
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 3 (2022), Article ID: JRPR-130
https://doi.org/10.33790/jrpr1100130Research Article
Influence of Chronic Pain on Cardiovascular and Locomotor Components in Hispanic-Latinos Living with HIV
Martín G. Rosario PT*, PhD, CSFI, ATRIC, Elizabeth Orozco, PT, DPT
Physical Therapy Program, Texas Woman’s University, Dallas Campus; Texas, United States.
Corresponding Author Details: Martín G. Rosario PT, PhD, CSFI, ATRIC, Assistant Professor, Texas Woman’s University, Physical Therapy Program, Dallas Campus, 5500 Southwestern Medical Ave. Dallas, TX 75235-7299. United States. E-mail: mrosario1@twu.edu
Received date: 11th December, 2021
Accepted date: 31th December, 2021
Published date: 03rd January, 2022
Citation: Rosario, M.G., & Orozco, E. (2022). Influence of Chronic Pain on Cardiovascular and Locomotor Components in Hispanic-Latinos Living with HIV. J Rehab Pract Res, 3(1):130.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Chronic pain is commonly reported in people living with the human immunodeficiency virus (HIV). Chronic pain has been linked to decreased quality of life, mobility impairments, and increased risk of cardiovascular complications in the general population. Therefore, the purpose of this study was to determine the relationship between chronic pain and cardiovascular and locomotor function in people living with HIV (PLWH).
Subjects: A total of 291 participants were enrolled in this study, 251 without chronic pain (non-CP), and 40 participants with chronic pain (CP). Both groups were comparable in terms of age and years of diagnosis.
Methods: Data was collected retrospectively from a community-based exercise program in San Juan, Puerto Rico from 2000-2020. The cardiovascular and motor components of this study were collected using the Ross submaximal cardiovascular test. The presence of chronic pain and Cd4 count was collected by interview and results from the participants’ most recent blood work.
Results: For the cardiovascular component, the CP group demonstrated significantly reduced heart rate (p<.05), systolic blood pressure (p<.05), and time completed on the Ross test (p<.001). The motor component portrayed by gait velocity and treadmill inclination was significantly reduced in the CP group (p<.05).
Conclusion: This study found that the presence of chronic pain in PLWH negatively affected locomotor and cardiovascular function. More research is needed to investigate the differences in lower extremity muscular activation and spatiotemporal parameters that could be associated with a reduction in gait speed and inclination in PLWH and chronic pain.
Keywords: HIV, Cardio-Motor, Gait, Walking, Treadmill, Treadmill Assessment
Introduction
Over 36.9 million individuals worldwide are living with the human immunodeficiency virus (HIV) [1]. According to the Center of Disease Control (CDC), there are more than 1.2 million people living with HIV (PLWH) in the United States [2]. Approximately 46% of PLWH reside in the southern part of the United States, with Texas and Puerto Rico being among the top seven locations with the highest incidence rates of the infection. Therefore, it was to be expected that the number of HIV infections would be more prevalent among Hispanic/Latino males, with infection rates of this population exceeding four times the amount seen in white males within the United States and its territories (www.cdc.gov).
While the incidence of HIV infections continues to rise, the advancement and availability of antiretroviral therapies (ART) has allowed for this population to live close to average life spans. However, this increase in life expectancy has been accompanied by the presence of comorbidities secondary to HIV infection, such as chronic inflammation, side effects of antiretroviral medications, and lifestyle factors often seen in PLWH [3,4]. With this, age-related illnesses including cardiovascular disease, kidney disease, liver disease, osteoporosis, sarcopenia, and neurocognitive impairments typically emerge earlier in PLWH than in seronegative age-matched controls [5].
Chronic pain is defined as pain that persists for more than three months [6] and is one of the most commonly reported comorbidities among PLWH. In fact, previous studies have found that more than 50% of PLWH will experience chronic pain at some point in their lifetime and that the prevalence of chronic pain in this population may be as high as 83% [7,8]. A systematic review that included 61 studies by Parker et al. [8] found that PLWH reported chronic pain that was moderate to severe in intensity and occurred in more than one anatomical location. The etiology of chronic pain in this population is multifactorial and has been attributed to chronic inflammation, neurotoxic effects of the virus on the nervous system, side effects of antiretroviral medications, and psychological distress. Neuropathic and musculoskeletal pain are among the most common types of pain experienced by this population [6,7].
While there is a high prevalence of chronic pain in PLWH, previous studies have found that pain is under-managed in this population and is more difficult to treat as a result of ART side effects, higher rates of psychiatric disorders, and the increased risk of substance abuse. For example, while opioids have been used for long-term management of chronic pain, the use of opioids is not recommended for PLWH due to the greater risk of substance abuse among this population [8,9]. Though non-pharmacological management treatments such as physical therapy, behavioral therapy, and cognitive therapy are less common, they continue to emerge for the treatment of chronic pain in PLWH.
Like most comorbidities, chronic pain has been associated with decreased quality of life, greater physical impairment, difficulty with completing activities of daily living, and increased depressive symptoms [10,11]. A systematic review by Vancamport et al. [12] found that while lower levels of physical activity were found to be associated with bodily pain and that this relationship is strengthened when coupled with depressive symptoms, bodily pain itself was a common barrier to physical activity in PLWH. Additionally, low levels of physical activity and greater physical impairment have been associated with poor cardiovascular fitness and slower gait speed in this population [13], though the effects of chronic pain on cardiovascular and locomotor function remains unknown. Therefore, the aim of this study was to determine how chronic pain influences cardiovascular function and locomotor components in PLWH. We hypothesize that PLWH and chronic pain will exhibit a poor cardiovascular profile and reduced locomotor outcomes, possibly due to decreased activity levels secondary to pain.
Methods
All data used in this study was retrospectively collected from the records of participants who were enlisted and participated in the community-based exercise program at La Perla de Gran Precio in San Juan Puerto Rico from the year 2000 to 2020. The main focus of the La Perla de Gran Precio (LPGP) community center is to promote wellness and aid in improving quality of life for Hispanic Latino individuals living with HIV through exercise therapy. As previously published by Orozco and Rosario [14] the protocol included a variety of strengthening, cardiovascular and stretching exercises. The exercise protocol was designed for a one hour 3 times a week routine, tailored to each participants to meet intensity requirements. This study was approved by LPGP and the privacy and confidentiality standards established by the organization were followed.
All subjects were cleared to participate in the community center by their primary physician, who was responsible for monitoring the progression of their patients’ HIV disease. Participants were evaluated by a physical therapist prior to any further involvement in the fitness center, followed by a certified personal trainer who administered a submaximal aerobic fitness test, known as the Ross treadmill test. The Ross test is a requirement of the LPGP and a pre-exercise tool to participate in the program in addition to capture a cardio-motor baseline of each subject.
As part of the LPGP requirements, all participants brought their current lab work and performed a series of exercise tests. Demographic information and the presence of chronic pain were collected by interview, whereas cd4 count was retrieved from the most recent lab report. For this study, chronic pain was defined as pain lasting for more than three months. Cardiovascular and motor components were collected using the Ross submaximal cardiovascular test.
Motor and Cardiovascular components:
The current study follows the Ross protocol used in previous studies by Rosario et al. [15] and Rosario et al. [16], which also recruited PLWH. Data retrieved from participants' records for this study included heart rate and blood pressure for the cardiovascular components and gait velocity and inclination for the motor components. Vitals were collected prior to cardiovascular testing, afterwhich the Ross treadmill test started with participants walking at a 2.0 mph speed and a 0% inclination. The Ross test is designed to gradually increase to a speed of 3.4 mph and inclination of 15% at 21 minutes. The test stopped when the 21 minute mark was achieved, maximal cardiac frequency was reached, when participants reported fatigue or lower limb pain.
The cardiovascular data reported in this study were the values found at the end of the Ross treadmill test.
Data Analysis
This study performed an analysis of variance (ANOVA) with SPSS version 25 to compare the two groups, those with chronic pain and those with no chronic pain. Based on the diagnosis of CP, 251 participants were allocated to the Non-CP and 40 to the CP group. The two constituents collected and compared among groups were the cardiovascular and motor components. Cardiovascular components included heart rate, blood pressure, and time completed on the Ross test. The motor components included gait velocity and treadmill inclination. In the current study, a P value of 0.05 or less was considered significant.
Results
To ascertain the association mentioned above, participant data were allocated into two groups prior to comparing the values of the cardiovascular and motor components: 1) 251 participants without chronic pain (non-CP), and 2) 40 participants with chronic pain (CP).
Table 1 depicts the demographic information of the participants in this study. The non-CP and CP groups were comparable in age (non-CP =53.20+/-10.60 years and CP=54.20 +/7.80 years), years of diagnosis (Non-CP 18.60+/-8.30 and CP 20.40+/-9.50), and sex ratio, with the majority being males. Regarding cd4 count, the non-CP group had a lower cd4 count at 604.4+/329.2 compared to the CP group 816.7+/- 439.1.
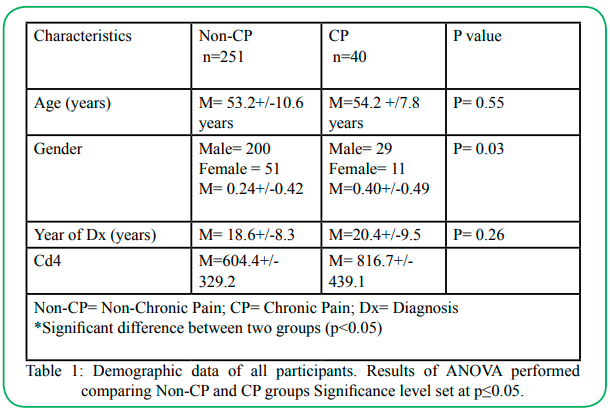
Table 1 : Demographic data of all participants. Results of ANOVA performed comparing Non-CP and CP groups Significance level set at p≤0.05.
Cardiovascular and motor components: Table 2 shows the differences in cardiovascular and motor factors between the two groups. The CP group exhibited significantly reduced heart rate (p<.05), systolic blood pressure (p<.05), and time completed on the Ross test (p<.001) in comparison to the non-CP group. Diastolic blood pressure was comparable between the two groups (p>.05). The motor component portrayed by gait velocity and treadmill inclination (as seen in Table 2) was significantly reduced in the CP group (p<.05).
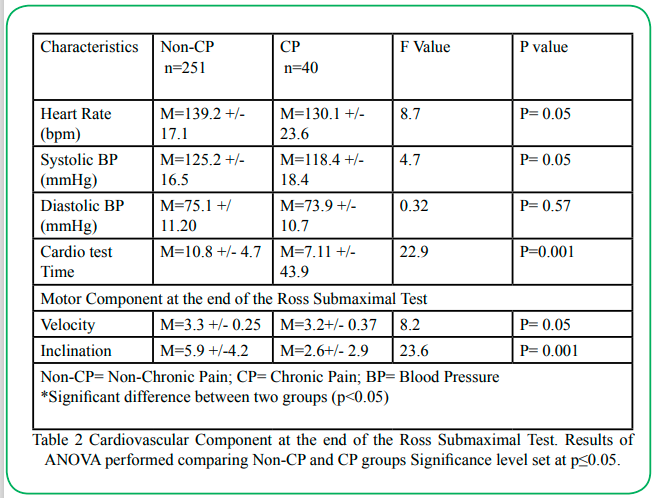
Table 2: Cardiovascular Component at the end of the Ross Submaximal Test. Results of ANOVA performed comparing Non-CP and CP groups Significance level set at p≤0.05.
Discussion
This study aimed to identify differences in cardiovascular and motor components secondary to chronic pain in people living with HIV. This study found that velocity, inclination, and time completed on the Ross test were significantly lower in the group with chronic pain. To our knowledge, this is the first study to investigate cardiovascular and motor components in individuals living with HIV accompanied by chronic pain. The study results were aligned with our hypothesis that participants with chronic pain would present with reduced cardiovascular and motor function; therefore, we accept our previously stated premise.
Motor Component: Our first main outcome focused on the time completed on the Ross test; the chronic pain group completed approximately 3-4 minutes less than the group without chronic pain. While both groups performed relatively lower than the standard of the test, the performance of the CP group was significantly inferior, demonstrating a magnified impairment in cardiovascular function. Similar findings have been discovered in people with chronic low back pain, as reported in the study by Smeets et al. [17] which identified that men with chronic low back pain performed worse during a submaximal test than age-matched healthy controls, indicating reduced cardiovascular fitness levels in the chronic pain group. It has also been reported that people with chronic pain are more likely to be deconditioned and present with deficits in strength [18,19].
Pain has been well documented in the literature as a barrier to physical activity in PLHIV, which would explain the lower times observed during the submaximal exercise test in this study [20]. However, one limitation of our study is that we were unable to assess whether pain was a contributing factor to the termination of the submaximal test rather than decreased aerobic fitness levels, alone, indicating the need for further research to clarify whether pain is a limiting factor in exercise testing. In addition, we support the participation of PLWH in aerobic exercise to improve the physiological and psychological aspects of chronic pain, as it is known that aerobic exercise increases blood flow throughout the body, enhancing the delivery of oxygen and other nutrients to the joints and surrounding muscles. In addition, aerobic exercise facilitates the release of endorphins, which can help reduce pain and improve mood [21]. Therefore, we recommend that people living with HIV and chronic pain participate in regular aerobic exercise to improve the cardiorespiratory fitness and pain reduction necessary in maintaining or improving functional performance.
The second main finding in this study was the significant reduction in gait speed during the Ross test in the chronic pain group. The previous report suggests that PLWH exhibit changes in neuromuscular function in the form of gait deficits, resulting in adaptations such as a decrease in gait speed. Similar findings of decreased gait speed have been reported in people experiencing neuropathic pain from diabetes and individuals with musculoskeletal pain [22,23]. A study by Lalli et al. [24] found that individuals with neuropathic pain secondary to diabetes mellitus demonstrated decreased step length and gait speed in comparison to those without neuropathic pain, indicating that the presence of pain is a contributor to slower gait speed. Similarly, Sawa et al. [23] found that moderate to severe pain was associated with slower gait speed in community-dwelling older adults who experienced chronic musculoskeletal pain.
As previously mentioned, neuropathic and musculoskeletal pain are the most common types of chronic pain experienced by people living with HIV [6,7]. The presence of neuropathy is associated with pain and damage to the sensory and motor nerves, which can affect dynamic stability, resulting in slower gait speed [22]. It is also known that musculoskeletal pain can alter gait mechanics and lead to compensation elsewhere, requiring greater energy expenditure with gait and decreasing gait speed. Therefore, it was expected that the CP group would experience a slower gait speed in our study.
Since the data in this study was collected retrospectively, we were unable to distinguish between types of chronic pain (i.e., neuropathic or musculoskeletal) experienced in our sample and how chronic pain affects gait mechanics (i.e., step length, cadence, etc.), making these factors limitations to our research. Gait speed is an important measure of functional mobility and has been shown to detect functional decline in people living with HIV [25]. Our study demonstrated that the presence of chronic pain can negatively affect gait; however, further investigation is needed to determine if there is a difference in gait speed based on the type of pain present in this population and which components of gait are most affected by the presence of chronic pain.
The third main finding of this study was a reduction in the treadmill inclination during the Ross test. Treadmill inclination mimics real ground walking and the difficulty increases with the angle of inclination [26,27], therefore this decrease in grade of inclination implies a lack of surface adaptability in relation to chronic pain. Previous studies have shown that walking at an incline requires increased joint range of motion at the hip, knee, and ankle, along with greater activation of the quadriceps, hamstrings, and gastrocnemius muscles [28-30]. While our study did not examine joint mechanics and muscle activation, we investigated whether pain can affect the level of inclination that can be achieved during a submaximal test. To the best of our knowledge, this is the first study to compare the level of inclination achieved during a submaximal test in people with and without chronic pain. Since inclined walking requires a greater range of motion and further muscle activation, we expected that the CP group would achieve less inclination on the Ross Test than the group without CP. One study found that people with chronic low back pain presented with impaired motor control of the lumbopelvic muscles and demonstrated a more stiff and guarded posture while walking [31]. Therefore, a reduction in range of motion and deficits in motor control would make it difficult to withstand the challenge of walking up an inclined surface.
As mentioned earlier, because this data was collected retrospectively, one limitation of this study is that it was not recorded whether pain due to inclination was a reason for termination of the Ross Test. Further research is needed to determine whether a lack of range of motion or poor muscle activation secondary to pain are reasons for the reduced inclination achieved during a submaximal exercise test. Additionally, there is insufficient information to identify the mechanisms that affect motor control in PLWH, therefore, gait training and assessment under various conditions, such as compliant surfaces, hills, and ramps that challenge the lower extremity musculature and the cardiorespiratory system, are encouraged for this population.
Cardiovascular component: The fourth main finding in our study demonstrated heart rate and systolic blood pressure were significantly reduced during the Ross Test in the CP group. Since the CP group completed less time on the Ross test, one possible explanation is that the CP group was less likely to achieve a higher heart rate and systolic blood pressure in comparison to the non-CP group, indicating potential deficiencies in cardiorespiratory fitness. It is important to point out that our study assessed heart rate and blood pressure achieved at the termination of the Ross test rather than with the addition of resting blood pressure data, which may have allowed for the identification other factors, such as an increase in systolic blood pressure in the CP group compared to the non-CP group, leading to other associations. For instance, research has shown a positive correlation between chronic pain and hypertension [32], and various studies have focused on the cardiovascular components of PLHIV and established an association between having the HIV disease and cardiovascular dysfunction, particularly diastolic dysfunction [33]. Our findings indicate that pain may also be a contributing factor to cardiovascular function in PLHIV, potentially negatively affecting cardiorespiratory fitness. A recent systematic review and meta-analysis by Fayaz et al. [34] found that the presence of chronic pain may be associated with an increased risk of cardiovascular disease.
However, since this study measured blood pressure at the termination of the Ross test, we were unable to adequately identify a physiological explanation for our findings, therefore making the previous report a limitation of this research. Future studies should consider investigating how resting blood pressure compares between the two groups to better understand whether hypertension is more prevalent in the CP group. Furthermore, we encourage heart rate monitoring and the utilization of target heart rates tailored to aerobic interventions during all stages of the disease. Similar to previous studies, we recommend frequent cardiopulmonary assessments in PLHIV to reduce the occurrence of cardiovascular complications in this population [35,36].
Conclusion
The aim of this study was to determine whether there was a relationship between chronic pain, cardiovascular function, and motor components in PLWH. Our study found that pain may negatively influence gait, resulting in a reduction in gait speed and possible alterations in neuromuscular activation that create difficulties in walking up inclined surfaces. Additionally, this study found that the presence of chronic pain may negatively affect cardiorespiratory fitness, as evidenced by a reduction in time completed on the submaximal test, along with reductions in heart rate and blood pressure. The major limitation of this study was that the data was collected retrospectively, which created barriers to determining the presence of and extent to the following in accordance with our data: if the submaximal test was terminated due to pain, the type of pain experienced in this sample, if spatiotemporal factors were affected by the presence of pain, and whether resting blood pressure and heart rate were significantly different between the CP and non-CP groups.
Therefore, future studies should consider investigating the difference in lower extremity muscle activation in the presence of pain when walking on an even surface in comparison to an inclined surface. Similarly, spatiotemporal measures of gait should be collected and compared to determine how pain affects different components of gait speed, such as cadence, stride length, and double limb support time versus single limb support time. This information would further explain the differences in gait speed and inclination observed in the current study. Regarding the cardiovascular component, more research is preferred to determine whether hypertension and tachycardia are prevalent at rest in the presence of PLWH and chronic pain. In addition to the aforementioned, further evidence is needed to understand how pain affects cardiorespiratory fitness levels. If lower extremity pain or low back pain was the reason for termination of the test, a submaximal test utilizing an upper extremity ergometer may be more appropriate for aerobic testing in those with both HIV and chronic pain.
The findings of this study provide clinicians with a general understanding of how chronic pain can affect locomotor and cardiovascular function in people living with HIV. Chronic pain should be considered when assessing gait to better understand the differences observed in the mechanics and spatiotemporal parameters secondary to alterations induced by pain. Lastly, clinicians should be aware of the presence and cause of chronic pain in their patients who have HIV in order to effectively and comprehensively tailor gait and aerobic training to reduce pain and ultimately improve function.
Competing interests:
The authors report no conflict of interest.
References
Global HIV & AIDS statistics — 2018 fact sheet http://www. unaids.org/en/resources/fact-sheet Accessed [January 2019].View
HIV in the United States by Region. https://www.cdc.gov/hiv/ statistics/overview/geographicdistribution.html Accessed [May 2021].View
Allavena, C., Hanf, M., Rey, D., Duvivier, C., BaniSadr, F., Poizot-Martin, I., Jacomet, C., Pugliese, P., Delobel, P., Katlama, C., Joly, V., Chidiac, C., Dournon, N., Merrien, D., May, T., Reynes, J., Gagneux-Brunon, A., Chirouze, C., Huleux, T., Cabié, A., Dat’AIDS study group (2018). Antiretroviral exposure and comorbidities in an aging HIV-infected population: The challenge of geriatric patients. PloS one, 13(9), e0203895. https://doi.org/10.1371/journal.pone.0203895.View
Vancampfort, D., Mugisha, J., Rosenbaum, S., Firth, J., De Hert, M., Probst, M., & Stubbs, B. (2016). Cardiorespiratory fitness levels and moderators in people with HIV: A systematic review and meta-analysis. Preventive medicine, 93, 106–114. https:// doi.org/10.1016/j.ypmed.2016.10.001. View
Berner, K., Morris, L., Baumeister, J., & Louw, Q. (2017). Objective impairments of gait and balance in adults living with HIV-1 infection: a systematic review and meta-analysis of observational studies. BMC musculoskeletal disorders, 18(1), 325. https://doi.org/10.1186/s12891-017-1682-2.View
Merlin, J. S., Long, D., Becker, W. C., Cachay, E. R., Christopoulos, K. A., Claborn, K., Crane, H. M., Edelman, E. J., Harding, R., Kertesz, S. G., Liebschutz, J. M., Mathews, W. C., Mugavero, M. J., Napravnik, S., C OʼCleirigh, C., Saag, M. S., Starrels, J. L., & Gross, R. (2018). Brief Report: The Association of Chronic Pain and Long-Term Opioid Therapy With HIV Treatment Outcomes. Journal of acquired immune deficiency syndromes (1999), 79(1), 77–82. https://doi. org/10.1097/QAI.0000000000001741. View
Madden, V. J., Parker, R., & Goodin, B. R. (2020). Chronic pain in people with HIV: a common comorbidity and threat to quality of life. Pain management, 10(4), 253–260. https://doi. org/10.2217/pmt-2020-0004.View
Parker, R., Stein, D. J., & Jelsma, J. (2014). Pain in people living with HIV/AIDS: a systematic review. Journal of the International AIDS Society, 17(1), 18719. https://doi. org/10.7448/IAS.17.1.18719.View
Addis, D. R., DeBerry, J. J., & Aggarwal, S. (2020). Chronic Pain in HIV. Molecular Pain. https://doi. org/10.1177/1744806920927276.View
Merlin, J. S., Westfall, A. O., Chamot, E., Overton, E. T., Willig, J. H., Ritchie, C., Saag, M. S., & Mugavero, M. J. (2013). Pain is independently associated with impaired physical function in HIV-infected patients. Pain medicine (Malden, Mass.), 14(12), 1985–1993. https://doi.org/10.1111/pme.12255.View
Uebelacker, L. A., Weisberg, R. B., Herman, D. S., Bailey, G. L., Pinkston-Camp, M. M., & Stein, M. D. (2015). Chronic Pain in HIV-Infected Patients: Relationship to Depression, Substance Use, and Mental Health and Pain Treatment. Pain medicine (Malden, Mass.), 16(10), 1870–1881. https://doi.org/10.1111/ pme.12799.View
Vancampfort, D., Mugisha, J., Richards, J., De Hert, M., Probst, M., & Stubbs, B. (2018). Physical activity correlates in people living with HIV/AIDS: a systematic review of 45 studies. Disability and rehabilitation, 40(14), 1618–1629. https://doi.or g/10.1080/09638288.2017.1306587.View
Mbada, C. E., Onayemi, O., Ogunmoyole, Y., Johnson, O. E., & Akosile, C. O. (2013). Health-related quality of life and physical functioning in people living with HIV/AIDS: a case-control design. Health and quality of life outcomes, 11, 106. https://doi. org/10.1186/1477-7525-11-106. View
Orozco, E., & Rosario, M.G. (2020). Overall fitness benefits in individuals with HIV participating in a community-based exercise program. J Rehab Pract Res 1(2):109. https://doi. org/10.33790/jrpr1100109
Rosario, M.G., Gines, G., Jamison, L. (2020). Lifestyle, Physical and Cardiovascular Components Associated with Immune Profile in Hispanic-Latino People Living with HIV. J Ment Health Soc Behav 2(1):121. https://doi.org/10.33790/ jmhsb1100121.
Rosario, M.G, Jamison, L., & Gines, G. (2021). Motor and Cardiovascular Distinctions among genders in Hispanic-Latinx People Living with HIV. International Journal of Physiotherapy, 8(1), 64-69. https://doi.org/10.15621/ijphy/2021/v8i1/909.
Smeets, R. J., Wittink, H., Hidding, A., & Knottnerus, J. A. (2006). Do patients with chronic low back pain have a lower level of aerobic fitness than healthy controls?: are pain, disability, fear of injury, working status, or level of leisure time activity associated with the difference in aerobic fitness level?. Spine, 31(1), 90-97. View
Verbunt, J. A., Seelen, H. A., Vlaeyen, J. W., van de Heijden, G. J., Heuts, P. H., Pons, K., & Knottnerus, J. A. (2003). Disuse and deconditioning in chronic low back pain: concepts and hypotheses on contributing mechanisms. European journal of pain, 7(1), 9-21.View
Van der Velde, G., & Mierau, D. (2000). The effect of exercise on percentile rank aerobic capacity, pain, and self-rated disability in patients with chronic low-back pain: a retrospective chart review. Archives of Physical Medicine and Rehabilitation, 81(11), 1457-1463. View
Gray, L., Schuft, L., Bergamaschi, A., Filleul, V., Colson, S. S., & d’Arripe-Longueville, F. (2019). Perceived barriers to and facilitators of physical activity in people living with HIV: A qualitative study in a French sample. Chronic Illness. https:// doi.org/10.1177/1742395319826638. View
Hayden, J. K., Keegan, M., Kardong-Edgren, S., & Smiley, R.A. (2014). Reliability and validity testing of the Creighton Compe tency Evaluation Instrument for use in the NCSBN National Sim ulation Study. Nursing Education Perspectives (in press). doi:10.5480/13-1130.1View
Alam, U., Riley, D. R., Jugdey, R. S., Azmi, S., Rajbhandari, S., D'Août, K., & Malik, R. A. (2017). Diabetic Neuropathy and Gait: A Review. Diabetes therapy : research, treatment and education of diabetes and related disorders, 8(6), 1253–1264. https://doi.org/10.1007/s13300-017-0295-y. View
Sawa, R., Doi, T., Misu, S., Saito, T., Sugimoto, T., Murata, S., Asai, T., Yamada, M., & Ono, R. (2017). The severity and number of musculoskeletal pain associated with gait in community-dwelling elderly individuals. Gait & posture, 54, 242–247. https://doi.org/10.1016/j.gaitpost.2017.03.013. View
Lalli, P., Chan, A., Garven, A., Midha, N., Chan, C., Brady, S., Block, E., Hu, B., & Toth, C. (2013). Increased gait variability in diabetes mellitus patients with neuropathic pain. Journal of diabetes and its complications, 27(3), 248–254. https://doi. org/10.1016/j.jdiacomp.2012.10.013.View
Schrack, J. A., Althoff, K. N., Jacobson, L. P., Erlandson, K. M., Jamieson, B. D., Koletar, S. L., Phair, J., Ferrucci, L., Brown, T. T., Margolick, J. B., & Multicenter AIDS Cohort Study (2015). Accelerated Longitudinal Gait Speed Decline in HIV-Infected Older Men. Journal of acquired immune deficiency syndromes (1999), 70(4), 370–376. https://doi.org/10.1097/ QAI.0000000000000731.View
Boldt A. What Incline on a Treadmill Is the Same As a Flat Surface? SportsRec. https://www.sportsrec.com/156224-what-incline-on-a-treadmill-is-the-same-as-a-flat-surface.html. Published October 15, 2019. Accessed April 28, 2020.
Lee, S. J., & Hidler, J. (2008). Biomechanics of overground vs. treadmill walking in healthy individuals. Journal of applied physiology (Bethesda, Md. : 1985), 104(3), 747–755. https:// doi.org/10.1152/japplphysiol.01380.2006.View
McIntosh, A. S., Beatty, K. T., Dwan, L. N., & Vickers, D. R. (2006). Gait dynamics on an inclined walkway. Journal of biomechanics, 39(13), 2491–2502. https://doi.org/10.1016/j. jbiomech.2005.07.025.View
Lange, G. W., Hintermeister, R. A., Schlegel, T., Dillman, C. J., & Steadman, J. R. (1996). Electromyographic and kinematic analysis of graded treadmill walking and the implications for knee rehabilitation. Journal of Orthopaedic & Sports Physical Therapy, 23(5), 294-301.View
Franz, J. R., & Kram, R. (2012). The effects of grade and speed on leg muscle activations during walking. Gait & posture, 35(1), 143–147. https://doi.org/10.1016/j.gaitpost.2011.08.025.View
Koch, C., & Hänsel, F. (2018). Chronic Non-specific Low Back Pain and Motor Control During Gait. Frontiers in psychology, 9, 2236. https://doi.org/10.3389/fpsyg.2018.02236. View
Saccò, M., Meschi, M., Regolisti, G., Detrenis, S., Bianchi, L., Bertorelli, M., Pioli, S., Magnano, A., Spagnoli, F., Giuri, P. G., Fiaccadori, E., & Caiazza, A. (2013). The relationship between blood pressure and pain. Journal of clinical hypertension (Greenwich, Conn.), 15(8), 600–605. https://doi.org/10.1111/ jch.12145. View
Oursler, K. K., O'Boyle, H. M., Briggs, B. C., Sorkin, J. D., Jarmukli, N., Katzel, L. I., Freiberg, M. S., & Ryan, A. S. (2019). Association of Diastolic Dysfunction with Reduced Cardiorespiratory Fitness in Adults Living with HIV. AIDS patient care and STDs, 33(12), 493–499. https://doi.org/10.1089/ apc.2019.0149.View
Fayaz, A., Ayis, S., Panesar, S. S., Langford, R. M., & Donaldson, L. J. (2016). Assessing the relationship between chronic pain and cardiovascular disease: A systematic review and meta-analysis. Scandinavian journal of pain, 13, 76–90. https://doi.org/10.1016/j.sjpain.2016.06.005. View
Erqou, S., Lodebo, B. T., Masri, A., Altibi, A. M., Echouffo-Tcheugui, J. B., Dzudie, A., Ataklte, F., Choudhary, G., Bloomfield, G. S., Wu, W. C., & Kengne, A. P. (2019). Cardiac Dysfunction Among People Living With HIV: A Systematic Review and Meta-Analysis. JACC. Heart failure, 7(2), 98–108. https://doi.org/10.1016/j.jchf.2018.10.006. View
Rosario, M.G. and Gonzalez-Sola, M. (2018). Autonomic nervous system assessment in people with HIV: A cross-sectional study [version 1; referees: awaiting peer review]. F1000 Research., doi: 10.12688/f1000research.14685.1.View