
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 1 (2020), Article ID: JRPR-105
https://doi.org/10.33790/jrpr1100105Mini Review
Connecting the Classroom to the Community: The Effects of Service Learning on Affective Skills in Doctor of Physical Therapy Students
Jennifer Adame-Walker DPT, OCS, PMA-CPT*,Leslie Zarrinkhameh PT, DPT, GCS $ Amy Brogan Ed.D
Department of Physical Therapy, California State University Fresno, United States.
Corresponding Author Details: Dr. Jennifer Adame-Walker DPT, OCS, PMA-CPT, Assistant Professor, Director Musculoskeletal Care Clinic, Department of Physical Therapy, California State University Fresno, United States. E-mail: jadame@mail.fresnostate.edu
Received date: 11th May, 2020
Accepted date: 08th June, 2020
Published date: 10th June, 2020
Citation: Adame-Walker, J., Zarrinkhameh, L., & Brogan, A. (2020). Connecting the Classroom to the Community: The Effects of Service Learning on Affective Skills in Doctor of Physical Therapy Students. J Rehab Pract Res 1(1):105.
Copyright: ©2020, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: As the profession of Physical Therapy moves towards greater autonomy, new graduates will be faced with more complex cases and in-depth psychosocial issues that have not previously been addressed in Physical Therapy education. Experiential learning has been promoted in the literature as beneficial in providing an arena for practicing interpersonal skills, professional behaviors and clinical reasoning. Service-learning, one component of experiential learning has been established as an effective pedagogical system to marry cognitive, psychomotor and affective skills.
Methods: This study was a pre-post design that evaluated the affective, psychomotor, and cognitive skills of students enrolled in an integrated clinical experience (ICE). Prior to transitioning this course to a service-learning course, thirty-one 3rd year students enrolled and completed the course, which consisted only of in clinic activity. Following transition of this course to service-learning, thirty 3rd year students enrolled in and completed the course.
Results: There was a significant difference found in Clinical Performance Instrument (CPI) scores in all categories, both affective and psychomotor. Following incorporation of the service-learning components, the scores in the affective domain increased significantly in all areas of the CPI.
Discussion: This study shows the efficacy of service-learning on the development of affective skills in Doctor of Physical Therapy students during an integrated clinical experience. When scores were compared on the affective categories of the CPI from before and after inclusion of service-learning activities, there were significant positive changes (p=.00). Clinical instructors rated students at entry-level for safety, professional behavior, accountability, communication, cultural competence and professional development.
Keywords: Service-Learning, affective skills, Integrated Clinical Experience,PT Education
Introduction
The education of future physical therapists is complex and ever evolving. As the profession moves towards greater autonomy, new graduates will be faced with more complex cases and indepth psychosocial issues that have not previously been addressed in physical therapy education. The American Physical Therapy Association (APTA) established the Normative Model of Physical Therapist Professional Education with the mission of producing “knowledgeable, service-oriented, self-assured, adaptable, reflective practitioners”[1]. Within this model of education, the association has established practice expectations for behaviors, skills and knowledge of an entry level physical therapist. One example of this is practice expectation 5.0 of the Normative model, which includes demonstrating professional behavior, and participating in both peer and self-assessment activities [1]. Physical therapist educators have the responsibility of promoting these practices and developing curricular experiences that allow students to move beyond skill competency to develop professional behaviors also known as “soft skills” outlined by the APTA’s Core Values [2] and Commission on Physical Therapy Education (CAPTE) criteria[3]. The challenge remains in creating, sustaining, and cultivating these types of experiences to produce well rounded, autonomous therapists upon graduation. The normative model developed by the APTA describes 3 areas of skill; cognitive, psychomotor and affective [1]. According to Hayward et al, physical therapy students (SPT) require “the integration of knowledge, clinical skills and professional skills" [4] to be successful in their field. The cognitive and psychomotor domain, such as skill acquisition, is more easily recognized, taught and assessed. The affective domain, which includes responsibility, communication, interpersonal skills and clinical reasoning, has historically been a more challenging deliverable [3]. Current literature supports the need for improved teaching methods to develop affective and professional skills of SPTs as we move into the doctoral level [4,5]. According to Hayes et al. [5] even though Clinical Instructors (CI) felt a lack of professionalism and poor communication were unacceptable, they were less likely to address these behaviors as compared to poor cognitive or psychomotor performance. Not only is the need for instruction and mentoring apparent, a reliable method for assessing affective skills is also lacking [3,4,6].
The Commission on Accreditation for Physical Therapist Education (CAPTE) is the regulatory body responsible for the accreditation of Physical Therapy and Physical Therapist Education in the United States. CAPTE outlines standards of education to which DPT programs must adhere. One such standard is standard 6I: “The curriculum plan includes a variety of effective instructional methods selected to maximize learning. Instructional methods are chosen based on the nature of the content, the needs of the learners, and the defined expected student outcomes.” Service-learning and other types of experiential learning ensures Physical Therapy education programs meet this standard.
Experiential learning has been promoted in the literature as beneficial in providing an arena for practicing interpersonal skills, professional behaviors and clinical reasoning [7-11]. Servicelearning, one component of experiential learning, has been established as an effective pedagogical system to marry cognitive, psychomotor and affective skills. One approach for experiential learning, which includes service-learning, is an integrated clinical experience (ICE), which is another requirement of CAPTE. CAPTE defines ICE as clinical education experiences which occur before the completion of the didactic portion of the program. In this setting, SPTs perform patient care duties including examination, evaluation and treatment under the supervision of experienced licensed clinicians or faculty, with actual patients who have differing symptom presentations, psychosocial factors and various communication styles, without significant risk of harm, while developing and refining their professional skills. Wetherbee et al. supported faculty and student ICEs, because it allows students early interaction with patients to establish clinical reasoning and apply academic knowledge, which can make the ICE an effective service-learning tool in physical therapy education. In addition to promoting professional behavior, service-learning focuses on the community-academic relationship which allows reciprocal learning between the student and the patient [5].
Service-learning encompasses 3 distinct areas as described by Reynolds et al. including “a structured teaching and learning experience that meets identified needs in the community…reciprocal learning between the student and the community member… and reflection activities that facilitate students’ connection between their service in the community and instructional objectives” [12]. The reflective piece of service-learning is the component which sets it apart from community service and solidifies the assimilation of academic work into real world applications [11,13]. According to Anderson et al, reflection may be the key to higher self-assessment and Clinical Instructor (CI) ratings of professional behavior [14]. The study compared CI rating of professional behavior in 2 groups of SPTs; one group participated in a 1-week service-learning activity during their internship while the other group had only traditional internship experience. The results of the study showed significantly higher scores for professional behavior from the CIs as well as the students’ self-assessment for the group who participated in servicelearning compared to their peers. Understanding the significance and the impact of reflection on learning may help educators understand the importance of addressing affective skills and professional behavior rather than viewing them as personal character traits.
The purpose of this study was to examine the effects of servicelearning activities on the affective skills of Doctor of Physical Therapy students during patient care in an on-campus integrated clinical experience.
The on-campus integrated clinical experience course is held in the Student Health Center at California State University, Fresno (Fresno State) and is entitled Musculo-Skeletal Care Center or MSCC. DPT students are enrolled in this course two times - first in the second semester of the DPT program and again in their seventh of eight semesters. Students function in the role of a student physical therapist and treat patients, under the supervision of a clinical instructor who is a licensed physical therapist. The patients treated in MSCC are referred by health care practitioners in the on-campus Student Health, Psychological and Counseling Center and consist of the Fresno State student body.
Initially, the faculty who designed the MSCC course, did not design it as a service-learning course. Two of the authors (Adame and Zarrinkhameh) re-designed the course to meet service-learning objectives and put the course through the University process to reclassify the course as service-learning. The course consists of both clinic hours and a weekly seminar. Students are divided into morning and afternoon groups for the entire semester. Students provide 6 hours a week of service-learning in the form of patient care. This is in addition to the seminar portion of the course and the regular reflective assignments.
Methods
This study was a pre-post design that evaluated the affective, psychomotor, and cognitive skills of students enrolled in an integrated clinical experience (ICE) during the Fall semester in their 3rd year of a DPT program. Students spent 3 hours twice a week in the clinic with the expectation of treating 2 patients, under supervision, during that time period each day. They also spent 1 hour per week in an inclass seminar or on independent reading and reflection activity.
Prior to transitioning this course to a service-learning course, thirty-one 3rd year students enrolled and completed the course, which consisted only of in clinic activity. Following transition of this course to service-learning, thirty 3rd year students enrolled in and completed the course. The process for transition to a servicelearning course included restructuring of the seminar portion, as well as written assignments, with the goal of changing the focus to higher level clinical reasoning and reflection.
The seminar portion of the course was adjusted to promote the goal of developing reflective practitioners by increasing the direct correlation of academic work to clinical situations through grand rounds, small group discussion and lecture. Additional education regarding service-learning was emphasized, including several readings that related to service-learning as a whole and specifically to physical therapy with written reflection required each week. Again, the goal was to promote reflection on the students’ activity within the clinic, engagement with the community and development of professional behaviors.
Clinical instructors assigned to supervise students in the ICE used the Clinical Performance Instrument to assess individual skills of SPTs. The Clinical Performance Instrument was developed by the American Physical Therapy Association and published for use with students in 199715. Due to changing licensure and levels of education, the CPI was revised and approved by the APTA Board of Directors in November 2006 15. The newer version of the CPI has been shown to be a valid measure of student performance16 and is used in a vast majority of physical therapy educational programs.
The rating scale of the CPI is designed to be on a continuum, in order to reflect growth of the student throughout the DPT program. The CPI has standardized definitions of the anchor ratings used in the assessment of students from Beginner to Beyond Entry Level. These anchor ratings take into account student consistency of behaviors, complexity of patients, quality of behaviors, level of supervision required and efficiency of behaviors for each anchor rating. In order to standardize the assignment of anchor ratings, students and CIs must take a 2-hour online course which outlines the 18 criteria assessed in the CPI and defines the behaviors and elements in each of the anchor ratings. Students and CIs must pass a test in order to be able to use the CPI for student assessment.
Both the student and the CI complete the CPI at midterm (7 weeks) and final (15 weeks). For the student, filling out the CPI is one of the reflective assignments in this course. As is comparing their assessment of their performance to their CI’s assessment. Having the student complete the CPI meets a variety of criteria: students selfreflect on their own performance, strength and weaknesses, and it serves as a starting point for students and CIs to have a meaningful conversation regarding the student’s performance in MSCC, including the professional skill categories that make up the first portion of the instrument.
The first 6 categories of the CPI (safety, professional behaviors, accountability, cultural competence, professional development and communication) assess the affective domain of physical therapy practice. The next 12 criteria are more indicative of psychomotor and cognitive skills. Each of the categories on the CPI are rated by the Clinical Instructor at both mid-term and final using a 0-10 scale with numbers corresponding to proficiency levels from Beginning to Beyond Entry Level. See appendix for CPI and anchor ratings.
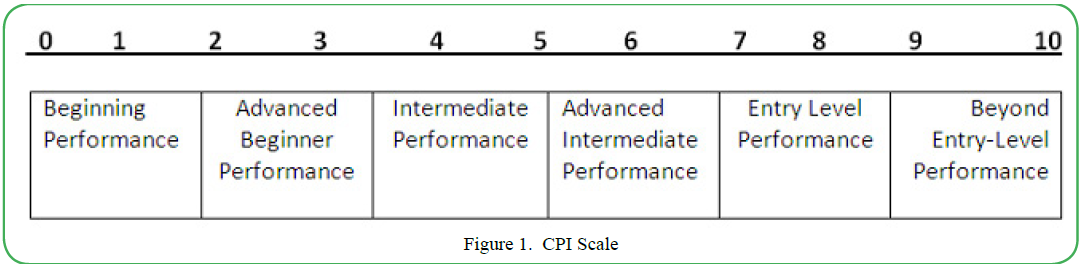
Figure 1. CPI Scale
Results
CPI scores were analyzed using IBM SPSS statistics, version 25. The means for each CPI category were compared between the pre S-L group and the post S-L group using independent samples t-tests with p <.05. There was a significant difference found in CPI scores for the first 6 categories of the CPI. Following incorporation of the service-learning components, the scores in the affective domain increased significantly in all areas. The SPTs scored in the advanced intermediate zone prior to service-learning and in the entry level zone following transition. There were positive increases in all areas of the CPI with the exception of category 18 (Direction and Supervision). However, these increases were not significant.
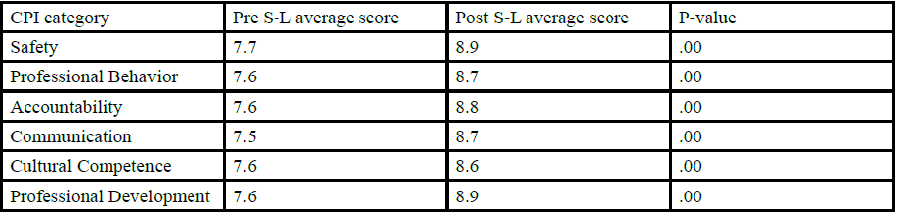
Table 1. CPI scores
Additional qualitative data collected from CIs was also positive. All CIs felt the Differential Diagnosis assignment was “appropriate and beneficial to the students’ level of education” and “exactly what they should be considering at this point in their program”. They were also supportive of the self-assessment performed by each student on the CPI in regards to their overall performance and application of academic work in the clinic setting.
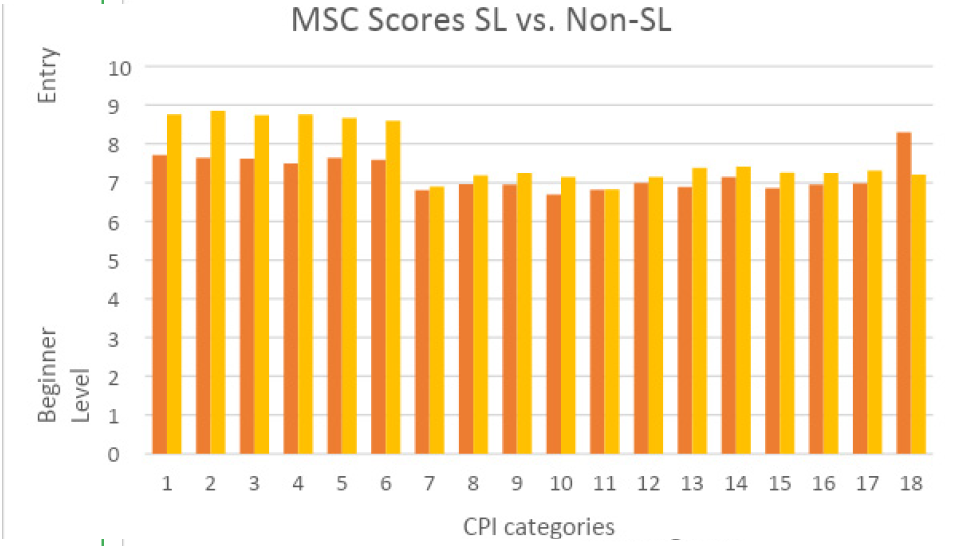
Chart 1. CPI score changes
Discussion
This study shows the efficacy of service-learning on the development of affective skills in Doctor of Physical Therapy students during an integrated clinical experience. When scores were compared on the affective categories of the CPI from before and after inclusion of service-learning activities, there were significant positive changes (p=.00). Clinical instructors rated students at entry-level for safety, professional behavior, accountability, communication, cultural competence and professional development. Other areas of the CPI increased as well, including clinical reasoning and evaluation but the changes were not significant.
The areas of the CPI which appear to be a direct assessment of affective skills include
1. safety
2. professional behavior,
3. accountability,
4. communication,
5. professional development and
6. cultural competence.
Each of these areas is an essential component of the affective domain and closely related to the Code of Ethics established by the
APTA [2].
According to the CPI, safety is comprised of “recognizing physical and physiological changes in patients and adjusting treatment as necessary, maintaining a safe environment for the patient, self and others throughout the clinical interaction” [16]. This may seem like a common-sense task but many SPTs are so narrowly focused on specific treatments or interventions that these simple tasks can be overlooked. Taking the time to educate students on environmental factors and psychosocial aspects of patient care gives them a solid foundation for patient care. Asking SPTs to reflect on their application of these skills and how it impacts the population they are serving, can help them to recognize the importance of widening their frame of reference and improving their awareness. An article by Village indicated “structured reflective opportunities are imperative” for a successful student experience [11].
Numerous studies in the literature focus on the lack of professional behavior displayed by physical therapy students [5,17,18]. The CPI lists professional behaviors as “demonstrating initiative and integrity, exhibiting compassion, caring and empathy in providing services to patients and managing conflict in constructive ways” [15]. Again, incorporation of reflection on treatment selection, differential diagnosis and the impact on their patients, increases not only the “soft skills” of the SPT, but improves the interpersonal communication and increases the chance of a successful outcome for the patient.
Accountability is another area that is difficult for students to conceptualize. The CPI defines accountability as “placing patient’s needs above their own self-interests, displaying generosity as evidenced by effort and time to meet patient’s needs and recognizing the need for physical therapy services to underserved populations” [15]. This area is most closely tied to the tenets of service-learning in that students are tasked with providing services to underserved populations. In this study, students provided services to the student body at a university that has a high percentage of first-generation college students and those who otherwise would not be able to receive these services. Of the patients treated in this ICE, approximately 50% reported having no insurance or California Covered insurance which would significantly limit their access to physical therapy services.
Current literature also identifies poor communication skills as another area of significant concern when educating SPTs. A study by Wolffe-Burke states “communication is what we do! It’s what we do all day long, we teach, we explain diagnoses…Then we instruct on exercise and how not to hurt”[18]. The CPI describes communication as “demonstrating professionally and technically correct written and verbal communication, initiating communication in difficult situations and identifying the most appropriate person with whom to communicate” [16]. This was one of the areas most strongly focused on during seminar in the service-learning ICE. During seminar, students were given the opportunity to explore different types of verbal and written communication through grand rounds and role play activities. They were then able to translate that academic practice into the clinic setting when attempting to educate or gather information from their patients. Additionally, students were required to document on patient care, provide written education to their patients in the clinic and complete reflective activities further assessing the effectiveness of their communication with their patients, colleagues and other health care providers. A study by Gazsi et al. described the importance and value of communication for SPTs in patient care. Their study showed the difficulty students have in understanding effective communication with patients of different backgrounds when attempting to learn in a strictly academic setting. SPTs reflection on effective communication came only after participating in the service-learning project [13].
Cultural competence is closely tied to communication. SPTs need to be aware of different customs and behavior patterns of different cultures, age and gender demographics and how their communication, both verbal and non-verbal, impacts their treatment of, and relationship with, that patient. A study by Galantino et al indicates the difficulty with providing SPTs exposure to diversity in just a classroom setting. Their study supports the benefit of service-learning in “providing a context for faculty to connect students with various populations”[8]. Some examples of components of cultural competence on the CPI are “providing care in a non-judgmental manner when the patient’s beliefs and values conflict with the individuals’ and communicates with sensitivity by considering differences in race/ethnicity, religion, age, gender, national origin, sexuality and disability”[16]. The University Student Health, Counseling and Psychological Services center is a wonderful opportunity for SPTs to work with a wide variety of different cultures, gender identities, age groups and patients of differing backgrounds and socioeconomic statuses. The demographics of this ICE were rich in representing a number of these populations and gave the SPTs ample opportunity to recall and apply their academic work from previous professional colloquium courses. Feedback from patients in this clinic gave evidence to the SPTs’ effectiveness in this area.
The last of the categories in the affective domain of the CPI is professional development. This is described as “using self-evaluation, ongoing feedback, inquiry and reflection to conduct regular ongoing self-assessment to improve clinical practice and discussing their progress of clinical and professional growth”[16]. This category may be the most important area for measuring improvement in the affective domain. Service-learning is predicated not only on service to the community but service to the provider or student. What makes service-learning unique and effective is the emphasis on the equal benefit to both the giver and the receiver, with those roles regularly revolving between those involved. Having students reflect on their service, perform regular self-assessment of their treatments and plans of care was instrumental in improving in this area.
While this study focused on the effects of adding service-learning activities to an existing ICE, it is clear the ICE itself can be beneficial in the education of SPTs. In this model, there was a partnership between the physical therapy department and the University with space provided by the Student Health, Counseling and Psychological Services Center and service provided by the Physical Therapy students and clinical instructors. A full-time faculty member served as the Director of the clinic and provided the bridge between the two departments. Further collaboration with the community allowed licensed clinicians to serve as CIs and supervise the SPTs in their development and delivery of care. A study by Wolffe-Burke lends weight to the need for strong clinical instructors to help guide developing SPTs towards professional behavior. She further states, “It is the right and responsibility of CIs to hold students to standards of professional behavior, just as there are standards for safety, effectiveness and efficiency for the cognitive and psychomotor domains” [18].
The outcomes of this study are closely related to current literature in describing the benefits of Service-Learning in physical therapy education. This study compares the outcomes of student performance in an integrated clinical experience before and after incorporation of and focus on service-learning activities. Both cohorts worked under the supervision of a licensed Physical Therapist to provide PT services to the student body of the University. The major differences between the 2 groups was the education of SPTs on Service- Learning principles prior to beginning patient care in the ICE and the incorporation of structured reflection activities designed to increase the SPTs awareness of their skill development and its effect on the patient population. In a study be Silcox et al, it is proposed that reflection activities “engage the individual in a cycle of thought and action based on experience, introspection, shared and examined analysis, and finally synthesis” [19,20]. Critical reflection is shown to improve clinical reasoning and higher order analysis [20].
Nowakowski et al found that SPTs were shown to develop clinical competency while providing services to elderly patients in a servicelearning course [21]. The current study did show an increase in all areas of the CPI competencies, with the exception of category 18, but only the affective domain, categories 1 to 6, had a significant increase. In another study, both SPTs and CI’s described the benefit to learning of reflective activity and experiences [6].
In an article by Anderson et al, the authors state “reflection may be the key to understanding why the SL group had higher selfassessment and preceptor ratings” [14]. They agree with previous literature that states “opportunities for self-reflection allow for internalization of core values” [14]. Their study showed the SPTs who participated in the SL activity had the highest assessment by preceptors as compared to the SPTs who did not participate. Another study by Mai et al describes SPT performance in an ICE, similar to the current study. They found the ICE to allow for SL activity that provided strong tie to the community as well as opportunities for SPTs to develop professional skills through continued practice in a real world setting [22]. Lastly, a study by Haines et al. described overall growth in “personal maturity, professional development, and cultural competence when studying the effects of a SL program in physical therapy assistant students [23].
Conclusion
Service-learning can be an effective means for improving the affective domain or ‘soft’ skills of SPTs during a physical therapy education program. This study showed significant improvement in the affective skills demonstrated by the increased scores in the first portion of the CPI after incorporating service-learning activities into an existing integrated clinical experience. Promoting reflective practitioners is important as we develop new curricula in physical therapy education and move into direct access and the Doctoral level. Future research is needed to strengthen these findings and to continue to explore which service-learning activities are most effective in improving students’ professional behaviors. Consistently practiced reflection appears to be the essential component in cultivating these skills but additional studies are needed to confirm.
Conflicts of interest/Competing interests:
Authors report no conflict or competing interest.
References
A Normative Model of Physical Therapist Professional Education: Version (2004). American Physical Therapy Association. Alexandria, Virginia. www.apta.org.
Code of Ethics. Alexandria, VA: (2000). American Physical Therapy Association.
Commission on Accreditation for Physical Therapy of Education. (1998). Evaluative Criteria for Accreditation of Educational Program for the Preparation of Physical Therapists. Alexandria, VA: American Physical Therapy Association.
Hayward, L., & Blackmer, B. (2010). A Model for Teaching and Assessing Core Values Development in Doctors of Physical Therapy Students. Journal of Physical Therapy Education. 24(3):16-27.View
Wise, H., & Yuen, H. (2013). Effect of Community-Based Service-Learning on Professionalism in Student Physical Therapists. Journal of Physical Therapy Education. 27(2):58- 64.View
Plack, M. (2006). The Development of Communication Skills, Interpersonal Skills and a Professional Identity Within a Community of Practice. Journal of Physical Therapy Education. 20(1):37-46.View
Smith, S., & Crocker, A. (2017). Experiential Learning in Physical Therapy Education. Advances in Medical Education and Practice. 8: 427-433.View
Galantino, M.L., House, L., Olsen, B., Fayter, T., & Frank, M. (2006). Multifaceted Aspects of Assessment in Service Learning: Lessons Learned. Journal of Physical Therapy Education. 20(3):49-54.
Musolino, G., & Feehan, P. (2004). Enhancing Diversity Through Mentorship: The Nurturing Potential of Service Learning. Journal of Physical Therapy Education. 18(1):29-42.
Bringle, R., & Hatcher, J. (1996). Implementing Service Learning in Higher Education. Journal of Higher Education. 67(2):1-8.View
Village, D. (2006). Qualities of Effective Service Learning in Physical Therapist Education. Journal of Physical Therapy Education. 20(3):8-17.View
Reynolds, P. (2009). Community Engagement: What’s the Difference Between Service Learning, Community Service and Community-Based Research? Journal of Physical Therapy Education. 23(2):3-9.View
Gazsi, C., & Oriel, K. (2010). The Impact of a Service Learning Experience to Enhance Curricular Integration in a Physical Therapist Education Program. Journal of Allied Health. 39(2):e-61-67.View
Anderson, J., Taylor, L., & Gahimer, J. (2014). Assessing the Impact of a Short-Term Service-Learning Clinical Experience on the Development of Professional Behaviors of Student Physical Therapists: A Pilot Study. Journal of the Scholarship of Teaching and Learning. 14(4) doi:10.14434/josotl.v4i4.12788
The Development and Testing of APTA Clinical Performance Instruments. (2002). American Physical Therapy Association. Phys Ther. 82(4):329-53.View
Kathryn, E., Roach, Jody, S., Frost, Nora, J., Francis, Scott, Giles., & Jon, T. (2012). Nordrum, Anthony Delitto, Validation of the Revised Physical Therapist Clinical Performance Instrument (PT CPI): Version 2006, Physical Therapy, Volume 92, Issue 3, Pages 416–428, https://doi.org/10.2522/ptj.20110129View
Arnold, L. (2002). Assessing Professional Behavior: Yesterday, Today and Tomorrow. Academic Medicine. 77(6):502-515View
Wolff-Burke, M. (2005). Clinical Instructors’ Descriptions of Physical Therapy Student Professional Behaviors. Journal of Physical Therapy Education. 19(1):67-76.View
Silcox, H.C. (1993). A How To Guide to Reflection: Adding Cognitive Learning to Community Service Programs. Philadelphia, PA. Brighton Press.
Hoppes, S., Bender, D., & DeGrace, B. (2005). Service Learning is a Perfect Fit for Occupational and Physical Therapy Education. J Allied Health. 2005; 34:47-50.View
Nowakowski, K., Kaufman, R., & Pelletier, D. (2014). A Clinical Service Learning Program Promotes Mastery of Essential Competencies in Geriatric Physical Therapy. Journal of Physical Therapy Education. 28(2):46-53.View
Mai, J., Thiele, A., O’Dell, B., Kruse, B., Vaassen, M., & Priest, M. (2013). Utilization of an Integrated Clinical Experience in a Physical Therapist Education Program. Journal of Physical Therapy Education. 27(2):25-32.View
Haines, J., Stiller, C., Thompson, K., & Doherty, D. (2017). Recent Graduates’ Perceptions of the Impact of a 1-Month International Service Learning Experience in Kenya During Their Physical Therapist Assistant Education. Journal of Physical Therapy Education. 31(1):73-79.View