
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 1 (2020), Article ID: JRPR-114
https://doi.org/10.33790/jrpr1100114Mini Review
Use of Cognitive Assessments across the Continuum of Care on a Single Health Care Campus
Amanda J. Blattman, OTD, OTR/L, Sara J. Stephenson*, OTD, OTR/L, BCPR, CBIS, CSRS
Department of Rehabilitation Services, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, 350 W. Thomas Rd, Phoenix, AZ 85013, Arizona, United States.
Corresponding Author Details: Sara J. Stephenson, OTD, OTR/L, BCPR, CBIS, CSRS, Department of Occupational Therapy, Neuroscience Publications; Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, 350 W. Thomas Rd.; Phoenix, AZ 85013, United States. E-mail: Neuropub@barrowneuro.org
Received date: 14th January, 2021
Accepted date: 17th March, 2021
Published date: 19th March, 2021
Citation: Blattman, A.J. & Stephenson, S.J. (2021). Use of cognitive assessments across the continuum of care on a single health care campus. J Rehab Pract Res, 2(1):114.
Copyright: ©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: This article describes occupational therapists’(OTs) use of cognitive assessments (standardized and nonstandardized) over 6 months on a healthcare campus. Also described are OTs’ use of the results of cognitive assessments to substantiate recommendations such as family education, safety, discharge disposition, and return to driving.
Method: An anonymous, 10-question survey was emailed to over 50 occupational therapists on a healthcare campus in three practice settings: acute hospital, neurological rehabilitation, and outpatient. Survey questions included the use of standardized and nonstandardized cognitive assessments and how results influence occupational therapist’s recommendations and clinical decision making.
Results: Over 80% of the reported tests administered over 6 months were nonstandardized or screening assessments versus 14% standardized assessments. Trends for the use of nonstandardized over standardized tests appeared to be related to time constraints and productivity demands, although comments stated that limited inferences could be made from nonstandardized assessments. Additionally, themes emerged regarding the influence that practice setting has on clinical decision-making and the overall use of cognitive assessments.
Conclusion: Across practice settings, OT on this healthcare campus use cognitive assessments and results to provide various recommendations that are influenced by the setting. In all practice settings, therapists more often implement nonstandardized versus standardized assessments to access cognition.
Running Title: Cognitive assessments across the continuum of care on a healthcare campus
Keywords: Cognition; Nonstandardized Cognitive Assessments; Occupational Therapy; Standardized Cognitive Assessments
Abbreviations
ACLS, Allen Cognitive Level Screen; ADL, activities of daily living; AOTA, American Occupational Therapy Association; CA, cognitive assessment; DLOTCA, Dynamic Lowenstein Occupational Therapy Cognitive Assessment; EFPT, Executive Function Performance Test; IADL, instrumental activities of daily living; LOTCA, Lowenstein Occupational Therapy Cognitive Assessment; MMSE, Mini-Mental Status Exam; MoCA, Montreal Cognitive Assessment; NCSE, Neurobehavioral Cognitive Status Exam; OT, occupational therapist or therapy; SLUMS, Saint Louis University Mental Status Exam; WPCA, Weekly Calendar Planning Activity
Occupational therapists (OTs) are educated in the intricacies of cognition. They are well-positioned to evaluate and address cognitive impairments in individuals who have been diagnosed with specific diseases such as Parkinson’s disease; sustained injury such as brain, spinal cord, and orthopedic trauma; or experienced neurological events such as strokes [1]. These individuals, especially those with neurological diagnoses, may have cognitive impairments that impact activities of daily living (ADLs), for example, bathing, and instrumental activities of daily living (IADLs), like financial or medication management [1-3]. The use of cognitive assessment (CA) instruments to identify impairment is, therefore, essential to the OT client’s well-being. OTs are positioned to improve client quality of life by appropriately assessing cognitionin at least three ways. First, accurate identification of cognitive impairment allows OTs to effectively address its effects on IADLs, such as money management, childcare, managing a chronic illness, driving, working, and planning for future needs [2-4]. Second, based on recent literature, through the consistent use of CAs over time, measurable changes in cognition, performance, and participation data can provide evidence of therapeutic achievement [5,6]. Third, the use and documentation of CAs can substantiate or justify the need for ongoing services or further specialized evaluation [2].
Importance of Cognitive Assessments in Occupational Therapy
Recent research highlights the pivotal role that OT has in reducing readmission rates. For example, assessment of cognition and subsequent assistance with medication management have been shown to be successful components of readmission reduction strategies [7,8]. Evidence supports that OT that focuses on clients’ daily functioning needs specifically as a spending category is the only rehabilitation discipline for which an increase in spending on OT has a statistically significant impact in lowering readmission rates and therefore supporting the need for ongoing and elevated CAs [8].
Cognitive impairment as a risk factor has also been associated with a 17% greater risk of first-time hospitalization; accordingly, OT is positioned to provide services to assess and address cognition to reduce hospitalizations [9]. Edwards and colleagues found that although individuals who experienced a mild-to-moderate stroke were deemed fully recovered when physical symptoms were resolved, there was evidence of residual cognitive impairments [2]. Such deficits in attention and concentration could have long-term negative effects on the person’s quality of life and imposed barriers to their engagement in meaningful activities [2]. In this study, Edwards and colleagues surveyed clients [6] months after they had experienced a mild-to-moderate stroke. They found that 35% were discharged home with no further therapy services [2]. However, clients continued to experience significant issues: 62% reported decreased proficiency in employment and volunteer activities, 36% reported decreased engagement in social activities, and 18% reported a decreased return to driving [2]. These findings indicate that despite independence with routine ADLs and mobilization, clients restricted their participation in preferred occupations and reported ongoing stroke-related deficits affecting life satisfaction [2]. In a second study, Edwards and associates compared OT hospital documentation to the results from a post stroke battery of standardized assessments that measured cognition, language, visual acuity, visual-spatial neglect, hearing, and depression [10]. Results indicated that clients demonstrating impairment had at least one cognitive or sensory deficit that was not documented by the primary therapist [10]. This study identified that the cognitive skill of memory was one of a cluster of components that failed to be documented in clients’ medical records most often and that 35% of clients had three or more undocumented impairments. Researchers determined that standardized CA was more efficient in detecting cognitive impairments than was routine clinical care [10]. These authors concluded that by not formally assessing cognitive abilities with standardized assessments, several deficits could go unrecognized and, therefore, untreated [10]. Di Carlo, Edwards, and their colleagues argued that if attention was focused on CAs to measure the impact of impairments on ADLs and IADLs, OTs could better help reduce the long-term effects of stroke and recommend appropriate follow-up services [2].
AOTA’s Vision 2025 supports the consistent assessment of cognition in clinical practice, recognizing that CA is client-centered, evidencebased, and cost-effective [11]. In addition, AOTA supports the use of CA for providing critical links between education, research, and clinical practice [1,11]. AOTA’s recent statement on cognition, cognitive rehabilitation, and occupational performance not only delineates the role of OT but also provides a narrative to describe the theoretical and research foundations that support OT’s key position in addressing cognition [1]. The statement highlights OTs’ roles in assessing cognition in many contexts to gain a holistic picture of the impact on clients’ roles, daily activities, or preferred occupations, rather than assessing cognition components in isolation [1]. OTs bring an understanding of the interrelatedness of cognition to a client’s overall function in the home and community [1]. Unfortunately, despite supportive statements and OT educational practices, CAs are documented in the literature as underused in clinical OT settings. There is little evidence to indicate that the use of CA instruments in allied health is increasing [12,13].
Underuse of CA in OT Clinical Settings
In a review of CAs across allied health professions, including OT, Duncan and Murray [13] described the routine use of standardized assessments as an ambition. Wolf and associates [14]found that 71% of clients diagnosed with mild to moderate stroke were discharged home with little to no ongoing therapy services. The authors posited that this gap is due partly to no singular stroke scale having the item breadth and sensitivity to identify all deficits impacting clients’ post stroke participation. Despite the OT knowledge base and welldeveloped theoretical frameworks regarding the evaluation and treatment of clients with cognitive impairments, current research suggests that the use of standardized assessments in clinical OT practice could be improved [14,15]. Evidence shows that therapists have restricted their scope of OT practice by discharging clients from OT services due to mobility and ADL independence, without formally assessing cognition [12,15]. Two reasons the researchers identified were limited time and ease of informal observations to determine cognitive status [12,15]. Occupational therapists may be underusing CAs in nonneurological populations as well. This situation is potentially detrimental to these populations because the incidence of postoperative cognitive dysfunction after major elective orthopedic surgery at the1-year follow-up is documented at threefold higher than in the general public [16,17]. Additionally, 25% to 50% of clients with heart failure are estimated to have cognitive deficits that may impact their performance, independence, and compliance with medication management, contributing to poor health outcomes and readmissions for care [8,[18].
Situational Factors Influencing OT Practitioner Use of Cognitive Assessment
In the home health setting, Burns and Neville’s CA study found that therapists preferred using nonstandardized OT assessments, which was influenced by situational factors that could partly explain the presumed underuse of CAs in various clinical settings [12,19]. Situational influences should be considered when evaluating OT practices as they relate to the frequency of CA use in any practice setting. These situational influences can be grouped by structural or administrative, clinician-specific, and client-specific categories. Structural or administrative influences include the cost of assessments, time constraints, the availability of assessments, specialized practice, and other allied health professionals addressing cognition. Clinicianspecific influences include lack of familiarity with appropriate measurements and CA being conducted through simple activities or interviews. Client-specific influences include diagnoses indicating the need for testing, endurance for the assessment, and client cooperation. Because of system and site-specific factors, the implementation of CA is not a straightforward matter. Although our study’s primary goal was not to investigate these factors, it is important to keep them in mind when looking at healthcare systems as a whole.
Our study aimed to assess and compare key aspects of CA practices among OTs in a single healthcare system across three clinical settings: the acute hospital, neurorehabilitation, and outpatient settings. Accordingly, at a large healthcare campus, we surveyed OTs to identify the CA instruments they used and how frequently they assessed cognition and applied the results to inform practice decisions. To our knowledge, no studies have reported a single healthcare system’s approach to CA across the continuum of OT care to assess care quality, which involves identifying the appropriateness, alignments, and variations in CA methods across clinical settings. We believe it is essential for OTs to assess their practices across clinical settings within various healthcare environments to identify gaps and strengths in CA and to understand the impact of OT on client outcomes. Our methods may be applied to other systems and settings to support OTs in assessing and improving the quality of CA practices.
Methods
Participants and Procedures
A total of 57 survey invitation emails were sent to OTs employed at a large healthcare campus with three OT practice settings: the acute hospital, neurorehabilitation, and outpatient settings. Twenty-eight individuals (49% rate of return) participated in the online survey administered through Survey Monkey, which was available for 45 days. The survey questions inquired about how OTs assess cognitive function across the continuum of care within the healthcare campus.The survey consisted of 10 questions designed to take approximately 20 minutes to complete, including one free-response item. Reminders were sent 14 and 30 days after the initial invitation. The authordesigned survey was anonymous, and no identifying information was recorded. The hospital’s institutional review board gave this survey study exempt status.
Experience and Type of OT Practice
Three items asked respondents for demographic information regarding OT experience. The first question addressed the primary practice area on the hospital campus, where the study was conducted. The second question asked how long OTs have been practicing (options ranged from 1 = less than 1 year to 5 = more than 15 years). The third item asked respondents to indicate the type of population with whom they typically work. Respondents could select as many populations as were relevant from this list: brain injury, spinal cord injury, Parkinson’s disease, hand/orthopedics, and stroke.
Cognitive Assessment Use and Frequency
Respondents were asked to indicate which CAs they used and their frequency of use in the past 6 months. The survey covered the use of 10 CA instruments or methods, which we chose because they were available in all three settings on campus. The 10 CAs were organized in general categories of standardized CA, screening CA, and nonstandardized CA, including clinical observations. The five standardized cognitive assessments were as follows: (1) Dynamic Lowenstein Occupational Therapy Cognitive Assessment (DLOTCA) [20]; (2) Lowenstein Occupational Therapy Cognitive Assessment (LOTCA) [21]; (3) Cognistat Neurobehavioral Cognitive Status Exam (NCSE) [22]; (4) Executive Function Performance Test (EFPT) [23]; and (5) Weekly Calendar Planning Activity (WPCA) [24]. The four CA screens were as follows: (1) Allen Cognitive Level Screen (ACLS) [25]; (2) Montreal Cognitive Assessment (MoCA) [26]; (3) Saint Louis University Mental Status Exam (SLUMS) [27]; and (4) Mini-Mental Status Exam (MMSE), [28] and nonstandardized client observation.
Use of Cognitive Assessment Results
Respondents were asked three questions regarding how frequently they used CA results to inform practice decisions in the previous 6 months. These questions included the use of CA results to provide client and or caregiver education; to make recommendations for safety, driving, return to work, and supervision in the home or community; and to make recommendations regarding the living situation or discharge disposition. Responses for the frequency items were all rated on a 5-point scale. For the analysis, the five categories were collapsed into three basic categories: never used, sometimes use, always used (see Table 1 for survey items). One free-response question asked respondents to describe barriers to using CA in practice.
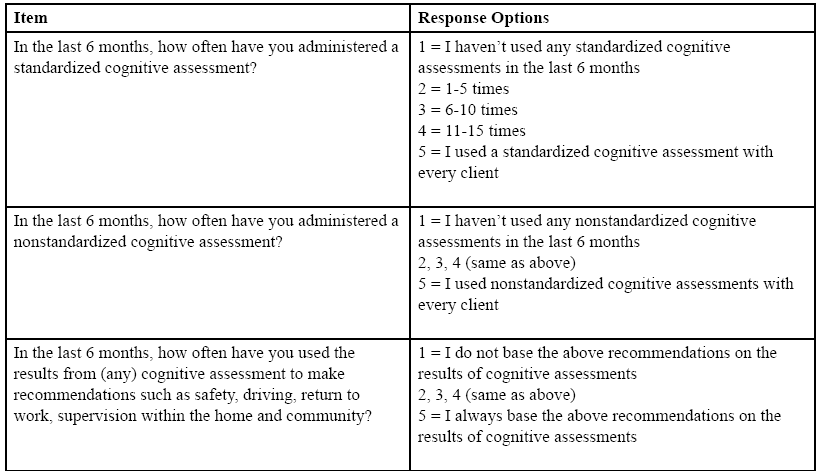
Table 1.Cognitive assessment survey items
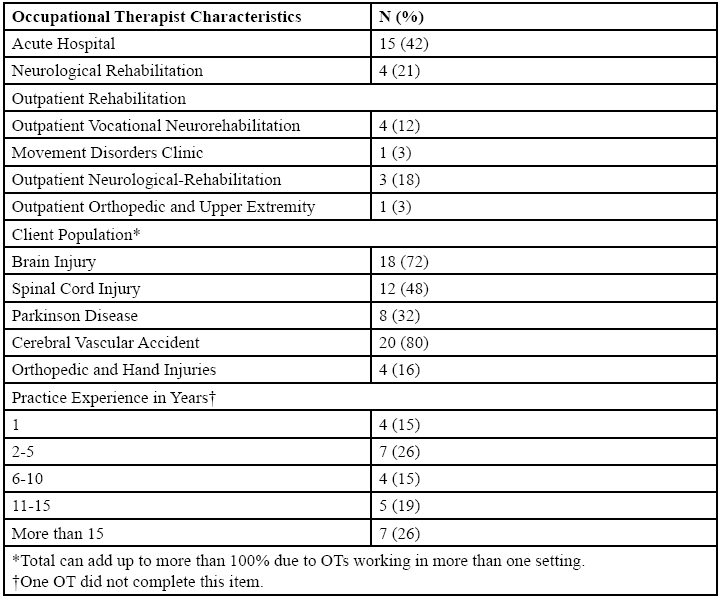
Table 2.Participants (n = 28), practice setting, practice experience
Results
Participants were OTs employed across three different settings at a single hospital healthcare campus. Descriptions of participants’ practice settings and experiences are presented in Table 2.
Cognitive Assessment Use
Respondents were asked to indicate which types of CAs they used in the past 6 months. Table 3 presents the results across the three practice settings. Seventy of 84 (82%) total CA responses were nonstandardized or cognitive screen assessments, versus 13 of the 84 total CA responses were standardized CAs. Of the cognitive screens, the MoCA was used by 21 of 28 therapists (75%). Participants used the SLUMS (15/28) (54%) and MMSE (11/28)(40%) to a lesser degree. Of the standardized cognitive assessments, the EFPT was reported to be used by 9 of 28 therapists (32%). The other assessments in this category were rarely used.
In the acute hospital setting, 40 of 45 (86%) reported CAs were nonstandardized or cognitive screen assessments, and 5 of 45 (11%) were standardized CAs. Of the cognitive screens, the MoCA was used by 11 of 15 therapists (73%). The EFPT was reported to be used by 4 of 15 therapists (27%).
In the neurorehabilitation setting, 9 of 11 (82%) OTs reported the CAs used were nonstandardized or cognitive screen assessments, and 2 of 11 (18%) used standardized CAs. Of the cognitive screens, the MoCA was used by all 4 therapists in the neurorehabilitation setting. The CAs EFPT and WCPA were reported to be used by 1 of 4 therapists (25%).
In the outpatient setting, 11 of 28 (75%) OTs reported CAs used were nonstandardized or cognitive screen assessments, and 7 of 28 (25%) reported were standardized CAs. Of the cognitive screens and nonstandardized CAs, clinical observation was reported to be used by 8 of 9 therapists (89%). The CA EFPT was reported to be used by 4 of 9 therapists (44%).
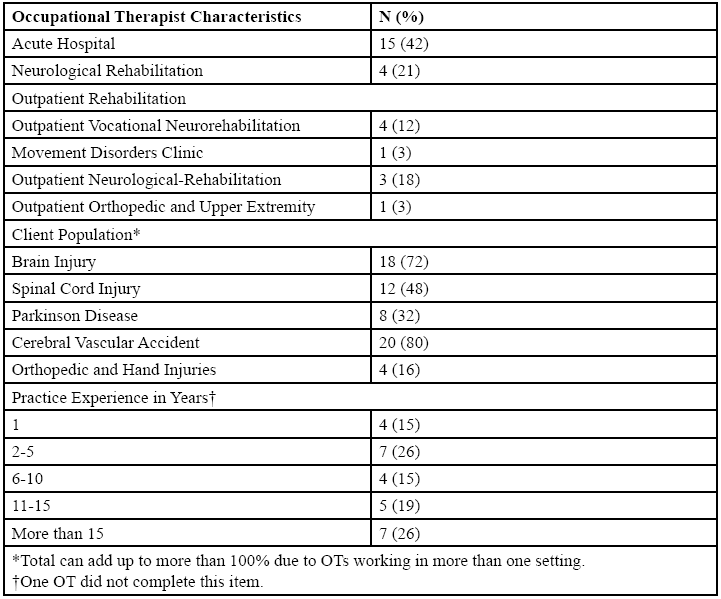
Table 3.Cognitive assessments used by OT by setting
Frequency of Cognitive Assessment Use
Respondents were asked to indicate how frequently they assessed cognition using standardized, nonstandardized, or cognitive screen assessments in the past 6 months. Table 4 presents the overall results and the results for the three practice settings. Overall, the OTs reported always using standardized assessments 14% of the time. They reported always using nonstandardized or cognitive screens 43% of the time. Respondents reported never using CAs 22% of the time. In the acute hospital setting, no OT reported always using a standardized CA, and 93% reported using a standardized CA sometimes. About half (53%) of the OTs in the acute hospital setting reported always using a nonstandardized CA or cognitive screen, whereas 26% reported using a nonstandardized CA or cognitive screen sometimes. In the neurorehabilitation setting, one of the four OTs reported always using a standardized CA, and half reported using a standardized CA sometimes. None of the OTs in the neurorehabilitation setting reported always using a nonstandardized CA or cognitive screen, and one of four reported sometimes using a nonstandardized CA or cognitive screen. In the outpatient setting, a lower percentage of OTs reported using standardized CAs always (33%) versus sometimes (56%); nonstandardized CAs or cognitive screens were reported to be used by 44% of OTs always and sometimes.
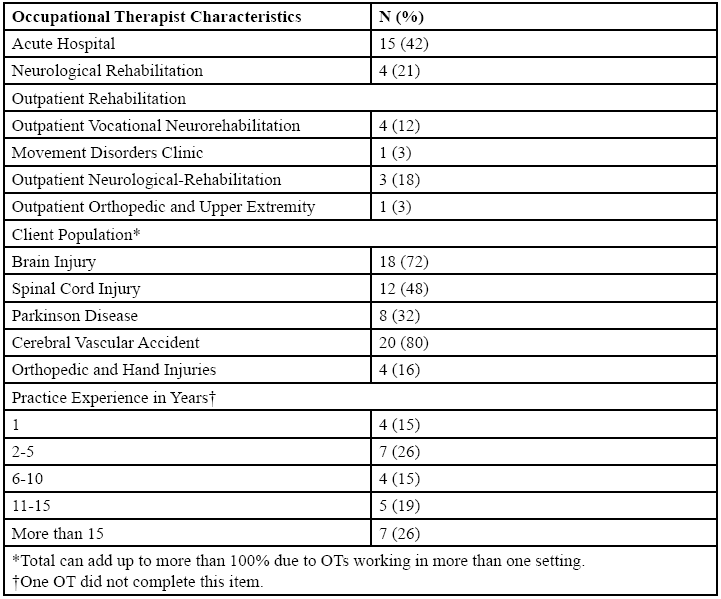
Table 4.OT frequency of use of cognitive assessments by setting
Cognitive Assessment Use to Inform Practice and Recommendations
Respondents were asked to indicate the use of results from any CA for specific clinical purposes in the past 6 months (Table 5). Overall, 37% of clinicians reported that they always use assessment results to inform practice and recommendations, 61% reported sometimes, and 9% reported never. Across the settings, clinicians reported using CA results to inform practice and recommendations similarly.
Barriers to Using in Practice
Three clinicians responded to the free-response question, which asked to identify barriers to using CA in practice. Participants reported that 1) “nonstandardized assessments are easier and quicker to administer than standardized assessments”; 2) “the results are interesting but difficult to correlate to ADLs and IADLs”;3) “there is not enough information on the available tests to select the most appropriate CA for clients”; and 4) CA is perceived as not relevant due to the diagnosis, as one respondent indicated “the patient population is primarily cardiothoracic and orthopedic.”
Discussion
We examined the current practices of OTs regarding the use of CAs (standardized, nonstandardized, and screens) across three clinical settings (acute care hospital, neurorehabilitation, and outpatient care). A key finding of the study is the large extent to which nonstandardized assessments and screens are used instead of standardized assessments. In all three settings, OTs responded "sometimes" more frequently than "always" to describe their use of standardized CAs. The study indicates that, while CAs are used in all practice settings, nonstandardized CAs, such as observations, are preferable to the available standardized CAs. This finding aligns with recent research findings, which indicate that nonstandardized CAs were used most frequently to determine the cognitive status of clients [12,29]. There were responses in the "never" category, which supports the concept that OTs may be limiting their scope of practice. According to Wolf and associates, [14] this lack of CA can lead to clients not receiving appropriate ongoing services, which may impact their quality of life [2,5].
A key study aim was to examine the frequency of use of any CA to inform OT practice regarding clinical recommendations and client or caregiver education. The reported results for CA use were similar among the groups: In all three groups (settings), CA use was inconsistent and limited. This finding supports the need for further investigation into why clinicians may implement CA with clients but not use the results. The results also support the concept that OTs may be limiting their scope of practice in providing in-depth recommendations regarding the impact of cognitive impairments on ADLs and IADLs [2].
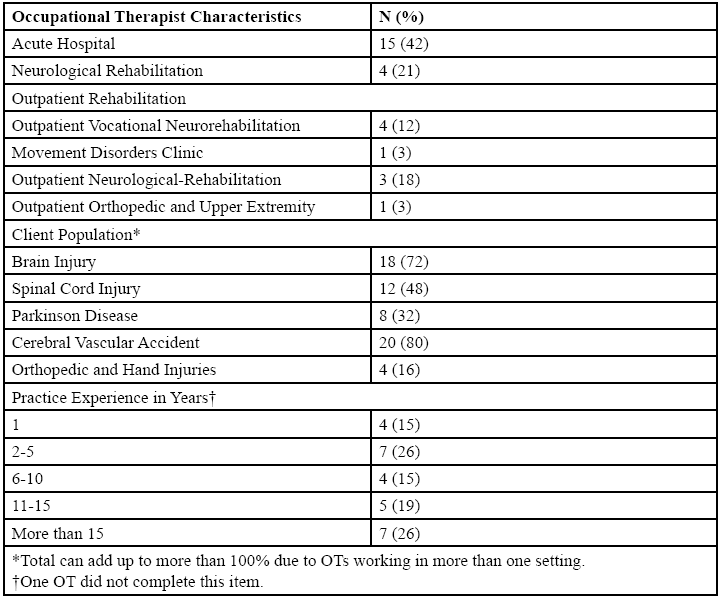
Table 5.OT frequency of use of cognitive assessments by setting
Lastly, although there were a limited number of responses to the openended question on barriers to the use of CA, we find this information valuable as a starting place to discuss CA practices further. The time it takes to administer the CA, knowledge of appropriate tests, and the ability to correlate the results to ADLs and IADLs were identified as barriers to consistently using the standardized CAs in clinical practice.
Limitations and Future Research
The survey response rate of 49% was too low to perform meaningful statistical significance testing across the three practice settings. A larger response rate per practice setting would be required in the future to determine if the observed differences reach a level of significance. Selection bias is present because the groups were not randomly selected, and the sample obtained is not representative of all OT settings. The study was further limited by the design of the questions and the response selections, which were created to indicate frequency but limited the overall choices from which OTs could select. Additionally, the survey did not separate which assessments informed recommendations, standardized or nonstandardized. Researchers were unable to determine what effect the years of OT experience had on the results. Thus, the results for this construct should be interpreted with caution. Future survey design studies should select a more robust scale for CA frequency of use and client populations to capture more information, especially in the cardiac and transplant patient populations.
Implicatons for Practice
This study has several implications for OT practice. It supports that OTs should seek to expand their practice habits to include routine CAs with clients regardless of diagnosis and incorporate more standardized CAs. There is a potential that more frequent implementation of robust, standardized CAs could lead to increased use of CA instruments, improved skill proficiency in administration, and concrete evidence of the benefits of providing evidence-based recommendations to clients and their families. Clinicians should incorporate meaningful CAs based on their clients’ needs, which aid in not only informing various discharge recommendations but informing ongoing therapeutic intervention. There is an opportunity to develop setting-specific practice information for CA selection, administration, result interpretation, and translation of findings to practice by setting. By providing and implementing setting-specific CA information, OTs are more likely to feel confident and provide more holistic care, which may enhance client outcomes.
Conclusion
This study was conducted to contribute to the body of knowledge regarding OT use of CAs in different practice settings. The survey results highlight the similarity in the frequency of use among the settings: (1) CAs are used inconsistently and in a limited fashion across all settings, (2) standardized CAs are underused, and (3) when OTs do use CAs, they do not use the results to make clinical decisions on some issues such as discharge recommendations, safety, driving recommendations, or family education. This discovery further supports the notion that OTs restrict their scope of practice by overlooking or not prioritizing cognition. AOTA’s statement on cognition purports that “cognitive functioning is always embedded in occupational performance (ADLs, IADLs) and cannot be accurately understood in isolation”[30]. As such, OTs should implement CA as part of routine care for clients to better meet the societal needs of their clients [14]. With the implementation of CA, the ecological validity of the testing situation would be heightened, and OTs would have more evidence-based information regarding client abilities, and this would allow them to make better-informed recommendations.
Disclosures:
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this manuscript.
Financial Support :
None
Acknowledgments:
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation. A portion of this manuscript was presented at the virtual Arizona Occupational Therapy State Association Conference on October 24, 2020. Statistical support was provided by Heidi Wayment and supported, in part, by funds from grant NIH/ NIMHD RCMI U54MD012388 (Baldwin/Stearns-MPI).
References
American Occupational Therapy Association. Cognition, cognitive rehabilitation, and occupational performance. Am J Occup Ther. Nov/Dec 2019;73(Supplement_2):731241001 0p7312410011-7312410010p7312410026.
Edwards, D.F., Hahn, M., Baum, C., & Dromerick, A.W. (2006). The impact of mild stroke on meaningful activity and life satisfaction. J Stroke Cerebrovasc Dis, 15(4):151-157.View
Marshall, G.A., Rentz, D.M., Frey, M.T., et al. (2011). Executive function and instrumental activities of daily living in mild cognitive impairment and Alzheimer's disease. Alzheimers Dement, 7(3):300-308.View
American Occupational Therapy Association. (2014). Occupational Therapy Practice Framework: Domain and Process (3rd Edition). Am J Occup Ther, S1-S48.View
Di Carlo, A., Baldereschi, M., Lamassa, M., et al. (2016). Daily Function as Predictor of Dementia in Cognitive Impairment, No Dementia (CIND) and Mild Cognitive Impairment (MCI): An 8-Year Follow-Up in the ILSA Study. J Alzheimers Dis, 53(2):505-515.View
Unsworth, C.A. (2011). Evidence-Based Practice Depends on the Routine Use of Outcome Measures. British Journal of Occupational Therapy, 74(5):209-209.View
Bradley, E.H., Curry, L., Horwitz, L.I., et al. (2013). Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes, 6(4):444-450.View
Rogers, A.T., Bai, G., Lavin, R.A., & Anderson, G.F. (2017). Higher Hospital Spending on Occupational Therapy Is Associated With Lower Readmission Rates. Med Care Res Rev, 74(6):668-686.View
Callahan, K.E., Lovato, J.F., Miller, M.E., Easterling, D., Snitz, B., & Williamson, J.D. (2015). Associations Between Mild Cognitive Impairment and Hospitalization and Readmission. J Am Geriatr Soc, 63(9):1880-1885.View
Edwards, D.F., Hahn, M.G., Baum, C.M., Perlmutter, M.S., Sheedy, C., & Dromerick, A.W. (2006). Screening patients with stroke for rehabilitation needs: validation of the poststroke rehabilitation guidelines. Neurorehabil Neural Repair. 20(1):42-48.View
American Occupational Therapy Association. (2017). Vision 2025. American Journal of Occupational Therapy, 63(5):621- 625.
Burns, S.C., & Neville, M. (2016). Cognitive assessment trends in home health care for adults with mild stroke. Am J Occup Ther, 70(2):7002290020p7002290021-7002290028.View
Duncan, EA., & Murray, J. (2012). The barriers and facilitators to routine outcome measurement by allied health professionals in practice: a systematic review. BMC Health Serv Res, 12:96.View
Wolf, TJ., Baum, C., & Conner, L.T. (2009). Changing face of stroke: implications for occupational therapy practice. Am J Occup Ther, 63(5):621-625.View
Morrison, M.T., Edwards, D.F., & Giles, G.M. (2015). Performance-based testing in mild stroke: identification of unmet opportunity for occupational therapy. Am J Occup Ther, 69(1):6901360010p6901360011-6901360015.View
Ballard, C., Jones, E., Gauge, N., et al. (2012). Optimised anaesthesia to reduce post operative cognitive decline (POCD) in older patients undergoing elective surgery, a randomised controlled trial. PLoS One, 7(6):e37410.View
Choi, S., Avramescu, S., Orser, B.A., & Au, S. (2019). Protocol for a prospective cohort study of assessing postoperative cognitive changes after total hip and knee arthroplasty in the Greater Toronto area. BMJ Open, 9(2):e024259.View
Gallagher, R., Sullivan, A., Burke, R., et al. (2013). Mild cognitive impairment, screening, and patient perceptions in heart failure patients. J Card Fail, 19(9):641-646.
Muller-Engelmann, M., Keller, H., Donner-Banzhoff, N., & Krones, T. (2011). Shared decision making in medicine: the influence of situational treatment factors. Patient Educ Couns, 82(2):240-246.View
Katz, N., Bar-Haim Erez, A., Livni, L., & Averbuch, S. (2012). Dynamic Lowenstein Occupational Therapy Cognitive Assessment: evaluation of potential to change in cognitive performance. Am J Occup Ther, 66(2):207-214.View
Katz, N., Itzkovich, M., Averbuch, S., & Elazar, B. (1989). Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) battery for brain-injured patients: reliability and validity. Am J Occup Ther, 43(3):184-192.View
Nabors, N.A., Millis, S.R., & Rosenthal, M. (1997). Use of the Neurobehavioral Cognitive Status Examination (Cognistat) in traumatic brain injury. Journal of Head Trauma Rehabilitation, 12(3):79-84.View
Baum, C.M., Connor, L.T., Morrison, T., Hahn, M., Dromerick, A.W., & Edwards, D.F. (2008). Reliability, validity, and clinical utility of the Executive Function Performance Test: a measure of executive function in a sample of people with stroke. Am J Occup Ther, 62(4):446-455.View
Toglia, J. (2015). Weekly Calendar Planning Activity (WCPA): a performance test of executive function: AOTA Press.
Allen, C.K. (1985). Occupational Therapy for Psychiatric Diseases: Measurement and Management of Cognitive Disabilities: Little Brown & Co.View
Nasreddine, Z.S., Phillips, N.A., Bedirian, V., et al. (2005). The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc, 53(4):695- 699.View
Tariq, S.H., Tumosa, N., Chibnall, J.T., Perry, M.H., 3rd, & Morley, J.E. (2006). Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder-a pilot study. Am J Geriatr Psychiatry, 14(11):900-910.View
Folstein, M.F., Folstein, S.E., & McHugh, P.R. (1975). "Minimental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res, 12(3):189-198.View
Belchior, P.D., Bains, T., Hargadon, J., et al. (2016). Assessing functional impairment in individuals with mild cognitive impairment. The Open Journal of Occupational Therapy, 4(2).View
American Occupational Therapy Association. (2013). Cognition, cognitive rehabilitation, and occupational performance. Am J Occup Ther, 67 (Suppl):S9-S31.