
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 5 (2023), Article ID: JMHSB-179
https://doi.org/10.33790/jmhsb1100179Research Article
Suicide and Violence against Women in Azerbaijan: Risk Factors and Barriers for Seeking Mental Healthcare
Dana Alonzo1*, Pinar Zubaroglu – Ioannides2
1* Graduate School of Social Service, Fordham University, New York, USA.
2 Department of Social Work, Suleyman Demirel University, Isparta, Turkey.
Corresponding Author Details: Dana Alonzo, Ph.D., Graduate School of Social Service, Fordham University, 400 Westchester Ave, West Harrison, NY 10604, USA.
Received date: 02nd February, 2022
Accepted date: 02nd March, 2023
Published date: 06th March, 2023
Citation: Alonzo, D. & Zubaroglu-loannides, P. (2023). Suicide and Violence against Women in Azerbaijan: Risk Factors and Barriers for Seeking Mental Healthcare. J Ment Health Soc Behav 5(1):179.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Azerbaijan is ranked among the 3 countries with the highest rates of suicide in the Muslim world, and rates are increasing. Violence against women is an equally alarming public health issue in Azerbaijan. A scarcity of data has limited accurate identification of risk factors for suicide and violence against women and barriers to help-seeking. This study aims to address this gap.
Method: Thirty (30) in-depth qualitative interviews with women in the community and 4 semi-structured focus groups with key informant groups (mental health providers (psychologists, social workers, psychiatrists), teachers, and survivors of suicide) were held to examine perspectives regarding suicide and violence against women in Azerbaijan. A mixed method was employed using quantitative analysis and thematic content analysis. Thirty (30) of interviews were conducted and 4 of focus groups were held (see table 1).
Results: Employed participants were more likely to consider suicide a problem compared to unemployed participants (p=.05); unemployed participants were more likely to view treatment as acceptable compared to employed participants (p=.05). Additionally, older participants were more likely to view both suicide (p=.03) and violence against women (p=.026) as significant problems facing the country. The majority of participants viewed suicide (83%) and violence against women (73%) as problems in Azerbaijan. Nevertheless, 33% reported negative stereotypes regarding suicide and mental healthcare and 50% reported psychological treatment as unaccepted in Azerbaijan.
Conclusion: Suicide and violence against women are recognized problems for women in Azerbaijan. Stigma against mental illness is high and the mental healthcare system remains disproportionately institutionalized and under-funded. This highlights the need for building mental health workforce capacity and promoting advocacy efforts addressing policies regarding the allocation of funding for mental healthcare. Key recommendations for such programming are presented.
Introduction
Suicide is a global phenomenon that affect all regions of the world, with some 800,000 individuals dying by suicide annually. Yet, research indicates this is an underestimate due to stigma related to reporting suicide and suicidal behavior and given that many Muslim-majority countries, where populations exceed 100 million, do not report data in this area [1].
Based on the limited research that is available, Azerbaijan is ranked among the 3 countries with the highest rates of suicide in the Muslim world [2]. Data further demonstrate that the rates of suicide have increased in Azerbaijan over the last decade, particularly among women and youth [3]. Among individuals who die by suicide in Azerbaijan, research notes the most prominent methods of suicide are hanging, self-immolation, and overdose poisonings, in general, and self-immolation among females, in particular [3,4].
Violence against women is an equally alarming public health issue in Azerbaijan. Violence against women takes different forms, with the most extreme being femicide. Data indicates multiple forms of femicide exist with the most frequent including: 1) Killing of women by their partners; 2) “Honor Killings”, when the relatives of a woman consider her behavior shameful for the family and compromising their reputation and decency and kill her to restore honor to the family; and, 3) Deliberate elimination of women during armed conflicts; this type of killings is often is considered as a weapon of war and is often accompanied by mass rapes, aimed at humiliation of the adversary.
Given the critical lack of research to date focused on suicide and violence against women in Muslim countries, in general, and in Azerbaijan in particular, it remains unclear what the relevant risk factors for suicide and violence against women are and whether existing services for mental healthcare are being readily identified and accessed by at-risk women. This gap in knowledge significantly limits efforts aimed at prevention and intervention development. This study aims to address this gap and to increase our understanding of suicide risk in this region of the world by examining: 1) the culturally relevant risk factors related to suicide and violence against women, and 2) the factors serving as barriers to mental health treatment utilization.
Methods
Sample
With approval from the appropriate Institutional Review Board and in collaboration with a well-known and trusted local non-for-profit organization working to promote women’s rights in Baku, Azerbaijan, a total of 61 women from urban and suburban communities, teachers working with at-risk youth, and mental health providers participated in the study. Participants were provided with information on the nature of the study and verbal informed consent was secured by the local study interviewers in accordance with their standard procedures and the parameters of the IRB approval secured by the study Principal Investigator.
Thirty (30) in-depth qualitative interviews with women in the general community were conducted and 4 focus groups (n=31) were held with women with lived experience of suicide attempt, mental health providers, and teachers working with at-risk youth. Data collection was carried out over a 1-month period during December 2021. On average, interviews lasted approximately 45 minutes and focus groups lasted approximately 95 minutes.
Measures
The study PI designed the semi-structured interview guide for both the focus groups and the one-on-one interviews and provided support to in-country staff overseeing the data collection. Questions covered three key categories regarding risk factors and help-seeking including: 1) Perspectives on Suicide and Violence against Women (to elicit the respondent’s views regarding the nature and extent of the problems of suicide and violence against women in their community); 2) Perspectives on Help-Seeking (to elicit the respondent’s views on the stigma related to mental health and barriers to and facilitators for outreach in their community); and, 3) Perspectives on Existing Resources (to elicit the respondent’s view of the nature and quality of existing resources for mental healthcare in their community).
Questions regarding perspectives on suicide and violence against women included, 1) Do you believe suicide is recognized as a problem in your country? What about within your community?; 2) Who do you think is at the greatest risk of suicide? Why?; 3) Is suicide preventable? Please explain.; 4) What do you think causes suicide?; 5) Is violence against and the killing of women and girls a problem in your country? Community?; 6) What are the consequences of violence against women and girls?; 7) Do you think there is a connection between violence against and violence against women and emotional distress or psychological problems among women?; 8) Do you think there is a connection between violence against women and suicide risk? 9) Is partner/family violence an issue one should seek help for? Why or why not?
Questions regarding perspectives on help-seeking for psychological distress included, 1) How is mental health treatment viewed in your community?; 2) Is mental health treatment accepted in the community? 3) What are the main barriers to seeking help for psychological and emotional problems in your community?; 4) What would make help-seeking more likely?;
Questions regarding perspectives on existing resources for mental health support included, 1) Do you think there are enough resources in the community for people in need of mental health treatment? 2) Do you think people know what resources exist?; 3)What resources are available that you know of?; 4) How did you learn of these resources?; 5) Do you know how to find such resources if you were to need them?; and, 6) What should be done to make these resources more known to people who may need them?
Questions regarding perspectives on help-seeking included, 1) 2) What are the main barriers to seeking help for psychological and emotional problems in your community?; and 3) What would make help-seeking more likely?
In addition to the noted in the 4 core areas above, suicide attempt survivors were asked to share their experiences related to their attempt including, 1) Did you seek mental health treatment before you attempted suicide? If yes, what is your opinion of the care you received? What was one thing that was most helpful? Least helpful? If no, what prevented you from receiving care in your opinion?; 2) How would you describe the reaction of your family/extended family to your suicide attempt?; 3) How would you describe the reaction of your friends to your suicide attempt?; 4) If you were to experience a problem in the future, would you seek help? Why or why not?
In addition to the questions in the 4 core areas noted above, mental health professionals were also asked to comment on the nature of their training regarding engaging with individuals at risk of suicide. These questions included, 1) Did you receive specific training focused on suicide assessment and intervention when in your mental health training program?; 2) If Yes, how much training did you receive? (Approximate hours)? Was that amount of training sufficient to equip you with the knowledge and skills you feel you need to effectively treat individuals at risk of suicide?; 3) If no, do you feel you have the skills and knowledge you need to effectively treat individuals at-risk of suicide?; 4) What do you think contributes to the lack of educational content focused on suicide in training programs? 5) What are the main barriers to engaging at-risk individuals in treatment?; 6) What are the main facilitators of treatment engagement with at-risk individuals?; and, 7) What additional training do you feel would help you in this work?
Qualitative One-on-One Interview Questions
For the one-on-one in-depth interviews, women in the general community residing in urban and suburban areas were asked 11 questions regarding their perspectives on suicide and femicide including, 1) Is suicide a problem in your country? What about within your community?; 2) Have you had any personal experience with suicide- either your own suicidal thoughts/behaviors or a relatives or friend? Please describe; 3) What comes to mind when you think of suicide or a suicidal person?; 4) Who do you think is at the greatest risk of suicide? Why?; 5) What do you think causes suicide?; 6) Is femicide a problem in your country? Community?; 7) What do you think causes violence within families/relationships?; 8) Does interpersonal violence contribute to emotional distress or psychological problems among females?; 9) Does interpersonal violence contribute to suicide risk?; 10) What could prevent suicide?; and, 11) What could prevent femicide?
The interview survey also included 9 questions pertaining to the women’s perspectives on help-seeking including, 1) What comes to mind when you think of mental illness?; 2) What comes to mind when you think of psychological or psychiatric treatment?; 3) Is mental health treatment accepted in the community?; 4 What are the barriers to seeking help of psychological and emotional problems?; 5) What would make help-seeking more likely? 6) Who do you usually turn to for help/support when you are feeling stressed or overwhelmed? 7) What is one thing that you have found helpful when asking for help?; 8) Have you ever experienced a problem that mental health treatment could have helped you with? If yes, did you seek help for that problem? Why or why not? If no, if you were to have such a problem in the future, would you seek help? Why or why not?; and, 9) What would have to happen for you to seek professional help?
Lastly, women were asked 3 main questions regarding their perspectives on existing resources including, 1) Do you think there are enough resources in the community for people in need of mental health treatment?; 2) What resources are available that you know of?; and, 3) you know how to find such resources if you were to need them?
Data Analysis
A mixed methods approach was utilized. Quantitative analyses were performed using IBM SPSS Statistics for Windows, version 27 (IBM Corp., USA). Descriptive statistics were computed for the sociodemographic characteristics of the sample and the study variables consisting of frequencies and percentages for categorical variables and means and standard deviations (SDs) for scale variables using t-tests and chi-square as appropriate.
Conventional content analysis was used to analyze the qualitative data, a widely accepted methodology that allows for the description of qualitative data through a systematic process of coding and classification, [5]. Responses to the open-ended questions from the culturally-responsive, evidence-informed interview guides designed for this project were reviewed to identify recurring themes. Initial coding was conducted independently after which team meetings were held to review the categories and idiosyncratic and/or redundant responses were removed. In the case of discrepancies, definitions of the categories were clarified and rating was repeated until inter-rater consistency of at least 80% for these items was reached, per standards in the literature [6]. This inductive process allows for identification of the overarching views regarding the extent of suicide and violence against women as problems facing women in the community as well as barriers to and facilitators of help-seeking for women in need of mental health support from the perspectives of community members, individuals with lived experience, teachers, and mental health providers.
Quantitative Analysis
Table 1 reports on the characteristics of the participants from the one-on-one interviews with female community member. Overall, the sample of women was largely single (53%), without children (53%), employed (60%), and, with high educational achievement (73%).
There were few significant differences found in the bivariate for any of the themes raised by participants based on the sociodemographic characteristics of the sample (i.e., the level of education, employment status, or marital status, parental status) (see table 2). Those participants who were employed were more likely to consider suicide a significant problem as compared to those who are unemployed (p=.05); reflecting, perhaps, the fact that those who are more at risk of suicide (such as those who are unemployed and experiencing financial hardship) are less likely to disclose thoughts about suicide. Additionally, those participants who were unemployed were more likely to view treatment as acceptable as compared to those who were employed (p=.05).

Table 1. Sociodemographic Characteristics of Key Informant Interview Participants
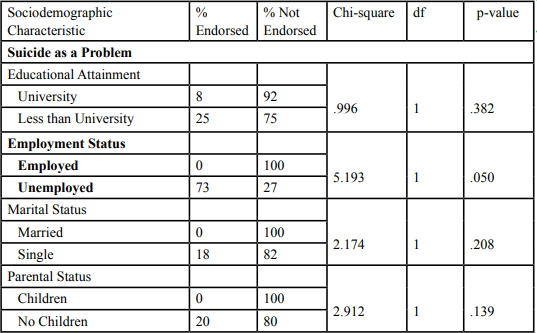
Table 2. Bivariate Analyses of Women’s Perspectives on Suicide, Violence, and Treatment by Education, Employment Status, Marital Status, and Parental Status
Although there were no significant differences by age for the treatment related variables, significant differences were found by age in regard to perspectives on suicide and violence against women (see table 3). More specifically, older participants were more likely to view both suicide (p=.03) and violence against women (p=.026) as significant problems facing the country.

Table 3. Bivariate Analyses of Women’s Perspectives on Suicide, Violence, and Treatment by Age
Qualitative Analysis
I-Perspectives on Suicide and Violence against Women
Participants largely endorsed suicide as a significant problem in Azerbaijan (83%). Most participants reported a belief that adolescents are most at risk for suicide (30%). Representative comments from participants include:
• “It is mostly in women (at risk) I would say especially in teenage girls. The reason for this is that in our society, the approach to teenage girls and the way they are raised are wrong. Teenage girls are usually more afraid of their families. Because the family or environment in which she grew up raises hers in such a way that if she makes a mistake, her family will break up... This is usually a direct negative effect on human psychology.”- Survivor of Attempted Suicide
• “It is mostly happening when there is conflicts in the family, in failed families”- Psychologist
• “A woman who has been abused needs psychological help. And many women are suicidal because they cannot use this service.”- Suicide Attempt Survivor
• “Violence against women encourages suicide. The abused woman feels guilty. Because her parents instilled it in her from an early age. Maybe someone instilled those parents. If we teach girls that violence from an early age is not their fault, the result may be quite different.”- Suicide Attempt Survivor
Further, 73% of respondents reported that violence against women was a significant problem in Azerbaijan. The majority of respondents (83%) reported that violence against women contributes to psychological distress and 83% of the sample reported that violence against women is a trigger for suicide. Representative comments of participants include:
• “there are many reasons for suicide. Mental stress, disorder, domestical difficulties, judgment in the society.”- Psychologist
• “the vast majority of women in our country teach their daughters to be afraid, not courageous...our society (creates) women and mothers who can not even claim their rights.- Survivor of Attempted Suicide
• “I was under the care of my uncle from an early age. He and his wife beat me many times. Then I ran away from home. I could not stand it. A boy was working at the place where the car was being repaired. I ran with him. But after a while he started beating me... I came to Baku. With a baby in my arms. The child was very hungry...I was ashamed to ask anyone for anything... In the end, I said I would kill myself. I went to the beach...Leaving the child nearby, I started running towards the sea. At that moment, a police officer stopped me. He saw me in advance and knew that I would kill myself. Then other police officers came. I was told not to do it again. I was told that we would help you. They brought my child to me... Now I am grateful to that police. I didn't really want to die...I thought it would save my child's life. There will be no hunger under the auspices of the state. I could not find another way. I was alone”- Attempt Survivor
II- Perspectives on Help-Seeking
Despite acknowledging the extent of these issues and the psychological distress experienced by women, 33% of the sample reported negative stereotypes associated with suicide, mental illness and psychological treatment.
• “If they knew the prohibitions of our religion, they would not attempt suicide or murder.”-Psychologist
• “Suicide is also a sin in our religion. It is important to instill this in children in the family from childhood.”- Psychologist
• “If there is an elder in the family, the problem can be solved.”- Psychologist
• “It should be noted that life is given to man once, and this life is a trust. He must protect this deposit until the last moment of his life. In addition to being a religious sin, it is also a legal crime. It is necessary to instill this in children so that they understand.”- Psychologist
Additionally, 50% of respondents reported that mental healthcare was not accepted in the country. Further, 48% of participants reported a belief that personal and public stigma were significant barriers to help-seeking.
• “Confidence in the science of psychology has just been strengthened in our country. This was not the case before. Even now, there are people who see psychological services as a shame. I think that extensive trainings should be held on these topics.”- Suicide Attempt Survivor
• “Mental health treatment is not always accepted in society. Sometimes even the person receiving mental health assistance cannot accept it, and the result is not the desired.”- Suicide Attempt Survivor
The main triggers for suicide identified by participants were largely at the micro and mezzo level and include: 1) domestic violence (37%); 2) psychological distress (28%); 3) familial conflict (30%); and, 4) weakness/insecurity (23%).
• “When the child fails, the parent pressures and reprimands him. Sometimes he is forced to commit suicide. No matter how much the parent regrets, it is too late.”- Teacher
• “Prohibitions, violence and betrayal in the family lead to suicide.”- Teacher
• “Family restrictions and betrayal lead to suicide.”- Psychologist
• “Women are often not allowed to leave the house, locked in houses, or even go to their parents. The result is often suicide”- Psychologist
The main contributors for violence against women identified by participants spanned micro, mezzo, and macro levels and include: 1) cultural values regarding gender roles and moral (38%); 2) lack of communication and understanding (38%); 3) jealousy (17%); and, 4) socioeconomic stressors (i.e., poverty, unemployment) (17%).
• “I see the reason in a society that is not properly educated. For example, if a woman betrays her husband, she is called an immoral person, and the punishment is often death. When a man cheats, it is normal for everyone and the woman is pressured to close the case. It is this discrimination that ultimately leads to such crimes” Suicide Attempt Survivor
• “Early marriages in girls, lack of education, unemployment, girls are exposed to violence, they are afraid, they cannot solve the problem and cannot tell anyone.”- Teacher
• “In our religion, it is forbidden to humiliate a woman. However, men implement prohibitions for women, lock the door when they go to work, they do not allow women to meet with anyone, not even with her family in which she was raised, torture, beat and sometimes kill.”- Teacher
• “Murder and violence occur most often as a result of betrayal and jealousy.”- Psychologist
• “If there is a danger, the family, friends, society, the whole sphere around it is to blame. There was indifference, lack of communication, inattention that the man touched her.”- Psychologist
III- Perspectives on Existing Resources
Regarding treatment utilization, the majority of participants noted a significant lack in existing resources in the community to support women at-risk of suicide or experiencing violence and in training on these issues for providers of treatment (72%). Yet, 37% reported not knowing what services exist at present in their community and 33% reported being unaware of how to find out about what services are available in their community for mental healthcare. Participants further noted that access to care could be improved if psychological support was made more available (62%), families were more supportive of care (21%), and individuals were educated about resources and the benefits of treatment (17%).
• “There are almost no psychiatrists.”- Teacher
• “We have not received training on this topic in training programs. It would be very good to have such training. We do not have knowledge and skills in this area.”- Teacher
• “I think there are enough resources in society for people in need of mental health treatment. It's just that not many people know how to use these resources. It is unknown. It is not right to blame people here either. Because although there are enough resources, their promotion is very weak.”- Suicide Attempt Survivor
• “(Programs) should be advertised to reach everyone, and live meetings and trainings should be held “- Suicide Attempt Survivor
• “(Lack of training) due to the indifferent attitude to the field. Lack of knowledge on these topics in current training materials.”- Psychologist
Discussion
This is the first study of women with lived experience of suicide attempt and violence, and mental health providers serving this vulnerable population that examines their perspectives of risk factors for suicide and violence against women, and barriers to help-seeking for mental healthcare in the Muslim majority country of Azerbaijan. Data on these issues in this region of the world is sorely lacking and has hindered accurate estimation of risk as well as efforts to identify and provide support to at-risk women. This study begins to fill that gap and provides insight into the culturally relevant attitudes and beliefs regarding suicide, violence against women, and mental illness to inform the development of prevention and intervention programming, responsive to the unique cultural needs, values, and beliefs of the population.
Findings of this study indicate that both attempt survivors and mental health professionals strongly identified violence against women as a significant risk factor for suicide among women. The association between intimate partner violence and non-partner physical violence, and poor mental health of women, including increased risk of suicide, have been demonstrated in numerous international and national studies [7-10]. In fact, one of the most consistent risk factors for suicide attempts after controlling for common mental health disorders is intimate partner violence followed by non-partner physical violence [7,8,10,11]. Overall, this body of research indicates that there is a clear and direct correlation between experiences of violence and suicide risk. A positive correlation has repeatedly been found in research between domestic violence and suicide risk such that that as a women’s exposure to domestic violence increases, their suicide risk also increases. Further, research indicates that showed that women who have experienced physical or sexual violence, or both, are as much as seven times more likely to have suicidal ideation and approximately four times more likely to have attempted suicide on one or more occasions to have ended their lives [12,13]. This study extends this relationship to Muslim majority countries.
Findings also indicate that stigma is a major barrier against help-seeking for mental healthcare in Azerbaijan. Research has found that in setting where mental illness is highly stigmatized, individuals with mental illness often internalize these negative beliefs and come to accept the discrediting prejudices held against them. As a result, they lose self-esteem, experience feelings of shame and alienation, and socially withdrawal, increasing risk of suicide ideation and behavior (Figueroa, 2014; Ritsher et al., 2003; Ritsher & Phelan, 2004). This process of internalized stigma leads individuals struggling with mental illness and at risk of suicide to expect to be treated in a discriminatory way (‘anticipated discrimination’) and try to hide their suicidal thoughts and feelings illness, rather than to seek sources of treatment [14-16].
Mental health stigma is not relegated to those in the general population. Research focused on other cultures that share an equally stigmatizing view of mental illness demonstrates significant rates of stigma against individuals with mental illness perpetuated by practicing both practicing mental health providers and graduate students in mental health training programs (Mascayano et al., 2016; Thornicroft, 2006). Mental health providers in such contexts often endorsed negative attitudes and social distance toward people with severe mental illness and have also been found to view individuals with severe mental illness as aggressive and to endorse pessimistic predictions about their recovery [17,18]. This points to the importance of addressing the stigmatizing, biased attitudes held by helping professionals against individuals with severe symptomatology, such as suicidal ideation, in order to improve the quality of care they provide.
This study found that existing resources for mental healthcare are largely unidentified, under-recognized and not readily accessible by women at risk of suicide and/or experiencing violence. Overall, mental healthcare services in Azerbaijan are limited [19,20]. The first formal mental healthcare institution was established in Baku in 1892 with a total 30 beds. This institution doubled its capacity to a total of 60 beds in the early twentieth century due to the need for increased mental healthcare services related to the intensive growth of the population of the capital. Additionally, a second psychiatric hospital was founded at that time also with a 60-bed capacity. Following the establishment of Soviet governance in Azerbaijan in the mid-1920s, the structure of psychiatric care in the country was reorganized towards creating a psycho-neurological institute along with a colony for 150 mentally ill. In 1960s, the mental healthcare system was again restructured towards outpatient care. In 1990s, there was an overall decline in the provision of traditional mental healthcare services [21].
At present, Azerbaijan is experiencing yet another large-scale reform of the mental healthcare system [19]. This effort is aimed at improving the protection of the human rights of those with psychiatric illnesses, creating updated community-based services, building human resources capacity, and increasing participation in international psychiatric research [19,22].
The outcome of these efforts has yet to be realized, however. The mental healthcare system remains disproportionately institutionalized and under-funded. The range of services provided are limited for persons with serious mental illness with the greatest treatment needs, such as those experiencing suicidal thoughts and behaviors, and those experiencing violence. Notably, person-centered service outcome indicators such as assessment of needs, quality of life, and satisfaction with care are not currently used to inform the allocation of mental health resources [22]. This points to the need for building mental health workforce capacity; providing existing mental healthcare providers specialized training to improve their attitudes towards at-risk individuals and improve their knowledge and increase their skill at working with women who have suicidal thoughts and behaviors and those who are experiencing violence; and, promoting advocacy efforts to address policies regarding the allocation of funding for mental healthcare and appropriate measures for evaluating services.
According to the Commission on Social Determinants of Health (CSDH) of the World Health Organization [1], health inequalities and inequities result from the contexts within which people grow, live, work, and age, and the systems that exist to deal with illness. Further, the social determinants of behavioral health impact not only quality-of-life outcomes, such as socioeconomic status, educational attainment, access to healthy and affordable food choices, employment and job stability, housing status, exposure to toxic environments, but also access to quality health and behavioral health services [1]. The Social Determinants of Health framework can contribute to a better understanding of health inequalities within and across populations and support to the design of clinical interventions and public health policies. Socially predetermined forces contribute to create the contexts that essentially determine who will live and what their quality of life may be. Although conceptualizations of mental illness and suicide vary by setting, culture, socioeconomic and political influence and historical context, the social determinants of health related to risk of suicide and violence are modifiable and can serve as a point of intervention for reducing suicide and for violence prevention. This study indicates key social determinants of health related to suicide that require attention, namely, violence, family disintegration and conflict, stigma around mental illness, limited access to care, and gender norms regarding the role of women.
Clearly, prevention efforts are needed that address the intersectionality between violence and suicide among Azerbaijani women across micro, mezzo, and macro factors. Recommendations to shape such efforts include:
1. Developing culturally adapted trainings for key constituent groups on suicide assessment and intervention, including, Mental Health providers (psychiatrists, psychologists, social workers), Lay professionals in the community (primary care doctors, pediatricians), and, School personnel (teachers, school nurses, guidance counselors);
2. Implementing a public health campaign using social media to promote mental health awareness and reduce stigma, provide strategies for self-care, provide strategies for violence de-escalation, increase knowledge of available resources, and empower women’s voices to address cultural biases;
3. Building a safe and accessible early warning network system for women to communicate safety concerns;
4. Creating and promoting guidelines for the safe use of technology to reduce risk of suicide related to social media use;
5. Implementing a targeted texting campaign promoting message of safety and notifying women of where help can be received
6. Developing a system for on-going peer case consultation for mental health providers working with at-risk women
7. Collaborating with key constituents at the State level who can influence policy change regarding allocation of resources for mental healthcare
8. Identify existing safe spaces in the community that can be made accessible to women to express safety concerns and receive information and resources
9. Building relationships with local universities providing educational programming in psychology and psychiatry and develop curriculum regarding suicide assessment and treatment and violence prevention that can be integrated into their program to prepare the next generation of mental health providers to be trained with the knowledge and skills they need to work effectively with at-risk women
10. Creating digital narratives of women with lived experience of suicidal ideation and behavior violence who can present their experiences to key constituent groups for advocacy, awareness raising, training, and education purposes
11. Exploring community police programming within local communities to promote appropriate care for at-risk women and women experiencing violence.
12. Developing peer programming for youth that can support risk identification and promote mental health awareness
13. Collaborating with community-based programs to explore, create and support opportunities for youth leadership programs and female employment to empower youth and women and promote opportunities to increase self-efficacy and self-esteem
14. Identifying key stakeholders at the judicial level who can collaborate to promote justice and human rights for women who disclose safety concerns
15. Developing a system for on-going evaluation of the effectiveness of developed programming for suicide and violence prevention and intervention to identify potential gaps and on-going needs
Conclusions
This study reflects an overarching view of the challenges facing women in Azerbaijan related to suicide and violence against women and the barriers to and facilitators of mental healthcare help-seeking, from the perspective of not only those who serve this population, but of women with lived experiences, themselves. Key results from the needs assessment highlight that domestic violence is the strongly identified as risk factor for suicide among women in Azerbaijan. Stigma and related cultural values regarding gender norms are significant contributors to violence against women and suicide. Individuals and families lack understanding of the nature of suicide and mental illness and the impact of violence on women’s well-being. Existing services are underrecognized and perceived of as unavailable or insufficient.
Accordingly, employing a social determinants of health lens and an ecosystems framework, multi-level programming is needed that spans micro (individual level supports), mezzo (family level supports), and macro (advocacy and outreach) levels to support a comprehensive strategy that beings with prevention and extends to address intervention, management, and capacity building to halt the increasing rates of suicide and deter violence against women.
References
World Health Organization. (2018). Suicide. Available from http://www.who.int/mediacentre/factsheets/fs398/en/View
Eskin, M., AlBuhairan, F., Rezaeian, M., Abdel-Khalek, A. M., Harlak, H., El-Nayal, M., ... & Khatib, S. (2019). Suicidal thoughts, attempts and motives among university students in 12 Muslim-majority countries. Psychiatric quarterly, 90(1), 229- 248.View
Aghazadeh, J., Motlagh, M. E., EntezarMahdi, R., Eslami, M., Moheb- bi, I., Yousefzadeh, H., & Farrokh-Eslamlou, H. (2017). Cause-spe- cific mortality among women of reproductive age: Results from a population-based study in an Iranian community. Sexual & Re- productive Healthcare, 14, 7–12. https://doi. org/10.1016/j.srhc. 2017.08.003 View
Kanchan, T., Menon, A., & Menezes, R. G. (2009). Methods of choice in completed suicides: gender differences and review of literature. Journal of Forensic Sciences, 54(4), 938–942.View
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative health research, 15(9), 1277-1288. View
Shek, D. T., Tang, V. M., & Han, X. Y. (2005). Evaluation of evaluation studies using qualitative research methods in social work literature (1990-2003): Evidence that constitutes a wake-up call. Research on Social Work Practice, 15(3), 180-194. View
Devries, K., Watts, C., Yoshihama, M., Kiss, L., Schraiber, L. B., Deyessa, N., ... & WHO Multi-Country Study Team. (2011). Violence against women is strongly associated with suicide attempts: evidence from the WHO multi-country study on women’s health and domestic violence against women. Social science & medicine, 73(1), 79-86.View
Kavak, F., Aktürk, Ü., Özdemir, A., & Gültekin, A. (2018). The relationship between domestic violence against women and suicide risk. Archives of psychiatric nursing, 32(4), 574-579.View
Romito, P., Turan, J. M., & De Marchi, M. (2005). The impact of current and past interpersonal violence on women's mental health. Social science & medicine, 60(8), 1717-1727.View
World Health Organization. (2014). Violence against women: Intimate partner and sexual violence against women: Intimate partner and sexual violence have serious short-and long-term physical, mental and sexual and reproductive health problems for survivors: Fact sheet (No. WHO/RHR/14.11). World Health Organization.View
Devries, K. M., & Seguin, M. (2013). Violence against women and suicidality: does violence cause suicidal behaviour?. In Violence against women and mental health (Vol. 178, pp. 148- 158).View
Afifi, T. O., MacMillan, H., Cox, B. J., Asmundson, G. J. G., Stein, M. B., & Sareen, J.(2009). Mental health correlates of intimate partner violence in marital relationships in a nationally representative sample of males and females. Journal of Interpersonal Violence, 24, 1398–1417.View
Cavanaugh, C. E., Messing, J. T., Del Colle, M., O’Sullivan, C., & Campbell, J. C. (2011). Prevalence and correlates of suicidal behavior among adult female victims of intimate partner violence. Suicide and Life Threatening Behavior, 41(4), 372- 383.View
Figueroa, C. (2014). State of Terror, States of Mind: Ladinas, Mental Health and Systems of Care, in Guatemala City. Retrieved from the University of Minnesota Digital Conservancy, https:// hdl.handle.net/11299/185181.View
Ritsher, J. B., Otilingam, P. G., & Grajales, M. (2003). Internalized stigma of mental illness: psychometric properties of a new measure. Psychiatry research, 121(1), 31-49. View
Ritsher, J. B., & Phelan, J. C. (2004). Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Research, 129(3), 257-265. View
Mascayano, F., Tapia, T., Schilling, S., Alvarado, R., Tapia, E., Lips, W., & Yang, L. H. (2016). Stigma toward mental illness in Latin America and the Caribbean: a systematic review. Brazilian Journal of Psychiatry, 38(1), 73-85.View
Thornicroft, G. (2006). Tackling discrimination against people with mental illness. Mental Health Foundation, London.View
Ismayilov, F. N. (2022). Community-Based Mental Health Services in Azerbaijan: a Course Toward Development. Consortium Psychiatricum, 3(1), 106-112.View
Rasulov, A., Ismayilov, F., Ahmedova, G., Ismayilova, J., Sultanova, A., Velimammadova, G. (2019). Needs assessment in care provision for in-patients with severe mental disorders. Modern Achievements of Azerbaijan Medicine, 14(1), 51–57.
Ismayilova, J., Xavier, M., & Munir, K. M. (2019). Needs Assessment Framework for Mental Health Policy in Treating Persons With Serious Mental Illness in Azerbaijan. Psychiatric Services, 70(5), 432-435.View
Rasulov, A. R. (2017). Development of mental health system in Azerbaijan. Kazan medical journal, 98(4), 656-661.View