
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 5 (2023), Article ID: JMHSB-183
https://doi.org/10.33790/jmhsb1100183Research Article
A Renewed Commitment to Life: A Grounded Theory Study of Suicide Attempts in Badakhshan, Tajikistan
Shahnaz Savani, PhD
Assistant Professor, Department of Social Work, University of Houston-Downtown, United States.
Corresponding Author Details: Shahnaz Savani, PhD, Assistant Professor, Department of Social Work, University of Hous ton-Downtown, United States.
Received date: 06th October, 2023
Accepted date: 14th November, 2023
Published date: 16th November, 2023
Citation: Savani, S. (2023). A Renewed Commitment to Life: A Grounded Theory Study of Suicide Attempts in Badakhshan, Tajikistan. J Ment Health Soc Behav 5(2):183.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Suicide is a serious and complex problem. The majority of suicides occur in low and middle-income countries. Also, suicide presents differently in different parts of the world and needs to be studied in its socio-cultural-religious context. Research on suicide in Central Asian countries, which are majority Muslim countries is limited. This study focuses on lived experiences of suicide in Badakhshan, Tajikistan; a remote Muslim province in Central Asia using the constructivist grounded theory methodology. This study also attempts to identify factors associated with suicide in this region. Twelve participants who identified as Muslim and made a suicide attempt were interviewed face-to-face in Tajikistan. Data from the interviews, including field notes, were analyzed using the constructivist grounded theory method to form a mid-range theory on the experience of suicide in Badakhshan. Findings include the development of a mid-range theory of suicide attempts in Badakhshan, Tajikistan and include the core categories of experiencing extreme hardship, seeking or not seeking help and the factors associated with suicide in the province. Findings that shed light on the lived experiences of suicide in this province its social, cultural, religious and political context.
Keywords: Suicide, Muslim, Badakhshan, Tajikistan, Central Asia
Introduction
Suicide is a serious and complex problem experienced in every region and among every religious group all over the world. Suicide is a multidimensional issue, often with no single cause or reason being able to explain its occurrence. Seventy-nine percent of all suicides happen in the low and middle-income countries of the world, which include most majority Muslim countries, where resources for prevention and intervention are minimal [1]. Although research has focused more on developed countries, research on suicide in low- and middle-income countries has increasingly emerged that provides insights into risk and protective factors, lived experiences, and contextually appropriate interventions. Further, 60% of all suicides occur in Asian countries [2]. Socio-familial and economic factors are predominantly associated with suicide rather than mental illness in developing Asian countries [3]. Unfortunately, research in Central Asian countries is diffuse and has received scant attention, despite their high rates of suicide.
Striking differences in the presentation and meaning of suicide, the methods used for suicide and the factors associated with suicide between the rich and poor countries prompt urgent attention to studying suicide in its local socio-cultural, religious contexts [4]. Particularly, suicide methods employed by individuals are culturally relevant and dependent on availability of means in the local context. In Asian countries including Tajikistan, hanging is the most common method of suicide [5,6]. The present study also revealed hanging followed by drowning to be the most commonly used methods for suicide due to availability of means.
A recent systematic review of the literature on suicide in Central Asia identified only 15 studies that examine suicide in the five Central Asian countries (Kazakhstan, Kyrgyzstan, Uzbekistan, Tajikistan, Turkmenistan) [6]. In Tajikistan, of the six studies identified, no study was found that focused on suicide in Badakhshan, the poorest province in the country with most of its population identifying as Muslim. Thus, this research study seeks to address this gap by investigating the phenomenon of suicide in Badakhshan, Tajikistan. Specifically, this qualitative grounded theory study aims to 1) describe the lived experiences of suicide in Badakhshan, Tajikistan; and 2) identify the factors associated with suicide in Badakhshan.
Methods
Study Overview
This study was guided by the following research questions: 1) How do individuals in Badakhshan experience a suicide attempt? And 2) What are the factors that have contributed to that attempt? The study setting was the large, but remote province of Badakhshan in Tajikistan. The study used Charmaz’s [7] constructivist grounded theory methodology because it allowed for the examination of how social, historical, cultural and religious context of this region influences the phenomenon of suicide among those who experienced it.
Study Setting
The geographical setting for this study is the province of Badakhshan in Tajikistan. Tajikistan is the smallest and poorest country in Central Asia [8] with 97% of its population identifying as Muslim [9]. Also, it is one of the most under-resourced countries in the world with a per capita income of USD 2,300 [10]. The average monthly salary in Tajikistan is USD 93 with almost 40% of its gross domestic product derived from remittances sent home by migrant workers. Limited research has estimated the rate of suicide in Tajikistan to be 7.2 deaths per 100,000 people [11].
In Tajikistan, Islam is the predominant religion and Islam explicitly forbids suicide [12]. Further, according to the criminal code of Tajikistan, pushing someone to suicide is punishable by law [13]. The context of criminality associated with suicide is largely responsible for the significant underreporting of suicide attempts, making Tajikistan a country where reported deaths by suicides are higher than attempts [14]. Culturally, similar to other Asian countries, patriarchy is deeply embedded in the socio-cultural milieu, women occupy the lowest position in the family and gender-based oppression is rampant [15]. Adult children tend to live with their families of origin until they get married, and issues of mental health and suicide are highly stigmatized among families and the wider society [4].
Badakhshan is the poorest province in Tajikistan and is home to only 3.3% of the Tajik population, which is approximately 218,000 people [16]. The Pamir Mountain range goes through Badakhshan and extends into Afghanistan, China, Kyrgyzstan, and Pakistan. As such Badakhshan is often called ‘The Pamirs’ and the people who live in Badakhshan are called Pamiris. Many scholars recognize the extreme geographical remoteness of the region which influences the socio-economic vulnerability and isolation of the communities living there [17]. The remote location, harsh geographical environment, mountain landscape and the weather have an impact on life in Badakhshan increasing the isolation and lack of accessibility to the province [18].
Constructivist Grounded Theory
Grounded theory methodology is a prominent qualitative research method, originally developed by Glaser and Strauss in the 1960s. According to the principles of grounded theory method, theories should be developed inductively from lived experience [19]. Specifically, theories should be “grounded” in data from the field, and theories must focus on the actions, interactions and social processes of the participants [19,20]. The purpose of conducting grounded theory research is to develop an emergent theory that is grounded in the data by utilizing systematic, theoretical data collection and inductive data analysis procedures [7,19]. Charmaz [7] further posits that theories do not emerge from the data; they are constructed by the researcher through active interaction with the data. A key aspect of qualitative research is being clear about one’s position, biases and motivations for why and how the study is being conducted. Thus, the researcher’s decisions, the questions that the researcher asks of the data, as well as their background shapes the research process and the findings [21]. As such, this author investigates suicide in this remote province of the world as a social worker and as a Muslim American woman attempting to alleviate human suffering and understand lived experiences of suicide in the local socio-cultural, and religious context.
This exploratory qualitative research sought to understand the lived experience of a phenomena like suicide among individuals who have attempted it in Badakhshan, within their sociocultural and religious context. It sought to generate a theory about the perspectives on the experience of suicide and factors contributing to the suicide attempts in Badakhshan using the constructivist grounded theory methodology [7].
Understanding lived experiences of phenomenon like suicide is essential in research, not just as a human rights issue but necessary for development of culturally appropriate interventions [22]. The constructivist grounded theory approach employed examined how social, historical, religious, and cultural contexts of the studied phenomenon (suicide) affects people’s actions, meanings and experiences, and how power, inequality and oppression shape people’s actions, meanings and experiences [23]. In the context of Badakhshan, Tajikistan, this methodology had the most promise for the study of lived experiences of suicide, given the unique socio cultural, religious and political context of the region.
Recruitment and data collection
This study aimed to explore the lived experiences of individuals who attempted suicide in the province of Badakhshan, Tajikistan and was guided by the following research questions:
I) What are the lived experiences of individuals who attempted suicide?
II)What are the factors associated with suicide in this region?
Recruitment in Badakhshan, Tajikistan was conducted over a two-month period in 2019. The inclusion criteria included being at least 18 years of age, residing in Badakhshan, and experiencing a suicide attempt. Participants were recruited from the community through word-of-mouth, referrals by local leaders, community service provider agencies and snowball sampling. Data was collected using a semi-structured interview protocol, with in-depth interviews being conducted with 12 (7 female and 5 male) participants who had attempted suicide. Demographic information was gathered through a survey. Interviews were conducted in the homes of the participants with the help of two interpreters. Each participant received a food basket worth USD 5.00.
The following is an example of a question from the interview protocol. ‘All of us face difficulties in life. What are some difficulties that you are experiencing in your life? Prompt: Let’s start with work, money, family.’ Interviews were conducted in the participants’ native language, including Tajik, Shughni, Rushani, Russian and English and lasted 45-60 minutes each. Interviews were recorded and transcribed directly into English. Two multilingual research assistants independently translated and transcribed all the interviews into English, which were then coded by the author. Translated versions of data from both research assistants were compared and discrepancies were resolved through discussion. Both translators agreed on the final transcript which was then coded by the author. Data for this study also included the descriptive and reflective field notes of the author.
Data Analysis
Analysis of the data considered how participants constructed meanings and actions related to their suicide attempt. In line with grounded theory methods, the data started to be coded as soon as it was gathered; thereby, data collection and data analysis proceeded simultaneously [19] to produce an emergent theory. Initial codes were developed at the same time as more data was collected. Tentative conceptual ideas were developed early in the process and then examined through further sampling, inquiry and comparative analysis. Codes and categories were agreed upon by all members of the research team and discrepancies were resolved through discussion. Memos were written during the coding process and were discussed with the research team.
Data from interviews, observations, field notes, and reflections formed all the data that were analyzed. All the data were entered into NVivo-9, a qualitative data analysis software package designed for use with qualitative research. Codes and concepts were developed using the software.
Rigor
One of the key characteristics of qualitative research is its attention to maintaining rigor in the research. Rigor is defined as the quality of being thorough and accurate [24]. Lincoln and Guba’s [25] four concepts in maintaining rigor—credibility, transferability, auditability, and confirmability were all applied in the study. Early familiarity with the culture, triangulation of data, peer scrutiny of analysis, frequent debriefing, and detailed descriptions [26] were used to ensure credibility. Clear scope and boundaries of the study were established at the onset and procedures were systematically documented. A written audit trail was kept that documented major turning points and decisions during data collection and analysis.
Ethical Considerations
The Institutional Review Board at the University of Houston Downtown provided the ethics approval for the study after a review of the study protocols by the University of Central Asia. Given that this study focused on experiences of suicide, the risk for unpleasant thoughts and feelings was inevitable. A suicide risk assessment protocol was developed and referrals to the local social services agency were provided if needed. Participants had the option to withdraw from the study at any time.
Findings
Twelve individuals were interviewed for this study: seven female and five male. All 12 participants screened positively to the following three questions: i) Are you over 18 years of age? ii) Do you live in Badakhshan? iii) Have you made a suicide attempt? Table 1 represents the demographic information of the participants.

Table 1: Participant Demographic Information
Data was coalesced into three core categories and several concepts within each category that responded to the research questions of this study. A total of 546 individual codes were developed that were subsequently grouped into more than 20 concepts. A total of 15 concepts were organized into three core categories which included 1) experiencing extreme hardship, 2) social support; and 3) factors associated with suicide.
1. Experiencing Extreme Hardship
Experiencing extreme hardship is defined as all the economic, social and geographical conditions that make up the difficulties associated with living life in Badakhshan. Experiencing extreme hardship is comprised of the following five concepts; no job/ income; working hard but not having enough; day to day survival is hard; harsh life conditions; and everybody is poor. All participants (n = 12) reported on their experiences with extreme hardship and how they struggled in their daily lives to meet their basic needs. All participants spoke of having no stable income and/or very sporadic sources of income. Participants expressed having very limited options for making a living and not having enough money to take care of essential things in life that included having enough food for the year. Also, participants talked about refraining from seeking help from others, because everybody was too burdened with their own troubles, struggling to survive, and everybody was poor.
The concept of no job and no income reflected participants’ descriptions of not having any employment outside of the home and not having any work to generate a source of income. Working hard but not having enough meant that participants worked hard, they were not lazy or unskilled. Yet, they did not make enough to live and meet their basic needs. All the participants (n=12) had more than a high school education and reported working very hard–but simply could not make enough to live on. As illustrated by a 22-year-old female from Rushan, “I want to live here (in Tajikistan), but here, life is not good, and here if we work and if we earn money, it’s not enough…our people work so hard here but it’s just not enough.”
The physical and environmental context of Badakhshan renders harsh life conditions making day to day survival for people hard. The climate is cold (below freezing temperatures for nine months in a year) and energy sources (to heat homes) are scarce. All participants (n=12) talked about life being very hard in the mountains. Families are large and there are lot of people to sustain. A 38-year-old female participant in Ishkashim offers a glimpse into how hard she had to work just to survive. “I don’t have time to visit my relatives, my family or even go to weddings. I have to work all the time. From morning until evening, I am thinking of my life— how to make it better. I know that my life is difficult.” Family separation was another significant concept that emerged from the data. It meant being separated from members of the family, due to economic reasons, which is the case with many families in Badakhshan. Because of lack of work in Badakhshan, most families have at least one member working abroad to support those back in Tajikistan. Seven of the participants interviewed either had a family member residing abroad, or they themselves had gone to Russia at some point in their life to find work. Three female participants expressed a lack of support in their lives during the time of their suicide attempt and wished for their mothers to be living with them. Everybody is poor meant that most people in Badakhshan were in the same austere economic reality, where they faced poverty and lack of income. Together, participants’ struggles with living in Badakhshan reflected the extreme hardship they faced just to survive.
2) Social Support
Social support emerged as a significant category in the data and is defined as the act of seeking and receiving help in the form of emotional and social support or in-kind material help (e.g., food, clothing, medicines, etc.). This category consisted of the following five concepts: who can help, who should help, no help available and needing help but not asking for help. All participants (n=12) spoke about their experiences with getting help or not getting help and their ideas about who should help and how. Participants who sought help had a clear idea about who could actually help. All participants maintained that not everybody can help in a suicidal crisis. Participants who avoided getting help [reported] they did not believe that other people had the capacity to help them, or they did not want to burden others with their own problems. Who can help meant the acknowledgement of a class or category of people who had the capacity and the willingness to help other people. The categories of people who could provide meaningful help were doctors, psychologists, religious authorities (Khalifas) and those family members who had the material resources to assist.
Who should help is defined as a body of individuals or institutions that should exist in order to assist those individuals who are suicidal. All participants (n=12) stated that help should be available to those thinking about suicide. Who should help was strongly articulated by a 22-year-old female from Rushan.
First of all, I think in Badakhshan, we are weak. We do not talk about our problems with our parents and our parents do not know about our problems. If I’m sad, my parents don’t ask me “what happened, why you are sad?” And this is all over our society. I talked about my friend [who died by suicide]—her mother said, “What was her problem? Everything was okay with her, so why did she do it [attempt suicide]? But she had a problem, and everything was not okay with her. We feel shame talking with our parents, telling them our problems, [telling them] what’s happening with us. They do not know our problems; they just feed us and give money and that is it. Parents should help their children and observe [their children]. [They should] use psychologists. Parents should talk with their children. (22-year old female, Rushan)
Many participants expressed a lack of parental support and guidance in times of emotional need. Many participants also said that professional help must be available to people for this issue. No help available meant that in Badakhshan, no real help is available to those who think about and consider suicide and people do not perceive that help is available. For instance, one participant said, “This is a problem, I think… there are no psychologists to even ask for advice or something—there is nothing. There is nobody who you can go to and ask for help.”
Some participants talked about having no confidence in the kind of help that was available and confidentiality being a major issue in seeking help. Participants acknowledged that the community in Badakhshan is small and close knit and that there was no assurance that if one asked for help, that their confidentiality would be honored. For instance, one participant said,
There is no one who could help suicidal people because here you can’t find support, here you can only be humiliated and criticized. Even if you go to the psychologist, he won’t help you; instead, he will go to your relatives and tell your family members. (20-year-old female, Shughnan)
Participants were skeptical about the trustworthiness as well as the competence of the professional help that was available. Needing help but not asking for help meant that help was needed but not sought. Many participants acknowledged that they could have done with “help” during their crisis with the suicide attempt but acknowledged that they never considered asking someone for help. Most of them said that they would not go for help because everybody is busy in their own lives and that they would not want to bother others by asking for help. Feeling shame in going to others for help and feeling a sense of weakness in doing so were some barriers to people seeking help. Also, not wanting to burden others was a powerful motivator. As illustrated by one participant who said, “I kept all my problems to myself. Even now if something happens, I don’t share with my parents. I don’t want them to suffer about my issues, they have their [own] problems.” (38-year-old female, Ishkashim)
3) Factors Associated with Suicide
Several distinct factors contributed to the suicide attempts of the participants. These included having easy access to means of suicide, impulsivity, insurmountable problems, resilience, and having a moral stance on suicide. Factors associated with suicide reflect both risk and the protective factors. All participants (n=12) spoke about their own decisions leading up to their suicide attempt, what actions they took and what meanings they ascribed to their actions.
Having easy access to means of suicide meant that for participants in Badakhshan, it was effortless to find a way to take their own life, as means were readily available. The geographical context of Badakhshan with its network of mountains and valleys across the province provided unlimited access to heights and raging rivers. Some participants (n=4) considered drowning by jumping in the river as a method, others (n=4) ingested a substance, and the remaining (n=4) used rope to hang themselves inside or outside of their home. All three methods were readily and easily accessible to the participants. Rope is abundantly available in rural homes and is used to tie firewood and animals. It would be rare to find a home in the villages that did not have rope. One participant explained, “We have rope in almost every house, we use it for bringing wood from outside, carrying [things] during housework. So, I took it [rope] and hung myself.” (62-year-old male, Rushan)
The traditional pamiri home with its structural pillars and ceiling beams presented an easy and private access to means of suicide by hanging. The concept of means restriction as we understand it in the western context as limiting access to means of suicide is almost inconceivable in context of Badakhshan. Given the mountains, valleys and rivers; the structural design of the pamiri home and the availability of rope in the rural context; and the ready availability of substances like vinegar, acid and regular medicines—all of this provided easy and unrestricted access to means of suicide for the participants.
Impulsivity was an important factor associated with suicide. Impulsivity in terms of a suicide attempt means being hasty, instinctive, and spontaneous in the decision to attempt suicide. It also means not having thought about suicide at length and having come to a quick and sudden decision to take one’s own life. In our sample, eight out of 12 participants made their suicide attempt within minutes of thinking about it. There was very little time and distance between their decision to take their life and the actual action of the attempt. For example, one participant ingested a substance immediately after hearing that people were talking about her having an affair with her stepfather. She recalled,
I remember the exact moment clearly. My grandmother and I were in the corridor and she [my grandmother] said “don’t you think that our neighbors and relatives—all of them know that you are not my son’s daughter; you don’t have a mother and you are living with him [my stepfather] in the same house?” After that, I went to my room…I was hysterical, and I decided to take the pills. At home, we have a big medicine box full of medicines and the pills were there. It was after lunch around 3pm. I knew that I could [take the pills and] sleep and never wake up. (20-year-old female, Khorog)
The combination of the geographical context of Badakhshan with the ease of access to means of suicide and the participants’ impulsive action in making the attempt added to the complexity and potential lethality of the attempt.
Insurmountable problems refer to participants having such monumental and enormous problems, which had no foreseeable solutions. Insurmountable problems refer to the reality of the problems being difficult and the perception of the participants— an inability to resolve them. Among the problems that participants considered insurmountable included physical and emotional issues related to the threat of losing parents for young women, feeling worthless, having constant headaches, and feeling sad all the time.
Other problems included experiencing cruelty or sexual abuse while growing up, having no help or respite in the incessant labor work, facing impending immobility for a child, having no support from husband in the marriage and facing a lifetime of poverty and loneliness with no hope in sight. Although these problems may not seem insurmountable to the western reader, in the context of Badakhshan, they appeared to have no solutions for the participants.
One female participant recalled being sexually abused as a child and said,
When I was just was 6 or 7 years old, I was in my aunt’s house, and it was nighttime. I remember that there was a man, he was drunk, and at night when we slept, I felt him touch me…I was sleeping, and he was near me and it was dark there and he slept near me. My cousin was sleeping on one side (of me) and my aunt and uncle slept on the other side. But the man was near me, and I felt—he put his hands on my body—this man, he ruined my life, he raped me with his finger, he ruined me…I didn’t talk to anyone, I just suffered until now [sobbing]. (22-year-old female, Rushan)
This participant never told anyone about the abuse and suffered alone. Within the close-knit community that she lived in, disclosing sexual abuse was very shameful and to her this problem was clearly insurmountable. Another participant further illustrated the concept of insurmountable problems as she recalled an incident when she and her family did not have anything. She said,
There was a time I had nothing. I made something to sell in the Afghan market in Ishkashim. I was so happy that I made some money. I bought some things—food, tea, bread to take home for my children. I bought everything and came out. On my way I realized that I don’t have money to go back home. I thought maybe the driver can take me home. When I came to the car, the driver right away asked for money. It was only one somoni to go from Ishkashim [Tajik-Afghan border] to my village, but I did not have one somoni. The driver asked me to get out (of the car) because I could not pay him. That incident affected me so much. I asked the driver if I could give him the tea that I bought, although I thought to myself—if I give him the tea how will I manage without tea for the whole week. Yet, I decided to give him the tea, but he did not agree to take me. And I walked all the way, for 6-7 kilometers to come home. Up until today— I will never forget—there was a time when I did not have even one somoni to go home. (38-year-old female, Ishkashim)
The extreme desperation of this participant in that moment, with her larger issues of abject poverty and isolation added to her list of insurmountable problems.
Resilience meant the courage and undertaking of the participants to continue to live their life, no matter the circumstances. One participant recalls,
Every time I wanted to jump [in the river], I saw my youngest daughter’s face and couldn’t do it because I thought no one can defend her. I am going crazy now with all my problems; my daughter needs surgery, her university is not paid, and problems with my husband. I don’t know what to do. I am so tired. But I didn’t jump because I imagined my daughter’s face which stopped me from doing that [jumping]. I came back and sat on the bench to calm down. Then I went home. The only happiness which I have, are my children. (40-year-old female, Khorog)
What can be surmised from participants’ experiences is the courage, resilience, and sheer determination to keep going against all odds. Collectively, participants’ experiences of hope, conviction and persistence proved to be a protective factor associated with suicide in Badakhshan.
Having a moral stance on suicide means endorsing a value system about suicide on cultural or religious grounds. For participants in Badakhshan, as per their religious doctrine, having a moral stance meant that “suicide is wrong or bad.” Despite the fact that all participants had thought about suicide, seven participants expressed a very clear moral stance on suicide and maintained that it was “wrong or bad.” One participant said, “It is worst for Muslims, God gave to us a soul, a clean soul, and we have to give it back clean—but not this way, not with suicide—only if God wants.” (23-year-old female, Rushan) For her, there was a distinct clarity – a moral judgment on the act of suicide. Another participant illustrated her moral stance on suicide. She said, “If people are attempting suicide, their place is in hell when they die”. (38-year-old female, Ishkashim) Collectively, participants’ inherent value about suicide being wrong emerged as a protective factor for most participants. Their moral stance on suicide, in addition to the sheer determination to live life were significant protective factors associated with suicide in Badakhshan.
Overview of Emerging Theory
This study explored the lived experiences of suicide in Badakhshan and attempted to identify factors associated with suicide in a diverse sample of participants who ranged in age, gender, and socioeconomic status. Although all participants were poor, two of the 12 participants lived in abject poverty. The participants in this study developed their understanding of suicide through their own religious and moral code, the societal norms and their personal values and beliefs regarding suicide. Some participants made sense of their attempt in rational ways, and others attributed their attempt to a force outside of their control. The emergent theory—a renewed commitment to life— reflects a process of enduring the experience of making and surviving a suicide attempt in the context of a remote Muslim community. The theory is comprised of a series of experiences that include enduring continual and extreme hardship, thinking about suicide and planning for suicide, followed by a series of cognitive considerations and behavioral actions. These actions include initiating the attempt or deciding to not initiate the attempt, making the attempt or encountering the attempt, aborting the attempt or being saved by others, making sense of the attempt and eventually making a renewed commitment to life. Whatever path the participants took in this process, eventually they all emerged stronger with a clearer will to go on, to live life and to endure whatever life brought to them.
The three core categories of experiencing extreme hardship, social support, and factors associated with suicide form the bedrock of the emerging theory. The emerging theory is reflected in a process that starts with a struggle to live life and a struggle to manage and survive. This struggle involves a series of incidents that include facing an added stressor to an already burdened life, thinking about suicide, initiating or not initiating action, aborting the attempt or being saved by someone, making sense of the attempt, receiving or not receiving help and emerging from the attempt with a renewed commitment to life (see Figure 1). All participants expressed that life was better for them now and that they were stronger now, which further illustrates their renewed commitment to life. They exhibited positive thinking, stating that they will not attempt suicide again. By this point in their life, they had figured out some of their vulnerabilities to the act of suicide and resolved to continue to live life to the best of their ability, although nothing significantly had changed around them. Participants found strength in the determination and resolve to continue living, even though that might be difficult. Wanting to be strong and conviction in their own strength suggests a restored spirit of hope and a renewed commitment to life itself.
Discussion
The present study examines the unique experience of the social process underpinning the phenomenon of suicide from the perspective of the people of Badakhshan. The study generates a theory to explain why and how individuals in Badakhshan reach the decision of suicide, the circumstances surrounding that decision, and the consequences of that decision. The emerging grounded theory entitled, a renewed commitment to life, is a process of struggle and survival, going through the process of making the suicide attempt and emerging from it with a stronger commitment to live. This process reflects the lived experiences of the people of Badakhshan and details the hardships endured by the participants. Although the findings in this study are unique to Badakhshan, results have support in the literature on suicide in low- and middle-income countries.
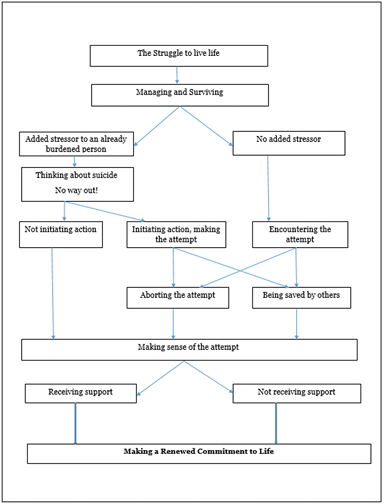
Figure 1: Emerging Theory: A Renewed Commitment to life
This study specifically highlights the psychosocial stressors of economic hardship and lack of employment as predominant struggles within the lived experiences of the people of Badakhshan. Lack of income stability and financial indebtedness as acute stressors for suicide is well established in the poorer countries around the world [2,27-29]. In the economically challenged, developing countries of the world, there is a significant and consistent relationship found between unemployment and suicide [2]. Among Asian men, unemployment or job-related stress is found to be a more common risk factor of suicide compared to men in the developed nations of the world [27,29]. The work-related issues including job-instability, financial indebtedness or unavailability of work acutely affected the men in our sample.
Findings from this study suggest that in Badakhshan, although the education level of the population is relatively high, lack of economic opportunity and the inability of people to meet their basic needs are acute stressors in people’s lives. Interestingly, economic issues and poverty are significant issues also found in suicides in other parts of Central Asia [6]. In a UNICEF study on suicides in the Sughd region of Tajikistan, financial debt for males was reported to be one of the main reasons for suicide among men [14].
Tajikistan has high rates of international labor migration and family separation for economic reasons is commonplace [30,31]. In Badakhshan, many young adults have lived without one or both parents since they were children. Approximately 49% of Tajikistan’s gross domestic product comes from remittances sent home by migrant workers, amounting to USD 2.67 billion [30]. In Badakhshan, there is a higher incidence of female migration than the other regions of Tajikistan [31]. An important negative effect of migration is the lack of parental guidance and its influence on the mental health of the children. Among families with migrant parents, children are often affected negatively by the absence of a parent, with a particular impact on their psycho-social well-being [32]. Research has found that children left behind tend to become withdrawn, sad and depressed [33]. This was found to be more common with girls than with boys [31]. This was confirmed by participant interviews; three young female participants had their mothers living and working abroad and were unable to receive emotional support from them during the time of their suicidal attempt. Studies show suicidal adolescents, compared to non-suicidal adolescents, demonstrate higher rates of early losses including long-term separation from one parent [34]. In a UNICEF study on suicides in the Sughd region of Tajikistan, findings indicate that a young person whose mother has migrated will do much worse than a young person whose father has migrated [14]. In Badakhshan, this seemed to be the case for young women participants who were attempters of suicide.
Among the findings of this study, relationship issues, family conflict and “gossip” or “rumors” particularly about women’s moral character are acute stressors for women attempters of suicide. In many Asian countries around the world, family disputes are a pivotal trigger in suicides [35]. Studies have identified that stresses associated with arranged marriages, young motherhood, sexual and physical violence, economic dependence make women more susceptible to suicidal behavior [36]. These factors that are uniquely associated with suicides among women and largely corroborated in the present study on suicide in Badakhshan.
In the U.S. and other developed countries around the world, mental health issues have a critical role in suicide [1]. Findings from this study suggest that in the context of Badakhshan, economic hardship and social issues seemed to have more prominence. Participants predominantly expressed a struggle with psychosocial issues, economic issues, and family issues. Psychosocial support of any kind is very limited in Badakhshan with a clear stigma around accessing these services even if available. Actual treatment for mental health issues is almost non-existent. In low- and middle-income countries around the world and particularly in Asia, socio-economic issues, family problems, gender-based oppression, and cultural factors have an overwhelming role in suicide [6]. Furthermore, in India and China, mental illness accounts for only 35-40% of all suicides [35].
Stigma related to help seeking is consistently found in the larger literature on mental health and psychological well-being [37]. Among Asian women, lack of help-seeking is related to stigma, subordination within the family system and lack of social support. Such stigma translates to help seeking behavior with attitudes like “no one is able to help,” “I should be able to cope with this myself”, and “my problems will not remain confidential” [38]. The present study corroborates the deeply imbedded nature of such stigma among the participants who attempted suicide in Badakhshan.
Interestingly, in addition to this stigma, a powerful motivator among participants for not seeking help was the desire to not burden others with their troubles. Even in situations of life and death, the desire to not burden others was more powerful than the desire to be helped.
An important global public health strategy to reduce suicides has been the modification of the environment to lessen access to means of suicide [39]. This approach of means restriction is reported to be one of the intervention measures with strongest empirical support [40]. Also, restriction of access to a specific suicide method can have a powerful impact when the method is highly lethal and common [41]. In the case of Badakhshan, jumping into a river or hanging are the most common methods for suicide; both are highly lethal and access to neither of the methods can be restricted by modifying the environment.
This research found impulsivity predominantly associated with suicide attempts. A study in Sri Lanka with 268 patients hospitalized for poisoning found that over half of these patients ingested the poison after less than 30 minutes of thought, generally immediately following an argument [42]. This research is consistent with the findings of the present study. Many of the participants in the study made their attempt on an impulse, they either made the attempt with other people present or immediately called someone and disclosed that they made the attempt. Further, impulsivity is identified as one of the five constructs consistently associated with fatal attempts.
Childhood sexual abuse, considered to be part of adverse childhood experiences (ACE) has consistently been shown to be associated with increased risk of suicidal thoughts and behavior [43]. ACEs are potentially traumatic events that occur in childhood which are linked to chronic health problems, mental illness and substance abuse issues in adulthood [44]. Particularly in the context of Badakhshan, which is a close-knit traditional society, childhood sexual abuse carries a lot of stigma and shame. Disclosure of sexual abuse has the potential to render the person ostracized, humiliated, and isolated from others. The present study found childhood sexual abuse and the consequent disclosure therefore, associated with suicide.
Limitations
This is the first study to our knowledge investigating suicide among the population in Badakhshan, Tajikistan; a remote Muslim province of Central Asia. The sample size in this study is relatively small (n=12) limiting the inferences that can be made with this research. This study set out to explore the lived experiences of suicide in a limited geographical location which is large and spread out with some very isolated areas. Another limitation of the study was an entirely female research team (resulting in more female participants) and the author’s inability to speak the local languages. Given the paucity of prior research on suicide in Tajikistan, and no studies on suicide in the province of Badakhshan, the present study although limited in scope, attempts to lay the basic groundwork for future research to be initiated.
Conclusion
This study is an important contribution to the field of suicide. Suicide research in remote communities is rare. Such research is very sensitive—much more sensitive than studying physical illness in these communities. Investigating suicide in a province like Badakhshan, akin to researching suicide in remote communities around the world, requires a unique and insightful approach. Integral to such studies in remote parts of the world is a holistic examination of the context in which suicide is investigated. The present study attempts to investigate the lived experiences of suicide in the unique cultural, religious, geographic, and environmental context of Badakhshan, Tajikistan. This research lays the groundwork for future work on community specific and culturally appropriate suicide prevention and intervention strategies. Culture, context, religion, and environment significantly influence suicide across the world and to effectively develop preventative strategies and interventions for suicide in Tajikistan, more targeted research into the unique cultural, family, and social context of this province is warranted.
Acknowledgement:
This research was partially funded by The Institute of Ismaili Studies, London through the Alumni Research Grant.
Conflict of interest:
The authors declare no conflict of interest.
References
World Health Organization, (2019). Fact Sheet: Suicide.View
Chen, Y., Chien-Chang Wu, K., Yousuf, S., & Yip, P. (2012). Suicide in Asia: Opportunities and Challenges. Epidemiologic Reviews, 34(1), 129-144.View
Patel, V., Chisholm, D., Parikh, R., Charlson, F. J., Degenhardt, L., Dua, T., et al. (2016). Addressing the burden of mental, neurological, and substance use disorders: Key messages from Disease Control Priorities, 3rd edition. Lancet; 387:1672-85.View
Savani, S., (2020). Suicide in Asia: A Literature Review in Institute of Public Policy Working Paper Series, University of Central Asia https://ucentralasia.org/Resources/Item/2779/ENView
Ajdacic-Gross, Vladeta, Weiss, Mitchell G, Ring, Mariann, Hepp, Urs, Bopp, Matthias. et al. ( 2008). Methods of suicide: international suicide patterns derived from the WHO mortality database. Bulletin of the World Health Organization, 86 (9), 726 - 732. World Health Organization. http://dx.doi.org/10.2471/ BLT.07.043489View
Savani, S., Gearing, R., Frantsuz, Y., Sozinova, M. (2020). Suicide in Central Asia in Suicidology Online 2020; 11(1), 1-12 View
Charmaz, K. (2006). Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. Sage Publications.View
Khodjamurodov, G., Sodiqova, D., Akkazieva, B., Rechel, B. (2016). Tajikistan: Health system review. Health Systems in Transition, 18(1):1–114.View
Karagiannis, E. (2006). The Challenge of Radical Islam in Tajikistan: Hizb ut-Tahrir al-Islami. Nationalities Papers, 34(1), 1-20.View
United States Central Intelligence Agency. (2017). The World Fact book. Retrieved on June 3, 2018View
World Health Organization (2015). Suicide rates, Age standardized Data. View
Gearing, R. and Alonzo, D. (2009). Religion and Suicide. Journal of Religion and Health 48(3).View
Savani, S. (2020b). A grounded Theory Study of Suicide Attempts in Badakhshan: A Renewed Commitment to Life (Order No. 28182264). [Doctoral dissertation, University of Houston] ProQuest Dissertations & Theses Global.View
UNICEF-Tajikistan. (2013). Prevalence and Dynamics of Suicide among Children and Young People (12-24 years of age) in Sughd region, Tajikistan. View
Haarr, R. N. (2010). Suicidality among battered women in Tajikistan. Violence Against. Women., 16, 764-788.doi: 10.1177/1077801210374409.View
Mastibekov, O. (2014). Leadership and authority in Central Asia: The Ismaili community in Tajikistan, New York: Routledge.View
Davlatshoev, S. (2006). The Formation and Consolidation of Pamiri Ethnic Identity in Tajikistan, Masters Thesis, The Graduate School of Social Sciences, Middle East Technical University.View
Hinz, S. (2007). Dance, Mysticism and Sensuality: Perspectives from Tajikistan. Master’s Thesis, University of Hawai’i.View
Glaser, B. G., & Strauss, A. (1967). The Discovery of Grounded Theory. Chicago: Aldine.View
Creswell, J. (1998). Qualitative Inquiry and research design: Choosing among five traditions, Thousand Oaks, CA: Sage Publications.View
Willig, C. (2013). Introducing Qualitative Research in Psychology. City University, London.View
Byrne, L. (2017). Promoting lived experience perspective: Discussion paper prepared for the Queensland Mental Health Commission. Brisbane: Queensland Mental Health Commission. View
Charmaz, K. (2012). Mixing or Adding Methods?: An Exploration and Critique, in N. K. Denzin and M. Giardina (eds.), Qualitative Inquiry and the Politics of Advocacy. Walnut Creek, CA: Left Coast Press.View
Cypress, B.S. (2017) Rigor or Reliability and Validity in Qualitative Research. Dimensions of Critical Care Nursing, 36, 253-263.View
Lincoln, Y., & Guba, E. G. (1985). Naturalistic Inquiry. Newbury Park, CA: Sage. View
Shenton, A. K. (2004). Strategies for Ensuring Trustworthiness in Qualitative Research Projects. Education for Information, 22(2), 63-75.View
Amagasa, T., Nakayama, T. and Takahashi, Y. (2005), Karojisatsu in Japan: Characteristics of 22 Cases of Work Related Suicide. Journal of Occupational Health, 47: 157-164. doi:10.1539/joh.47.157View
Mishara, B. (2008). Suicide and the Economic Depression: Reflections on Suicide during the Great Depression, International Association of Suicide Prevention News bulletin.
Phillips, M.R.; Li, X.; Zhang, Y. (2002). Suicide rates in China, 1995–1999. Lancet, 359, 835–840.View
Lemon, E. (2014). Dependent on Remittances, Tajikistan’s Long-Term Prospects for Economic Growth and Poverty Reduction Remain Dim (Washington, DC: Migration Policy Institute).View
United Nations Children’s Fund (UNICEF). 2011. Impact of Labor Migration on “Children Left Behind” in Tajikistan. Dushanbe, Tajikistan: UNICEF. View
Graham, E. and Jordan, L.P. (2011), Migrant Parents and the Psychological Well-Being of Left-Behind Children in Southeast Asia. Journal of Marriage and Family, 73: 763-787.View
Zhao, C., Wang, F., Zhou, X., Jiang, M., & Hesketh, T. (2018). Impact of parental migration on psychosocial well-being of children left behind: a qualitative study in rural China. International journal for equity in health, 17(1), 80. https://doi. org/10.1186/s12939-018-0795-zView
Séguin, M., Lynch, J., Labelle, R., & Gagnon, A. (2004) Personal and Family Risk Factors for Adolescent Suicidal Ideation and Attempts, Archives of Suicide Research, 8:3, 227-238.View
Vijayakumar, L. (2005). Suicide and mental disorders in Asia. International Review of Psychiatry; 17(2):109–114.View
Vijayakumar, L. (2015). Suicide in Women, Indian Journal of Psychiatry, 57 (6), p 233-240.View
Tucker, J., Hammer, J., Vogel, D., Bitman, R., Wade, N., & Maier, E. (2013). Disentangling Self-Stigma: Are Mental Illness and Help-Seeking Self-Stigmas Different? Journal of Counseling Psychology, 60(4), 520–531.View
Gilbert, P., Gilbert, J., Sanghera, J. (2004). A focus group exploration of the impact of izzat, shame, subordination and entrapment on mental health and service use in South Asian women living in Derby, Mental Health, Religion & Culture. 109-130.View
Yip, P., Caine, E., Yousuf, S., Chang, S., Wu, K., & Chen, Y. (2012). Suicide 3: Means restriction for suicide prevention. The Lancet, 2393–2399. docview/1022967728/View
Daigle M.S. (2005). Suicide prevention through means restriction: assessing the risk of substitution. A critical review and synthesis. Accidental Analysis and Prevention; 37: 625–32.View
Sarchiapone, M., Mandelli, L., Iosue, M., Andrisano, C., & Roy, A. (2011). Controlling access to suicide means. International Journal of Environmental Research and Public Health, 8(12), 4550–4562.View
Eddleston, M., Karunaratne, A., Weerakoon, M., Kumarasinghe, S., Rajapakshe, M., Sheriff, M. H., Buckley, N. A., & Gunnell, D. (2006). Choice of poison for intentional self-poisoning in rural Sri Lanka. Clinical toxicology (Philadelphia, Pa.), 44(3), 283–286. View
Molnar, B. E., Berkman, L. F., & Buka, S. L. (2001). Psychopathology, childhood sexual abuse and other childhood adversities: Relative links to subsequent suicidal behaviour in the US, Psychological Medicine, 31(6), 965–977.View
Adverse Childhood Experiences Study. Centers for Disease Control and Prevention Web site. View