
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 1 (2021), Article ID: JRPR-127
https://doi.org/10.33790/jrpr1100127Research Article
Does Balance Fluctuates Depending on Leg Dominance? A Cross-sectional Study
Carley Bowman SPT & Martín G. Rosario PT, PhD, CSFI, ATRIC*
Physical Therapy Program, Texas Woman’s University, Dallas Campus; Texas;United States.
Corresponding Author Details: Martin G. Rosario, PT, Ph.D., CSFI, ATRIC, Assistant Professor, School of Physical Therapy Texas Woman's University, Physical Therapy Program, Dallas Campus; 5500 Southwestern Medical Ave. Dallas, TX 75235-7299,United States. E-mail: mrosario1@twu.edu
Received date: 17th September, 2021
Accepted date: 12th November, 2021
Published date: 15th November, 2021
Citation: Bowman, C., & Rosario, M.G. (2021). Does Balance Fluctuates Depending on Leg Dominance? A Cross-sectional Study. J Rehab Pract Res, 2(2):127.
Copyright: ©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Falls due to altered balance are a worldwide health issue. Various components are involved in maintaining postural stability, such as the base of support, integration of sensory information, and the ability of the body to adapt to perturbations. Understanding balance strategies and components is imperative for rehabilitation when stability is affected.
Purpose: This study aimed to characterize the balance distinction between left and right leg dominance and identify postural adaptations during left and right rotations in young healthy adults.
Method: This study assessed single-leg stance on a firm surface, clockwise (right), and counterclockwise (left) rotation on a balance board with a fixed middle fulcrum on 70 health young adults participants, 7 males and 63 females aged 25 ± 4.66 SD (37 left leg dominant and 32 right leg dominant). Accelerometer and gyroscope sensors were used to capture the total sway area, medial-lateral (ML) and anterior-posterior (AP) directions, velocities, and distances.
Results: The MANOVA revealed similarities in the left and right single stance balance. The comparison of clockwise rotations versus counterclockwise rotations showed a significant increase in sway and distance in the anteroposterior (AP) direction while rotating towards the left or CCW (P<0.05). The comparison of right-leg dominant versus left-leg dominant during CW rotation revealed a significantly increased sway and distance of sway in the ML direction (P<0.05) for individuals with right-leg dominance when compared to their left-leg dominant counterparts during CW rotations.
Conclusion: The current study found distinctions in balance adaptation or changes within the central nervous system to compensate for an increase in sway during counterclockwise rotation. Furthermore, individuals with right leg dominance had increased difficulty in maintaining stable sway during clockwise rotational movements. Clinicians should consider examining rotational adaptations or one’s ability to make alterations within the central nervous system during rotational movements to maintain the center of mass within the base of support in balance activities which compromise postural control.
Introduction
The World Health Organization considers falls to be a major health problem worldwide. Falls can be fatal and account for one of the two top risk factors associated with the worldwide mortality rate. As individuals age, fall risk and the aftermath injuries of falls increase in severity, with the highest percentage of falls being at 60 years of age and above (www.WHO.org).
This fall risk can be reduced by improving and maintaining intact balance resources. Balance can be defined as an individual’s success in maintaining their center of gravity (COG) inside their base of support (BOS) with minimal postural sway [1]. Furthermore, all humans have a cone of stability, referencing the surrounding most stable region in upright standing. If deviation exceeds the cone of stability boundaries, then postural control mechanisms elicited by muscle activity must be recruited to preserve balance and avert a fall [2]. Postural control mechanisms such as ankle, hip, and stepping strategies are effectively utilized in static and dynamic balance by muscle engagement ranging from the proximal trunk to distal body segments. The amplitude of the perturbations dictate the mechanisms employed for balance conservation. The ankle strategy can effectively counteract small-amplitude perturbations, whereas larger amplitude perturbations require a stepping strategy [1]. Falls result when an individual cannot successfully adapt to a perturbation [3].
However, the compliance of a support surface also dictates which strategy will be utilized for balance recovery. The ankle strategy can be successful in maintaining balance on a firm surface but once a surface has become “soft” or non-compliant, proprioceptive input becomes inaccurate to spatially orient the body. This inconsistency requires additional resources to be employed by the central nervous system with a counter-rotation mechanism of control to prevent a fall [4]. Similar to non-compliant surfaces, balance boards are unstable with a narrow BOS. Silva and colleagues [5] explored the effect of wobble board training on movement strategies described above. The authors described wobble boards to be comparable to our M-PAD balance board, a board with a narrow hemi-spherical base allowing for multi-planar movements inducing standing instability with increased stress on postural control mechanisms. Authors concluded in healthy young adult males, the effect of wobble board training enhanced postural control mechanisms by improving the trunk’s velocity of countermovements in response to board oscillations and overall body coordination [5]. Similarly, Rosario and colleagues found healthy young adults make postural control compensations seen as quicker sway velocity in the medial-lateral direction and increased sway distance in the anterior-posterior direction in bipedal stance on a high/low fulcrum rotating balance board. The balance board utilized in this study is identical to the M-PAD balance board in this inquiry (2021a).
In addition to the above, right or left leg dominance is common and to our knowledge, multiple studies have proven inconclusive in determining whether leg dominance has a ramification of the effectiveness of postural control mechanisms. For example, Yoshida and colleagues found leg dominance to be associated with an increased acuity in postural control mechanisms on the leg of dominance, such as ankle, hip, and stepping strategies [6]. However, a systematic review of 46 studies investigating whether leg dominance plays a role in balance performance concluded that there were no significant differences between dominant and non-dominant legs in unilateral balancing tasks with regard to postural sway [7].
Aside from postural control mechanisms, the balance system must integrate information from the vestibular, proprioceptive, and visual systems to appropriately balance perturbations. Abnormal integration among any of the three systems results in postural instability, as illustrated by an increased fall risk. The dynamic systems theory (DST) further explains the role of the three systems by stating they must work in cohesion when balance is challenged by a perturbation [3]. However, when any one of the three systems is underperforming or absent in the presence of disease, sensory reweighting or sensory modification must occur to maintain appropriate balance performance in different environments and on various surfaces. If one or more of these balance networks becomes compromised and the body is required to rely more heavily on other systems to conserve balance, then sensory reweighting has failed [3].
During therapeutic evaluations and interventions, physiotherapists typically use the assessment values of the non-injured limbs to make comparisons with injured limbs. However, prior studies have found inconclusive evidence to suggest whether side-to-side differences between dominant and non-dominant limbs can be detrimental to the injury risk of patients [8]. Postural control mechanisms for single limb landings are more likely to employ multiple postural control mechanisms simultaneously such as the ankle and hip mechanisms [9]. Contrary to Wang and Fu, [8] a study of female volleyball players postulated that single-leg jump landing tests of dominant versus non-dominant limbs could predispose athletes to the injury risk of one limb over the other. The authors found the responses between the two limbs do indeed vary in landing strategies with dominant limbs exhibiting less effective landing strategies and awkward postures compared to non-dominant limbs predisposing athletes to higher injury risks of their dominant limbs [10]. We asked whether interlimb differences in balance as it pertains to postural control can be identified, as in the study described with landing mechanics, then the opportunity to counteract these balance deficits might be possible before individuals experience increased fall risk. In addition, as described above in athletes, different populations present with varying levels of altered postural control. For example, in a study by Rosario, it was discovered individuals living with human immunodeficiency virus have an impaired total postural sway creating a need for more extensive therapeutic interventions compared to healthy counterparts (2020).
The emergence of balance board training has elicited multiple inquiries into their ability to identify and treat postural control impairments. Interestingly, it has been suggested that balance board training might be able to challenge motor and postural control strategies, which include heavy reliance on visual fields due to visual tracking components often associated with balance board training, such as the Wii Fit Balance Board [11]. Additionally, in a study by Rosario et al. [12], balance board training with a fixed fulcrum was found to provide neuromuscular advantages not previously seen in stationary balance boards, such as the Wii Fit Balance Board. Rosario and colleagues’ [12] balance board with a fixed fulcrum is identical to the M-PAD balance board used in the current query with the hopes to discover the effects on postural control mechanisms.
With the above referred to in mind, the current examination intends to answer the following questions: What are the postural patterns rotating to the left compared to the right while balancing on a balance platform? Further, do people with right leg dominance balance differently than those with left leg dominance? This examination seeks to answer these questions by determining the postural patterns of young adults during rotational balance activities on a fulcrum board. We hypothesize that individuals with right limb dominance will demonstrate decreased clockwise sway (sway in right rotation), whereas individuals with left limb dominance will demonstrate decreased counterclockwise sway (sway in left rotation).
Methods
All subjects were enrolled from the Texas Woman’s University (TWU) Dallas campus and nearby areas by word of mouth from a research team member. All participants signed the approved informed consent documents after being instructed about their role in the investigation by a research team member. The researcher then collected the subjects' demographic information (age, sex, weight, and height).
As inclusion criteria, the current study recruited adults, males, or females, within the ages of 18-45 years old to avoid common age-related differences in balance and posture. The exclusion criteria for this study were as follows: 1. serious balance problems (inability to maintain balance for 30 seconds with eyes closed); 2. Untreated severe visual acuity, 3. surgeries or traumas within the prior six months; and 4. drugs that provoke drowsiness 24 h prior to taking part in this study; 5. Women who are pregnant or believe they are pregnant.
Measures
Data were obtained using MobilityLab APDM MobilityLabTM (APDM WEARABLE TECHNOLOGIES INC. 2828 S Corbett Avenue, Suite 135, Portland, OR 97201, APDM Inc., http://apdm. com). MobilityLab uses a set of gyroscope and accelerometer movement sensors that are placed using straps to estimate the movement, distance, direction, and velocity of sway. More specifically, for this investigation, the lumbar sensor was used in isolation to calculate medial-lateral (ML) and anterior-posterior (AP) sway velocity, direction, and distance. The sensor was placed at the level of the third lumbar vertebrae found via palpation of the participant’s twelfth rib which was followed to the twelfth thoracic vertebrae, then to the third lumbar vertebrae. The use of this specific sensor and location has been previously discussed and published by other studies with diverse populations, such as asymptomatic individuals living with human immunodeficiency virus, healthy young adults, and healthy young adults during caffeine consumption [12-16].
Balance Assessment
Each participant wore a lumbar Mobility Lab sensor for testing. Postural sway was examined during the four balance activities. Before the balance protocol, leg dominance was assessed by perturbation. The perturbation consisted of asking participants to look at a fixed mark on the wall. Subsequently, a research member pulled participants from behind (without warning them) from both shoulders simultaneously. The extremity used to adapt to the perturbation (step back) was considered the dominant leg for that subject.
All balance tests were performed at a distance of 10 feet from a TV screen mounted on the wall at approximately 6 feet from the ground. First, after placing the lumbar sensor, participants were instructed to stand on their right leg for 20 s while looking at a fixed target (orange circle) on the TV screen. The same procedure was repeated on the left-hand side.
The second part of the balance test consisted of participants standing on an M-PAD balance board. This M-PAD balance board is a specially designed fixed fulcrum board with adjustable foot placements. The fulcrum on this board is fixed and allows for users to rotate freely while standing in a bipedal stance. The fulcrum height of the M-PAD balance board was at the lowest height from the ground for all participants. The M-PAD balance board was placed approximately 6 feet from the TV, as in the previous tests. As researched by Rosario et al. [12,15], this balance board with a fixed middle fulcrum is effective for examining postural sway with rotational components. The visual tracking factor of the balance task was achieved by projection to the TV 6 feet in front of participants through Apple Airplay via the M-PAD cellular device application interface. The tracking component consisted of participants looking directly ahead while standing on the M-PAD balance board while following a gray ball in a clockwise and counterclockwise direction with an orange ball counterpart controlled by their lower extremities. Participants were instructed to track the gray ball with their eyes in an attempt to keep the orange ball on top of the gray one, in tracking motion. The participants were able to control the direction the gray ball went due to the cellular phone being adhered to the balance platform between the feet. The gyroscopes within the phone are able to detect spatial movement created by the participant. The balance tasks consisted of clockwise (CW tracking rotation to the right) and counterclockwise (CCW-tracking rotation to the left) activities. Each task was 15 s long with a 10-second practice interval preceding each activity to allow participants time to become acquainted with the apparatus. Each rotational task (clockwise and counterclockwise) was performed one time in a bipedal stance with the freedom to move freely within the trunk and upper extremities to maintain balance. If participants required to remove one foot from the M-PAD balance platform, participants were instructed to recenter themselves on the platform and begin again.
Data Analysis
All data gathering transpired at the TWU Dallas. A spreadsheet organizing mediolateral (ML) and anteroposterior (AP) sway velocity, direction, and distance were provided by the Mobility Lab software. These variables were then organized for all participants in a spreadsheet for single-leg balance (left and right) and rotational tasks (CW and CCW). The current study performed various MANOVA comparisons for sway, AP-ML jerk, AP-ML velocity and AP-ML distance during: 1) left versus right single limb balance, 2) base on leg dominance, CW versus CCW rotation, and 3) difference between CW and CCW rotations. A P-value of ≤ 0.05, was deemed significant in this investigation.
Results
Participants: A total of 70 participants, 7 males and 63 females between the ages of 22 and 32 (average age 25 ± 4.66 SD) completed this study. Their average BMI was 24.34 +/-2.71. Table 1 shows the demographic data of all the participants. Table 1 shows the demographic profiles of the participants. Of the 70 participants, 37 were left-leg dominant, and the remaining 32 were right-leg dominant.
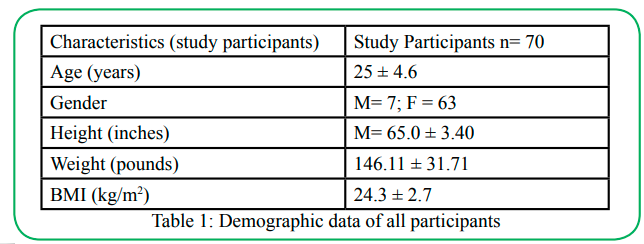
Table 1:Demographic data of all participants
Table 2 shows the comparisons of the right single-limb stance versus the left single-limb stance. Sway data exhibited similarities in single-limb support, regardless of extremity (P>0.05). Table 3 shows a comparison of clockwise rotations versus counterclockwise rotations. The results showed a significant increase in sway in the anteroposterior (AP) direction while rotating towards the left or CCW. Additionally, there was an increase in the distance in the AP direction during CCW rotation (P<0.05). No significant differences were observed in any other variables.
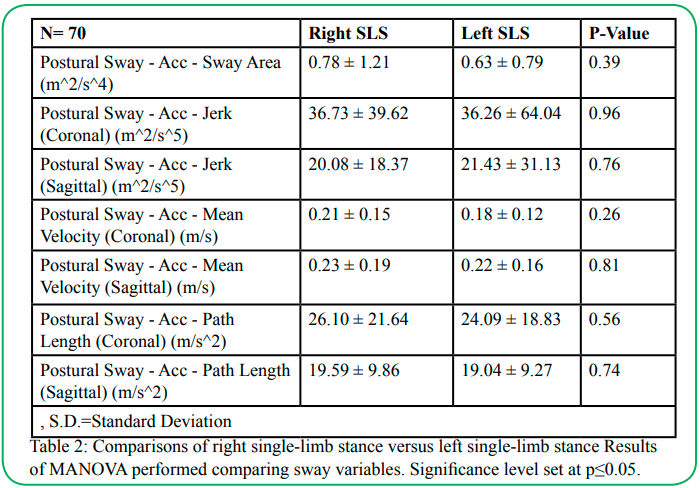
Table 2:Comparisons of right single-limb stance versus left single-limb stance Results of MANOVA performed comparing sway variables. Significance level set at p≤0.05.
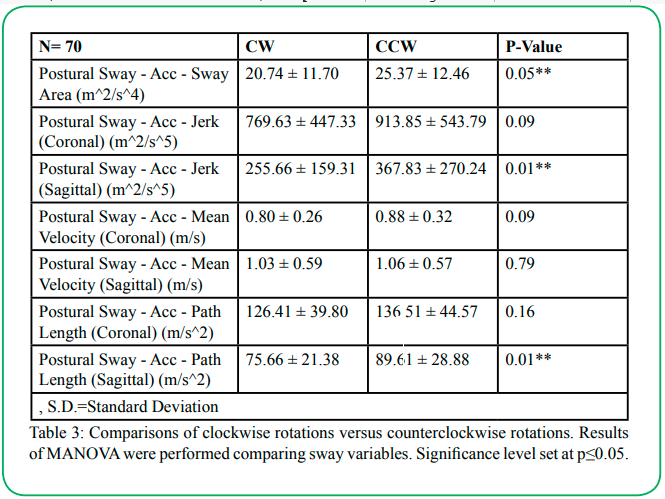
Table 3:Comparisons of clockwise rotations versus counterclockwise rotations. Results of MANOVA were performed comparing sway variables. Significance level set at p≤0.05.
Table 4 illustrates the comparison of right leg dominant versus left leg dominant during CW rotation. The data showed a significantly increased sway and distance of sway in the ML direction (P<0.05) for individuals with right-leg dominance when compared to their left-leg dominant counterparts during CW rotations. The other variables were comparable between the groups. Table 5 shows the comparison of right leg dominant versus left leg dominant during CCW rotations. The results showed compatibility for all variables (P>0.05).
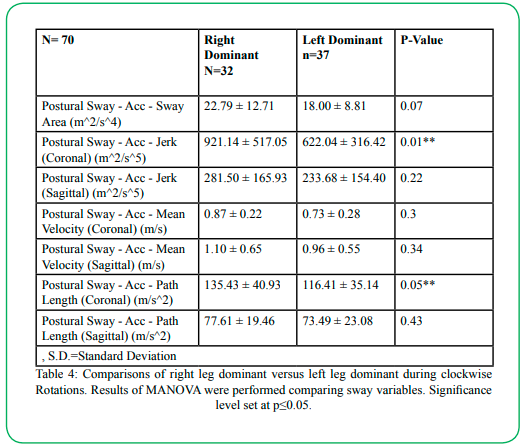
Table 4: Comparisons of right leg dominant versus left leg dominant during clockwise Rotations. Results of MANOVA were performed comparing sway variables. Significance level set at p≤0.05.
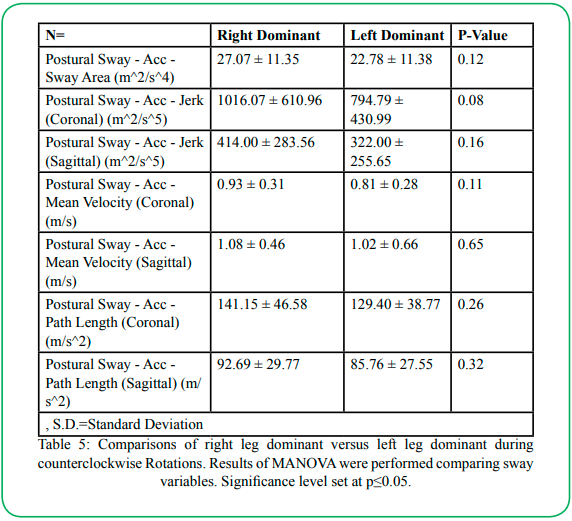
Table 5:Comparisons of right leg dominant versus left leg dominant during counterclockwise Rotations. Results of MANOVA were performed comparing sway variables. Significance level set at p≤0.05.
Discussion
The current examination intends to answer the following questions: What are the distinct postural patterns rotating to the left compared to the right while balancing on a balance platform? Additionally, do people with right leg dominance balance differently than those with left leg dominance?
The first main finding of this study showed similarities during single-limb (SL) support between the bilateral lower extremities (dominant or non-dominant). These findings are comparable to those of Alonso et al. [17], who found no differences between dominant and non-dominant in SL balancing tasks on a Biodex balancing system in 40 healthy young males. Similarly, an earlier study conducted by Alonso et al. [18] using the Biodex balancing system on 64 young and healthy soccer players found no asymmetries in either lower extremities in injured soccer players or sedentary individuals during monopedal balancing activities. However, a recent systematic review examining factors that facilitate or prohibit postural variations among limbs found such differences to be context-dependent [19]. Furthermore, the authors suggested that singular factors should not be enough to affect postural control during single-limb stance activities between the lower extremities; for example, fatigue should be considered in combination with environmental or experimental factors to produce postural asymmetries between dominant and non-dominant. The review by Paillard and Noé [19] raises the concern that our environmental or testing conditions were not challenging enough to elicit interlimb differences; however, our findings are in agreement with both the Alonso et al. studies mentioned above that no asymmetries exist between dominant and non-dominant.
Our secondary main outcome exhibited increased movement or sway in the AP direction in individuals rotating toward the left or counterclockwise condition. To our knowledge, there has only been one other publication examining postural sway during rotations on fixed fulcrum balance boards [15]. However, a study performed with varying balance board fulcrum heights in healthy young adolescents found a positive correlation between postural sway in the ML direction and higher fulcrum heights [20]. These findings are consistent with the findings of Rosario et al. [15], who evaluated sway during balance on a fixed fulcrum balance board at varying vertical heights. Similar to our findings, researchers discovered that with increased task complexity (rotation movements), an increased postural sway was provoked in both medial-lateral and antero-posterior directions [15]. This discovery is important because of its potential implications for activities of daily living. For instance, a simple daily task of looking both ways before approaching a street crossing is vital to daily functioning, but if CCW rotational movements are difficult for the individual, then this simple task could elevate the fall risk of this individual before initiation of the crossing [21]. Since counterclockwise conditions provoke AP sway, prospective studies should examine hip musculature engagement during these challenging activities. Knowing the muscle activation pattern is the next step in understanding motor control with a rotational component.
Lastly, our third main result demonstrated increased sway in the ML direction for individuals with right-leg dominance when compared to their left-leg dominant counterparts during clockwise rotations. As mentioned previously, Rosario et al. [15] reported similar findings with increased ML velocity or sway during all tasks, which included clockwise and counterclockwise movements, when compared to AP sway. The inquiry did not delve into inter-extremity differences, but we can infer from these findings that the possible mechanism of differences stems from right-leg dominant individuals having a preferential turning pattern (motor behavior) toward the counterclockwise direction exhibited with increased sway in the opposite direction (clockwise). This interpretation is supported by Promsri et al. ’s [22] analysis of physically active young adults during balance training to deduce leg dominance influences motor behavior during bipedal stance on an unstable balance board. Thus, our proposed explanation of the ML sway increases seen in right-leg dominant individuals in the clockwise direction is a result of established and preferred motor behaviors formed over time in the counterclockwise direction. Further research is needed to prove or disprove this proposition via muscle activity analysis during clockwise and counterclockwise balancing tasks.
Conclusion
In summation, our initial premise that, as a whole, individuals with left versus right leg dominance will balance differently was disproved, similar to previous studies looking into the same concept [17,18]. However, we successfully found significant differences in the ability of individual tasks, such as counterclockwise rotations, to elicit increased sway in the ML direction. Additionally, we found that individuals with right leg dominance had an increased difficulty in maintaining stable sway in the AP direction during clockwise rotational movements. Future studies could delve into neuromuscular adaptations during similar rotational movements. Professionals studying and treating balance should consider assessing the rotational aspects of their clients’ balance to understand possible stability deficits.
Conflicts of interest:
The authors declare no conflict of interest.
Ethics approval:
Texas Woman’s University IRB approval, protocol # 20092
Authors' contributions:
All authors contributed equally to the study conception and design.
References
Pollock, A. S., Durward, B. R., Rowe, P. J., & Paul, J. P. (2000). What is balance? Clinical Rehabilitation, 14(4), 402-6. doi:http://dx.doi.org.ezp.twu.edu/10.1191/0269215500cr342oaView
Haddas, R., & Lieberman, I. H. (2017). A method to quantify the “cone of economy.” European Spine Journal, 27(5), 1178– 1187. https://doi.org/10.1007/s00586-017-5321-2View
Shumway-Cook, A., & Woollacott, M.H. (2007). Motor control: Translating research into clinical practice. (6th ed.) Philadelphia: Lippincott Williams & Wilkins. APAView
Ivanenko, Y. P., Levik, Y. S., Talis, V. L., & Gurfinkel, V. S. (1997). Human equilibrium on unstable support: the importance of feet-support interaction. In Neuroscience Letters (Vol. 235, Issue 3, pp. 109–112). Elsevier BV. https://doi.org/10.1016/ s0304-3940(97)00721-0View
Silva, P., Mrachacz-Kersting, N., Oliveira, A., & Kersting, U. (2018). Effect of wobble board training on movement strategies to maintain equilibrium on unstable surfaces. Human Movement Science, 58, 231-238.View
Yoshida, T., Ikemiyagi, F., Ikemiyagi, Y., Tanaka, T., Yamamoto, M., & Suzuki, M. (2014). The dominant foot affects the postural control mechanism: examination by body tracking test. Acta Oto-Laryngologica, 134(11), 1146–1150. https://doi.org/10.31 09/00016489.2014.940556View
Schorderet, C., Hilfiker, R., & Allet, L. (2021). The role of the dominant leg while assessing balance performance. A systematic review and meta-analysis. Gait & Posture, 84, 66–78. https:// doi.org/10.1016/j.gaitpost.2020.11.008View
Wang, J., & Fu, W. (2019). Asymmetry between the dominant and non-dominant legs in the lower limb biomechanics during single-leg landings in females. Advances in Mechanical Engineering, 11(5),168781401984979. https://doi. org/10.1177/1687814019849794View
Zhou, H., Xu, D., Chen, C., Ugbolue, U. C., Baker, J. S., & Gu, Y. (2021). Analysis of Different Stop-Jumping Strategies on the Biomechanical Changes in the Lower Limbs. Applied Sciences, 11(10), 4633. doi:10.3390/app11104633View
Sinsurin, K., Srisangboriboon, S., & Vachalathiti, R. (2017). Side-to-side differences in lower extremity biomechanics during multi-directional jump landing in volleyball athletes. European journal of sport science, 17(6), 699–709. https://doi.org/10.108 0/17461391.2017.1308560View
Murray, N. G., Fernandez, E., Salvatore, A. P., & Reed-Jones, R. J. (2016). Assessment of the Wii Basic Balance Test in measuring postural deficits post-concussion. Journal of clinical and translational research, 2(4), 123–128.View
Rosario, M., Bowman, C., Versemann, A., Heistand, D. (2021a). The Impact of a Rotating Balance Platform on Leg Neuromuscular Activity in Healthy Young Adults. Internal Journal of Sports Medicine and Rehabilitation, 22. https://doi. org/10.28933/ijsmr-2021-04-0505View
Correa, A., Hanrahan SPT, C., Basye SPT, L., & Rosario, M. G. (2021). Energy Drinks May Improve Postural Sway While Provoking an Early Onset of Muscle Fatigue. Journal of Public Health Issues and Practices., doi: hdoi.org/10.33790/ jphip1100176. [Spring]
Rosario, M. G. (2020). Lower Limb Neuromuscular Modification and Standing Postural Control Alteration in Apparent Asymptomatic People Living with HIV. Journal of Rehabilitation Practices and Research., doi: https://doi. org/10.33790/jrpr1100102.
Rosario, M., Bowman, C., Versemann, A., & Heistand, D. (2021b). The Impact of a High/Low Fulcrum Rotating Balance Platform on Standing Postural Stability in Healthy Young Adults. Journal of Sports Research, 8(1), 8–15. https://doi. org/10.18488/journal.90.2021.81.8.15View
Rosario, M. G., & Jose, A. (2021c). Anteroposterior and mediolateral postural adaptations during single and duals tasks in healthy young adults. International Journal of Physical Education, Fitness and Sports., doi: https://doi.org/10.34256/ ijpefs2139.
Alonso, A. C., Brech, G. C., Bourquin, A. M., & Greve, J. M. D. (2011). The influence of lower-limb dominance on postural balance. Sao Paulo Medical Journal, 129(6), 410–413. https:// doi.org/10.1590/s1516-31802011000600007View
Alonso, A. C., Greve, J. M., & Camanho, G. L. (2009). Evaluating the center of gravity of dislocations in soccer players with and without reconstruction of the anterior cruciate ligament using a balance platform. Clinics (Sao Paulo, Brazil), 64(3), 163–170. https://doi.org/10.1590/s1807-59322009000300003View
Paillard, T., & Noé, F. (2020). Does monopedal postural balance differ between the dominant leg and the non-dominant leg? A review. Human Movement Science, 74, 102686. https://doi. org/10.1016/j.humov.2020.102686View
Gebel, A., Lüder, B., & Granacher, U. (2019). Effects of Increasing Balance Task Difficulty on Postural Sway and Muscle Activity in Healthy Adolescents. Frontiers in physiology, 10, 1135. https://doi.org/10.3389/fphys.2019.01135View
Lee, S. W., Verghese, J., Holtzer, R., Mahoney, J. R., & Oh-Park, M. (2014). Trunk sway during walking among older adults: Norms and correlation with gait velocity. Gait & Posture, 40(4), 676–681. Available at: https://doi.org/10.1016/j. gaitpost.2014.07.023.View
Promsri, A., Haid, T., Werner, I., & Federolf, P. (2020). Leg Dominance Effects on Postural Control When Performing Challenging Balance Exercises. Brain Sciences, 10(3), 128. https://doi.org/10.3390/brainsci1003012View