to conduct research on this study will help AI/ ANMHPs and researchers apply a wellness component to self-care for personal and professional counseling interventions.
Conclusion
The current study contributes to the body of knowledge about self-care, the relationship between social support, and psychological distress and wellness among AI/ANMHPs in the United States. Opportunity for future research of this study will help AI/ANMHPs and researchers apply a wellness component to self-care for personal and professional counseling interventions. Specifically, this study allows AI/ANMHPs to understand the importance of meaning and purpose in wellness and self-care. I concluded that there was a negative, moderate correlation between social support and psychological distress and a positive, moderate-to-strong correlation between social support and wellness. The first is from the test of normality called the Shapiro-Wilk test. If the assumption of normality has been violated, the "Sig." value will be less than .05 (i.e., the test is significant at the p < .05 level). All the variables have a significance value of less than .05; therefore, the normality assumption has been violated in each case. Initially, since that method did not work in our favor, I chose to look at the data differently, calculating a z-score for the skewness and kurtosis of each variable.
The results suggest that psychological distress decreases as one’s social support increases. This indicates that social support is beneficial in combatting psychological distress in this population. Similarly, as social support increases, so does wellness. This suggests that as one engages more with the social support structures around them, the higher one’s health is. The results help shed light on the significance of social support and wellness of AI/ANMH practitioners as they continue to deal with stress resulting from their roles in the mental health professions. Although more research is needed, success in wellness activities assists in decreasing vulnerability to vicarious traumatization among counselors [33,34,35], and wellness activities are essential to maintaining effectiveness, decreasing the risk of impairment, and supporting the ethical obligation not to harm [36]. Although not significant in the magnitude of the relationship, the results of this study support the notion that social support and wellness may contribute to NAMHPs lower levels of psychological distress.
Competing interest:
The author declares that they have no competing interests.
References
American Counseling Association. (2010). ACA’s task force on counselor wellness and impairment. http://www.counseling. org/ wellness_taskforce /index.htmView
Bradley, N., Whisenhunt, J., Adamson, N., & Kress, V. E. (2013). Creative approaches for promoting counselor self-care. Journal of Creativity in Mental Health, 8(4), 456-469. https:// doi.org/10.1080/15401383.2013.844656View
Baldwin-White, A. (2014). Psychological distress and substance abuse counselors: An exploratory pilot study of multiple dimensions of burnout. Journal of Substance Use, 21(1), 29–34. https://doi.org/10.3109/14659891.2014.949316View
Zur, O. (2014). Codes of ethics on therapists’ impairment, burnout, and self-care. Zur Institute. https://drzur.com/ethics-of-burnout/ View
Bearse, J. L., McMinn, M. R., Seegobin, W., & Free, K. (2013). Barriers to psychologists seeking mental health care. Professional Psychology: Research and Practice, 44, 150–157. https://doi.org/10.1037/a0031182View
Stamm, B. H. (2010). The concise ProQOL manual (2nd ed.). ProQOL.org. https://www.researchgate.net/ publication/340033923_The_Concise_ProQOL_Manual_ The_concise_manual_for_the_Professional_Quality_of_Life_ Scale_2_nd_EditionView
Rudaz, M. (2017). Review articles: Mindfulness and acceptance-based training for fostering self-care and reducing stress in mental health professionals: A systematic review. Journal of Contextual Behavioral Science, 6(4), 380. https:// doi.org/10.1016/j.jcbs.2017.10.001View
Barnes, P. M., Adams, P. F., & Powell-Griner, E. (2010). Health characteristics of the American Indian or Alaska Native adult population: the United States, 2004-2008. National Health Statistics Reports, (20), pp. 1–22.View
Ates, B. (2016). Perceived social support and assertiveness predictor candidates’ psychological counselors’ psychological well-being. International Education Studies, 9(5), 28–39. https://doi.org/10.5539/ies.v9n5p28View
Cohen, S., Underwood, L. G., & Gottlieb, B. H. (Eds.). (2000). Social support measurement and intervention: A guide for health and social scientists. Oxford University Press. https:// doi.org/10.1093/med:psych/9780195126709.001.0001View
Harandi, T. F., Taghinasab, M. M., & Nayeri, T. D. (2017). The correlation of social support with mental health: A meta-analysis. Electronic Physician, 9(9), 5212–5222. https://doi. org/10.19082/5212View
Sánchez-Moreno, E., de La Fuente Roldán, I., Gallardo-Peralta, L. P., & Barrón López deRoda, A. (2015). Burnout, informal social support and psychological distress among social workers. British Journal of Social Work, 45(8), 2368-2386. https://doi. org/10.1093/bjsw/bcu084View
Grayshield, L., Rutherford, J. J., Salazar, S. B., Mihecoby, A. L., & Luna, L. L. (2015). Understanding and healing historical trauma: The perspectives of Native American elders. Journal of Mental Health Counseling, 37(4), 295–307. https://doi. org/10.17744/mehc.37.4.02 View
American Psychological Association (2019). Manage Stress: Strengthen Your Support Network. Retrieved on June 28th, 2022, from https://www.apa.org/topics/stress/manage-social-support View
SAMHSA. (n.d.). [SAMHSA Tips for Healthcare Professionals: Coping with Stress and Compassion Fatigue]. Retrieved June 28, 2022, from https://store.samhsa.gov/sites/default/files/ SAMHSA_Digital_Download/PEP20-01-01-016_508.pdfView
Witmer, J. M., Sweeney, T. J., & Myers, J. E. (1998). The Wheel of Wellness. Greensboro, NC: Journal of Counseling & Development,78(3). https://doi.org/10.1002/j.1556-6676.2000. tb01906.xView
Myers, J. E., & Sweeney, T. J. (2005). Counseling for wellness: Theory, research, and practice. American Counseling Association Publication. https://doi.org/10.1891/9780826171825.0093View
Hattie, J. A., Myers, J. E., & Sweeney, T. J. (2004). A factor structure of wellness: Theory, assessment, analysis, and practice. Journal of Counseling and Development, p. 82, 354- 364. https://doi.org/10.1002/j.1556-6678.2004.tb00321.xView
Myers, J. E., Sweeney, T. J., & Witmer, J. M. (2004). The Wellness Evaluation of Lifestyle. Redwood City, CA: Mind Garden,Inc. https://doi.org/10.1002/j.1556-6678.2004.tb00321.xView
Gallagher, E. N., & Vella-Brodrick, D. A. (2008). Social support and emotional intelligence as predictors of subjective well-being. Personality and Individual Differences, 44(7), 1551- 1561. https://doi.org/10.1016/j.paid.2008.01.011View
Gone, J. P. (2016). Alternative knowledge and the future of community psychology: provocations from an American Indian healing tradition. American Journal of Community Psychology, 58(3/4), 314-321. https://doi.org/10.1002/ajcp.12046View
Baez, M. S. E., Isaac, P., Baez, C. A. (2016). H.O.P.E. for indigenous people battling intergenerational trauma: The Sweetgrass Method. Journal of Indigenous Research, 5. View
Gone. J. P. (2004). Mental health services for Native Americans in the 21st century United States. Professional Psychology: Research and Practice, 35. https://doi.org/10.1037/0735-7028.35.1.10View
American Mental Health Counselor Association (AMHCA). (2015). Principles for AMHCA Code of Ethics. http://connections. amhca.org/ HigherLogic System/ DownloadDocumentFile. ashx?DocumentFileKey=d4e10fcb-2f3c-c701-aa1d-5d0f53b8bc14View
Rovai, A. P., Baker, J. D., & Ponton, M. K. (2013). Social science research design and statistics: A practitioner’s guide to research methods and IBM SPSS. Watertree Press LLC.View
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191. https://doi.org/10.3758/bf03193146View
Zimet, G. D., Dalhem, N. W., Zimet, S. G., & Farley, G. K. (1988). The Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 52, 30–41. https:// doi.org/10.1207/s15327752jpa5201_2View
Lambert, M. J., Morton, J. S., Hatfield, D., Harmon, C., Hamilton, S., Reid, R. C., & Christopherson, C. (2004). OQ-45.2 (Outcome Questionnaire). OQ Measures LLC. https://doi. org/10.15448/1980-8623.2016.4.24600
Witmer, J. M., & Sweeney, T. J. (1992). A holistic model for wellness and prevention over the life span. Journal of Counseling and Development, pp. 71, 140–148.View
Laerd Statistics (2015). Two-way mixed ANOVA using SPSS Statistics. Statistical tutorials and software guides. https://doi. org/10.17504/protocols.io.bhyaj7se
Portman, T. & Garrett, M. (2006). Native American healing traditions. International Journal of Disability Development and Education, p. 53. 453–469. https://doi. org/10.1080/10349120601008647View
Bennett L, et al. (2015). Detection of composite communities in multiplex biological networks. Sci Rep 5:10345.View
Foreman, R.D., et al. (2015). Mechanisms of Cardiac Pain. Comprehensive Physiology, 5:929-960. https://doi.org/10.1002/ cphy.c140032View
Pearlman, L. A., & Saakvitne, K. W. (1995). Trauma and the therapist: Countertransference and vicarious traumatization in psychotherapy with incest survivors. Norton, xix, pp.451. https://doi.org/10.1080/00029157.1996.10403354View
Williams, A., Helm, H., & Clemens, E. (2012). The effect of childhood trauma, personal wellness, supervisory working alliance, and organizational factors on vicarious traumatization. Journal of Mental Health Counseling, pp. 34, 133–153. https:// doi.org/10.17744/mehc.34.2.j3l62k872325h583View
Foreman, T. (2018). Wellness, exposure to trauma, and vicarious traumatization: A pilot study. Journal of Mental Health Counseling, 40(2), 142–155. https://doi.orgView