
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 5 (2023), Article ID: JMHSB-175
https://doi.org/10.33790/jmhsb1100175Research Article
Kawaida Theory and the Nguzo Saba: African-centered Caregiving for the Elders
Claudia Thorne
Assistant Professor, Department of Social Work, Coppin State University, 2500 West North Avenue, Baltimore, MD 21216, United States.
Corresponding Author Details: Claudia Thorne, Ph.D., LISW, LCSW, Assistant Professor, Department of Social Work, Coppin State University, 2500 West North Avenue, Baltimore, MD 21216, United States.
Received date: 07th December, 2022
Accepted date: 11th January, 2023
Published date: 14th January, 2023
Citation: Thorne, C., (2023). Kawaida Theory and the Nguzo Saba: African-centered Caregiving for the Elders. J Ment Health Soc Behav 5(1):175.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
There is limited research on culturally sensitive interventions to support African American caregivers of elderly relatives. This qualitative research study explores caregiving among twenty African American professional and managerial women baby boomers caring for older parents. Study findings generate a culturally relevant, African-centered caregiving perspective to add to the literature on caregiving. Study results support the application of Nguzo Saba principles – Umoja (Unity), Kujichagulia (Self-Determination), Ujima (Collective Work and Responsibility), Ujamaa (Cooperative Economics), Nia (Purpose), Kuumba (Creativity), and Imani (Faith) to African American caregiving practices. The knowledge generated from this study has implications for social work interventions with individuals, groups, and communities to support African American caregivers.
Keywords: African American, African-centered social work, Caregiving, Nguzo Saba, Kawaida Theory, Women, Aging, Elders, Social work
Introduction
This qualitative research study explores caregiving through the lens of Kawaida theory and the principles of the Nguzo Saba among African American women baby boomers, born between 1946 1964, who are caring for elderly relatives. Fairfax [1] asserts that African-centered social work calls for "a fundamental need for people to learn how to live to their fullest potential and realization that stays true to who they are, how they understand themselves, and their priorities as people, based upon philosophical frameworks that are relevant in their long histories." Approaching caregiving through the lens of Kawaida theory and Nguzo Saba provides an opportunity for social workers to support the humanity of African American caregivers within the context of race, culture, family, and community. Simultaneously, approaching caregiving through the lens of the Nguzo Saba can inspire social workers to support caregivers in culturally appropriate and strength-based approaches to address the holistic needs of caregivers, their families, and the communities in which they live.
A plethora of best practice and randomized controlled trial caregiver interventions targeted toward caregivers are examined in the literature. However, there is sparse research on the applicability of these interventions with African American caregivers. The interventions do not address some of the significant concerns of African American caregivers.
Literature Review
The significant growth in the number of persons age 65 and older has broad-sweeping financial and social implications for individuals, families, and society. According to the Administration for Community Living, Administration of Aging [2], the population of persons age 65 and older is 54.1 million in 2019 and is expected to reach 94.7 million in 2060. The number of African Americans 65 and older was 4,979,133 in 2019, or 9% of the older population. The projected growth is to12.1 million or 13% of the older population by 2060. This increase in the African American older population has significant implications for caregiving within a cultural context. African American family caregivers provide more support to aging adults through the direct provision of informal care and formal care coordination and advocacy [3]. Aging in place, within the context of family and community, emerges from African culture and tradition deeply grounded in filial loyalty, respect for older family members, the interconnectedness of family members, and the spiritual essence of life [4-8]. The caregiving experience of African American caregivers is complex and varies within the African American community [9]. Caregiving benefits can include the development of compassion, understanding of the older person's perspective, forgiveness of unresolved issues with parents, spiritual growth, preparation for their own aging, being present to the reciprocity of giving and receiving, having a more universal and loving perspective on the human condition, leaving a family legacy, and motivation to make the necessary lifestyle changes to ensure active aging [9-11].
There is gender fluidity in carrying out caregiving roles with women more likely to be caregivers and provide the majority of unpaid informal care [12]. Yet more African American men are assuming the caregiving roles [13]. African American female caregivers have historically reported a lower caregiver burden than other groups [14,15,16]. However, the historical support system for African Americans to care for elders has changed due to increasing mobility, smaller family size, more persons remaining single, and the growing rates of divorce [16-18]. These changes have resulted in increased caregiver burden and adverse health, mental health, and financial consequences [16,19,20]. Recent studies suggest African American caregivers caring for dementia family members display higher rates of physical and psychological symptomology of stress and anxiety at similar levels to White caregivers [21] and they are at higher risk of developing Alzheimer's themselves [22]. Caregivers will often prioritize their relatives' health while compromising their own [21]. They choose to care for the family members in their own homes and are reluctant to utilize formal and informal support in alignment with the intergenerational cultural value, "we care for our own" [18].
The historical context for the current health status of African American women is embedded in the intersectionality of race and gender across time [23]. African American women have experienced " an accumulation of racial inequality; social, political, and economic exclusion; and medical under service. These inequities decrease access to resources and heighten susceptibility to psychological stress and premature stress-related illness" [24]. African American women experience gender-related stress and race-related stress that is often internalized into the strong Black women roles and schemas [24,25]. Research indicates a relationship between racism and the health status of African American women. Comparing women's health indicators across ethnic groups, African American women fare the worse [26]. African American women report "general psychological distress, depression, alcohol consumption, poorer perceived health status" [27], cardiovascular disease, and health conditions [24,28,29]. However, addressing health disparities also means that we must address the role of structural racism to improve health outcomes [30].
Critique of Contemporary Interventions
The National Academies of Science [31] reviewed the available evidence of caregiver intervention programs implemented over several decades to summarize the effectiveness of therapeutic strategies, care delivery models, programs, and services. Caregiver interventions in this review included education and skills training, environmental modifications, care management, counseling, and multi-component models. The study examined individual-level interventions designed to improve the following outcomes for caregivers physical and emotional health, knowledge and skills, social support, coping strategies, and quality of life. The ability to assess the effectiveness of the interventions with African American caregivers was limited due to the small numbers participating in the programs [31]. (See Table 1: Review and Critique of Caregiver Interventions).

Table 1. Review and Critique of Caregiver Interventions
The literature review and critique of caregiving programs indicate that several decades of caregiver interventions are not specific to the culture, heritage, and needs of African Americans, nor do they take into account the practical concerns such as balancing financial and physical strain, caregiver work, and managing health care providers [31]. Interventions are targeted at individual caregivers [31], and they do not consider the interconnectedness of African American families and community life.
Upon receiving the assessments, the data were scored per the protocols of each assessment manual. Per protocol, the data for the MSPSS, OQ-45.2, and 5F-WEL were inputted into an online scoring database system. The data were then entered with verification from a second party for each participant on an Excel spreadsheet and finally uploaded into an SPSS data file for statistical analyses. Specifically, each AI/ANMHP was examined to determine if the sample size requirements (84 + 13 = 97) as per the G*Power analyses were adequate. Only the surveys that were fully completed were used in this study.Other studies identified the intervention needs as expressed by caregivers. Research conducted by Samson et al. [21] found that African American caregivers desire culturally appropriate and familiar care. They preferred to engage in support services attuned to African American heritage and culture, including food, language, and physical setting. Authenticity and familiarity are critical variables for engaging support services for an elder. In this study, African American caregivers stated in retrospect that they wish they were more proactive about planning for caregiving by having knowledge of medical issues, living wills, financial planning, and legal issues. Caregivers also acknowledge the lack of information about community-based resources designed for eldercare. Keller's [34] study of African American women caregivers' perception of health and factors that influence health identified the following outcome domains for positive health outcomes: "spirituality, relationships, character, coping, preserving oneself, support, personal empowerment, resources, striving for peace, handling emotions, wellness, and taking care of self and place."
Theoretical Approach: African-centered Worldview
Historically, the elder is held in high esteem in the African American family as the keeper of the family legacy, a position of honor. A return to African-centered principles as a value system for caregiving honors "the fundamental goodness of people, recognizes the importance of family and community, encourages individual and collective functioning, understands the role and significance of spirituality, and acknowledges the critical ways the people are interdependent." [35]. An African-centered caregiving paradigm for elders focuses on an approach to human services that reflects African Americans, cultural and political reality and fosters spiritual and moral development [8]. Harvey [36] calls for a shift to social work practice using African values, ethics, and philosophy to reclaim ancient African values and principles to support optimal functioning [6].
Kawaida theory calls for African people to restore and heal their consciousness by recovering the objective and subjective African deep cultural structures and values so that African American lives can reflect optimal wellbeing, health, and wholeness [6,37]. Kawaida is an African communal philosophy created in the 1960s liberation struggle and represents the highest level of an African philosophy of life and thought. Karenga defines African-centeredness as a methodology of philosophy and practice rooted in the cultural image and human interest of African people. Rootedness in African culture includes spiritual orientation, ethical thinking and behaviors, traditions of living history, and respect for all humanity, elders, the environment, and the community [38]. Kawaida theory provides ethical and moral guidance for children, families, women, men, and communities to create a cultural legacy of achievement by living in alignment with ethical standards and commitments. Principles emerging from Kawaida theory provide a model for African American excellence by continuing dialogue with African culture to reinforce strengths and build upon the best in the culture. The following chart (Figure 1) describes the philosophical underpinnings of Kawaida theory as described by Maulana Karenga [37,38]: (1) Sankofa: to return and reconstruct African Culture; (2) Nguzo Saba: to imagine a new way of being; (3) Kwanzaa: to reinforce the principles of the Nguzo Saba; and (4) Family, Community and Culture: Spiritual grounding, reflection, action and giving thanks [37,38].
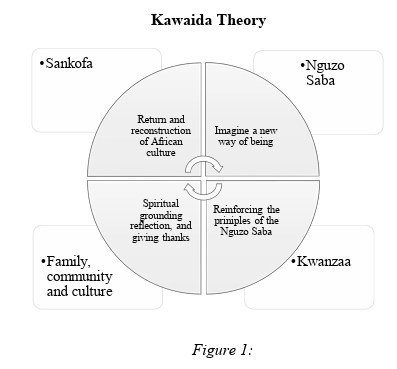
Figure 1: Kawaida Theory
This model, inclusive of the principles of the Nguzo Saba, can be applied to caregiving to build individual, family, and community resiliency and reduce many of the risk factors associated with caregiving. As described by Karenga [39](pp. 7-8), the principles of the Nguzo Saba are:
1. Umoja (Unity): To strive for and maintain unity in the family, community, nation, and race.
2. Kugichagulia (Self-Determination): To define ourselves, name ourselves, create for ourselves and speak for ourselves.
3. Ujima (Collective Work and Responsibility): To build and maintain our community together and make our brother's and sister's problems our problems and to solve them together.
4. Ujamaa (Cooperative Economics): To build and maintain our own stores, shops, and businesses and profit from them together.
5. Nia (Purpose): To make our collective vocation the building and developing of our community to restore our people to their traditional greatness.
6. Kuumba (Creativity): To do always as much as we can, in the way that we can, in order to leave our community more beautiful and beneficial than when we inherited it.
7. Imani (Faith): to believe with all our heart in our people, our parents, our teachers, our leaders, and the righteousness and victory of our struggle.
The research will explore the application of the Nguzo Saba to caring for African elders. The application will include the four philosophical underpinnings of Kawaida theory and the principles of the Nguzo Saba to create a model for African-centered caregiving.
Methodology
Research Design
This phenomenological qualitative study describes the lived caregiving experiences of African American women caring for older relatives to learn more about caregiving through the lens of an African-centered perspective. Phenomenology allows for examining and describing subjective meanings and emotional responses to caregiving as a research methodology. To illuminate caregiving women within the framework of Kawaida theory and the Nguzo Saba, the following research questions were raised:
• What are the caregiving experiences of professional and managerial African American women?
• What supports and approaches are available for caregiving?
Research Procedures
Following the approval and consent of the Institutional Review Board (IRB), I studied 20 African American women caregivers of older parents who are working in professional and managerial positions.
Sample
Snowball sampling, a non-probability sampling technique [40], was utilized to identify 20 professional and managerial women born between 1946 and 1964 who are caring for elderly parents with specialized knowledge of the study topic. Nineteen women described themselves as African American. One woman described herself as a Caribbean American.
Data Collection
Informed consent was obtained from each interviewee before conducting interviews. Once informed consent was obtained, 20 in-depth interviews were conducted for this study. Pseudonyms were assigned to each interviewee to ensure confidentiality in data analysis. Data was collected in semi-structured interviews.
Ethical Considerations
The researcher ensured that ethical principles were employed. Participants were fully informed about the research purpose, potential risks, and benefits. They knew they were free to withdraw from participation in the research study at any time without any consequences. Caregiver support resources were available for referral if indicated.
Data Analysis & Findings
I utilized horizontalization and reviewed statements leading to the development of a constellation of meanings and themes [41,42]. Rich, textural descriptions of caregiving were developed from the themes. I examined the thematic content for structural descriptions or the context [41,42] related to the Nguzo Saba. These textural and structural descriptions produced the universal essence of caregiving shared among African American professional and managerial women. Conceptual saturation was reached as transcripts were read and re-read. Qualitative creditability was established by documenting the research procedure while conducting the research. The documentation of research methods supports stepwise replication and confirmability. Transcripts generated from semi-structured interviews were checked to ensure accuracy. Peer debriefing was employed to ensure the perspective of another researcher who queried the researcher about the project. Rich, thick descriptions added validity by providing several perspectives on themes that support data analysis grounded in the theoretical framework to ensure structural coherence.
Findings
These perspectives inform African-centered caregiving for aging family members through the lens of the Nguzo Saba. Caregivers have mixed perceptions of caregiving. Many caregivers believe it is their responsibility to care for their parents, and they feel joy in providing care, while other caregivers feel overwhelmed and resentful about caregiving. Most caregivers experienced stress related to caregiving, caregiving tasks, and the progression and duration of caregiving. However, caregivers are resilient and resourceful, and they utilize informal and formal support to provide care for elderly relatives and various coping strategies. Preparation for caregiving is intergenerational and takes place long before actual caregiving begins. The findings relating to the principles of the Nguzo Saba are highlighted below.
Umoja (Unity)
Family members value communication, togetherness, and shared responsibility in caring for the elder. Caregivers remembered their parents caring for their grandparents as a family tradition and they felt honored to carry out and pass the torch to younger family members.
• My grandfather lived with us when he elderly, and my paternal grandmother lived with us until she died. The model was always there. Respect your elders. You take care of them, they took care of you, and that's your duty, your honor.
• My parents lived with my grandparents in the same home. My mother took care of my grandmother since the day my grandfather passed away. I watched my mother care for my grandmother my entire life. My grandmother was not incapacitated to need assistance for eating, bathing, or anything like that until she was 91. Now I call [my teenage] niece and ask her to help. Her response is, "Sure, I'll come to hang out with grandma."
• I think optimal and best caregiving would be in an environment where the whole family came together and played a vital and important role in looking at what the elder needs and how to minimize the load because everybody carries a piece of the load.
Caregivers acknowledged the role of the family in shaping values, fostering wellbeing, facilitating communication, and providing educational opportunities for family members. Caregivers spoke of their elders as trailblazers in the civil rights movement of the 1960s with pride. Their parents were race women, racial firsts, and successful entrepreneurs. The caregivers recognized they stood on the shoulders of their elders in continuing a legacy of success. They spoke of the sacrifices made to achieve intergenerational academic and career success.
• After making sure that my brother, grandmother, and I were fed, housed, and clothed properly, the most important thing for my mother, in terms of our family, was rights. Her children would have opportunities that were not hers because it was their right to have such access.
Caregivers also acknowledged the impact of family conflict between generations and among siblings in carrying out caregiving roles and responsibilities. Family conflict is often related to long-standing patterns of negative communication among parents and caregiving offspring and sibling rivalry, one person taking on more responsibility, and conflict over finances and inheritance. Caregivers desired family harmony and shared responsibility for caregiving, and sought professional help in resolving family conflict. Therapy was sought to resolve issues that emerged during the period of caregiving.
• People who enjoy their families are very supportive of caregiving, and they understand. There's always a question for people who don't enjoy family or people who have got some things going on from before that they haven't gotten over yet.
• There's always an opportunity to process because there's a lot. When you are caregiving, you subconsciously don't think about it until somebody asks you, "Oh yeah, okay, let me talk about this."
• I've had various feelings over the years. I had resentment for a while because I felt she could have done things differently in her life. It took me a while to work through that. That people do what they do and it is what it is and she's now at a stage where she needs help.
Kujichagulia (Self Determination)
Kujichagulia engages generations in establishing individual and family goals across multiple domains to ensure each family member can fulfill their destiny as the family is caring for older relatives.
• Caregiving has been passed down to me and I'm passing it on to my children.
• My cousin has a multi-generational household. My aunt, my father's sister, lived there with her daughter - my cousin who's not that young anymore; she is now 79, 80 herself - and her daughter, who is my age, 50, and all these assorted people and children.
• And maybe my situation is sort of unique in that it's not just my Mom. I have that 96-year-old and a 6-year-old dynamic going on, and both need my time and attention. I believe that part of the reason Ma is still here and still going strong is that she has things she does. And I do make sure that she's involved in some things like caring for my son.
• For my family, we recognize caregiving is a communal thing, and it doesn't fall on one person, and each person can bring their gifts to the care person.
Caregivers acknowledged the importance of having a shared vision for their lives to support interdependence among family members. A shared vision allows each family member to establish and achieve goals across multiple domains.
• My mother was very much focused on things that should be happening with us as a race, and she's always promoted that in us. Family first, race second. You ought to go for your family, and you want to do for your people. You will do it for your family, do it for your community, and do it for your people.
One caregiver acknowledged that she made her career choice by the income earning power associated with the career. She knew she had to make a significant income to take care of herself and her mother. She provides financial support to her mother because she knew she would be financially responsible for her.
• I looked in the Bureau of Labor Standards book…, and I knew I needed to have a non-traditional career because I knew I needed to make enough money to take care of me and some money to take care of her. And that was not a traditionally female career. I saw computer science and electrical engineering and I said that is it, and that's what I'm doing.
Caregivers model the aspirations and determination of their parents who were engaged in the great migration north or to the United States from the West Indies in search of a better life. The caregivers remember their parent's accomplishments with modest means and the sacrifices to benefit the family.
• For a single parent who's had to bring up a child who had to deal with a permanent disability, I'm very happy with what I have achieved, what I have accomplished. The fact that I can retire to go live with my Mama and my child is capable of moving into my house and keeping my house intact is a blessing.
Ujima (Collective Work and Responsibility)
Ujima engages families' informal social support and encourages utilizing available formal services. It takes a village to care for an elder, and this village includes both formal and informal support systems. The family system is fluid and continues to provide significant support to elders. Family is broadly defined as family, grandchildren, neighbors, kinship groups, spouses, and even former spouses.
• My immediate family, meaning my sisters and my husband, all participate; we are all supportive and do what is necessary. We keep coverage. We keep up on all of the health appointments. We participate together. We may not all be there at the same time, but we catch up with one another. So, we're all aware of my mother's state of mind and my mother's health.
Formal support services may include the Visiting Nurses Association, Meals on Wheels, in-home services, assisted living, nursing homes, respite services, hospice, and intergenerational programs. Caregivers may find themselves socially isolated in caring for an elderly relative. As the responsibilities of caregiving increase, caregivers are often reluctant to ask for assistance or to seek outside resources until they reach a point of feeling overwhelmed. When they reach the end of the rope, they are forced to decide to seek support that is in the collective best interest.
• I made a decision. I consulted with my other sibling, who doesn't live here, and we agreed to [place my mother in assisted living]. I just said, 'I can't do it anymore.' And the night I did [place her in assisted living], I just cried. But in America, you don't feel like you have a choice. There's no support other than your friends. When I placed her in assisted living, I was able to rest. It was the best rest I had in months.
Some caregivers are intentional in gaining knowledge of formal resources, including enlisting the support of a geriatric care manager and joining caregiver support groups.
• I found a caregiver support group. It was free, and I went every Monday for almost five years. In that setting, I learned a lot about resources - who to go to. I was sitting in an environment with women and sometimes men who were doing the same thing I was doing, so it was an opportunity to blow it off.
• We learned a lot about Medicare, the medical system, and the importance of being a very strong advocate for the patient. Our mother always had a favorite saying, 'Speak up, express yourself,' so we made sure we always had that capability and characteristic.
Ujamaa (Cooperative Economics)
This principle emphasizes collective economic strength and encourages families and communities to meet everyday needs through mutual support. As it applies to caregiving, the emphasis of this principle is legal and financial planning for aging and retirement, wills, and power of attorney. Caregivers state that they learned to plan for aging from what their elders did or did not do. Many of the caregivers and parents of the caregivers are prepared for aging-related expenses through savings and pensions, and they acknowledge that it is a blessing. One caregiver stated that everyone needs to have a will starting from in their 20s. Having power of attorney is essential for the financial management of the elders' finances and assets and for making health care decisions.
• My name was on the house from the time I can remember. It was never an issue when she decided that it was time for me to take over. When she had to go on Medicaid, there was never an issue - not that the house is worth a lot, but they couldn't get at it. She had an advance directive, and she had a living will. When she could no longer handle her responsibilities, it was easy for me to do what needed to be done.
Home ownership is an important asset that can serve as a family home where children, grandchildren, or kin can live economically while caring for the elder within an extended family. Home ownership can also pay for care in the event assets are not protected.
• We turned the basement into a whole suite for her, put a new bathroom down there, took up the floor, put a new floor, walls, everything. And at a certain point in your life, your house is supposed to take care of you. If you have a house, you're so fortunate. That's what it's for.
Preparing financially for aging makes a difference in the quality of life for both the caregiver and the elder. Persons who have financial resources can hire help or pay for respite care, which makes a difference in caregiving stress levels. The hired support can include hiring family members to increase family members' income.
• The bigger challenge is people who don't have the resources. How do they cope? But people who are just making ends meet, how do they deal with this and how do they deal with the stress of it? I think it's a big challenge.
Conversely, the financial burden is overwhelming for persons struggling to make ends meet. The challenges include the inability of the caregiver to meet their own needs and the person they are caring for.
• The challenge is my employment has changed, so my financial situation is horrible. My brother, even though he is far away, is good support. He'll send my mother money if I call and say and touch base with him. Say my mother needs x, y, and z. You need to send this. He's very good about doing that.
Many of the elders were financially savvy, and they were able to accumulate assets initially through thrift, home purchasing, investing, and transferring assets to younger family members.
• Well, fortunately, mother is financially pretty good. She and daddy didn't spend a lot. We have people in the family who knew a lot, and I knew a lot [about investing and managing assets]. Mother's income pays for everything that she needs. She is fortunate enough to have resources that gave us options, and that's probably not the norm.
Nia (Purpose)
Caregiving with purpose is a life mission that is carried out to leave a legacy and contribute to the family and community. How caregivers define themselves as caregivers, and how they engage in self-care to fulfill the commitment to self and others.
• Giving to her and making sure she's comfortable are the most important parts of my life. That is my mission. When that mission is done, then I'll be able to relax. It is exhausting in that I'm thinking all the time. When I get up I schedule her day in my mind, and then I communicate it to her when I call her first thing in the morning.
Purpose in caregiving is creating balance in caring for others while caring for self so that one can bring their best self to the caregiving process. It requires a level of awareness and intentionality in caregiving. Many caregivers are engaged in self-care that includes preventative health maintenance, nutritional management, exercise, therapy, and support groups.
• Caregiving is life for me. You have to be watchful of the person that you're caring for. You have to be in tune with that person you're loving, and it will give you the joy you're looking for. The joy that you're experiencing with the person. You're producing a relationship.
• You're creating an experience. It's not a chore. It's a part of your life. It's the travel. It's the journey. It is life. That's the way I see it.
• I just had a physical. So far, so good. I expect results from treating my body and my soul very positively.
• I ride my bike. I am in various social networks. That helps me, where I can just forget about it. Sometimes I will go to church. Sometimes I'd read some completely escapist book. I talk to those two or three girlfriends who are going through caregiving. It's not really a formal thing that we have. Whenever one of us is going through something, one of us will call the other one and just talk. And then, at the end, we are laughing or something. Because sometimes you don't want to talk about caregiving. You just want to laugh.
Some caregivers state that they do not have the time or resources to engage in self-care, and their health and quality of care are compromised. They report numerous health conditions, depression, and being quick-tempered with the elder.
Kuumba (Creativity)
This principle highlights creative energies to build and maintain a vibrant and robust community for caregivers and elders. Caregivers report engaging their parents in recreational and creative endeavors either at home, in adult day-care, or in church-related activities. Kuumba is also related to creating beautiful spaces and maintaining elder glamour routines.
• My Mom is an atypical 96-year-old because she is far from a feeble little person sitting in a chair who can't do anything for herself. She's vivacious, and she has her routines that she still wants to do. For the past 25 years, she has been growing food in her backyard. One of her big things is to tend her yard - her garden, every morning. Her doctor feels it has probably kept her going as long as she has. She's got a daily routine, 'I got to go dig in my yard.'
• I remain in a state of gratefulness and seek things that will orient me towards peacefulness and keep me grounded. Music is one thing, and singing is awesome to me.
Maintaining hair care is essential for the self-esteem of older women, and finding African American stylists in an assisted living can be a challenge. Extra effort is made to maintain hair care and other beauty routines.
• You look at my nails, and you look at her nails. Her nails are always manicured and polished. Her hair was thinning, so she keeps her hair cut short, and she has a texturizer. She wanted to look good because she was going to the theatre.
Imani (Faith)
The principle of faith provides strength and guidance during the caregiving process. Prayer, meditation, religious and spiritual reading, pastoral care, devotional prayer, and traditional healing practices support faith. As an active principle, faith is a way of being throughout the life course. Caregivers feel that God is always near and available for a conversation. Caregivers expressed relying on faith to cope with caregiving. Faith and religion have been a part of the caregivers' experience since their formative years, and they rely on faith in their daily walk.
• What I have discovered is that, in this process, is that God is able to keep you and give you strength.
• You still remember all the lessons, and all the mysteries, and all the mystique. But even more importantly, I get to see the miracles often. That keeps my faith fresh for me. I do my reading and meditation, and I get to see the fruit of the Spirit. That's when you know you're in the Spirit when you get to see the work of God, just in your daily walk.
• I remember praying,''Oh God, what am I going to do. And immediately felt this answer come back, and God said, """''Well, you know, you're going to have to be with them during those hard times - through death or whatever.'"
• For me, the spirit is everything. I believe that God has got me, no matter what. So, I'm very, very faithful. I'm in church every Sunday I'm in town, and sometimes when I'm not in town. I'm a strong believer in God, and my faith is very strong.
• I learned to read from my grandparents' Bible. But even more importantly, I get to see the miracles often. That keeps my faith fresh for me. I do my reading and my meditation. I get to see the work of God in my daily walk. I see the fruit of the Spirit.
Results
The findings of this research are based on the intersection of race, gender, and culture to provide a lens to describe caregiving and identify new insights into caregiving among African American women. While the focus of this research was on professional and managerial African American women, the application of Kawaida and the principles of the Nguzo Saba apply to African Americans across educational attainment and income levels. The following is a summary of the findings as it applies to the Nguzo Saba:
The principle of Umoja (Unity) focuses on giving meaning to family elders, creating opportunities for intergenerational communication, and healing family conflict. Caregivers describe the evolution of family unity, established over time through family traditions and reunions, communal caregiving, and passing on the legacy of caregiving. There is a sense of pride in the struggles the person being cared for overcame during periods of overt and systemic racism. When family conflict and perceptions of caregiving became overwhelming, the caregiver obtained therapy.
The principle of Kujichagalia (Self Determination) can be described through intergenerational caregiving, living within an extended family where members identify common interests and make personal, educational, and career decisions in the collective interest of the individual and the person being cared for. Caregivers reported being guided by the legacy of determination in the face of struggle the elder made over the life course that has allowed them to live a comfortable life and they want to reciprocate by ensuring the elder receives the best care possible. This category includes career decisions, residence decisions, and a legacy of care.
The principle of Ujima (Collective Work and Responsibility) engages the family in informal support in meeting the activities of daily living and instrumental activities of daily living through mobilizing the family and accessing formal support services when necessary. Caregivers report that this principle involves planning, education, and advocacy to corral resources from family check-ins, home health care, and placement in assisted living and hospice. As conditions advance, the caregiver must become more knowledgeable about the range of services available. Caregiver support groups are instrumental in learning about the eldercare landscape.
The principle of Ujamaa (Cooperative Economics) addresses the financial and legal aspects of caregiving through planning before the person being cared for becomes incapable of making decisions. Caregivers report learning about financial planning through wise elders who practiced frugality with modest means and could save so they could take care of themselves. A level of legal and financial savvy is required to protect assets and or utilize assets for the care of the elder. Many of the stressors of caregiving are financially related. Caregivers also access public and nonprofit services such as home aids and meal delivery and request financial support from siblings.
In the principle of Nia (Purpose), the caregiver assumes the role identity of caregiving with intentionality. Caregivers acknowledge that caregiving is demanding and they engage in self-care to bring their best self to the caregiving process. Caregiving is about perspective and having a positive mindset about caregiving even in the hard times. Caregivers acknowledge that they are not always engaged in self-care, or they have a negative attitude about caregiving which impacts the quality of care provided to the elder.
The principle of Kuumba (Creativity) recognizes that the elder still appreciates culture, beauty, and art. Caregiving is not simply about meeting the activities of daily living and instrumental activities of daily living, rather Kuumba expands caregiving to include inspiration. The elder is not their diagnosis. In Kuumba, the caregiver and the person cared for are involved in physical, creative, and grooming activities to bring grace and beauty into their lives.
The principle of Imani (Faith) has been the bedrock of coping for African American women since they were children, and their faith is extended into caregiving. Caregivers report a deep and personal relationship with God that is supported through prayer, meditation, and witnessing miracles in everyday life. This relationship with God supports caregivers in meeting caregiving demands and making decisions.
Discussion
The African-centered social worker uses the Nguzo Saba in psycho-social-spiritual assessment, intervention, and evaluation of social work intervention. The application of the Nguzo Saba requires the social worker to be a competent micro and mezzo practitioner to meet the holistic needs of the caregiver within the context of family, community, history, African culture, and African principles. This is the critical difference between African-centered caregiving interventions and caregiving interventions targeted at the general population of caregivers. Kawaida theory and the Nguzo Saba are a way of living and being, and the principles must be internalized as a way of life. The role of the social worker is to internalize the Kawaida theory and the principles of the Nguzo Saba through (1) Sankofa: to return and reconstruct African culture; (2) Nguzo Saba: to imagine a new way of being; (3) Kwanzaa: to reinforce the principles of the Nguzo Saba; and (4) Family, Community and Culture: Spiritual grounding, reflection, action and giving thanks [37]. The African-centered social worker is grounded in the Nguzo Saba principles as a philosophy of practice and a way of life. Umoja focuses on giving meaning to family elders, creating opportunities for intergenerational communication, and healing family conflicts. Kujichagulia engages generations in establishing individual and family goals across domains to ensure each family member can fulfill their destiny while caring for the older family members. Ujima engages families' informal social support and encourages utilizing available formal services. Ujamaa focuses on financial planning and preparation for aging, such as power of attorney. It promotes cooperative economics and the generation of capital to serve older adults in the community. Nia encourages family members to identify their purpose in caregiving and engage in self-care to carry out the commitment to self and others with the highest level of compassion. Kuumba recognizes the creative energies of elders and their caregivers and promotes application of the arts to create beauty and meaning in their lives. Imani engages the caregiver and elder in spiritual support to cope with caregiving challenges and prepare for the end of life. Application of the Nguzo Saba to caregiving supports both objective and subjective transformation. The Nguzo Saba promotes healing through shaping a African-centered caregiving approach that provides a purpose, direction, and caregiving support.
Caregiving can be a time of family conflict between the caregiver and the person cared for, siblings, and extended family members. An African-centered psychosocial assessment can determine family history, values, and actions in caring for elders, the quality of intergenerational and sibling relationships, and the extent to which there is unity in the family through periodic gatherings and family reunions. Genograms are designed for use with African American families to gather information and assess cultural values, thinking, spirituality, and traditions [43]. A genogram can be a valuable tool to assess the quality of family relationships within and across generations for both individuals and the family. Therapy can heal relationships and improve communication skills to support caregiving.
Social workers can employ coaching to support the caregiver, the family, and the elder in creating a vision and implementing the vision for their lives to achieve individual, family, and community goals. Coaching can activate the principle of Kujichagulia (Self Determination) to build support to achieve family goals. The caregiving period can be protracted and life goes on even while caregiving. There are experiences that everyone wants to have from age five to 95 in the following domains of life: spirituality, family, career, education, personal growth, health, finances, and recreation. Kujichagulia supports the intentionality of achieving continued growth and development goals even while caregiving.
It takes a village to care for an elder, both formal and informal resources are needed to support the caregiving process through Ujima (Collective Work and Responsibility). On an informal level, Ujima involves visiting, providing respite care, assistance with shopping, cooking, cleaning, and activities of daily living. On a formal level, Ujima is becoming knowledgeable and connecting with the vast array of community-based and institutional support resources available in the community, from home health care aids to hospice. The role of social workers in Ujima is to identify informal sources of support for different situations and to build caregiver skills in asking for help. Social workers must also be very knowledgeable about the formal resources that are available, eligibility requirements, costs, and referral process. Participation in an African entered caregiving approach does not preclude participation in formal services. Social workers' engagement in aging networks supports the information and referral process to available community-level resources.
Addressing Ujamaa (Cooperative Economics) requires competency in financial social work to assist caregivers in developing financial skills in elder financial management, including financial planning and budgeting. Social workers need to know about the public and private sector resources based on income so that elders with limited financial means can access goods and services that improve their quality of life. Families need to assess the elder's finances with the elder, determine assets, available income, and cash flow to make decisions about housing, medical management, and asset protection. Legal consultation is required to develop wills, trust, and power of attorney. Ideally, financial planning should occur before retirement and incapacitation. The role of social workers is to use financial social work skills and develop a network of financial and legal professionals for the referral [44].
Nia (Purpose) focuses on the caregivers' self-care to fulfill the purpose of caregiving. Social workers can support clients in defining their purpose for caregiving and in living in alignment to create a legacy of care. Nia recognizes a balance in caregiving, giving to others and to self. While the focus is on the elder's needs, the caregiver has health and mental health needs that must be addressed to reduce the health and mental health risks associated with caregiving. Social workers ensure clients follow health care and health promotion protocols developed by appropriate health professionals.
Kuumba (Creativity) is the recognition that aging is also about beauty, joy, and creativity, expression in art, music, dance, theatre, and gardening. The African-centered social worker creates opportunities for cultural expression and beauty. There is more to aging than medical management, and the person is not their disease and can still enjoy and benefit from creative outlets. The African centered social worker creates the opportunity for cultural expression and community celebrations for the caregiver, the elder, and the community.
Imani (Faith) requires the African-centered social worker to be grounded in spirituality as the essence of all of life. The social worker can support clients in utilizing religion and spirituality as a philosophy with practical applications for coping with life, caregiving, and end-of-life decisions. The African-centered social worker is competent in spiritual social work with African Americans, respecting the diversity of religions and expressions of spirituality within the African American experience. The African-centered social worker supports the client in utilizing spirituality as a coping tool and a way of life.
The African-centered social worker collaborates with social workers and other professionals to address the broad needs of caregivers and the elders and to create a comprehensive and communal approach for support by applying the Nguzo Saba principles. The collaboration includes family therapists, coaches, care managers and managers, financial social workers, attorneys, art therapists, artists, and social workers with experience in pastoral care and an orientation toward African-centered practice.
Conclusion
The future direction for African-centered social workers in gerontology practice is to continually build personal and professional clinical competencies to bring forth the best of African history, culture, and customs into personal and clinical competencies. This is a mandate for social work education to teach and train students on "perspectives, concepts, and theories that have proven critical to effectively work with African American people and communities [45]." The Nguzo Saba are not just something that a social worker does. It is a way of life, a way of being in the world, personally and professionally. The African-centered social worker acknowledges the limitations of evidence-based practice and takes constructive action in designing interventions for caregivers grounded in African-centered theory and demonstrated effectiveness in practice evaluation. Future directions can include developing an African- centered psychosocial, spiritual assessment tool to address the multi-dimensional needs of African American caregivers, taking into account race, culture, history, family, and community.
The principle of Ujamaa, cooperative economics, presents an opportunity to build businesses providing an aging service. As the African American aging population continues to expand, there is a need for assisted living group homes, adult day centers, respite care, home health aides, and transportation services with an African centered focus. The establishment of businesses created for African American elders can ensure quality, African-centered service and generate income and employment opportunities within the African American community.
African-centered approaches to caregiving hold great promise for honoring African American elders with dignity and respect, supporting the caregivers through the conscious application of the principles of the Nguzo Saba, and providing spiritual grounding and connectedness to the circle of life.
Those who respect the elderly pave their own road toward success.
Competing interest:
The authors declare that they have no competing interests.
References
Fairfax, C. (2017). African philosophy: The center of African centered social work. Journal of Human Behavior and the Social Environment, 27(1-27-14).View
Administration for Community Living, Administration on Aging. (2021). 2020 Profile of Older Americans of African Americans Age 65 and Older. U.S. Department of Health and Human Services. Retrieved May 11, 2022, from https://acl. gov/sites/default/files/Aging%20and%20Disability%20in%20 America/2020Pr ofileOlderAmericans.Final_.pdfView
Crewe, S., & Gadling-Cole, C. (2015). African American caregivers: Seasons of care practice and policy perspectives for social workers and human service professionals. Nova Science Publishers. 30 View
Hill, R. (1971). The strength of black families. Emerson Hall. View
Hill, R. (1993). Research on the African American family: A holistic perspective. Auburn House.View
Myers, L. (1988). Understanding an Afrocentric worldview: Introduction to an optimal psychology. Kendall Hunt.
Nobles, W. (1980). African philosophy: Foundations for black psychology. In R. Jones, Black Psychology (pp. 23-55). Harper and Row.
Schiele, J. (2010). Human services and the Afrocentric paradigm. New York: NY: Routledge.
Sheridan, M., Burley, J., Hendricks, D., & Rose, T. (2014). Caring for one's own: Variation on the lived experience of African American caregivers of elders. Journal of Ethnic and Cultural Diversity in Social Work, 23(1), 1-19. doi:10.1080/15 313204.2013.849642 View
Ross-Sheriff, F., & Swigonski, M. (2009). Caregiving for the elderly: Personal and professional response. Affilia, 24, 221-225. View
Vickrey, B., Strickland, T., Fitten, L., Adams, G., Ortiz, F., & Hays, R. (2007). Ethnic variations in dementia and caregiving experiences: Insights from focus groups. Journal of Human Behavior in the Social Environment, 15, 233-249.View
AARP. (2020). Caregiving in the US. AARP and National Alliance for Caregiving. doi:10.26419/ppi.00103.001View
Deskins, B., Letvak, S., Kennedy-Malone, L., Rowsey, P., Bedine, L., & Rhew, D. (2022). The experiences of African American male caregivers. Healthcare (Basel), 10(2). doi:10.3390/healthcare10020252View
Dilworth-Anderson, P., Moon, H., & Aranda, P. (2020). Dementia caregiving research: Expanding and reframing the lens of diversity, inclusivity, and intersectionality. The Gerontologist, 60(5), 797-805. doi:10:1093/geront/gnaa050 View
Siegler, I., Brummett, B., Williams, R., Haney, T., & Dilworth Anderson, P. (2010). Caregiving, Residence, Race, and Depressive Symptoms. Aging & Mental Health, 14(7), 771-778. View
Thorne, C. (2020). African American professional and managerial women's journeys through caregiving for elderly parents. Journal of African American Studies, 24, 238-257. doi:10.1007/s12111-020-09480-9 View
Eifert, E., Adams, R., Morrison, S., & R, S. (2016). Emerging trends in family caregiving using the life course perspective: Preparing health educators for an aging society. American Journal of Health Education, 47(3), 176-197. doi:http://doi.or g/10.1080/193250037.20161158674View
Gadling-Cole, C., & Williams, G. (2014). African American Caregivers of Older Adults: An Overview. In C. Gadling-Cole, & S. Crewe, African American Caregivers: Seasons of Care Practice and Policy Perspectives for Social Workers and Human Service Professionals (pp. 1-15). Nova Science Publishers. Retrieved May 11, 2022View
Cannon, S., & Fawcett, J. (2018). Correlates of psychological and physical health outcomes among African American caregiving daughters. Association of Black Nursing Faculty, 86 97. Retrieved March 15, 2019View
Weiss, D. (2015). Caregiving in the African American community: An examination of mental health and well being. In S. Crewe, & C. Gadling-Cole, African American Caregivers: Seasons of care. Practice and policy perspectives for social workers and human service professionals (pp. 63-78). New York.
Samson, Z., Parker, M., & Dye, C. H. (2016). Experiences and learning needs of African American family dementia caregivers. American Journal of Alzheimer's Disease & Other Dementias, 31(6), 492-501. Retrieved May 11, 2022, from https://journals. sagepub.com/doi/pdf/10.1177/1533317516628518View
Dilworth-Anderson, P., Williams, I., & Gibson, B. (2002). Issues of race, ethnicity, and culture in caregiving research: A 20year review. The Gerontologist, 42, 237-272.View
Chinn, J., Martin, I., & Redmond, N. (2021). Health equity among Black women in the United States. Journal of Women's Health, 30(2), 212-219. doi:10.1089/jwh.2020.8868 View
Woods-Giscombe, C. (2010). Superwoman Schema: African American Women's Views on Stress, Strength, and Health. Qualitative Health Research, 20(5), 668-683View
Childs, J. (2020). Effects of stress on the health of African American women in low income neighborhoods. McNair Scholars Research Journal, 13(5), 28-44. Retrieved February 5, 2022, from https://commons.emich.edu/cgi/viewcontent. cgi?article=1155&context=mcnairView
Belgrave, F., & Abrams, J. (2016). Reducing disparities and achieving equity in African American women's health. American Psychologist, 71(8), 723-733. doi:10.1037/a0026325View
Hall, J., Everett, J., & Hamilton-Mason, J. (2012). Black women talk about workplace stress and how they cope. Journal of Black Studies, 43(2), 207-226. View
Beauboeuf-Lafontant, T. (2009). Behind the Mask of the Strong Black Woman: Voice and the embodiment of a costly performance. Temple University Press.View
Greer, T. (2011). Coping strategies as moderators of the relations between individual race-related stress and mental health symptoms for African American women. Psychology of Women Quarterly, 35, 215-226. View
Lacizzo-Mourey, R., Besser, R., & Williams, D. (2021). Understanding and mitigating health inequities- past, current, and future directions. New England Journal of Medicine, 384, 1681-1684. doi:10.1056/NEJMp2008628 View
National Academies of Sciences, Engineering, and Medicine. (2016). Families caring for an aging America. In R. Schultz, & J. Eden. Washington, DC: National Academies Press. Retrieved July 30, 2019, from https://www.johnahartford.org/ images/uploads/reports/Family_Caregiving_Report_Natio nal_ Academy_of_Medicine_IOM.pdfView
Gitlin, L. M. (2015). Translating evidence-based dementia caregiving interventions into practice: State-of-the-science and next steps. The Gerontologist, 55(2), 210-226. doi:10.1093/ geront/gnu123 View
Bakas, T., Clark, P., Kelly-Hayes, M., King, R., Lutz, B., & Miller, E. (2014). Evidence of stroke family caregiver and dyad interventions: A statement for healthcare professionals from the American Heart Association and American Stroke Association. Stroke, 45(9), 2836- 2852. View
Keller, A. (2020). A health life for African American Healthy Women caregivers: A concept mapping study. Health Equity, 31(2), 130-139. doi:10.1016/j.whi.2020.11.011View
Bent-Goodley, T., Fairfax, C., & Carlton-LaNey, I. (2017). The significance of African-centered social work for social work practice. Journal of Human Behavior in the Social Environment, 27(1-2), 1-6. doi:10.1080/10911359.2016.1273682View
Harvey, A. (2018). A Reader of Afri-Centric Theory and Practice: Philosophical and Humanistic Writing of Aminifu Harvey. Third World Press Foundation.View
Karenga, M., & Karenga, T. (2007). The Nguzo Saba and the Black family. In M. H.P., Black families.: SAGE publications. View
Karenga, M. (2008). Kawaida and questions of life and struggle.: University of Sankore Press. View
Karenga, M. (2008). Kwanzaa: A celebration of family, community and culture. University of Sankore Press.
Engel, R., & Schutt, R. (2017). The Practice of Research in Social Work. Sage.View
Creswell, J. (2007). Qualitative inquiry & research design: Choosing among five approaches. Sage Publications.View
Moustakas, C. (1994). Phenomenological research methods. Thousand Oaks, CA: Sage. View
McCullough-Chavis, A., & Waites, C. (2008). Genograms with African American families: Considering cultural context. Journal of Family Social Work, 8(2), 1-19. View
Thorne, C., Crewe, S., & Mendez, G. (2019). Struggling to make ends meet: The impact of economic distress on older persons. In J. Edwards, & L. Openshaw, Empowering clinical social work practice during a time of global economic distress. Washington, D.C.: National Association of Social Workers.
McPhatter, A. (2016). Urban social work with African Americans. In R. Wells-Wilbon, A. McPhatter, & H. Vakalahi, Social work practice with African Americans in urban environments (pp. 1-19). Springer. View