
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 7 (2025), Article ID: JMHSB-207
https://doi.org/10.33790/jmhsb1100207Review Article
Assessing the Social Skills of Children with Autism in Clinical and Educational Settings: A Guide for Practitioners
Scott Bellini, Ph.D.,
Department of Emergency and Protective Services, Capitol Technology UniversityAssociate Professor, Department of Counseling and Educational Psychology, Indiana University, Bloomington, 201 N. Rose Avenue, Bloom ington, United States.
Corresponding Author Details: Scott Bellini, Ph.D., Associate Professor, Department of Counseling and Educational Psychology, Indiana University, Bloomington, 201 N. Rose Avenue, Bloomington, United States.
Received date: 19th September, 2025
Accepted date: 16th December, 2025
Published date: 18th December, 2025
Citation: Bellini, S., (2025). Assessing the Social Skills of Children with Autism in Clinical and Educational Settings: A Guide for Practitioners. J Ment Health Soc Behav 7(2):207.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Effective social skills programming is essential for interpersonal success and quality of life for children with autism. Social skill interventions require comprehensive assessment to identify individual needs and measure outcomes accurately. This article provides practical guidance to practitioners wishing to design effective social skills programming. Best practices for assessing social skills in clinical and educational settings will be provided, emphasizing the importance of linking assessment data to intervention objectives. Three categories of assessment are outlined: Type I measures, which use rating scales and interviews to evaluate social competence and stakeholder perceptions; Type II measures, which involve direct observation of social behaviors using systematic methods such as frequency, duration, latency, time sampling, and response ratio; and Type III measures, which assess social-cognitive skills like perspective taking and problem solving through role-play and standardized tasks. While Type III measures provide insight into cognitive processes, they do not reliably predict behavioral change, underscoring the need for multi-method approaches. The article also examines psychometrically sound assessment tools, and discusses the utility of self-report measures for capturing perceptions of social competence of children with autism. Beyond skill assessment, two factors critical to program success are also addressed: treatment integrity, the degree to which interventions are implemented as intended, and social validity, which ensures goals, strategies, and outcomes are meaningful and acceptable to stakeholders. By integrating rigorous assessment practices with attention to fidelity and social validity, practitioners can design individualized, evidence based interventions that promote sustainable social success for children with autism.
Introduction
Social skills play a critical role in building successful interpersonal relationships and enhancing overall quality of life. However, children with autism often face substantial difficulties in this area of functioning [1]. Assessing social skills and social competence is an essential step for designing effective social skills interventions [2]. Despite this, many programs neglect to evaluate these skills prior to implementing a social skills training program [2,3]. Social skills assessment serves two primary purposes: first, to pinpoint specific skill deficits that should be addressed during intervention, and second, to measure the effectiveness of the program. Although research on social skills interventions frequently includes outcome evaluations, or objective measures of change, it often overlooks initial assessments to identify target skills [4,5]. Furthermore, studies have suggested that the limited success of many interventions stems from poorly designed assessment tools that fail to align measured skills with those taught [3]. Adding to the challenge, there is a notable lack of published “best practices” to guide practitioners in assessing social skills among youth with autism. This article aims to outline the key components of a comprehensive social skills assessment and provide practical recommendations for educators and practitioners on how to accurately evaluate program outcomes.
The Need for Comprehensive Social Skills Assessment
Numerous quantitative meta-analyses have examined social skills interventions for children and adolescents, both with and without autism [4-13]. These reviews have yielded mixed findings regarding the effectiveness of such interventions for children with disabilities. Despite this variability, the collective evidence provides important insights into the essential components of successful social skills programs for children with autism. Bellini and Heck [3] synthesized research in this area and identified key elements of effective programming, one of which is the need for a comprehensive social skills assessment prior to implementing any intervention.
The initial step in any social skills program should involve a detailed evaluation of the child’s current social functioning [2]. This assessment seeks to answer a fundamental question: What factors are preventing the child from forming and maintaining social relationships (see Figure 1)? For many children, the barriers include specific skill deficits or performance challenges. In some cases, problematic social behaviors interfere with success, while in others, peer rejection or bullying, not the child’s skills, are the primary obstacles. For some children, all these factors may play a role. Conducting a thorough assessment of these dimensions of social functioning is therefore critical, yet it is often overlooked in practice. A well-designed assessment provides the foundation for effective intervention by identifying which skills should be targeted. For example, a child on the autism spectrum may struggle with initiating interactions, but what type of initiation difficulties are present? Is the child initiating rarely, or frequently but inappropriately? Does the child avoid initiating play but repeatedly asks questions? If so, are these questions about people or about topics? Are the topics of interest to the child or to the other person?
Unfortunately, many programs emphasize intervention strategies without offering guidance on assessing social functioning [2,3], which often leads to ineffective outcomes [3-13]. Not all children require the same strategies or need to learn the same skills. Too often, interventions begin without a clear understanding of the child’s unique needs. Typically, evaluations are conducted by professionals trained in observation and interviewing, such as teachers, psychologists, social workers, counselors, autism specialists, or speech-language pathologists. These evaluators gather information from individuals who know the child best, including parents and classroom teachers. While this section is primarily intended for practitioners, parents and teachers may also contribute by observing and recording social behaviors. As with all aspects of social skills programming, assessment should be a collaborative effort involving families and professionals from multiple disciplines. The evaluation should document both strengths and weaknesses in social functioning and directly inform intervention planning by establishing relevant goals, objectives, and component skills.
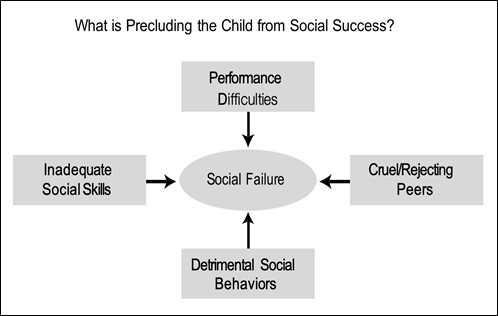
Figure 1. Illustrates the factors that contribute to social failure in youth with autism and the areas that are the focus of the evaluation.
Three Types of Social Skills Assessment
Gresham [14] identifies three categories of social skills assessment methods, each targeting different dimensions of social functioning (see Figure 2). Type I assessments typically use rating scales and interviews to evaluate social competence or perceptions of social performance. Type II assessments focus on directly measuring a child’s social skills and observable social behaviors. Type III assessments involve role-play activities to gauge understanding of social rules, along with observations and structured questions to assess social-cognitive abilities such as perspective-taking, joint attention, and problem-solving.
Type I Measures
Type I assessments evaluate social competence through rating scales and interviews. These methods are considered highly socially valid because they capture the perspectives of key stakeholders, such as parents and teachers, whose impressions often influence the acceptability of intervention goals [14]. As a result, objectives derived from these measures are generally viewed as relevant and socially appropriate. A major strength of Type I assessments is their efficiency; they allow practitioners to quickly gather information about a child’s social functioning across multiple settings and sources. However, a notable limitation is their inability to detect short-term behavioral changes. For instance, a child may demonstrate improvement in targeted behaviors without these changes being recognized by stakeholders. This section highlights two common Type I procedures: interviews and rating scales.
Interviews of Social Functioning
Interviews provide a practical way to collect and synthesize information about a child’s social functioning from multiple respondents across different environments. These interviews often serve as the starting point for a social skills program, helping evaluators make informed decisions about program goals and priorities. They also assist evaluators, especially those unfamiliar with the child, in understanding the child’s strengths and challenges in social interactions. Unlike rating scales, these interviews are broad and exploratory, offering a comprehensive view of social functioning.
Respondents typically include parents and teachers, but it is also beneficial to interview playground supervisors who observe children in natural settings and can provide valuable normative insights. The child is another critical source of information. Through questions such as “Do you have friends?” or “Do you want friends?” evaluators can gain insight into the child’s social awareness, interests, and problem-solving abilities. The child’s perspective may differ from that of adults, which adds depth to the assessment. Additionally, the interview offers an opportunity to observe the child’s communication skills firsthand, including eye contact, reciprocity, nonverbal cues, tone of voice, affect, and conversational abilities. To ensure accuracy, the interaction should remain natural, without excessive accommodations.
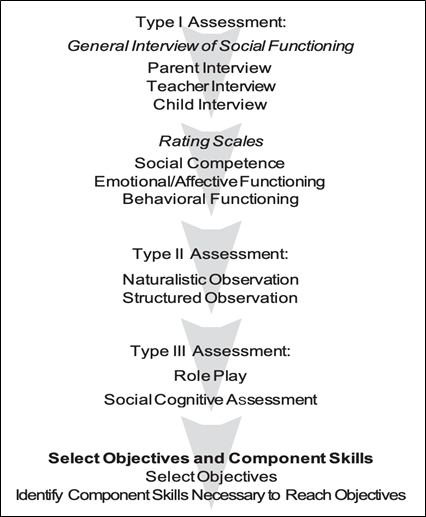
Figure 2. Three types of social skills assessment.
Rating scales
Rating scales are another widely used Type I tool for assessing social functioning. These instruments range from informal checklists to standardized measures and can be completed by parents, teachers, and sometimes the child. While not exhaustive, this section reviews several psychometrically sound tools with strong clinical utility: the Social Skills Improvement System (SSIS), the Social Responsiveness Scale Second Edition (SRS-2), and the Autism Social Skills Profile (ASSP-2). These measures have demonstrated high reliability and validity in research and practice and are commonly used by mental health professionals and educators in schools, clinics, and hospitals. Standardized administration procedures such as instructions and sample items should always be followed as outlined in each test manual. These tools are also valuable for monitoring performance over time.
Social Skills Improvement System (SSIS). The SSIS [15] is a standardized questionnaire designed to assess the social behaviors of children and adolescents ages 3–18. It evaluates whether a child demonstrates key social skills during social interactions. The parent and self-report versions consist of two scales: Social Skills and Problem Behaviors. The Social Skills Scale is most relevant to social skills programming. It consists of five subscales: Cooperation, Assertion, Responsibility, Empathy, and Self-Control. The Cooperation subscale includes questions related to helping others such as “completes household tasks without being reminded,” and “finishes class- room assignments within time limits.” The Assertion subscale measures initi- ating behaviors such as “initiates conversations with classmates” and“makes friends easily.” The Responsibility subscale pertains to behaviors that demon-strate the ability to communicate with adults and includes items such as “asks permission before using another family member’s property” and “informs you before going out with friends.” The Empathy subscale measures behaviors that show concern and respect for others’ feelings and viewpoints. Items include “I feel sorry for others when bad things happen to them” and “I say nice things to others when they have done something well.” The Self- Control subscale measures behaviors in response to conflict and non-conflict situations. Items include “controls temper during conflict with peers” and “responds appropriately when hit or pushed by other children.”
Social Responsiveness Scale–Second Edition (SRS-2). The SRS 2 [16] is a widely studied instrument with strong psychometric properties. It is the only commercially available social competency measure designed specifically for youth and adults with autism. Designed as a diagnostic tool and as a treatment monitoring tool, the SRS-2 covers social behaviors in addition to items related to other areas of autistic symptomatology, such as preoccupations and other repetitive stereotypical behaviors. It contains five subscales: receptive, cognitive, expressive, motiva-tional aspects of social behavior, and preoccupations and can be used with children ages 2–18 and with adults ages 19 and above.
Autism Social Skills Profile–2 (ASSP-2). The ASSP-2 [2] is an assessment tool created by the author that provides a comprehensive measure of social competence for youth on the autism spectrum. It covers a broad range of social behaviors, including initiation skills, social reciprocity, perspective taking, and nonverbal communication skills. Designed for use with youth aged 6 to 17, the ASSP-2 has demonstrated strong validity and reliability in preliminary analyses with 340 participants. The ASSP-2 was revised based on clinical experience, feedback from other clinicians, and earlier psychometric analysis results. It includes three subscales identified through factor analysis: Social Reciprocity, Social Participation Avoidance, and Detrimental Social Behaviors. These subscales represent specific social behaviors commonly associated with youth on the autism spectrum, which become the direct targets of subsequent interventions, referred to as component skills. The ASSP-2 (and its earlier version, the ASSP) has been used extensively in research and applied settings as a social skill outcome measure. The instrument has been empirically examined in published research articles over the past 20 years by numerous researchers in multiple countries including the United States, Greece, Turkey, Portugal, Brazil, Canada, Thailand, and Jordan [2].
The ASSP-2 serves two primary functions. First, it acts as an intervention planning tool by identifying specific social skill deficits that can be targeted during instruction. Its items are phrased so they can easily be adapted into social goals for educational or behavioral plans. Second, the ASSP-2 is useful for monitoring progress, making it appropriate as both a pre- and post-intervention measure of social functioning. Administering the tool before intervention provides a baseline for discussing the child’s social skills with parents. For example, an evaluator might say, “I noticed on the ASSP-2 you indicated Johnny rarely joins activities with peers. Could you tell me more about that?” The ASSP-2 can be completed by parents, caregivers, and other individuals, such as school personnel, who have direct knowledge of the child’s social functioning. It is designed for use by professionals including educators, psychologists, psychiatrists, social workers, counselors, and speech-language pathologists to support the development and implementation of social skills interventions.
Use of Self-Report Measures for Children with Autism. The appropriateness of self-report measures for children on the autism spectrum has been debated [2]. Critics argue that these individuals may lack the self-awareness needed to accurately describe their emotional, social, and behavioral functioning. This concern is partly valid; for example, a child may not fully understand abstract terms like “anxious” or “stressed.” However, most self-report instruments use concrete, observable statements such as “my hands shake” or “I am afraid of other children laughing at me,” rather than vague feeling-based questions. While discrepancies between child and parent reports are common, this issue is not unique to autism.
Research and clinical evidence indicate that self-report measures can provide valuable insights into social and emotional functioning in children with autism. In fact, adolescents’ self-ratings of social skills often predict social anxiety more accurately than parent ratings. A child’s perception of their social competence may be more influential than their actual skill level; for instance, two children with similar social abilities may differ in anxiety levels if one perceives their skills as weaker.
For these reasons, self-report measures of social, emotional, and behavioral functioning should be included whenever possible. When using these tools, consider the child’s cognitive and reading abilities. Test manuals typically specify the reading level required, and items may need to be read aloud for children who struggle with reading or become easily frustrated. Standardized instructions should be followed, and evaluators should check comprehension, rephrase items if necessary, and encourage questions for clarification.
Some items, such as “my heart races” may be challenging to understand for certain children with autism. These can serve as indicators of whether the child seeks help when needed. It is also important to triangulate self-report data with parent and teacher observations, as these adults may be unaware of concerns like fear of peer ridicule. Finally, individual items can serve as conversation starters for deeper exploration after the assessment. For example, if a child endorses “my hands shake,” the evaluator should follow up to learn when, where, and how often this occurs, as such details often inform future intervention targets.
Type II Measures
Recent research suggests that caregiver and self-report scales may not fully capture nuanced constructs like social cognition and social behavior, which appear unique in autistic youth [17]. In addition, while Type I measures provide a broad understanding of social competence from the perspectives of key stakeholders, they often lack the precision needed to directly capture short-term changes in behavior [18]. To address this limitation, practitioners frequently turn to Type II measures, which emphasize direct observation and offer a more sensitive approach to tracking progress toward specific intervention goals. Type II assessments involve the direct observation and measurement of a child’s social skills and behaviors. These tools are particularly valuable for monitoring progress and are widely used in applied research, especially within single-case design studies. A key strength of Type II measures is their sensitivity to small behavioral changes because they are closely aligned with specific treatment objectives. For example, if “joining activities with peers” is identified as a goal, the clinician would observe the child to determine whether this behavior increases during the intervention. The effectiveness of treatment is evaluated based on measurable changes in the targeted behavior.
Observation
Observing social behaviors should occur after completing interviews and rating scales. Two primary observation methods are commonly used to assess social functioning in children with autism: naturalistic and structured. Both approaches aim to capture the child’s social performance across various settings, individuals, and contexts. By the time observation begins, the evaluator should have a clear understanding of which social skills to monitor and in which environments. Data collection should focus on the skills and contexts identified as areas of concern during interviews and rating scale assessments. These observations not only help pinpoint skills to target in intervention but also provide a detailed picture of the child’s social environment, addressing the critical question: What factors are preventing the child from achieving social success?
Naturalistic Observation. Naturalistic observation involves monitoring and recording a child’s behavior in everyday social environments, such as playgrounds, cafeterias, or community settings near the child’s home. This approach is highly valuable because it captures authentic, spontaneous interactions within the child’s typical contexts. It enables evaluators to observe behavior across multiple settings and with different individuals, offering insight into how the child functions in both structured and unstructured situations. In addition to documenting the child’s behavior, naturalistic observation provides important details about environmental factors, such as noise levels, clutter, and other sensory stressors, as well as peer behavior. Observing how peers respond to the child is critical for determining whether peer awareness or peer mentoring might be necessary.
Naturalistic observation also helps establish a normative reference for comparison. For example, if concerns exist about the child’s participation in group activities, recording instances of “joining-in” behavior can be compared to similar behaviors in other children. Two recommended methods for selecting a comparison group include: (a) randomly observing a small group of children, and (b) asking the teacher to nominate three children with varying levels of social skills, which provides a representative range of social performance. Despite its advantages, naturalistic observation has limitations. It is time- intensive and may yield limited data for socially withdrawn children. Additionally, some school systems restrict classroom access for outside professionals, making it challenging for private practitioners to conduct observations.
Structured Observations. Structured observations involve placing the child in a controlled environment designed to encourage social interaction with selected peers. This approach often yields more detailed information in less time compared to naturalistic observation. For example, creating an activity that requires the child to demonstrate specific social skills can provide valuable insights. Typically, the child with autism is paired with one or two peer mentors in a setting rich with social opportunities, such as games and toys. The children are instructed to “play together,” and peer mentors may receive guidance on how to include the child in their activities. Although this setup is somewhat artificial, it offers ample opportunities to observe targeted social behaviors, which is the primary goal of the assessment. Peer selection should be based on a positive social history with the child and a willingness to participate in the playgroup.
Observational Recording Methods. Two widely used approaches for recording social behaviors in both naturalistic and structured settings are recommended: narrative recording and systematic recording. Narrative recording is a qualitative method in which the observer watches the child and writes descriptive notes about social functioning and the surrounding environment. This approach provides rich, detailed information but is inherently subjective, which can lead to variability between observers. For example, two individuals may interpret the same behavior differently. Because of this lack of reliability, narrative recording is less suitable for tracking intervention progress. However, it remains valuable for gaining insights into the child’s social context and complements more structured methods. Systematic recording uses predefined behavioral categories to capture specific social behaviors. This method offers a more objective and reliable measure of the child’s current social functioning and serves as a baseline for monitoring progress. Behaviors are recorded based on dimensions such as frequency, intensity, duration, latency, and context (e.g., where and with whom the behavior occurred). Clearly defining these behaviors before observation significantly improves reliability and the ability to detect changes over time. The section provides a description of basic systematic recording methods that are useful for directly measuring social behaviors. This section outlines several systematic recording techniques: frequency recording, duration recording, time sampling, latency recording, and response ratio (see Figure 3).
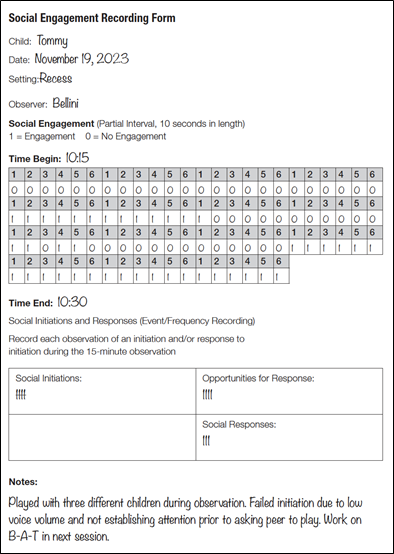
Figure 3. Example of systematic recording form using partial interval, frequency, and response ratio measures for three outcome measures: social initiation, social responding and social engagement.
Frequency recording. Also known as event recording, this method involves counting how often a behavior occurs within a specified time frame. For example, if tracking hand-raising during math class, the observer marks each occurrence throughout the observation period. Consistency in interval length is critical; varying observation times can distort results. If intervals differ due to uncontrollable factors (e.g., the child leaves the classroom), adjustments can be made by proportionally scaling the data. Social behaviors suitable for frequency recording include social initiations, responses, inappropriate comments, and verbal expressions of emotion.
Duration recording. Duration recording measures how long a behavior lasts from start to finish. This method is ideal for behaviors where time engaged is more meaningful than frequency. For instance, if the target behavior is social participation, frequency recording might show multiple brief interactions, giving a misleading impression of engagement. Duration recording, by contrast, captures sustained participation. Clear definitions of start and end points are essential for consistency. For example, a conversation might begin with verbal initiation and end after five seconds of silence.
Time sampling procedures. Time sampling provides an alternative, and less time-intensive method of recording behavioral durations and frequencies. The advantage of time sampling procedures is that they lessen the workload required of the observer, especially for behaviors with high frequencies and long durations. This is especially important when teachers are asked to record social behaviors in the classroom. Time sampling procedures require observers to record behaviors at specific points in time. That is, they do not have to continuously watch for behaviors to occur during the length of the observation period (as is the case with frequency recording), nor do they have to watch for specific beginning points and end points of a behavior (as is the case with duration recording). Using time sampling procedures, observation periods are divided into intervals. For instance, a 30-minute observation can be divided into thirty 1-minute interval or perhaps fifteen 2-minute intervals.
There are three types of time sampling procedures: whole interval, partial interval, and momentary time sampling. In whole interval recording, a behavior is considered to have occurred only if it is performed throughout the entire interval; that is, from beginning to end. This recording method is best suited for high-frequency behaviors and behaviors that occur without interruption, such as time on task. In partial interval recording, behaviors are considered to have occurred if they are performed at any time during the interval. The behavior does not have to occur for the entire interval. In addition, only one behavioral occurrence per interval is recorded. Even if the child initiates three interactions in one interval, only one initiation is recorded. This sampling technique is best suited for low-frequency behaviors and behaviors of very short durations, such as eye contact, emotional expressions, or certain inappropriate behaviors. Momentary time sampling is the most time efficient of the time sampling procedures because observers do not need to watch behavior for the entire interval. Observers record whether a behavior is occurring at a single moment in time, usually at the end of the interval. For instance, if the interval is 5 minutes in duration, then every 5 minutes the observer records whether the behavior is occurring at that moment in time. If the behavior occurred at other points during the interval, but not at that precise moment, the behavior is not recorded as having occurred. Therefore, this method is not recommended for low-frequency behaviors. It is best suited for high-frequency behaviors and behaviors for which duration is a primary concern, such as time on task, and social participation.
Latency recording. Latency recording, also called response latency, measures the time that elapses between a stimulus and a response, specifically, the interval between a directive and the child’s compliance. For example, if a teacher instructs the child to “line up for gym class,” latency is recorded from the moment the directive is given until the child lines up. The key to accurate latency recording is clearly defining the start and end points of the behavior.
This method is ideal for assessing response speed in situations requiring prompt reactions, such as following instructions, answering questions, responding to greetings, or other social behaviors. In these cases, latency provides a more meaningful measure than frequency because it reflects how quickly the child responds during interactions.
Response ratio. Response ratio is a method for evaluating the frequency of social responses relative to the number of opportunities to respond. It is calculated by dividing the total number of responses by the number of interaction opportunities (e.g., times others initiate contact). For instance, if a child responds 5 times out of 10 opportunities, the response ratio is 0.5. A perfect ratio would be 1.0.
This measure is more informative than simple frequency counts because it accounts for the context of social opportunities. A child may show zero responses during an observation, but this could reflect a lack of opportunities rather than an inability to respond. Conversely, comparing ratios across observations can reveal progress even when raw frequencies appear stable. For example, if a child responds 5 times out of 10 opportunities in one session (0.5) and 4 times out of 5 opportunities in another (0.8), the ratio indicates improved consistency in responding.
The Observational Social Competence Assessment (OSCA). Recent reviews underscore the importance of refining observational protocols to capture dynamic peer interactions and contextual factors in inclusive settings [19]. Liu et al. [20] introduced the Observational Social Competence Assessment (OSCA), a structured observation tool designed to capture multiple dimensions of social competence in children with autism. Unlike traditional rating scales, OSCA uses systematic coding procedures to evaluate behaviors such as initiation, reciprocity, and response to peers across naturalistic and semi-structured contexts. Psychometric analyses demonstrated strong internal consistency (Cronbach’s α values exceeding .82 across subdomains) and high inter-rater reliability, with intraclass correlation coefficients above .90. The measure also showed robust convergent validity with established social functioning scales and was sensitive to treatment-related changes, making it particularly useful for monitoring progress in intervention studies. These properties position OSCA as a valuable observational tool for both clinical practice and research, offering a reliable and responsive method for assessing real-world social behaviors.
Type III Measures
Recent research suggests that social cognition and observable social behavior are related but distinct constructs that should be assessed uniquely [17]. This underscores the importance of using these assessments alongside behavioral measures to obtain a comprehensive picture of social competence. Type III assessments target the cognitive aspects of social functioning, such as problem- solving, joint attention, and perspective-taking. These tools often use structured tasks to evaluate how children interpret and respond to social situations. For example, clinicians may present a video or scenario and ask the child to identify problems and propose solutions, or engage the child in role-play activities that require inferring another person’s thoughts or intentions. Classic measures include false-belief tasks like the Sally-Anne Test, which assess understanding that others can hold beliefs different from one’s own [21-23].
Although these skills are important for intervention, research indicates that Type III measures do not correlate strongly with measures of social competence (Type I) or observable social skills (Type II). Improvements on social-cognitive tasks do not necessarily translate into better social behavior, highlighting the psychometric limitations of these tools. For this reason, Type III measures are not used as outcome indicators in our BSR program. However, practitioners should employ them periodically to monitor progress in perspective taking, self-monitoring, and problem-solving abilities [2].
One well-known example is the False-Belief Test developed by Nelson, Plesa, and Hensler [23] to assess perspective-taking. In this task, children hear a story about Maxi, who places chocolate in a drawer before leaving home. While Maxi is away, his mother moves the chocolate to a cupboard. When Maxi returns, children are asked: Where will Maxi look for the chocolate? and Why will he look there? Correct answers require understanding that Maxi lacks the same information as the child and therefore has a different perspective. Typically, children around age five can infer that Maxi will look in the drawer, where he originally placed the chocolate. For children with autism, this ability often develops much later, if at all.
Assessing Treatment Integrity and Social Validity
Maintaining treatment integrity and ensuring social validity are critical for the success of any social skills program [3-5]. Ensuring that social skills interventions are implemented as intended is critical for achieving meaningful outcomes. Treatment integrity [24], often referred to as treatment fidelity, represents the degree to which intervention procedures are carried out according to the prescribed plan. High treatment integrity is essential for maintaining both internal and external validity in research and practice. When treatment integrity is compromised, it becomes difficult to determine whether poor results stem from an ineffective intervention or from improper implementation. This distinction is vital because interventions that appear unsuccessful may, in fact, fail due to inconsistent or incorrect application rather than flaws in the strategy itself. In educational settings, low treatment integrity is a major barrier to success, particularly when interventions require collaboration among multiple implementers such as teachers, parents, and paraprofessionals.
Assessing treatment integrity involves systematic procedures to verify adherence to intervention protocols (see Figure 4 for an example of a combined treatment integrity and social validity rating form). Direct observation is considered the most objective method, allowing evaluators to monitor implementation in real time and document whether each component of the intervention is delivered accurately. Observer post-rating scales provide structured evaluations immediately following sessions, offering a practical alternative when continuous observation is not feasible. Implementer self-reports and checklists are also valuable tools, enabling those responsible for delivering the intervention to record their own adherence and identify challenges encountered during implementation. Finally, interviews with implementers can uncover contextual factors that influence fidelity, such as time constraints, resource limitations, or misunderstandings about the intervention procedures. Using multiple assessment methods enhances reliability and provides a comprehensive picture of treatment integrity, guiding decisions about training, support, and program adjustments.

Figure 4. Example of a completed treatment fidelity and social validity rating form for a video self-modeling intervention.
Ensuring social validity [25], which refers to the social significance and acceptability of treatment goals, intervention strategies, and outcomes, is also critically important to program success. Social validity ensures that interventions are not only effective but also meaningful and acceptable to stakeholders, including parents, teachers, and the child. It encompasses three dimensions: the perceived importance and relevance of the goals, the perceived appropriateness of the intervention methods, and the perceived value of the results achieved. Social validity can have a direct impact on treatment integrity. For instance, if stakeholders do not view the treatment goals as significant or the strategies as acceptable or effective, they are less likely to support or implement the program consistently, undermining both treatment integrity and effectiveness.
Consumer satisfaction is a central component of social validity. When parents and teachers believe that the intervention addresses critical needs and employs strategies that are safe and practical, they are more likely to engage actively in the process. Establishing social validity begins during the initial assessment phase, where stakeholders provide input on treatment objectives and strategies, and continues throughout implementation via ongoing communication and feedback. Practitioners should present evidence of the intervention’s efficacy and explain the rationale behind selected strategies to build trust and commitment. By prioritizing both treatment integrity and social validity, practitioners create interventions that are not only scientifically sound but also socially meaningful, increasing the likelihood of sustained success and positive outcomes for children with autism.
Social validity can be assessed through structured interviews and systematic rating forms, which together provide a comprehensive understanding of stakeholder perceptions regarding treatment goals, intervention strategies, and outcomes. Interviews offer qualitative insights by engaging parents, teachers, and, when appropriate, the child in discussions about the relevance and acceptability of the program. These conversations typically explore whether the goals are considered important, the strategies practical and safe, and the anticipated outcomes meaningful, using open-ended questions to encourage detailed feedback and uncover potential barriers to implementation. Complementing this approach, rating forms provide a quantitative measure of social validity through Likert-scale items that gauge agreement with statements such as “The goals of this program are important for my child” or “The intervention strategies are acceptable and feasible” (see Figure 3). Collecting data from multiple stakeholders ensures a well-rounded perspective on the program’s perceived value. Combining interviews with rating forms not only strengthens the validity of the assessment but also fosters collaboration by giving stakeholders a voice in the process, ultimately guiding adjustments to goals or strategies, and increasing the likelihood of successful implementation and sustained engagement.
Summary
Comprehensive assessment of social skills is a cornerstone of effective intervention for children with autism. This article reviewed best practices for evaluating social functioning in clinical and educational settings, emphasizing the importance of linking assessment data to intervention objectives. Three primary assessment types were discussed: Type I measures, which include interviews and rating scales to capture perceptions of social competence; Type II measures, which involve direct observation and systematic recording of social behaviors; and Type III measures, which assess social- cognitive skills such as perspective taking and problem solving. Each method offers unique strengths and limitations, underscoring the need for a multi-method approach.
The article also highlighted the utility of psychometrically sound tools such as the SSIS, SRS-2, and ASSP-2, as well as the role of self-report measures in providing insight into perceived social competence of youth with autism. Observational techniques, including naturalistic and structured settings, were described alongside systematic recording methods such as frequency, duration, latency, time sampling, and response ratio. These procedures enable practitioners to monitor progress and tailor interventions to individual needs.
Finally, the article addressed two critical factors for program success: treatment integrity and social validity. Treatment integrity ensures that interventions are implemented as intended, while social validity reflects the acceptability and perceived importance of goals, strategies, and outcomes among stakeholders. Both elements require ongoing collaboration and feedback from parents, teachers, and the child. By integrating rigorous assessment practices with attention to integrity and social validity, practitioners can design interventions that are not only evidence-based but also socially meaningful, thereby improving the likelihood of sustained success in promoting social competence in youth with autism.
Competing Interests:
The authors declare that they have no competing interests.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author. View
Bellini, S. (2023). Building Social Relationships 3: A Systematic Approach to Teaching Social Interaction Skills to Children and Adolescents with Autism and other Social Challenges. Bloomington, IN: PDSA Publishing. View
Bellini, S., & Heck, O. (2019). The ingredients of effective social skills programming for children and adolescents on the autism spectrum. Journal of Autism, 6, 1-7. View
Gresham, F. M., Sugai, G., & Horner, R. H. (2001). Interpreting outcomes of social skills training for students with high incidence disabilities. Teaching Exceptional Children, 67, 331 344. View
Bellini, S., Peters, J., Benner, L., & Hopf, A. (2007). A meta analysis of school-based social skill interventions for children with autism spectrum disorders. Remedial and Special Education, 28, 153- 162. View
Babb, S., Raulston, T. J., McNaughton, D., Lee, J. Y., & Weintraub, R. (2021). The Effects of Social Skill Interventions for Adolescents with Autism: A Meta-Analysis. Remedial and Special Education, 42(5), 343-357. View
Dean, M., & Chang, Y.-C. (2021). A systematic review of school based social skills interventions and observed social outcomes for students with autism spectrum disorder in inclusive settings. Autism, 25(7), 1828–1843. View
Quinn, M. M., Kavale, K. A., Mathur, S. R., Rutherford Jr., R. B., & Forness, S. R. (1999). A meta-analysis of social skills interventions for students with emotional and behavioral disorders. Journal of Emotional and Behavioral Disorders, 7, 54–64. View
Reichow, B., Steiner, A.M., & Volkmar, F. (2012). Cochrane review: social skills groups for people aged 6 to 21 with autism spectrum disorders (ASD). Evidence-based child health: a Cochrane review journal, 82, 266-315. View
Wang, S. Y., Parrilla, R., & Cui, Y. (2012). Meta-analysis of social skills interventions of single-case re- search for individuals with autism spectrum disorders: Results from three level HLM. Journal of Autism and Developmental Disorders, 1–16. View
Forness, S. R., Kavale, K. A. (1996). Treating social skill deficits in children with learning disabilities: a meta-analysis of the research. Learning Disability Quarterly. 19(1), 2–13.16. View
Bellinger, J. M., Perlman, E. H., DiPerna, J. C. (2011). Social skill interventions for individuals with autism spectrum disorders. School Psychology Forum. 5 (4), 141-159. View
Alahmari, A., et al. (2025). Meta-analysis of social skills training interventions for children with autism spectrum disorder: Effect sizes and moderators. Review of Educational Research.
Gresham, F. M. (2002). Best practices in social skills training. Bethesda, MD: National Association of School Psychologists. 1029–1040 p. (Thomas A, Grimes J, editors. Best practices in school psychology. 4th ed). View
Gresham, F. M., & Elliott, S. N. (2008). SSIS rating scales. Minneapolis, MN: NCS Pearson View
Constantino, J. N., & Gruber, C. P. (2012). Social responsiveness scale (2nd ed) (SRS-2). Torrance, CA: Western Psychological Services. View
Simmons, C., et al. (2024). Distinguishing social cognition and social behavior in autistic youth: A structural equation modeling approach. Autism Research.
Sterrett, K., & Pizzano, A. (2025). Sensitivity of standardized social communication measures to short-term behavioral change in autism interventions. Journal of Autism and Developmental Disorders. View
Tsamitrou, A., & Plumet, M. (2024). Observational methods for assessing peer interactions in inclusive preschool settings: A scoping review. Early Childhood Research Quarterly.
Liu, Y., et al. (2025). Development and validation of the Observational Social Competence Assessment (OSCA) for children with autism. Journal of Autism and Developmental Disorders, 55 (11), 3838-3850.
Wimmer, H., & Perner, J. (1983). Beliefs about beliefs: representation and constraining function of wrong beliefs in young children’s understanding of deception. Cognition, 13(1), 103–128. View
Baron-Cohen, S., Leslie, A. M., & Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, 21, 37–46. View
Nelson, K., Plesa, D., & Hensler, S. (1998). Children’s theory of mind: An experiential interpretation. Human Development, 41, 7–29. View
Yeaton, W. H., & Sechrest, L. (1981). Critical dimensions in the choice and maintenance of successful treatments: Strength, integrity, and effectiveness. Journal of Consulting and Clinical Psychology, 49(2), 156–167. View
Wolf, M. M. (1978). Social validity: The case for subjective measurement or how applied behavior analysis is finding its heart. Journal of Applied Behavior Analysis. 11(2):203–214. View