
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 5 (2023), Article ID: JMHSB-176
https://doi.org/10.33790/jmhsb1100176Review Article
Telehealth Suicide Assessment and The Emergency Order of Detention (EOD) Process: A Systematic Review
Kathryn L. Diebold1*, Christopher Graham1, Martine Laventure1, NaKeisha Williams1, and Shahnaz Savani2
1 School of Social Work, Tulane University, New Orleans, LA, United States.
2 University of Houston- Downtown, Houston, TX, United States.
Corresponding Author Details: Kathryn L. Diebold, School of Social Work, Tulane University, New Orleans, 127 Elk Pl, New Orleans, LA 70112, United States.
Received date: 14th December, 2022
Accepted date: 12th January, 2023
Published date: 14th January, 2023
Citation: Diebold, K. L., Graham, C., Laventure, M., Williams, N., & Savani, S., (2023). Telehealth Suicide Assessment and The Emergency Order of Detention (EOD) Process: A Systematic Review. J Ment Health Soc Behav 5(1):176.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Emergency orders of detention (EOD) are used to hold potential suicidal individuals against their will. The COVID-19 pandemic altered the way these evaluations are conducted as virtual telehealth conferences became more frequently utilized. The purpose of this review is to identify screening practices of telehealth providers, describe assessment discrepancies used in telehealth versus in-person visits, and identify variance in EOD hospital admission rates.
Methods: A systematic review of literature was conducted utilizing the PRISMA model. Five electronic databases were searched for articles related to suicide, EOD, and telehealth spanning from 2001 to 2021. Of the eight (n=8) articles returned by the search, three (n=3) met inclusion criteria.
Results: Findings of this review reveal that there is virtually no research on standardized suicide screening tools used to make EOD determinations. Additionally, the research does not comment on discrepancies between suicide evaluations via telehealth or in-person. Research on telehealth evaluation and involuntary hospitalization rates is limited.
Discussion: Little is described in the current research about the types of assessment tools used in the EOD process when conducted via telehealth. Overall, this review found that protecting citizens by telehealth EOD is noticeably under-researched.
Keywords: Emergency orders of detention (EOD), Telehealth suicide assessment, Involuntary hospitalization, Telehealth suicide evaluations
Introduction
Suicide is a major public health problem in the United States, claiming the lives of 47,511 people in 2019 [1]. Suicide is the second leading cause of death for people between the ages 10 and 34, and the fourth leading cause of death for those between ages 35 and 44 [2]. Additionally, 1.38 million Americans attempted suicide and 4.8% of adults reported serious thoughts of suicide in 2019 [2,3]. People living with a mental health diagnosis and history of suicidal behaviors are at increased risk for suicide [4]. Additionally, research has found that one in 10 people who died by suicide had visited the emergency room in the two months prior to their death [5]. Studies have also found that 57% of people who died by suicide had a history of contact with a mental health professional in the past, with 31% having contact in the 12 months prior to their death [6]. Medical doctors and licensed social workers regularly encounter people at risk and can play an important role in suicide prevention efforts. One commonly used effort to address suicide is the emergency order of detention (EOD) process. EODs involve clinical assessment of risk, legal procedures, and involuntary detainment of an individual who presents as a danger of harm to self or others [7]. EODs are increasingly being issued via telehealth, especially during the pandemic; however, research is limited on both the use of telehealth in the EOD process and the types of clinical instruments that are used to assess for suicidality during this process.
The EOD process is centered around two key ideas: parens patriea and civil commitment. Parens patriea, Latin for “parent of his country,” is a legal concept that describes a governing body’s responsibility to protect a person who is a potential danger to themselves or others and hold them against their will [8]. When a person is detained under parens patria, further evaluation occurs to determine if longer detention is needed for mitigation of risk. If further detention is deemed necessary and the person is admitted to a higher level of care, this is referred to as civil commitment. Depending on geographic location, this process may also be referred to as an emergency petition (EP), emergency hold, involuntary commitment, or a mental health warrant. In this article, the process will be referred to as emergency order of detention (EOD).
EODs aim to identify patients who are at the highest risk for attempting suicide to further assess their mental health and determine the appropriateness of additional intervention or treatment [9]. Through an EOD, a patient who is deemed a danger to themselves can be held at a facility against their will and provided treatment with the overall goal of preserving the physical safety of the individual. EODs are meant to be short term, with the length of allowable involuntary commitment varying across states from two days to two weeks [10]. Although the exact number of involuntarily commitments issued each year in the United States remains unclear due to lack of reporting and differing EOD procedures across states [11], one recent study estimated that incidences of involuntarily commitment have increased 33-fold across 25 states between 2011 and 2018 [12]. EODs are issued during in-person encounters at emergency rooms and remotely via telehealth programs.
Telehealth is the practice of providing clinical services such as medical, mental health, and substance use counseling to patients using telephonic and web-based applications [13]. The use of telehealth has increased with the onset of COVID-19 due to its ability to connect patients to treatment while maintaining social distancing [14]. Recent studies indicate that 87% of behavioral health providers, including social workers, in the U.S. use telehealth to deliver services to their patients [15]. In addition to the benefit of social distancing, telehealth has the potential to remove barriers to treatment by connecting patients to services that are otherwise inaccessible to them, especially those living in rural and tribal areas [16,17]. Telehealth also allows for remote assessment of an individual prior to issuing an EOD and ambulance transport to a hospital where further observation may be provided [18].
Programs aimed at reducing suicidality using telehealth have demonstrated promising results [19-22]. However, there is concern among social workers and other mental health professionals regarding the accuracy of suicide risk assessments administered via telehealth. A 2019 study conducted by Gilmore & Ward-Ciesielski that surveyed 52 mental health providers across 26 states found that providers believed that it was not possible to conduct a thorough suicide assessment over telehealth due to their inability to read body language and non-verbal cues [23].
To contend with the country’s rising suicide risk, provider apprehensions related to accuracy of suicide assessment via telehealth during the EOD process must be addressed. Accurate suicide assessment during the EOD process is paramount to ensuring the safety of the suicidal individual. The consequence of error in this screening could lead to the consumer’s prolonged suffering at minimum and death at maximum. Additionally, if a low-risk individual is inaccurately screened, the wrongful detention of this person under an EOD would be a violation of their right to self-determination and a misuse of already sparse high-intensity resources. Inaccurate assessment carries serious ethical implications for clinicians and hospital systems, as well as suffering for individuals and families involved.
To ensure proper suicide assessment, the use of standardized suicide risk assessments in hospital emergency rooms and inpatient settings has become a well-established practice of suicide prevention efforts and the EOD process [24]. Several tools have been developed to assist providers in accurately assessing for suicide risk with the goal of early detection, intervention, and the determination of need for longer detention [25]. Such instruments are backed by research evidence as valid measures that reliably predict suicidality. These instruments include the Patient Health Questionnaire-9 (PHQ9), the Columbia-Suicide Severity Rating Scale (C-SSRS), and Collaborative Assessment and Management of Suicidality (CAMS) [26,27,28]. It is unclear if standardized instruments are being used by psychiatrists and social workers during the EOD process via telehealth, as research is scant in this area. Furthermore, it is unclear if suicide assessments conducted via telehealth produce fewer or more involuntary holds versus assessments conducted in person. The purpose of this systematic review is to (1) identify the suicide assessment instruments used to evaluate suicidality by telehealth providers during the EOD process, (2) describe the consistency or discrepancy between suicide assessment instruments used in-person as opposed to telehealth during the EOD process, and (3) determine if there is a difference in the number of EOD involuntary holds and hospital admissions rates among patients assessed via telehealth compared to in-person.
Materials and Methods
A systematic literature review was conducted utilizing the PRISMA framework. Five electronic databases (PsycINFO, MEDLINE, CINAHL, SocINDEX, and Academic Search Complete) were searched across 20 years between January 1, 2001, through December 31, 2021, to identify studies that reported quantitative or qualitative data on the use of standardized instruments during the EOD process via telehealth. Our search occurred between November 15, 2021, and November 27th, 2021. The Boolean search strategy matched the following criteria: (1) suicid* and civil commitment or involuntary commitment or mental health warrant or emergency order of protection or emergency detention or parens patriea (2) telehealth or telemedicine or telemonitoring or telepractice or telenursing or telecare and, (3) published as peer reviewed. Exclusion criteria included: (1) studies that did not specifically include suicide, civil commitment, or involuntary commitment or mental health warrant or emergency order of protection or emergency detention or parens patriea (2) studies that did not specifically include telehealth or telemedicine or telemonitoring or telepractice or telenursing or telecare (3) review articles (4) theoretical articles, and (5) letters to the editor.
The search returned eight articles, two articles in PsycINFO and six articles in MEDLINE. The abstracts of the eight articles were reviewed by each member of the four-person research team to determine if the article met inclusion criteria. Following each member’s individual review, the team met collectively to determine which articles met inclusion criteria and which articles to exclude. Inclusion criteria included: (1) articles were required to incorporate suicide assessment, (2) telehealth, and (3) the emergency order of detention process. Articles that did not address all three of these areas were excluded from the review. Articles with a primary focus on the pediatric population were also excluded due to the uniqueness of pediatric mental health assessment. Following evaluation of inclusion and exclusion criteria, three articles (n=3) were included in the systematic review. The three articles that met inclusion criteria were independently coded by each member of the team. Coding was completed using a data abstraction form, developed to synthesize findings from all three articles. That data abstraction form was used to systematically extract core study components including (1) the types of suicide assessment instruments used to evaluate suicidality during the EOD process via telehealth, (2) the consistency or discrepancy between suicide assessment instruments used in-person versus in telehealth EOD process, and (3) rates of hospitalization for in-person versus telehealth visits. Each study was coded for demographics (i.e. population, sample size, age, gender) and study characteristics (i.e. methods). In addition, studies were coded for suicide instruments, consistency/discrepancy of evaluation methods, and hospitalization rates.
Results
A total of three studies were included in the systematic review (see Table 1). One study (33%) was published in the 2008, one (33%) in the 2019, and one (33%) in 2020. Two out of three studies were conducted in rural areas. Methodologically, two studies used quantitative research methods and one was a narrative summary of the VA’s practices related to suicide assessment. Vakkalanka et al. [29] collected data from administrative claims, telemedicine provider logs, and chart reviews of hospital records. Fairchild et al. [30] collected data from hospital patient records and analyzed the data using independent t-test, ANOVA, and logistic regression. Godleski et al. [31] summarized the U. S. Department of Veterans Affairs’ (VA) current practices of conducting suicide assessments via telehealth.
Only two studies (66 %) reported clear sample details and all studies (100%) reported gender demographics. The outcomes across studies varied, with one study focused on emergency department length of stay among patients who received telemedicine, another on characteristics of patients who received a tele-mental health intervention, and the third reported on the VA’s best practices of remote telehealth suicide assessments. None of the studies reported on specific instruments used during suicide assessments via telehealth or in-person patient evaluations, nor did they describe consistency or discrepancy between suicide assessments used. One of the three studies reported on hospitalization rates of telehealth versus in-person patient assessments.
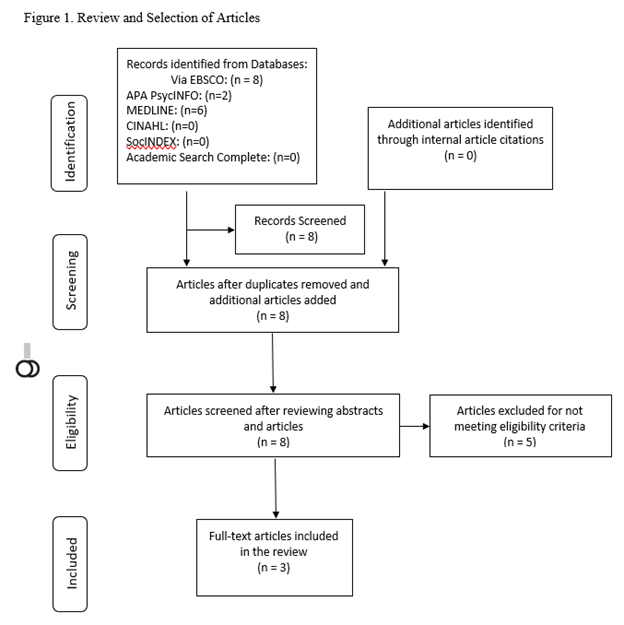
Figure 1: Review and selection of Article
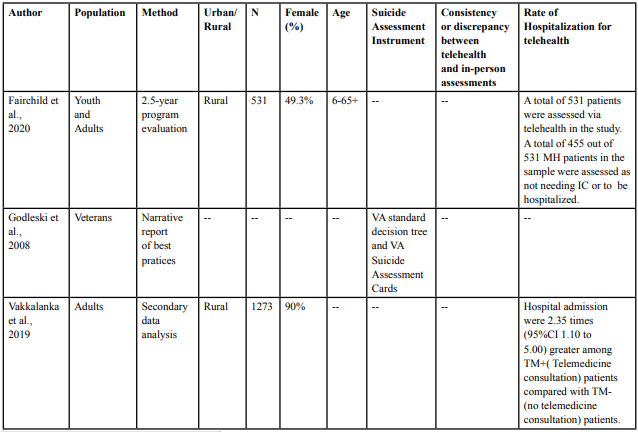
Table 1. Studies Included in the systematic review
Godleski et al. [31] reviewed the U. S. Department of Veterans Affairs’ (VA) best practices in evaluating suicide risk via remote telehealth assessment. The VA operates one of the largest telehealth networks in the country, utilizing remote sites for videoconferencing, in-home videophone, and in-home messaging devices. The article provided information on the VA’s remote care model and suicide prevention efforts, identified best practices in assessment via telehealth, and discussed legal concerns associated with detaining patients with suicidal or homicidal ideation via involuntary commitment. The authors aimed to establish better access to care for veterans and liability reduction for providers by identifying procedures for clinical assessment via telehealth. The authors identified four main best practices (1) practicing telehealth within local legal regulations and policies, (2) using clinical judgement to guide patient selection for remote video suicide assessments, (3) utilizing accepted suicide assessments and procedures, and (4) establishing contingency strategies during remote suicide assessment including plans for equipment failure and police back-up in the event involuntary commitment is warranted. The article reported on the standardized decision tree used by the VA for suicide assessments conducted via telehealth, however it did not elaborate on what types of instruments are utilized in this tree. VA Suicide Assessment Cards, based on the American Psychiatric Association’s Practice Guidelines for Assessment and Treatment of Patients with Suicidal Behaviors and the work of Rudd et al.[32], were mentioned. However, it unclear if these VA Suicide Assessment Cards are used in the assessment of patients presenting in-person and via telehealth, as the articled stated that the cards are not specific to telehealth practice.
Vakkalanka et al. [29] examined the impact of telemedicine in relation to clinical management and outcomes of patients with suicide attempts or suicidal ideation presenting in rural emergency rooms. The study population included patients who presented with a suicide attempt or suicidal ideation at 13 rural emergency departments utilizing a telemedicine network. The primary outcome of interest was emergency department length-of-stay among patients who received telemedicine assessment and intervention in comparison to patients who did not receive telemedicine. The secondary outcomes of interest included admission proportion, use of chemical or physical restraint, 30-day emergency departments return, involuntary detention orders, treatment/follow-up plan, and 6-month mortality. The study results suggested that telemedicine did not have any influence on the mean length of stay for clients in emergency departments. The study found that hospital admissions was 2.35 times greater among in-person patients than those who receive telemedicine. Furthermore, there were less involuntary holds issued for the patients who received telemedicine, than patients who did not receive telemedicine (ratio of (aOR): 0.48; 95% CI 0.23 to 0.97).
Fairchild et al. [30] conducted a 2.5-year observational evaluation of telemental health programs in Indiana that provided assessment and diagnosis of psychiatric conditions by rural emergency room providers from September 2017 to April 2020. The study population included adults (n=532) and children (n=115) who presented to participating rural emergency rooms for psychiatric assessment and treatment. The telemental health intervention received by participants involved one-on-one patient and psychiatric specialist evaluation using live video telehealth in a private examination room. Primary outcomes of interest were characteristics of patients who received the telemental health intervention, the number of involuntary commitments issued versus non-involuntary commitments, disposition upon discharge, and length of stay. Secondary outcomes of interest included cost, primary payor of services, and payor reimbursement related to involuntary commitment status, major diagnostics group, and disposition. The study found that patients that were voluntarily admitted into the emergency department (86%, n=455) were categorized into the following groups based on presentation: (1) depression, anxiety, or other mental illness (35%), (2) substance abuse (33%), or (3) suicide risk (32%). Among those patients who voluntarily admitted to the ED, 47% were admitted to inpatient hospitalization, 47% referred to outpatient, and 6% admitted to critical access hospitals. Approximately 14% (n = 76/531) of the patients included in this study were involuntarily admitted to the emergency room and 67% of these patients found to need further involuntarily inpatient commitment. The patients who were admitted had longer lengths of stay in the emergency room than those who were referred to outpatient treatment. Mean total payor reimbursements for emergency department mental health care was significantly lower than actual emergency department costs.
Suicide Assessment Instruments
Several main findings emerged from this systematic review. First, studies identifying suicide assessment instruments used to evaluate suicidality by telehealth providers during the EOD process are extremely limited in number. Of the three articles included in this review, only one article referenced use of a suicide assessment instrument in the EOD process via telehealth. Godleski et al. [31] stated that the VA utilizes a standard decision tree and VA Suicide Assessment Cards to assess for suicidality in the EOD process via telehealth. However, the authors’ description of these two tools was vague. Thus, it is difficult to determine if the screening tools used by the VA are standardized, valid, or reliable in predicting suicide risk. Additionally, Godleski et al. [31] stated that clinicians at the VA use their clinician judgement to decide which patients will receive telehealth suicide assessment as opposed to being screened in-person. It was unclear if a standardized protocol is used in this process, or if clinician judgement is completely relied upon to make such a determination. The two other articles included in this review made no reference to the types of assessment instrument used. Vakkalanka et al. [29] referred to the assessment conducted by providers in the EOD process as “telemedicine evaluation” or “telemedicine consultation,” but did not specify what assessment instruments were used during these encounters with patients. Similarly, Fairchild et al. [30] did not name the type of instrument used and referred to the assessment as “telehealth visit.” The ambiguity of suicide assessment tools in these articles make it difficult to determine which specific suicide screening tools have been used by providers in the EOD process via telehealth.
Consistency or Discrepancy Between Telehealth and In-Person Assessments
None of the articles included in this systematic review incorporated a discussion about the types of assessment instruments used in-person versus those utilized by telehealth providers. Therefore, the authors of this articles are unable to determine if telehealth providers are using the same assessment instruments as providers conducting assessments in-person during the EOD process.
Rate of Hospitalization for Telehealth
One article did provide information about the number of EOD involuntary holds and hospital admissions rates among patients assessed via telehealth compared to patients assessed in-person. Vakkalanka et al. [29] found that hospital admissions were 2.35 times greater among patients who did not receive telemedicine than patients who did receive telemedicine at emergency departments. The authors also found less involuntary holds issued for the patients who received telemedicine, than patients who did not receive telemedicine. The other two articles included in this review did not include information about admission rates.
Discussion
Despite the rise in the use of telehealth to assess for suicidality, the findings of this systematic review suggest that the use of standardized suicide assessments during the EOD process has received little attention in research. Only one of the three articles included in this review referred to the types of suicide assessment tools used during the EOD process. Furthermore, although Godleski et al. [31] made mention of tools used by the VA, due to the vague description provided in the article, the authors of this review were unable to determine if the assessments used by the VA are reliable and valid suicide screening instruments. Reliable and valid standardized suicide assessments are critical in providing care for those experiencing suicidal thoughts and behaviors [33,34]. The EOD process is in place across the United States to protect individuals who are at risk for suicide and to provide them with necessary treatment aimed at preventing suicide [35]. Studies have suggested that mental health professionals do not feel adequately trained to assess for suicide and lack awareness of the tools that are available for the assessment of risk [36,37]. To ensure that professionals and facilities issuing EODs are effective at assessing risk via telehealth, further research on assessment practices and education efforts are needed to increase use of standardized assessment tools.
In addition to inadequate training, research has suggested that some practitioners avoid the use of standardized suicide assessments due to an overreliance and confidence in their clinical judgement and interviewing skills [38]. The findings of this study also suggest that clinicians rely heavily on clinical judgement during the EOD process via telehealth. Godleski et al. [31] stated that the VA relies on providers’ clinical judgement to identify patients who will receive suicide assessment via telehealth. The use of clinical judgment alone without the use of a research-supported tool could raise concerns about patients not being appropriately screened and treated for suicide risk. As there is variation in providers’ clinical judgement, this may be an area for further research to identify how providers determine which patients are appropriate for suicide assessment via telehealth in the EOD process versus patients who should be evaluated in-person. Clinical judgment can be influenced by many provider-specific factors as well. A study conducted by Berman et al. [39] found that gender, marital status, and religious affiliation were all predictors of suicide risk and that male providers were more likely to recommend hospitalization than female providers. Additional studies are needed that compare the use of standardized assessment tools via telehealth and the use of clinical judgement alone via telehealth in the EOD process to determine if one method of assessment is more effective than the other.
Godleski et al. [31] also listed several other variables in the telehealth EOD process that were not addressed by the authors of the other two articles, including licensing, local regulations on telehealth, and liability. More research is needed to determine how these variables impact the EOD process when delivered via telehealth. Hesitancy to utilize standardized assessment tools has the potential to place patients at increased risk and could delay necessary treatment when risk is not detected in a timely manner [40].
Additionally, the findings of this review suggest that further research is needed on the differences in hospital admission rates between patients assessed during the EOD process via telehealth compared to those assessed in person, as one study included in the review found a considerable difference between these two groups with patients who did not receive telemedicine assessment [29]. The type of assessment used may or may not account for this difference, especially if dissimilar types of assessment tools were used between the two groups. A recent study conducted by Fasshauer et al. [41] found a significant increase in involuntary psychiatric admissions during the first year of the COVID-19 pandemic (2020) as compared to involuntary admission rates during 2018 and 2019. Therefore, further studies are needed to determine if telehealth can reduce unnecessary hospitalizations and involuntary commitments for patients or if telehealth prevents patients from accessing inpatient care that they need.
A secondary finding of this review is that research appears to be limited in the types of medical and mental health providers conducting suicide assessments via telehealth. The articles focused on psychiatrists, registered nurses (RN), and MDs. The articles found by the authors of this review do not include a focus on other mental health professionals such as Licensed Social Workers, Licensed Mental Health Counselors, or psychiatric nurse practitioners who also deliver suicide assessment via telehealth [42,43]. Research is needed on the work of these providers, as the type of provider may or may not have an impact on the EOD evaluation process when delivered via telehealth.
Our review had one major limitation, which was that only three published articles were identified and included in this review. Two of the three articles were research studies that collected and analyzed data, while the third article was a narrative report of procedures based on best practice experience at the VA. A strength of the review is the rigorous search strategy utilized by the researchers, including the use of the PRISMA framework. Four researchers independently reviewed the article abstracts, the full text of the articles, compared the results, and arrived at consensus for inclusion.
In the absence of studies that identify the types of instruments being used by telehealth providers, it is difficult to determine which suicide assessment instruments are being used by telehealth providers during the EOD process. Lack of studies in this area raises major ethical implications for telehealth EOD practice, as lack of standardization raises concerns about accuracy of the assessment of suicidality. The emergency order of detention process can temporarily detain an individual against their will and therefore an accurate assessment is essential to preserve the dignity of patients, as well as accurately screen patients who present as a risk to themselves or others. Therefore, further research on the types of assessments being used by telehealth providers is needed to evaluate the effectiveness of these assessments and to ensure that valid and reliable tools are being utilized. Additionally, it is unknown if providers who conduct assessments in-person are using the same assessment tools as providers delivering services over telehealth. Further research is needed to identify the instruments being used by providers and to ensure continuity between in-person and telehealth assessments in the EOD process. There is also a need to develop a standardized measure to determine the reliability and validity of clinical decision making related to emergency orders of detention. Lack of continuity, reliability, and validity of assessment tools has the potential to lead to inaccurate assessment of patients, which could cost lives.
Competing interest:
The authors declare that they have no competing interests.
References
Center for Disease Control and Prevention (2021). Suicide and self-harm injury. https://www.cdc.gov/nchs/fastats/suicide.htm. View
National Institute of Mental Health (2021). Suicide. https:// www.nimh.nih.gov/health/statistics/suicide.View
American Foundation for the Prevention of Suicide (2020). Suicide statistics. https://afsp.org/suicide-statistics/.View
Silverman, M. M., & Berman, A. L. (2013). Suicide risk assessment and risk formulation part I: A focus on suicide ideation in assessment suicide risk. Suicide and Life-Threatening Behavior, 44(4), 420-431. https://doi.org/10.1111/sltb.12065.View
Knesper, D. J. (2011). Continuity of care for suicide prevention and research: Suicide attempts and suicide deaths subsequent to discharge from the emergency department or psychiatry inpatient unit. American Association of Suicidology, & Suicide Prevention Resource Center. https://www.sprc.org/sites/default/ files/migrate/library/continuityofcare.pdf. View
Stene-Larsen, K., & Reneflot, A. (2019). Contact with primary and mental health care prior to suicide: A systematic review of the literature from 2000 to 2017. Scandinavian Journal of Public Health, 47(1), 9–17. https://doi. org/10.1177/1403494817746274.View
Boldt, R. C. (2017). Emergency detention and involuntary hospitalization: assessing the front end of the civil commitment process. Drexel Law Review, 10(1), 1-67. View
Thomas, G. (2007). Limitations on parens patriae: The state and the parent/child relationship. Contemporary Legal Issues, 16(51).
Vernick, J. S, Gakh, M., & Rutkow, L. (2012). Emergency detention of persons with certain mental disorders during public health disasters: Legal and policy issues. American Journal of Disaster Medicine, 7(4), 295-302. https://doi. org/10.5055/ajdm.2012.0102. View
Testa, M., & West, S. G. (2010). Civil commitment in the United States. Psychiatry, 7(10), 30–40.View
Morris, N. P. (2020). Detention without data: Public tracking of civil commitment. Psychiatric Services, 71(7), 741-744. https:// doi.org/10.1176/appi.ps.202000212.View
Lee, G. & Cohen, D. (2020). Incidences of involuntary psychiatric detentions in 25 U.S. states. Psychiatric Services, 72(1), 61-68, https://doi.org/10.1176/appi.ps.201900477. View
Gajarawala, S. H. & Pelkowski, J. N. (2021). Telehealth benefits and barriers. The Journal for Nurse Practitioners,17(2), 218- 221. https://doi.org/10.1016/j.nurpra.2020.09.013.View
Demeke, H. B., Merali, S., Marks, S., Zilversmit Pao, L., Romero, L., Sandhu, P., Clark, H., Clara, A., McDow, K. B., Tindall, E., Campbell, S., Bolton, J., Le, X., Skapik, J. L., Nwaise, I., Rose, M. A., Strona, F. V., Nelson, C., & Siza, C. (2020). Trends in use of telehealth among health centers during the COVID-19 pandemic —United States, June 26–November 6, 2020. Morbidity and Mortality Weekly Report, 70, 240–244. View
Traube, D. E., Cederbaum,J.A.,Taylor, A.,Naish, L., & Rau, A.(2021). Telehealth training and provider experience of delivering behavioral health services. The journal of Behavioral Health services & Research, 48(1),93-102. https://doi. org/10.1007/s11414-020-09718-0View
Morales, D. A., Barksdale, C. L., & Beckel-Mitchener, A. C. (2020). A call to action to address rural mental health disparities. Journal of Clinical and Translational Science, 4(5), 463–467. https://doi.org/10.1017/cts.2020.42. View
Rhoads, S. & Rakes, A. L. (2020). Telehealth technology: Reducing barriers for rural residents seeking genetic counseling. Journal of the American Association of Nurse Practitioners, 32(3),190-192.https://doi.org/10.1097/ JXX.0000000000000373. View
Hughes, M. C., Gorman, J. M., Ren, Y., Khalid, S., & Clayton, C. (2019). Increasing access to rural mental health care using hybrid care that includes telepsychiatry. Journal of Rural Mental Health, 43(1), 30–37. https://doi.org/10.1037/ rmh0000110.View
Sorvaniemi, M., & Santamaki, O. (2002). Telepsychiatry in emergency consultations. Journal of Tele-medicine and Telecare, 8, 183–184. https://doi.org/10.1177/1357633X0200800309.View
Jong, M. (2004). Managing suicides via videoconferencing in a remote northern community in Canada. International Journal of Circumpolar Health, 63(4), 422-428, https://doi.org/10.3402/ ijch.v63i4.17759.View
Lu, M. W., Woodside, K. I., Chisholm, T. L., & Ward, M. F. (2014). Making connections: Suicide prevention and the use of technology with rural veterans. Journal of Rural Mental Health, 38(2), 98–108. https://doi.org/10.1037/rmh0000021. View
Myers, K., Nelson, E., Rabinowitz, T., Hilty, D., Baker, D., Barnwell, S. S., Boyce, G., Bufka, L. F., Cain, S., Chui, L., Comer, J. S., Cradock, C., Goldstein, F., Johnston, B., Krupinski, E., Lo, K., Luxton, D. D., McSwain, S. D., McWilliams, J., North, S., Ostrowski, J., Pignatiello, A., Roth, D., Shore, J., Turvey, C., Varrell, J. R., Wright, S., & Bernard, J. (2017). American Telemedicine Association practice guidelines for telemental health with children and adolescents. Telemedicine and e-Health, 23(10), 779-804. https://doi.org/10.1089/ tmj.2017.0177.View
Gilmore, A. K., & Ward-Ciesielski, E. F. (2019). Perceived risks and use of psychotherapy via telemedicine for patients at risk for suicide. Journal of Telemedicine and Telecare, 25(1), 59–63. https://doi.org/10.1177/1357633X17735559.View
Bolton, J. M., Gunnell, D., & Turecki, G. (2015). Suicide risk and intervention in people with mental illness. BMJ, https://doi. org/10.1136/bmj.h4978. View
Bolton, J. M. (2015). Suicide risk assessment in the emergency department: Out of the darkness. Depression and Anxiety, 32(2), 73-5. httpsL://doi.org/10.1002/da.22320. View
Beard, C., Hsu, K.J., Rifkin, L.S., Busch, A. B., & Björgvinsson, T. (2016). Validation of the PHQ-9 in a psychiatric sample. Journal of Affective Disorders, 193, 267-273, https://doi. org/10.1016/j.jad.2015.12.075.View
Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K.V., Oquendo, M.A., Currier, G.W., Melvin, G.A., Greenhill, L., Shen, S., & Mann, J. J. (2011) The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168(12),1266-77. https://doi. org/10.1176/appi.ajp.2011.10111704.View
Jobes, D. A., Comtois, K. A., Gutierrez, P. M., Brenner, L. A., Huh, D., Chalker, S. A., Ruhe, G., Kerbrat, A. H., Atkins, D. A., Jennings, K., Crumlish, J., Corona, C. D., O’ Connor, S., Hendricks, K. E., Schembari, B., Singer, B., & Crow, B. (2017) A randomized controlled trial of the Collaborative Assessment and Management of Suicidality versus enhanced care as usual with suicidal soldiers. Psychiatry, 80(4), 339-356. https://doi.or g/10.1080/00332747.2017.1354607. View
Vakkalanka, J. P., Harland, K. K., Wittrock, A., Schmidt, M., Mack, L., Nipe, M., Himadi, E., Ward, M. M., & Mohr, N. M. (2019). Telemedicine is associated with rapid transfer and fewer involuntary holds among patients presenting with suicidal ideation in rural hospitals: a propensity matched cohort study. Journal of Epidemiology and Community Health, 73(11), 1033– 1039. https://doi.org/10.1136/jech-2019-212623. View
Fairchild, R., Ferng-Kuo, S.-F., Rahmouni, H., & Hardesty, D. (2020). An observational study of telemental care delivery and the context for involuntary commitment for mental health patients in a group of rural emergency departments. Telemedicine Reports, 1(1), 22–35. https://doi.org/10.1089/tmr.2020.0005. View
Godleski, L., Nieves, J. E., Darkins, A., & Lehmann, L. (2008). VA telemental health: Suicide assessment. Behavioral Sciences & the Law, 26(3), 271–286. https://doi.org/10.1002/bsl.81.View
Rudd, M. D., Berman, A. L., Joiner, T. E., Jr., Nock, M. K., Silverman, M. M., Mandrusiak, M., VanOrden, K., & Witte, T. (2006). Warning signs for suicide: Theory, research, and clinical applications. Suicide and Life Threatening Behavior, 36(3), 255–262. https://doi.org/10.1521/suli.2006.36.3.255.View
Chu, C., Klein, K.M., Buchman-Schmitt, J.M., Hom, M.A., Hagan, C.R. & Joiner, T.E. (2015), Routinized assessment of suicide risk in clinical practice: An empirically informed update. Journal of Clinical Psychology, 71(1), 1186-1200. https://doi. org/10.1002/jclp.22210. View
Kene, P., Yee, E. T., & Gimmestad, K. D. (2019) Suicide assessment and treatment: Gaps between theory, research, and practice. Death Studies, 43(3), 164-172. https://doi.org/10.1080 /07481187.2018.1440034. View
Hedman, L. C., Petrila, J., Fisher, W. H., Swanson, J. W., Dingman, D. A., & Burris, S. (2016). State laws on emergency holds for mental health stabilization. Psychiatric Services, 67(5), 529-535. https://doi.org/10.1176/appi.ps.201500205. View
Osteen, P. J., Jacobson, J. M., & Sharpe, T. L. (2014). Suicide prevention in social work education: How prepared are social work students? Journal of Social Work Education, 50(2), 349– 364. doi:10.1080/10437797.2014.885272.View
Liebling-Boccio, D. E., & Jennings, H. R. (2013). Current status of graduate training in suicide risk assessment. Psychology in the Schools, 50(1), 72–86. doi:10.1002/pits.21661. View
Jobes, D.A., Nelson, K.N., Peterson, E.M., Pentiuc, D., Downing, V., Francini, K. and Kiernan, A. (2004), Describing suicidality: An investigation of qualitative SSF responses. Suicide and Life-Threatening Behavior, 34(1), 99-112. https:// doi.org/10.1521/suli.34.2.99.32788. View
Berman, N. C., Stark, A., Cooperman, A., Wilhelm, S. & Cohen, I. G. (2015) Effect of patient and therapist factors on suicide risk assessment. Death Studies, 39(7), 433-441, https://doi.org/10.1 080/07481187.2014.958630. View
Weber, A. N., Michail, M., Thompson, A., & Fiedorowicz, J. G. (2017). Psychiatric Emergencies: Assessing and Managing Suicidal Ideation. The Medical Clinics of North America, 101(3), 553–571. https://doi.org/10.1016/j.mcna.2016.12.006.View
Fasshauer, J. M., Bollmann, A., Hohenstein, S., Mouratis, K., Hindricks, G., Meier-Hellmann, A., Kuhlen, R., Broocks, A., Schomerus, G., & Stengler, K. (2021). Impact of COVID-19 pandemic on involuntary and urgent inpatient admissions for psychiatric disorders in a German-wide hospital network. Journal of Psychiatric Research, 142, 140–143. https://doi. org/10.1016/j.jpsychires.2021.07.052. View
Hilty, D.M., Maheu, M.M., Drude, K.P., Hertlein, K., Wall, K., Long, R. P., & Luoma, T. L. (2017). Telebehavioral health, telemental health, e-therapy and e-health competencies: The need for an interprofessional framework. Journal of Technology in Behavioral Science, 2, 171–189. https://doi.org/10.1007/ s41347-017-0036-0. View
Rutledge, C. M., Kott, K., Schweickert, P. A., Poston, R., Fowler, C., & Haney, T. S. (2017). Telehealth and eHealth in nurse practitioner training: current perspectives. Advances in Medical Education and Practice, 8, 399–409. https://doi. org/10.2147/AMEP.S116071.View