
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 8 (2026), Article ID: JMHSB-211
https://doi.org/10.33790/jmhsb1100211Research Article
Permanent Housing as a Pathway to Mental Health and Social Well-Being: A Qualitative Interpretive Meta-Synthesis
Tracey Barnett McElwee*, PhD, LMSW, Theresa Flowers, PhD, LCSW, Courtney Bryan, MSP, Madeleine Flegal, B.A., Elizabeth “Ellie” Freeman, B.A. Ed., Alex Gillins, B. S and B. A., Payton Grannemann, B. S., Katelyn Orona, BSW, Brandy Rollins, B.S., LauraLyn Terherst, B.A., Alexia Thomas, B.A., Joe Veer, BA.HSE.SAB, ADC, Nancy White, B.A., Gracen Willhite, B.A.
School of Social Work, University of Arkansas at Little Rock, 2801 S. University Ave, Little Rock, AR 72204, United States.
Corresponding Author Details: Tracey Barnett McElwee, PhD, LMSW, Associate Professor, School of Social Work, University of Arkansas at Little Rock, 2801 S. University Ave, Little Rock, AR 72204, United States.
Received date: 03rd October, 2025
Accepted date: 27th January, 2026
Published date: 29th January, 2026
Citation: McElwee, T. B., Flowers, T., Bryan, C., Flegal, M., Freeman, E., Gillins, A., Grannemann, P., Orona, K., Rollins, B., Terherst, L., Thomas, A., Veer, J., White, N., & Willhite, G., (2026). Permanent Housing as a Pathway to Mental Health and Social Well-Being: A Qualitative Interpretive Meta-Synthesis. J Ment Health Soc Behav 8(1):211.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
People transitioning from homelessness to stable housing often face institutional obstacles, hazardous living conditions, and disconnected support systems that impact their psychological well-being, interpersonal connections, and behavioral health outcomes.This study employed an adapted Qualitative Interpretive Meta-Synthesis (QIMS) approach to explore the lived experiences of individuals residing in permanent supportive housing programs. A collaborative research team consisting of 12 Master of Social Work graduate students and faculty conducted systematic literature searches across eight academic databases from January through April 2025. Purposive sampling methods yielded nine qualitative studies comprising 358 participants, including program residents, staff members, and administrative personnel from the United States, Canada, and Norway. Through detailed line-by-line coding procedures, constant comparative analysis, and multiple triangulation strategies, six primary themes emerged: (1) Preserving Dignity and Personhood While Unhoused, (2) Structural Barriers to Independence, (3) Community as a Double- Edged Sword, (4) Navigating Unsafe or High-Risk Environments, (5) Distrust Rooted in Lived Experience, and (6) Experiences of Stability and Predictability in Permanent HousingFlexible Housing Models as a Pathway to Stability. These results demonstrate that permanent housing affects not only physical security but also emotional healing, personal identity, interpersonal trust, and social functioning. Although institutional discrimination and hazardous conditions can hinder recovery processes, interventions that prioritize adaptability, self-determination, and dignity promote safety, respect, and sustained wellness.
Keywords: Homelessness, Mental Health, Qualitative Interpretive Meta-Synthesis, Social Work
Introduction
Homelessness creates an enduring social issue, marked by housing instability and severe individual suffering [1]. Moving from homelessness to secure, permanent housing can involve a complicated journey, frequently filled by multiple personal and institutional obstacles [1,2]. People experiencing homelessness commonly move between different temporary accommodations, a pattern typically referred to as the "revolving door" effect of homelessness [1]. Successfully tackling this issue demands not only housing provision, but also thorough comprehension of the elements that prevent sustained stability and wellness [1,2]. The strong association between housing stability, mental wellness, and social conduct is thoroughly established, positioning this as an essential focus for research. Individuals facing homelessness commonly experience severe mental health disorders and overlapping substance abuse problems at disproportionate levels [3,4].
Permanent housing has proven to substantially enhance mental health results, by producing fewer hospital admissions, better symptom regulation, and decreased criminal justice involvement [4]. Beyond medical improvements, when one secures housing it aids in developing feelings of protection, self-worth, and capacity to reconstruct personal identity and life story, all of which are critical factors for emotional recovery and social reintegration [4]. Alternatively, housing uncertainty maintains an "institutional revolving door" where people cycle through homelessness, detention, treatment centers, and hospitals, demonstrating a mutual relationship between housing loss and incarceration, commonly moderated by psychiatric illness and substance dependency [5]. Consequently, reliable housing extends beyond simple accommodation; it serves as a primary factor in mental health and positive community integration, aligning precisely with publications focused on population health and social health determinants.
In this study, mental health is conceptualized as individuals' psychological and emotional well-being, by encompassing experiences of distress, recovery, safety, and autonomy subsequent to housing placement. Social well-being denotes individuals' sense of belonging, community integration, dignity, independence, and capacity to engage in meaningful relationships and fulfill social roles. These constructs are inextricably linked within the context of housing transitions and are predominantly manifested in qualitative narratives concerning stability, identity, and trust, rather than being solely reducible to clinical diagnostic criteria.
Review of Existing Literature
A substantial body of literature addresses housing interventions, their impact on mental health, and various challenges in achieving long-term stability.
Housing First and Supportive Housing Models
The Housing First model has become a prominent rights-based strategy, which prioritizes immediate access to permanent housing without mandating sobriety or treatment participation [4,6]. This framework commonly provides individuals with apartment options across dispersed locations while delivering intensive, personalized support services [4,7]. Research has repeatedly confirmed Housing First's success in fostering residential stability for people with severe mental illness and concurrent substance use disorders [1,3]. Likewise, Permanent Supportive Housing programs integrate subsidized accommodation with comprehensive wraparound services intended to assist participants in sustaining their housing arrangements [3,5]. Both Housing First and Permanent Supportive Housing seek to enable individuals with psychological health challenges to develop lasting social roles and achieve community integration [8]. Recent research continues to refine theoretical and empirical understanding of Housing First and permanent supportive housing models beyond traditional housing retention metrics. Post-2022 scholarship underscores the salience of service quality, relational support, and programmatic environments in mediating mental health outcomes, residential stability, and long-term well-being among formerly unhoused populations [9,10]. These findings indicate that while housing access constitutes a necessary foundation, participants' lived experiences within housing environments, including perceptions of safety, institutional responsiveness, and dignity function as critical determinants in sustaining housing stability and facilitating recovery trajectories.
Mental Health in Permanent Supportive Housing
Qualitative and mixed-methods scholarship consistently demonstrates that experiences of homelessness are inextricably linked with mental health challenges that frequently persist beyond the point of housing placement. Individuals experiencing homelessness exhibit disproportionately elevated rates of mental illness, substance use disorders, and psychological distress, attributable to prolonged exposure to residential instability, social stigmatization, and inadequate access to health services [11,12]. While access to permanent or supportive housing can ameliorate stress and anxiety, qualitative evidence reveals that mental health recovery during housing transitions is neither immediate nor uniform in its trajectory. Participants frequently articulate ongoing challenges associated with trauma, mistrust of institutional service systems, and insufficient relational or social support networks, which may compromise housing stability despite successful placement [13-15]. Qualitative narratives further illuminate how difficulties navigating housing bureaucracies, delays in service coordination, and constrained autonomy during transitional periods engender feelings of frustration, diminished agency, and emotional distress [16]. Collectively, this body of literature underscores the imperative of examining mental health not merely as a clinical outcome, but as a lived, experiential dimension of housing transitions.
Social Well-Being, Community, and Identity Post-Housing
Qualitative scholarship positions social well-being as a pivotal dimension of the transition from homelessness to permanent supportive housing, mediated by experiences of community integration, belonging, and dignity. Empirical studies consistently document that individuals residing in supportive housing frequently continue to experience social isolation and loneliness, which may attenuate well-being despite successful housing placement, whereas meaningful social connections and peer relationships function as protective factors that enhance psychological health and residential stability [17-19]. Community integration is characteristically described as a gradual and non-linear process, with residents reporting ameliorated feelings of belonging and inclusion relative to periods of homelessness, yet persistent challenges in negotiating social roles and community participation [9,20]. Qualitative narratives further foreground dignity, autonomy, and respect as constitutive elements of social well-being within supportive housing contexts, with residents ascribing value to environments that facilitate choice, self-determination, and affirmation of individual identity [6,21]. Collectively, this body of scholarship conceptualizes social well-being as a lived, relational phenomenon shaped by housing environments, service delivery practices, and community contexts, thereby reinforcing the imperative for qualitative synthesis that centers residents' experiential knowledge in theorizing housing transitions.
Barriers to Housing Stability
Although both models show considerable potential, many substantial obstacles can undermine sustained housing stability. These challenges encompass unsafe and insecure living conditions, unreliable case management services, restricted opportunities for individual development, and encounters with discriminatory or stigmatizing attitudes from service staff [2]. Harmful treatment by property owners and the assignment of residents to under-funded communities further contribute to residential instability [2]. Economic constraints, including elevated housing costs and the difficulty of aligning limited incomes with rising rental prices, represent fundamental structural impediments [1]. Additionally, individuals recently housed may encounter difficulties with social isolation and adjustment to unfamiliar living circumstances, therefore influencing their personal identity formation [4].
Identification of Gaps
Although current research demonstrates the effectiveness of Housing First and supportive housing programs, a significant gap persists in comprehensively understanding the personal experiences of people moving from homelessness to stable housing. Quantitative studies typically emphasize measurable outcomes such as housing maintenance and decreased hospital admissions, while qualitative assessments reveal intricate, personal impacts including enhanced feelings of safety, dignity, and identity reformation [4]. Nevertheless, even these qualitative findings sometimes offer only surface-level understanding [4].
A substantial knowledge gap exists in consolidating these lived experiences to comprehensively understand how people navigate the significant personal and social transformations that accompany rehousing [4]. Research has recognized these limitations including inadequate participant numbers and challenges in applying findings broadly, especially regarding the understanding of sustained effects on health outcomes [3]. The initial "honeymoon period" frequently observed following housing placement typically transitions into new difficulties such as social isolation, economic concerns, and challenges maintaining residential stability, all indicating that early positive responses do not reflect the complete, dynamic path of recovery [4].
Additionally, although service frameworks promote client autonomy and personalized assistance [7], the practical availability of these options can be limited by budgetary and institutional constraints, therefore creating potential disconnects between policy intentions and actual experiences [7]. For example, despite requiring ongoing support, resource scarcity can result in a "transition out" pattern where individuals showing progress are relocated to environments with reduced assistance [7]. Comprehending the complexities of these experiences, including trust development and community integration processes, from the viewpoint of participants themselves, is vital for improving interventions and policies [8]. Consequently, integrating lived experiences is essential to reveal the subtle yet significant effects of housing on personal recovery, identity formation, and social engagement, extending beyond measurable outcomes to examine the deep internal transformations and persistent challenges encountered by people with histories of homelessness.
Recent qualitative and mixed-methods studies published after 2022 extend Housing First and permanent supportive housing scholarship by foregrounding the lived experiences of adults transitioning from homelessness, with particular attention to mental health, social well-being, disability, and intersecting identities [20,21]. This emerging body of work demonstrates that while stable housing frequently contributes to enhanced emotional security and reduced psychological distress, mental health recovery and social integration remain ongoing, relational processes shaped by trauma histories, service environments, and access to supportive relationships [22,23]. Studies further reveal that individuals with disabilities or chronic mental health conditions often encounter challenges related to autonomy, accessibility, and continuity of care within supportive housing settings, underscoring the limitations of housing access as a standalone intervention [9,24]. Intersectional analyses indicate that race, gender, and aging shape experiences of belonging, dignity, and community integration, with marginalized groups reporting distinctive barriers rooted in structural inequities and stigma [25]. Across studies, social well-being emerges not as an automatic consequence of housing placement, but as a lived experience cultivated through safety, choice, meaningful relationships, and respectful engagement within housing environments [20,21]. These intersectional perspectives underscore that housing transitions are not experienced uniformly and reinforce the imperative for qualitative synthesis approaches that center lived experience across diverse social positionalities.
Method
Qualitative Interpretive Meta-Synthesis (QIMS) is a method that synthesizes outcomes from various qualitative research studies to create detailed, complex insights into specified phenomena [26]. While meta-synthesis approaches have been broadly utilized in areas like nursing and social work, Aguirre and Bolton [26] refined the QIMS framework particularly for social work policy, practice, and research purposes. QIMS determines the built-in sample size restrictions of individual qualitative investigations by pooling participants from diverse studies. This technique produces an aggregate sample that approximates the size characteristically seen in quantitative research approaches. The QIMS process consists of four connected components: (1) instrumentation, (2) literature sampling, (3) data extraction, and (4) consolidation of findings into harmonized comprehension of the research subject.
This study employed a modified Qualitative Interpretive Meta- Synthesis (QIMS) adapted for a graduate-level social work research methods project conducted under faculty supervision. While QIMS traditionally involves synthesis by experienced research teams, this project was intentionally structured as a pedagogical, teambased interpretive synthesis that preserved the core epistemological foundations of QIMS by centering meaning-making, participant voice, and interpretive rigor, while accommodating an instructional research context. Faculty involvement functioned as methodological guidance and quality assurance rather than direct data coding or interpretation. This ensured that analytic decisions remained studentled while adhering to established qualitative standards.
Several methodological adaptations were implemented. First, rather than presenting individual reflexivity statements for each researcher, as is typical in smaller QIMS teams, this project employed a combined collective credibility statement due to the size of the research team. This approach was selected to transparently represent the team’s shared academic training, professional backgrounds, lived experiences, and social locations while maintaining methodological clarity and feasibility within a large, course-based research context. Second, data extraction and analysis focused exclusively on verbatim participant quotations reported in the Results sections of included qualitative studies, rather than coding entire manuscripts or author interpretations. Line-by-line coding was applied to these extracted quotations to generate concise descriptive codes (2–5 words), which were then iteratively compared and grouped through a structured, multi-week synthesis process. This process emphasized independent initial coding, peer comparison, consensus-building discussions, and faculty-guided refinement of themes, rather than rapid team synthesis. Additionally, the research team operated within the same analytic roles (e.g., coding, synthesis, writing, credibility development) at various stages of the process to reflect the collaborative structure of the course-based research design. Together, these modifications maintained the interpretive depth of QIMS while ensuring analytic clarity, transparency, and methodological rigor within a structured educational research environment.
Instrumentation
Within qualitative research, investigators act as the main tools for data collection and analysis, thus making it essential to address potential biases and establish methodological rigor. This research was executed by a team of 12 Master of Social Work (MSW) graduate students working under the direction of the lead author, who concurrently fulfilled the role of course instructor, along with guidance from community experts and institutional collaborators. Because of the project's time constraints, the work was finished within a 15-week semester. The lead author served as project director and key point of contact, customizing the QIMS methodology for collaborative team implementation. Moreover, the lead author designed the research approach, educated the team in QIMS techniques modified for rapid group analysis, and ensured consistent supervision and coordination across the complete research timeline.
Since this research utilized exclusively secondary data from existing qualitative peer-reviewed studies, no additional participants were enrolled, therefore eliminating the need for Institutional Review Board approval. We acknowledge the potential dual role conflict arising from the instructor functioning as both academic faculty (responsible for student assessment) and research collaborator. To mitigate this possible bias, we implemented several protective measures including well-defined team responsibilities, collaborative decision-making processes, continuous reflexive conversations, and cross-team peer evaluation systems. These strategies promoted transparency, equity, and methodological excellence throughout both educational and investigative activities.
The lead author has extensive experience with the QIMS methodology, having published numerous studies using this approach [27-33], and consequently modified the framework to achieve both thorough analysis and effective student learning within a 15-week semester timeframe. Through this adapted QIMS version, the team worked collaboratively to maintain transparency and establish credibility. Students took on specified and rotating responsibilities including literature searches, article evaluation, quotation extraction, data coding, thematic analysis, and manuscript development. These tasks were reinforced through weekly team meetings, peer assessment processes, and instructor supervision to guarantee methodological rigor and procedural transparency.
Instead of including individual credibility statements for each researcher as customary in QIMS research projects, this modified approach highlights the team's collective credentials to emphasize the interdisciplinary and experiential diversity of the research group. The team comprised Master of Social Work students from the University of Arkansas at Little Rock, each contributing distinct educational, professional, and personal backgrounds. Their shared expertise encompassed housing policy, eviction prevention, forensic psychology, mental health services, child welfare, addiction recovery, grassroots interventions, and legal advocacy. Multiple team members possessed direct experience serving homeless populations through clinical practice, advocacy work, peer support roles, or employment in shelter facilities and housing programs. Additional members brought lived experiences of housing insecurity, economic hardship, and institutional discrimination, offering perspectives frequently absent from scholarly research. This breadth of knowledge and social positioning enhanced ongoing reflexivity as participants engaged in critical self-examination, mutual accountability, and liberationfocused research methods to ensure interpretations centered participant voices over researcher assumptions. The integration of academic training, experiential wisdom, and professional practice grounded the synthesis in both scholarly excellence and practical application, reflecting social work's fundamental commitments to dignity, justice, and human rights.
Sampling and Study Selection
A targeted sampling methodology was utilized to locate qualitative research investigating the personal experiences of people moving from homelessness to stable housing, specifically focusing on how individuals manage difficulties concerning dignity, autonomy, security, and community assistance during the transition period. Although some included studies contained staff or administrator perspectives, only data derived from participants with lived experience of homelessness were interpreted as lived experience findings. Staff and managerial perspectives were used solely to contextualize structural conditions and service environments. This sampling strategy was chosen to include the richness and intricacy of lived experiences and knowledge that quantitative research might not sufficiently capture [34].
Search Strategy
Thorough literature searches were executed between January and April 2025 by utilizing eight scholarly databases: Google Scholar, Web of Science, Academic Search Ultimate, Communication and Mass Media Complete, Education Research Complete, ERIC, Sociology Database, and PsycINFO. These resources were selected to guarantee extensive coverage across social work, sociology, psychology, public health, and policy analysis fields. Boolean search strategies were formulated to locate qualitative studies addressing the project's primary research objectives. Search methodologies integrated broad theoretical concepts with precise program-specific terminology to ensure complete retrieval of applicable scholarship. The search design consisted of five principal thematic groupings:
Permanent Housing Concepts: supportive housing, transitional housing, long-term housing solutions, Housing First model, permanent supportive housing, scattered-site housing
Systemic and Structural Factors: structural barriers, policy barriers, housing discrimination, affordable housing crisis, institutional barriers, systemic inequities
Population Terms: unhoused populations, people experiencing homelessness, housing-insecure individuals, formerly homeless individuals, chronically homeless
Housing Access and Services: housing accessibility, rental assistance, eviction prevention, low-income housing programs, housing vouchers, case management
Qualitative Methodology Indicators: lived experiences, personal narratives, focus groups, in-depth interviews, phenomenology, grounded theory, case studies, ethnography, participatory research
An example Boolean search string employed was: ("permanent housing" OR "supportive housing" OR "Housing First") AND ("lived experience*" OR "personal narrative*" OR "qualitative") AND ("homeless*" OR "unhoused" OR "housing insecur*") AND ("transition*" OR "housing access" OR "dignity" OR "independence").
Studies were eligible for inclusion if they: (1) employed qualitative or mixed-methods research designs with substantial qualitative components; (2) focused on adults (18+ years) with lived experience of homelessness; (3) examined transitions to permanent housing arrangements; (4) were published in peer-reviewed journals; and (5) were available in English. Studies were excluded if they: (1) employed exclusively quantitative methodologies; (2) focused solely on emergency shelter experiences without addressing permanent housing transitions; (3) examined only service provider or policymaker perspectives without including participant voices; (4) were conference abstracts, dissertations, or non-peer reviewed publications; or (5) did not explicitly address the experiential dimensions of housing transitions. This sampling strategy yielded nine peer reviewed studies that represent the voices of 358 individuals, which underwent systematic screening and quality assessment as detailed in the subsequent methodology section.
Selection Process
Literature searches performed across eight databases between January and April 2025 generated 8,550 potentially relevant records. After removing duplicates and conducting preliminary title screening, 6,200 articles proceeded to abstract evaluation. Abstract-level review excluded 5,800 studies that did not satisfy inclusion criteria, mainly because they employed quantitative methods or lacked adequate focus on permanent housing interventions. 400 studies received full-text assessment, with 391 ultimately eliminated for various factors including lack of qualitative data, governmental publications, or insufficient emphasis on housing transition experiences. The resulting sample included nine qualitative peer-reviewed studies that represented the viewpoints of 358 individuals with experiences of homelessness and recent placement in permanent supportive housing programs. The selection process is depicted in the study's flow diagram (Figure 1), with comprehensive details of each study provided in Table 1.
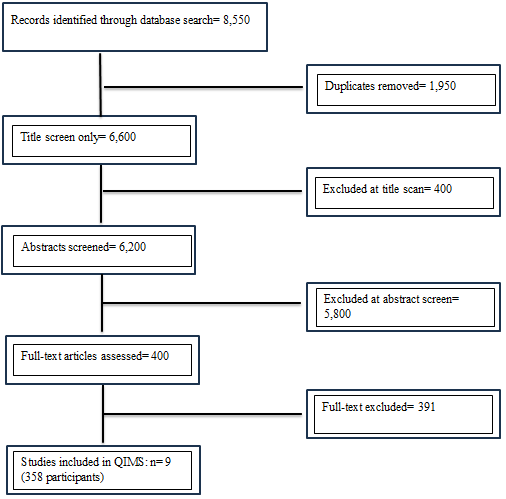
Fig. 1 Quorum Chart
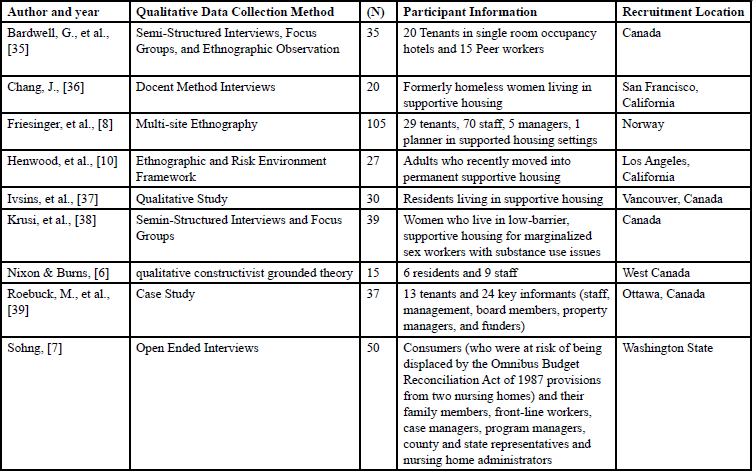
Table 1: Demographics of studies included in the qualitative interpretive meta-synthesis
Data for this synthesis consisted of verbatim participant quotes reported in the Results sections of the included qualitative studies. These quotes were extracted and subjected to line-by-line coding to identify interpretive patterns across studies. Original participant themes from the nine final studies were organized into a shared data matrix (see Table 2). The research team performed systematic line-by-line examination and created concise descriptive codes (2–5 words) to represent the fundamental aspects of participant experiences. Codes were analyzed across studies, organized into clusters, and integrated into overarching interpretive patterns. This recursive methodology illuminated points of convergence and variation across accounts and generated six principal themes: (1) Preserving Dignity and Personhood While Unhoused, (2) Structural Barriers to Independence, (3) Community as a Double-Edged Sword, (4) Navigating Unsafe or High-Risk Environments, (5) Distrust Rooted in Lived Experience, and (6) Experiences of Stability and Predictability in Permanent HousingFlexible Housing Models as a Pathway to Stability. These themes, presented in the Results section, illuminate how individuals navigate the transition from homelessness to permanent housing and the factors that influence their dignity, independence, safety, trust, and overall stability.
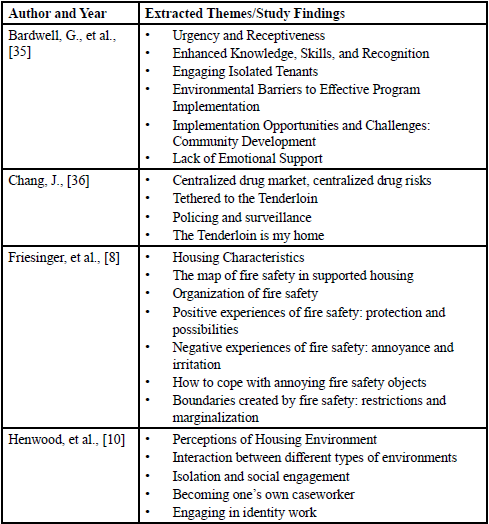
Table 2: Themes extracted from original studies
Analysis and Triangulation
Constant comparative analysis served as the method for understanding participants' experiential meanings across multiple contexts and settings. Several forms of triangulation were embedded within the analytical framework: (a) data triangulation was accomplished through combining insights from various qualitative investigations; (b) investigator triangulation was sustained through joint coding efforts, peer assessment, and team-based theme generation; and (c) methodological triangulation was reinforced by encompassing different qualitative research paradigms found in the selected studies (encompassing phenomenology, grounded theory, and narrative approaches). Continuous reflexive record-keeping and regular team meetings were maintained throughout the study to foster transparency and methodological integrity. This analytical strategy uncovered six core themes that collectively capture how individuals manage the transition from homelessness to stable housing and the variables that shape their experiences of dignity, autonomy, security, trust, and general well-being. The subsequent results describe each theme using representative participant statements and analytical discussion.
Results
In this synthesis, mental health is reflected through participants' shared experiences of psychological safety, trust, emotional regulation, and recovery, while social well-being is reflected through experiences of autonomy, dignity, community connection, and belonging. Themes are interpreted within these conceptual domains to facilitate cross-study synthesis across diverse contexts and temporal periods. Findings presented below derive from participant narratives reflecting lived experiences of homelessness and transition to permanent housing; references to staff or system-level perspectives are incorporated only where necessary to contextualize structural conditions shaping these experiences.
Theme 1: Preserving Dignity and Personhood While Unhoused
This theme revealed how people experiencing homelessness work to maintain their identity, dignity, and sense of humanity amid extremely challenging circumstances. Homelessness frequently involves losing not only physical housing but also personal autonomy, privacy, and social standing. Throughout the studies, participants articulated attempts to affirm their worth, safeguard their self-concept, and retain aspects of their identity despite facing stigma and social exclusion. One participant challenged the assumption that substance use defined their character, stating: “It affects your self-esteem... the first time you go outside the building [for drugs], you guarantee Tenant Services [staff] know... Just because I smoke some dope, that don’t make me scandalous, that don’t mean that I’m a thief. That means I’ve got a drug habit.” [36]
This resistance highlights how participants protected their dignity by insisting on respectful treatment, even while addressing substance use challenges. Older residents voiced frustration about being disregarded despite their lifetime contributions: "We've worked all our damn lives and found ourselves on the street and go 'What the hell! Is this it?'... I think that we deserve a little bit more attention than your youngster on the street" [6]. Collectively, these testimonies demonstrate the strength required to maintain dignity and identity while experiencing homelessness. Participants shared stories of resisting stigmatization, seeking normalcy, and navigating the emotional complexity of housing transitions. Their perspectives emphasize that homelessness extends beyond lacking physical shelter to encompass a fundamental threat to identity and human worth. These accounts advocate for policies and interventions that recognize individual humanity and ensure people are acknowledged, valued, and treated with dignity, even during periods of severe adversity.
Theme 2: Structural Barriers to Independence
This theme highlights how institutional obstacles compromise autonomy for people entering permanent housing. While housing programs typically aim to enhance safety and stability, participants reported that restrictive regulations, inflexible qualification requirements, economic pressures, and physically inaccessible environments frequently created dependency instead of promoting self-sufficiency. Genuine housing stability necessitates three interconnected components: suitable housing, sufficient income, and appropriate support. However participants consistently highlighted how system failures made achieving this equilibrium challenging. For some, design and policy decisions prioritized safety and liability over autonomy. One planner noted, “The small houses are designed to fulfill the common housing standard and are constructed as fire barriers each to prevent a fire from spreading” [8]. While meeting regulatory codes, such design choices often failed to account for the lived experiences or preferences of residents.
System-level barriers further constrained residents’ choices. As one individual explained, “I’m on a waiting list for Shelter Plus Care... I would like to move out of this building. I have had a lot of bad experiences here” [36]. Criminal records, county restrictions, and limited availability of units often left residents trapped in unsafe or unsatisfactory placements despite their motivation to move forward. For residents with disabilities, inaccessible infrastructure presented additional challenges. One participant recalled, “[The elevator] was out for eight days... It took me an hour to go down the stairs, one at a time, on my butt... There are no facilities for disabled people on this floor. On any of them” [36].
Collectively, these personal experiences demonstrate that obstacles to independence stem from institutional deficiencies rather than personal inadequacies. Inaccessible facilities, exclusionary eligibility requirements, economic hardship, and inflexible program structures combine to undermine autonomy. Independence, therefore, cannot be attained through individual determination alone; it requires structural reforms that ensure housing programs reflect the actual circumstances and varied needs of their participants.
Theme 3: Community as a Double-Edged Sword
This theme emphasizes the complex role of community in the experiences of people moving into permanent housing. Although many participants desired connection and support, their stories showed that community relationships could serve as both sources of recovery and potential harm. Social bonds frequently offered companionship, stability, or recovery pathways, but they could also maintain stigmatization, create exposure to violence, or encourage destructive behaviors.
Participants described forming bonds within communities structured by substance use or street economies. One resident reflected, “In front of [my apartment], most are crack dealers… I think everybody’s just out trying to make their little money” [36]. These connections, while offering a form of solidarity, also normalized unsafe environments. Others emphasized the difficulty of maintaining meaningful connections. Loneliness was a recurring concern, with some residents expressing a desire to return to institutional or communal settings where companionship had been more accessible. One resident explained, “I am so lonely… I want to go back to the nursing home. There, I have a lot of friends and staff” [7].
The safety of housing communities was also questioned. One participant recounted an assault: “I used to come downstairs to the TV lounge… and then I got stabbed in the lobby… I’ve been pretty badly victimized in there. That’s why I stay in my room. Most of the day. All day. Twenty-four hours, almost” [36]. These experiences illustrate how programs intended to provide safety sometimes reproduced environments marked by violence, fear, and isolation. Failures in supportive services left participants vulnerable to displacement and long-term harm, undermining the intended stability of permanent housing programs. Collectively, these accounts reveal the contradictory nature of community as both a stabilizing force and a potential threat. For numerous participants, housing provided an opportunity to rebuild relationships and restore social connections, but the challenges of dangerous neighborhoods, isolation, and institutional failures often undermined this potential. Community, therefore, functioned as a complex phenomenon possessing the power to support healing and strength, while simultaneously holding the capacity to maintain harm and disconnection.
Theme 4: Navigating Unsafe or High-Risk Environments
This theme discloses how people experiencing homelessness or entering permanent housing frequently face environments that feel dangerous, precarious, and harmful to both physical and psychological health. Participants reported experiencing vulnerability, fear, and despair when confronted with violence, substance abuse, racial prejudice, and institutional abandonment. These testimonies show that housing provision alone cannot ensure safety when surrounding community and organizational conditions continue to pose risks.
Several participants spoke about the prevalence of substance use and crime in their communities. One resident explained, “Well because sometimes a lot of people are just about the dope and you know they just rob you” [37]. Another observed that “The only time [the drug dealers] run and hide is when the police come… and then they come back” [36]. Such accounts suggest that high-risk behaviors and weak enforcement structures can normalize environments where safety feels out of reach. The consequences of this instability were reflected in harm reduction efforts, with one tenant organizer noting, “I responded to six overdoses prior to the program starting, and when I was responding then it was like ‘holy shit, who’s got Narcan?’” [35] In other cases, participants described being hypervigilant toward police presence. One sex worker explained, “I don’t like to be anywhere secluded and dark either, it’s too scary”[38]. These narratives demonstrate the fine line between police as a source of safety and as a source of surveillance and fear.
Collectively, these results demonstrate that dangerous or risky environments compromise the potential of permanent housing. Criminal activity, substance abuse, and unreliable law enforcement all create conditions where people feel insecure even after obtaining housing. Safety, therefore, cannot be achieved through accommodation alone; it requires comprehensive interventions that ensure housing placements avoid locations that continue cycles of harm, discrimination, and anxiety.
Theme 5: Distrust Rooted in Lived Experience
This theme tells the profound skepticism many residents held toward case managers, service staff, and institutional systems. Across studies, trust emerged not as an immediate outcome of housing placement, but as a relational process shaped by prior experiences of instability, surveillance, and harm. Although permanent housing aimed to deliver stability and assistance, participants often recounted experiences of neglected needs, privacy violations, and frequent staff changes that made them feel insecure, abandoned, and helpless. Both residents and providers recognized that establishing trust demands time, reliability, and reciprocal respect. All qualities which are frequently compromised by structural obstacles and funding limitations.
One resident explained, “No, I don’t feel safe living here. We don’t even answer our door anymore because we know the nurses have keys… we’re not going to answer the door” [37]. For this participant, a lack of privacy translated directly into a lack of trust, underscoring the importance of autonomy and safety in housing environments. Similarly, a healthcare worker observed, “A lot of these folks… have been let down so many times… I need to spend quite a bit of quality time, just even visiting with them” [6]. Both perspectives highlight that trust cannot be assumed; it must be actively cultivated through respectful engagement.
Other residents described frustration with the absence of meaningful support. One participant reported that her caseworkers “don’t do shit,” while another stated he felt forced to “become my own caseworker” [10]. These narratives suggest that when support is inconsistent or absent, residents not only lose faith in their providers but also develop resentment toward the broader systems designed to assist them.
At the same time, examples of respect were noted. One resident acknowledged, “We don’t see eye to eye quite a few times but at least they [staff] do respect, you know… I would put that as probably number one priority” [6]. This comment suggests that mutual respect can lay the foundation for stronger relationships, even amid disagreements. Caseworkers themselves echoed the challenges of building rapport in a system marked by turnover and short-term staffing. Combined, these narratives demonstrate that distrust originates not simply in individual incidents but in organizational systems that diminish agency, reduce options, and compromise service continuity. For trust to flourish, residents and providers must build connections founded on respect, steadiness, and balanced relationships. Absent institutional reforms that preserve independence and ensure stable, trustworthy support, distrust will persist as a central element of numerous housing experiences.
Theme 6: Experiences of Stability and Predictability in Permanent Housing Flexible Housing Models as a Pathway to Stability
This theme reflects participants’ descriptions of stability, predictability, and perceived responsiveness within permanent housing environments, which were associated with feelings of safety, respect, and emotional well-being during the transition from homelessness. This theme demonstrates how adaptable and personalized housing programs promote stability, respect, and healing for individuals moving from homelessness. Participants stressed that housing approaches offering tailored support, independence, and responsive case coordination produced more positive results. Conversely, inflexible or one-size-fits-all programs were characterized as poorly matched to the diverse and complex requirements of residents. The health implications of flexible housing were emphasized. One participant noted that residents described how permanent housing provided a safe environment to focus on recovery: “I would not have the quality of life I have had I not this lovely roof over my head” [39]; “Having my own place provided me a space to work on my recovery. I am clean and sober since July 2010” [39]. These accounts illustrate how housing can empower individuals to pursue sobriety, health, and long-term goals. Codes informing this theme reflected participants’ experiences of consistent housing access, relief from instability, and perceived responsiveness to individual needs rather than formal program-level customization or policy adaptation.
Together, these testimonies demonstrate that individualized housing programs transcend basic shelter provision to foster conditions for human thriving. Initiatives that prioritize autonomy, customize interventions, and deliver wraparound supports advance recovery, health outcomes, and personal dignity. Meanwhile, restrictive frameworks that establish barriers or disregard ongoing care coordination risk reinforcing destabilizing patterns. Adaptive housing approaches, consequently, emerge as fundamental to securing longterm stability and human development.
Discussion
This qualitative interpretive meta-synthesis aimed to explore the lived experiences of people moving from homelessness to permanent housing, focusing specifically on how dignity, independence, safety, community, and trust influence this transition. Drawing from nine studies representing 358 participants' voices, the analysis identified six interrelated themes: maintaining dignity and personhood, institutional obstacles to independence, community as both beneficial and harmful, managing dangerous environments, distrust based on personal experience, and adaptive housing models as routes to stability. Combined, these results demonstrate that permanent housing functions not merely as a physical intervention but as a social and psychological one, carrying significant consequences for mental health and overall well-being. Even following housing placement, restrictive program policies, physically inaccessible facilities, and hazardous environments frequently perpetuated dependency rather than fostering stability. These results indicate that housing interventions must address not only unit provision but also the broader environmental and systemic factors influencing residents' daily experiences.
Simultaneously, community functioned as both a protective and risk factor. While certain residents established meaningful connections and support networks, others experienced isolation, exploitation, or violence. Trust in staff and organizations remained questionable, often compromised by confidentiality breaches, neglect, or personnel instability. However, when programs incorporated flexibility, individualization, and relationship-centered approaches, participants characterized housing as transformative, providing necessary stability for pursuing recovery, enhancing health outcomes, and regaining self-determination.
These findings collectively underscore that permanent housing constitutes a multidimensional intervention that requires comprehensive assessment beyond retention metrics. Effectiveness depends on affirming resident dignity, dismantling structural barriers, ensuring environmental safety, and cultivating trust through consistent, adaptable support systems. For social work practitioners and policymakers, this necessitates resident-centered, equity-focused approaches that recognize housing as both a fundamental human right and a critical foundation for sustained well-being.
Implications for Social Work and Policy
These results have significant implications for social work practice, housing policy, and mental health service provision. Social workers hold strategic positions to champion trauma-informed, adaptable, and culturally sensitive housing approaches that emphasize selfdetermination and human worth. Policy changes must target institutional inequalities, including restrictive qualification criteria, dangerous housing placements, and inadequate comprehensive services that undermine stability and worsen psychological distress. Funding for Housing First and comparable accessible models could produce not only better housing outcomes but also decreased medical expenses and improved quality of life.
Limitations and Future Research
This synthesis faces constraints due to the limited scope of existing qualitative research, which primarily focused on urban U.S. settings and frequently excluded rural communities and racial minority populations. The interpretive nature of QIMS methodology also creates possibilities for researcher bias, although cross-study triangulation helps reduce this concern. Future stuides should emphasize longitudinal qualitative designs that track residents across time, examine racial and cultural inequities in housing experiences, and incorporate perspectives from families and children experiencing these transitions.
Conclusion
Permanent housing represents more than shelter. It is a crucible for dignity, trust, safety, and recovery. Yet for many, systemic barriers, unsafe environments, and fractured relationships compromise the promise of stability. The voices of 358 participants highlight that housing interventions must go beyond providing units to creating conditions where individuals can thrive. Embedding flexibility, autonomy, and respect into housing programs is not only consistent with social work ethics but essential for advancing mental health and social well-being.
Competing Interests:
The authors declare that they have no competing interests.
References
Distasio, J., McCullough, S., Havens, M., & St. Aubin, Z. (2014). Holding on!: Supporting successful tenancies for the hard to house. Institute of Urban Studies, University of Winnipeg. View
Milburn, N., Edwards, E., Obermark, D., & Rountree, J. (2021,October). Inequity in the permanent supportive housing system in Los Angeles. California Policy Lab, University of California. View
Pearson, C., Montgomery, A. E., & Locke, G. (2009). Housing stability among homeless individuals with serious mental illness participating in housing first programs. Journal of Community psychology, 37(3), 404-417. View
Rhenter, P., Moreau, D., Laval, C., Mantovani, J., Albisson, A., Suderie, G., French Housing First Study Group, Boucekine, M., Tinland, A., Loubiere, S., Greacen, T., Auquier, P., & Girard, V. (2018). Bread and shoulders: reversing the downward spiral, a qualitative analyses of the effects of a housing first-type program in France. International journal of environmental research and public health, 15(3), 520. View
Cusack, M., & Montgomery, A. E. (2017). Examining the bidirectional association between veteran homelessness and incarceration within the context of permanent supportive housing. Psychological services, 14(2), 250. View
Nixon, L. L., & Burns, V. F. (2022). Exploring harm reduction in supportive housing for formerly homeless older adults. Canadian Geriatrics Journal, 25(3), 285. View
Sohng, S. S. L. (1996). Supported housing for the mentally ill elderly: Implementation and consumer choice. Community Mental Health Journal, 32(2), 135-148. View
Friesinger, J. G., Topor, A., Bøe, T. D., & Larsen, I. B. (2019). The ambiguous influences of fire safety on people with mental health problems in supported housing. Palgrave Communications, 5(1), 1-9. View
Aubry, T., Bloch, G., Brcic, V., Saad, A., Magwood, O., Abdalla, T., & Pottie, K. (2020). Effectiveness of permanent supportive housing and income assistance interventions for homeless individuals in high-income countries: A systematic review. The Lancet Public Health, 5(6), e342–e360. View
Henwood, B. F., Lahey, J., Harris, T., Rhoades, H., & Wenzel, S. L. (2018). Navigating Rish Environments in Permanent Supportive Housing for Formerly Homeless Adults. Qualitative Health Research, 28(13), 2011-2019.
Fazel, S., Geddes, J. R., & Kushel, M. (2014). The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. The Lancet, 384(9953), 1529–1540. View
Tsemberis, S., & Eisenberg, R. F. (2000). Pathways to housing: Supported housing for street-dwelling homeless individuals with psychiatric disabilities. Psychiatric Services, 51(4), 487– 493. View
Bhui, K., Shanahan, L., & Harding, G. (2006). Homelessness and mental illness: A literature review and a qualitative study of perceptions of the adequacy of care. International Journal of Social Psychiatry, 52(2), 152–165. View
Chuah, C., Honey, A., & Arblaster, K. (2022). “I’m institutionalised … there’s not much I can do”: Lived experience of housing-related delayed discharge. Australian Occupational Therapy Journal, 69(5), 574–584. View
Voisard, B., Whitley, R., Latimer, É., Looper, K. J., & Laliberté, V. (2021). Insights from homeless men about PRISM, an innovative shelter-based mental health service. PLOS ONE, 16(4), e0250341. View
Nguyen, J., Honey, A., Arblaster, K., & Heard, R. (2021). Housing-related delayed discharge from inpatient mental health units: Magnitude and contributors in a metropolitan mental health service. Australian Journal of Social Issues, 57(1), 144– 163. View
Courtin, É., & Knapp, M. (2015). Social isolation, loneliness and health in old age: A scoping review. Health & Social Care in the Community, 25(3), 799–812. View
Coyle, C. E., & Dugan, E. (2012). Social isolation, loneliness and health among older adults. Journal of Aging and Health, 24(8), 1346–1363. View
Fleury, M.-J., Grenier, G., Sabetti, J., Bertrand, K., Clément, M., & Brochu, S. (2021). Met and unmet needs of homeless individuals at different stages of housing reintegration: A mixedmethod investigation. PLOS ONE, 16(1), e0245088. View
Marshall, C., McKinley, C., Costantini, J., Murphy, S., Lysaght, R., & Hart, B. (2022). “The Big Island Model”: Resident experiences of a novel permanent supportive housing model for responding to rural homelessness. Health & Social Care in the Community, 30(6). View
Bianchi, E., Corrêa, M., Eichstaedt, J., & Billington, S. (2024). Nature, buildings, and humans: Residents’ perceptions of well-being in permanent supportive housing. Environment and Behavior, 56(7–8), 577–613. View
Milligan, T., Resing, K., Littman, D., Bender, K., & Coddington, L. (2024). “It’s home for now”: Sense of home among emerging adults in permanent supportive housing through the lens of ontological security theory. Emerging Adulthood, 12(6), 1086– 1098. View
Harris, T., Rhoades, H., Duan, L., & Wenzel, S. (2019). Mental health change in the transition to permanent supportive housing: The role of housing and social networks. Journal of Community Psychology, 47(8), 1834–1849. View
David, C., Nipperess, S., Wiesel, I., & Weiss, C. (2024). Experiences of people with disability living in permanent supportive housing in the context of the National Disability Insurance Scheme. Australian Journal of Social Issues, 60(4), 1011–1028. View
Rhoades, H., Hsu, H., Rice, E., Harris, T., Motte-Kerr, W., Winetrobe, H., … Wenzel, S. (2020). Social network change after moving into permanent supportive housing: Who stays and who goes? Network Science, 9(1), 18–34. View
Aguirre, R. T., & Bolton, K. M. (2013). Why do they do it? A qualitative interpretive meta-synthesis of crisis volunteers' motivations. Social Work Research, 37(4), 327-338. View
Burse, J., McElwee, T. M., Heldman, E., Campbell, H. B. (2024). Unveiling the Silent Struggle: Exploring Intimate Partner Violence among Older African American Women: A Qualitative Interpretive Meta-Synthesis (QIMS). Journal of Clinical Nursing Reports 3 (2), 01, 9. View
Barnett, T. M., McFarland, A., Miller, J. W., Lowe, V., & Hatcher, S. S. (2019). Physical and mental health experiences among African American college students. Social Work in Public Health, 34(2), 145-157. View
Watkins, J., Barnett, T. M., Collier-Tenison, S., & Blakey, J. (2019). Why don’t they listen to me: A Qualitative Interpretive Meta Synthesis of a child’s perception of their sexual abuse. Child and Adolescent Social Work, 36(1), 337-349. View
Patterson, Y. K., & Barnett, T. M. (2017). Experiences and Responses to Microaggressions on Historically White Campuses: A Qualitative Interpretive Meta-Synthesis. Journal of Sociology and Social Welfare, 44(1), 3-26. View
Barnett, T.M. , Bowers, P. H., & Bowers, A. (2016). Using a social justice lens to examine and understand the experiences of sexual minority women who struggle with obesity: Qualitative interpretive meta-synthesis (QIMS). International Journal of Public Health, 8(2), 121-136.
Barnett, T. M., & Praetorius, R. T. (2015). Knowledge is (not) power: Healthy eating and physical activity for African- American women. Social work in health care, 54(4), 365-382. View
Barnett, T.M., & Aguirre, R.T.P. (2013). A Qualitative Interpretive Meta-synthesis (QIMS) of African Americans and Obesity: Cultural acceptance and public opinion. Hawaii Journal of Medicine and Public Health, 72(8 Suppl 3): 23. View
Patton, M. (2015) Qualitative Research and Evaluation Methods. 4th Edition, Sage Publications, Thousand Oaks. View
Bardwell, G., Fleming, T., Collins, A. B., Boyd, J., & McNeil, R. (2019). Addressing intersecting housing and overdose crises in Vancouver, Canada: opportunities and challenges from a tenantled overdose response intervention in single room occupancy hotels. Journal of urban health, 96(1), 12-20. View
Chang, J. S. (2017). Health in the Tenderloin: A resident-guided study of substance use, treatment, and housing. Social Science & Medicine, 176, 166-174. View
Ivsins, A., MacKinnon, L., Bowles, J. M., Slaunwhite, A., & Bardwell, G. (2022). Overdose prevention and housing: a qualitative study examining drug use, overdose risk, and access to safer supply in permanent supportive housing in Vancouver, Canada. Journal of urban health, 99(5), 855-864. View
Krüsi, A., Chettiar, J., Ridgway, A., Abbott, J., Strathdee, S. A., & Shannon, K. (2012). Negotiating safety and sexual risk reduction with clients in unsanctioned safer indoor sex work environments: a qualitative study. American journal of public health, 102(6), 1154-1159. View
Roebuck, M., Aubry, T., Agha, A., Manoni-Millar, S., Medd, L., & Sylvestre, J. (2023). A study of the creation of affordable housing for Housing First tenants through the purchase of condominiums. Housing Studies, 38(4), 661-681. View