
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 1 (2020), Article ID: JRPR-104
https://doi.org/10.33790/jrpr1100104Mini Review
An Overview of Lymphedema, Interventions, Functional Limitations, and the Disability Framework: Advocacy for Those Who Suffer from Lymphedema!
Cleve Carter III, PT, DPT, MEd, CSCS, CLT, C/NDT, Veronica Jackson*, PT, DPT, WCC, ACCE/DCCE & Dothal Edwards Rh.D., CRC, CLCP
Department of Physical Therapy, Alabama State University, 915 South Jackson Street, Montgomery, United States.
Corresponding Author Details: Veronica Jackson, PT, DPT, WCC, ACCE/DCCE, Associate Professor, Department of Physical Therapy, Alabama State University, 915 South Jackson St. Montgomery, United States. E-mail: vjackson@alasu.edu
Received date: 16th March, 2020
Accepted date: 07th April, 2020
Published date: 10th April, 2020
Citation: Carter, C., Jackson, V., & Edwards, D. (2020). An Overview of Lymphedema, Interventions, Functional Limitations, and the Disability Framework: Advocacy for Those Who Suffer from Lymphedema!. J Rehab Pract Res 1(1):104.
Copyright: ©2020, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Lymphedema is swelling of the arms or legs, and sometimes the face, which occurs when vessels in your lymphatic system are blocked, preventing the draining of lymph fluid. Lymphedema is usually caused by a condition or procedure that damages the lymphatic system, such as surgery on lymph nodes, cancer, radiation treatment for cancer, or repeated infections, including parasitic infections. Removal of lymph nodes from the underarm area following breast cancer is one of the most common causes. (Another type, primary lymphedema, is quite rare and is an inherited condition that is caused by the abnormal development of lymph vessels.) The Social Security Administration (SSA) published a listing of medical impairments that qualify for disability benefits if specified criteria are met. Even though lymphedema is not one of the listed impairments, there are ways you may be able to qualify for disability for lymphedema. Understanding what lymphedema is and some of its impairments and functional limitations will assist those who work with this population in providing information related to disability.
Keywords: Lymphedema, Disability, Exercise, Work
Introduction
The Social Security Administration (SSA) published a listing of medical impairments that qualify for disability benefits if specified criteria are met. Even though lymphedema is not one of the listed impairments, there are ways you may be able to qualify for disability for lymphedema. Understanding what lymphedema is and some of its impairments and functional limitations will assist those who work with this population in providing information related to disability [1].
Cathy Bates, actor and ovarian and breast cancer survivor, is the National Speaker for the Center for Disease Control and Prevention, Lymphatic Education and Research Network. In an online presentation, Ms. Bates talks about lymphedema as a “souvenir” of cancer. She describes lymphedema as a chronic, debilitating, and sometimes permanent swelling that can affect activities of daily living.
More Americans have lymphedema and lymphatic diseases than AIDS, Parkinson’s disease, multiple sclerosis, muscular dystrophy and Alzheimer’s disease combined. Up to 10 million Americans and hundreds of millions worldwide suffer from lymphedema. It will occur in up to 50% of breast cancer survivors, and 100% of those with head and neck cancer. Lymphedema looms for all cancer surgery survivors and that includes prostate, ovarian and melanoma [2].
Lymphedema can be due to hereditary or genetic causes. It can also be the result of infection or physical trauma such as surgery that harms the lymphatic system. After surgical interventions the removal of lymph nodes, radiation, and chemotherapy can potentially lead to damage of the lymphatic system. Up to 40% of breast can survivors and patients treated with other cancers will subsequently develop lymphedema.
The interruption of the flow of lymph fluid, can lead to a very serious condition called cellulitis, which is a bacterial skin infection which sometimes occurs in connection with lymphedema. If untreated, the infection can lead to sepsis if not treated with antibiotics, which is the body’s extreme response to infection that can become lifethreatening. Symptoms of cellulitis are redness, tenderness, pain and warmth to the touch. Cellulitis can also lead to chronic wound care management. Immediate medical attention should be given to this presentation of symptoms. Certified Lymphedema Specialist can provide a blueprint for the treatment of lymphedema.
Lymphedema
Lymphedema is a chronic inflammatory condition that develops as a result of lymphatic insufficiency. Lymphatic insufficiency occurs from a decrease in reabsorption or a decrease in transport capacity of the lymphatic system. It can be primary malformation of the lymph system or an acquired condition due to obstruction or damage to the system.
There are two types of lymphedema:
Secondary lymphedema is caused by another condition or disease that damages your lymph vessels or nodes. Secondary lymphedema may be caused by an infection in lymph nodes, parasites, cancer or radiation treatment, surgery, lymph node removal or injury.
Primary lymphedema is much less common. It’s a genetic problem that happens because your lymph nodes or vessels either aren't adequately developed or are missing altogether [3].
Symptoms
The most common symptom of lymphedema is swelling in one or both arms or legs. This swelling, which can extend into the fingers or toes, usually develops gradually over time.
At first, the swelling is soft and fluid. In time, it can become more dense and fibrous, and it may make your skin look grainy. You could also have pain, heaviness, or limited range of motion in the affected limb, which may make it hard to do other activities.
Patient complaints in the early stages of lymphedema include heaviness, tightness, aching, and sensory changes. Corresponding to these complaints, there may be loss of skin mobility. As the lymphedema progresses the skin becomes tighter and less mobile. The tightness of the skin and underlying tissue may also result in loss of range of motion and subsequently functional impairments. The difficulty to mobilize the skin over the back of the hand and foot is termed Stemmer’s sign.
The presence of any edema is a symptom of some underlying pathology that has to be identified in order to have an effective plan of care. Diagnosis is based upon the patient history, physical exam, and laboratory test to confirm certain metabolic disorders (eg, endocrine, cardiopulmonary, renal, or hepatic diseases) [3]. Some of the questions that can help with the differential diagnosis process include the following:
Benefits of Therapeutic Exercise
Decongestive or lymph drainage exercises are an essential component of Complete Decongestive Therapy (CDT) and should be integrated into the daily routine of those with primary or secondary lymphedema. Performance of decongestive or lymph drainage exercises pump, calf muscle pump, popliteal fossa pump, thigh pump, and inguinal pump are various general principles and mechanisms which assist the transport of lymphatic fluid throughout the body [4]. Skeletal muscle contraction increases interstitial pressure which is transferred to the walls of the veins and lymph vessels via connective tissue anchor filaments. The protein-rich fluid, waste products, and toxic substances are squeezed out when superficial veins are pressed against the skin during skeletal muscle contraction [4]. The vessels refill when the muscles are at rest. Thus, the alternating use of agonists and antagonists muscles and concentric and eccentric muscle contractions facilitate a decongestive effect whereas isometric exercises do not show any decongestive effect [4]. Thus, exercise encourages skeletal muscle contractions to utilize the various pump mechanisms mentioned earlier for lymphatic and venous drainage.
The importance of therapeutic exercise in the treatment and management of lymphedema has begun to emerge over the last 10- 20 years. There are several studies showing the benefits of various forms of therapeutic exercise in patients with lymphedema. A systemic review of the contemporary literature in regards to exercise in patients with lymphedema concluded that strong evidence is now available on the safety of resistance exercise performance without an increase in the risk of lymphedema or exacerbation of lymphedema for patients with breast cancer [5]. In addition, the authors concluded that it is not only safe for breast cancer survivors to perform exercise during their treatment but also incorporate exercise into their daily routine and living [5]. An exploratory, acute study conducted by Cormie et al. suggested that women with breast cancer-related lymphedema (BCRL) can perform moderate-to high-intensity upper body resistance exercise with both low and high loads without exacerbating their lymphedema [6].
These findings are clinically significant given the transparent potential for resistance exercise as a means to improve muscle strength and endurance and functional ability as well as assist in the long-term management of BCRL and preventing or decreasing disability [6].
In a pilot feasibility study, Ammitzboll et al. concluded that progressive strength training to prevent lymphedema in the first year after breast cancer was feasible and acceptable without detrimental adverse effects or events observed or measured from the initial examination and evaluation throughout the interventions [7]. Moreover,the supervised exercise program exhibited high compliance and adherence with significant gains in muscle strength among participants [7]. However, adherence along with muscle strength decreased during the home-based exercise duration, and one participant of six presented with lymphedema at the 50-week follow-up [7]. In their review article examining the effects that various exercise programs have on lymphedema, Bicego et al. concluded that exercise did not initiate nor exacerbate lymphedema even though more cases of new lymphedema were reported as adverse events in the exercise group in one of the studies reviewed [8]. Moreover, recent studies, which are limited in number and sample size, have provided novel evidence to propose that exercise may be safe and effective in the management of lymphedema [8].
Clinical Impression
As a licensed physical therapist and certified lymphedema therapist, I have evaluated and treated patients with primary and secondary lymphedema with the use of CDT. One of the major components of CDT is therapeutic exercise sometimes referred to as decongestive exercise or lymph drainage exercise. Typically, patients who are compliant and adhere to all of the components of CDT including therapeutic exercises experience positive outcomes with improvements in lymphatic circulation and functional capacity observed and measured. On the other hand, patients who are noncompliant and do not adhere to all of the components of CDT usually do not experience positive outcomes or significant improvements. In turn, lymphedema often results in aggravating functional limitations, disability, and psychosocial barriers for those who are affected. Most importantly, I have observed and measured significant improvements on functional assessments such as the Two-Minute Walk Test and the Chair Rise Test with those who were diligent with the performance of therapeutic exercises in conjunction with appropriate compression wear compliance. As a result, I have also seen a significant decrease in disability scores on scales such as the Lower Extremity Functional Scale, the Upper Extremity Functional Scale, and the Lymphedema Life Impact Scale version 2 with CDT’s interventions. In sum, objective data from functional assessments correlate with subjective data from questionnaires in either case of compliance or noncompliance with CDT.
Medical Model
From the medical model perspective, the disability is within the person, leaving the need for treatment to come from a medical professional. It follows, then, that the focus of treatment from the medical model perspective must be on either rehabilitating such difficulties that are caused by the disability or curing the person of that disabling condition in order to attain, or approach, normality [9]. Thus, the medical model is focused on the pathology of the disability, looking at the condition by set measures, and placing emphasis on medical treatment to discontinue or control the condition thereby returning a person to a normal state [10].
The role of influence between the ‘‘therapist’’ and the ‘‘patient’’ is significant. That is, the ultimate control exists with the medical professional. This model has its limitations in which it focuses on “normalcy according to societal roles and norms. Anything that deviates from this is viewed as abnormal, dysfunctional, or disabled. This view can negatively affect a person’s placement in society. The medical model focuses on the diagnosis and related limitation or functional limitation comparative to the societal norm [11].
Social Model
The model stresses societal and environmental barriers as the cause of disability. Equality is the focal point of this model, not looking for a cure of the disability so persons will conform to social norms. The social model reflects the civil/human rights movements, which was the driving force for the establishment of various social policies and legislative advancements. One such legislation is the Americans with Disabilities Act of 1990, which gave the right of persons with disabilities to receive reasonable accommodations that assist in functioning in the environment and prohibits discrimination. The social and environmental situation either promotes the disability or exaggerates a disability. The model looks at functional limitations as society’s inability to take these limitations as major contributors to the disability [12].
Biopsychocoial Model
The model uses aspects of the medical and social model of disability. It looks at the interactions of biological, psychological, and social factors in an interrelation approach. The model suggests that several variables, not simply the disability itself, determine the extent and type of function that persons with disabilities experience. Conceptualizing a disability in terms of functional capacity rather than as a medical diagnosis permits a greater understanding of the person’s personal experience of his or her disability [13].
Functional Limitation of Lymphedema
Functional limitation is the inability to conduct a task or a set of tasks, either physical or mental, due to a physical or emotional barrier (disability). A task can be a major life activity. A rehabilitation counselor understanding the functional limitations of Lymphoma must begin with the symptoms. Vocational implications of Lymphoma maybe understood based on the functional limitations. The following box explains this concept.
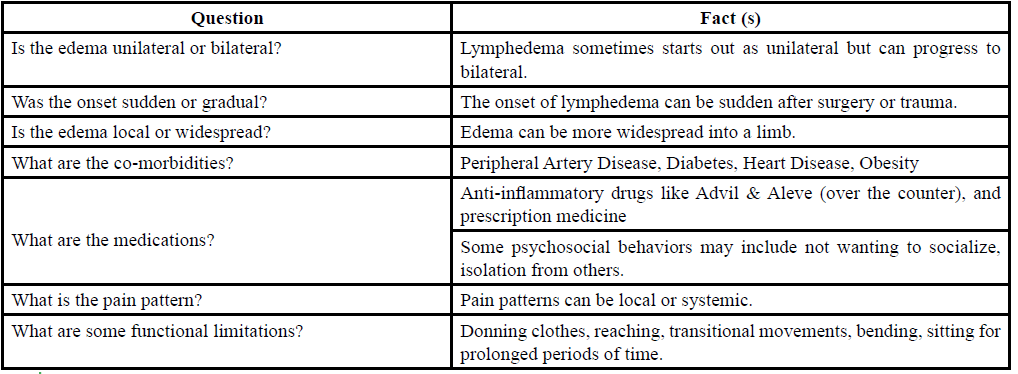
Box 1 Differential Diagnosis of Lymphedema Q & F
Workplace Accommodations Lymphedema
The U.S. Office of Personnel Management defines a reasonable accommodation as an accurate change to a position or work environment that allows a qualified person with a disability to perform the tasks of that position [14]. A qualified person with a disability is defined as a person with a disability who with or without reasonable accommodation, can perform the essential functions of the job [15]. An undue hardship can be suggested to not offer a workplace accommodation. According to the Americans with Disabilities Act (ADA), an undue hardship is when an action or accommodation requires significant difficulty or expense, which is determined on a case-by-case basis [15]. With the person who has Lymphedema (employee), the employer, and if applicable the vocational rehabilitation counselor must participate jointly to consider the accommodation process [16]. lists seven questions to consider in the accommodation process:
1. Was the employee actively involved in the accommodation process?
2. Does special equipment take advantage of the employee’s specialized abilities?
3. Was a simple, minimal cost solution found?
4. Was the “correct” issue solved?
5. Is the recommendation transferable and appropriate for other assignments with the company?
6. Has an accessible career path been provided for the employee?
7. Were all accommodations that the employee requested actually “reasonable?”
Examples of Reasonable Workplace Accommodations Lymphedema Pain
• Industrial
◊ Adjustable Workstations for Industrial Settings
◊ Anti-fatigue Matting
◊ Anti-vibration Gloves
◊ Anti-vibration Seats
◊ Anti-vibration Tool Wraps
◊ Carts
◊ Compact Material Handling
◊ Wearable Anti-fatigue Matting
• Office
◊ Adjustable Workstations for Office Settings
◊ Alternative Keyboards
◊ Alternative Mice
◊ Chairs with Head Support
◊ Ergonomic and Adjustable Office Chairs
◊ Ergonomic Assessments
◊ Ergonomic Equipment
◊ Forearm Supports
◊ Gooseneck and Other Telephone Holders
◊ Scribe/Notetaker
◊ Speech Recognition Software
◊ Supine Workstations
◊ Writing Aids
• Other
◊ Aide/Assistant/Attendant
◊ Automatic Door Openers
◊ Flexible Schedule
◊ Modified Break Schedule
◊ Scooters
◊ Service Animal
◊ Stand-lean Stools
◊ Telework, Work from Home, Working Remotely
◊ Worksite Redesign / Modified Workspace
◊ Workstation Space Heaters [17]
Bending
• Accessible Baby Changing Stations
• Adjustable Exam Tables
• Adjustable Massage Tables
• Animal Lift Tables
• Automatic Snow Chains
• Battery Powered Lift Tables
• Compact Material Handling [17]
Balancing
• High-Density Storage & Retrieval System
• Omni Trax Omni-Directional Mobility
• EcoLift 50
• Afikim SE Scooter
• Renegade Wheelchair
• All Terrain Cane
• Clever-Lite LS Rollator Walker with Seat and Push Down Brakes [17]
Fine Motor
• Tracker Pro
• iConcepts Flexible Foldable Keyboard
• Impacto Anti-Vibration Grip Wrap
• Electric File Cabinets
• Three Level Carousel Media Center
• Boss Ergonomic Kneeling Stool
• Kevlar Reversible Seamless Machine Knit with Plastic Dots on Both Side Gloves
• Ergonomic Adjustable Phone Arm with Desk Clamp
• Dragon Naturally Speaking Medical Solutions
• EksoZeroG [17]
Conflicts of Interest:
The authors declare no conflicts of interest.
References
Social Security Disability Benefits for Lymphedema.View
Lymphatic Education & Research Network. Web site. https:// lymphaticnetwork.org/. Accessed February 2020.View
Hamm, R. L. (2015). Text and Atlas of Wound Diagnosis and Treatment. McGraw Hill Education.View
Foldi, E., & Foldi M. (2012). Foldi’s Textbook of Lymphology for Physicians and Lymphedema Therapists. 3rd ed. New York, NY: Elsevier.View
Armer, J.M., Cohn, J.C., Cormier, J.N., Kwan, M.L., & Stewart, B.R. (2011). Exercise in patients with lymphedema: a systematic review of the contemporary literature. J Cancer Surviv, 5:320- 336.View
Cormie, P., Galvao, D.A., Newton, R.U., & Spry, N. (2013). Neither heavy nor light load resistance exercise acutely exacerbates lymphedema in breast cancer survivor. Integrative Cancer Therapies 12(5):423-432.View
Ammitzball, G., Lanng, C., Kroman, N., Zerahn, B., Hyldegaard, O., & Andersen, K.K. (2017). Progressive strength training to prevent lymphoedema in the first year after breast cancer-the lyca feasibility study. ACTA Oncologica 56(2):360-366.
Bicego, D., Brown, K., Ruddick, M., Storey, D., Wong, C., & Harris, S.R. (2006). Exercise for women with or at risk for breast cancer-related lymphedema. Phys Ther 86:1398-1405.View
Areheart, B.A. (2008). When disability isn’t ‘‘just right’’: The entrenchment of the medical model of disability and the Goldilocks dilemma. Indiana Law Journal 83(1): 181–232.View
Fowler, C.A., & Wadsworth, J.S. (1991). Individualism and equity: Critical values in North American culture and the impact on disability. Journal of Applied Rehabilitation Counseling 22, 19-23.View
Stuki, G., Cieza, A., & Melvin, J. (2007). The International Classification of Functioning, Disability and Health: A unifying model for the conceptual description of the Rehabilitation strategy. Journal of Rehabilitation Medicine 39, 279-285.View
Olkin, R., & Pledger, C. (2003). Can disability studies and psychology join hands? American Psychologist 58, 296-304.View
Pertson, D. B., & Rosenthal, D. (2005). The ICF as an historical allegory for history in rehabilitation education. Rehabilitation Education 19, 95-104.
Berkley Planning Associates. (1982). A study of recommendations provided to handicapped employees by federal contractors (Contract No. J-9-E-1-009). Berkely , CA: Author.
West, J. (1991). The Americans with Disabilities Act: From policy to practice. New York Millbank Memorial Fund.View
Szymanski E.M. & Parker R. M. (1996). Work and Disability: Issues and Strategies in Career Development and Job Placement Pro Ed.View
Job Accommodation Network. (2020). View