
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 3 (2021), Article ID: JRPR-134
https://doi.org/10.33790/jrpr1100134Research Article
Initiation of Body Segment Reorientation in Steering is not Altered While Dual Tasking
V.N. Pradeep Ambati1*, Guillermo Escalante1, Fabricio Saucedo2, Ivy Garcia-Guevara1, & Rebecca Reed-Jones3
1Department of Kinesiology, College of Natural Sciences, California State University, San Bernardino,United States.
2Department of Kinesiology, Division of Education, Human Development and Social Sciences, Penn State Altoona, United States.
3Department of Applied Human Sciences, Faculty of Science, University of Prince Edward Island, United States.
Corresponding Author Details: Venkata Naga Pradeep Ambati, PhD, Assistant Professor, College of Natural Sciences, California State University, San Bernardino,United States.
Received date: 04th August, 2022
Accepted date: 22nd August, 2022
Published date: 24th August, 2022
Citation: Ambati, V.N.P., Escalante, G., Saucedo, F., Reed-Jones, R., & Garcia-Guevara, I., (2022). Initiation of Body Seg-ment Reorientation in Steering is not Altered While Dual Tasking. J Rehab Pract Res, 3(1):134.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Changing the direction of locomotion, often referred to as “steering”, is an integral component of human locomotion. This study sought to investigate the role of cognition in steering using a dual task paradigm in healthy young and healthy older adults. Twenty-five healthy young adults and nineteen healthy older adults completed a 900 walking turn at a comfortable pace under single and dual task conditions. Dependent variables included the time taken to turn and the turn onset of the head, trunk, and pelvis segments. Results indicate dual tasking increases the time taken to turn but does not alter the sequence of initiation of segment reorientation into the turn. The effects of aging on these behaviors were minimal. Most notable was that the older adults did not slow their turns as much as the young adults did during dual tasking. These results suggest that initiation of segment reorientation is independent of cognitive influence but that increased cognitive load is considered when planning movement time.
Keywords: Steering; Turning; Adaptive Locomotion; Older Adults; Dual Task;
Introduction
An important component of human locomotion is the ability to adapt to the environment. Redirecting walking direction (a.k.a. steering) is a commonly performed activity that allows an individual to go around obstacles, turn corners, and avoid collisions [1-6]. Unfortunately, steering is also a movement that creates substantial difficulty in populations with reduced mobility. In particular, difficulties in steering coordination occur in older adults with a history of falls [7-9], individuals who have survived a stroke [10,11], and individuals with Parkinson’s disease [12,13].
Of recent interest in understanding steering control, is the role of cognition in the execution of turning. This is of great importance as humans rarely move in the environment without performing concurrent cognitive tasks (e.g., carrying on a conversation either in person or on a mobile telephone). Little research has addressed this question, but research has indicated a significant role of cognition in the planning and execution of turning tasks [14]. In particular, increased time to turn and adoption of more cautious gait parameters (e.g., wider step width and increased single support time) have been observed in older adults and stroke survivors while steering under a dual task paradigm [14]. Dual task paradigms challenge attention capacities by performing a secondary cognitive task while simultaneously performing a primary motor task. When two stimuli require processing at the same time, a “bottleneck” arises, resulting in a delay of one of the responses [15]. The hypothesis regarding dual tasking in gait is that if gait is an automatic activity that does not require deliberate attention, then dual tasking will not affect gait parameters. However, if dual tasking affects gait parameters, then some level of attention is required by the gait task itself. We used a similar hypothesis to examine the role of cognition in steering.
A critical component in studying steering coordination is the onset of segment reorientation at the initiation of the redirection. Segment reorientation is well defined in steering control literature [3,5,6-16-19] and disruption to the sequence is a significant indicator of steering difficulties [9,13]. Therefore, to better understand the role of cognition in steering control we must know how cognitive load influences the sequence of body segment reorientation.
The purpose of the current study was to measure the sequence of reorientation of the body segments in steering control under a dual task paradigm. The current study examined steering control in a group of healthy young adults and a group of healthy older adults to understand whether the healthy aging process affects the interaction of steering control and cognitive load. We hypothesized that if steering requires significant attentional resources, participants would increase turn time and display a significant delay in the turn onset of body segment reorientation under dual task conditions. In addition, we expected that older adults might also display interruption to the sequence of body segment reorientation. Specifically, the body may reorient as a single unit (en-bloc) because of a need to simplify motor control under a dual task condition. Use of this strategy would indicate that cognitive decline associated with healthy aging [20] influences the ability to coordinate the body’s segments during turning activities.
Materials and Methods
Participants
Twenty-five healthy young adults and nineteen healthy older adults participated in the study (Table 1 provides demographics). Sample size was determined using G power 3.1 with a set α level of 0.05, with a medium effect size (0.25) determined from prior research findings [16,21-24], with a desired β of 0.20 and a correlation value among the dependent variables of 0.50 [21].
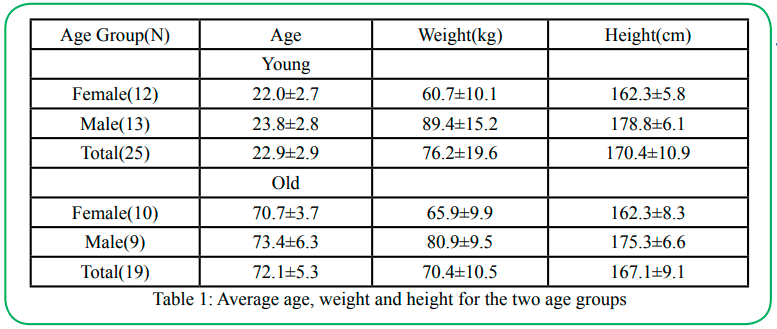
Table 1: Average age, weight and height for the two age groups
A general health questionnaire [25] was administered prior to inclusion in the study to ensure healthy volunteers were free of any neurological disorders (e.g., vertigo and hearing disorders) and did not have any medical conditions that contraindicated participating in the study (e.g., heart conditions). Human participant ethics approval was obtained from the University of Texas at El Paso and all participants provided informed written consent (IRB Reference # 521597-2).
Study design
The study used an ABCA-ACBA control group design with independent variables task condition (TASK) and age group (AGE). Dependent variables included the time taken to complete the turn (Turn Time) and rotation onset of the body segments. To determine the effects of TASK participants performed three types of activities. (A) baseline motor task where participants walked and made a 90o turn; (B) dual task where participants walked and made a 90o turn while performing serial 7 subtractions out loud; (C) single task serial 7 subtractions performed out loud for 45 seconds while sitting (approximately the time to finish the walking and turning task). The score on the single task serial 7 (C) was used to control for differences in the participants’ individual ability to perform serial 7 subtractions. Evaluation of performance on serial 7 subtractions was obtained by subtracting the number of mistakes from the number of subtractions made in the given time. To control for practice and fatigue affects, the order of B and C were counterbalanced between the research participants.
Procedures
Prior to the experimental trials, participants walked on a straight path with maximum length 5 meters (5 trials). Data from straight path walking trials were used to determine the turn onset of body segments as per previously published methods [16,21].
The experimental trials involved walking along a straight path and redirecting the walking trajectory to the right or left (90o) around a marker placed in the center of the walkway. To control for effects due to turn direction both right (5 trials) and left turns (5 trials) were randomized. Participants were instructed to walk at their normal pace. The instructions for the dual task condition (B) were to walk and make a 900 turn at a comfortable pace while performing the serial 7 subtractions out loud. No instruction for priority of tasks was given.
Experimental design
The single task condition (A) was performed before and after the dual task condition for all participants to control for threats to internal validity such as fatigue, testing and practice effects. The dual task condition significantly increased turning times in both YA and OA (Fig. 1). In addition, turn time returned to baseline following the dual task condition (Fig. 1). These results point to the strong effect of the dual task on turn time and support that the effects observed in the study were not due to fatigue or testing and practice effects. As the two A conditions were not statistically different, they were collapsed for further analysis.
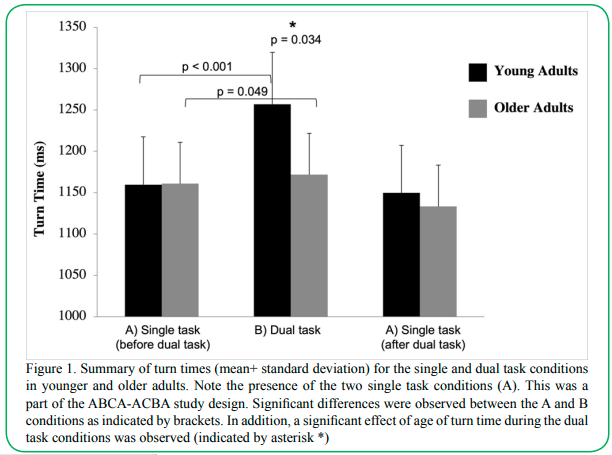
Figure 1. Summary of turn times (mean+ standard deviation) for the single and dual task conditions in younger and older adults. Note the presence of the two single task conditions (A). This was a part of the ABCA-ACBA study design. Significant differences were observed between the A and B conditions as indicated by brackets. In addition, a significant effect of age of turn time during the dual task conditions was observed (indicated by asterisk *)
The serial 7s score obtained from the single cognitive task condition (C) was intended as a covariate for statistical analysis to control for differences in the participants’ ability to perform the serial 7 subtractions while sitting. One of the assumptions of covariate analysis is that the covariate must have a linear relationship with the dependent variables [26]. On preliminary analysis, serial 7 scores had no significant relationship to the dependent variables, and therefore were not included in further statistical analysis.
Measures and instrumentation
Three-dimensional kinematic data (120 Hz) was collected using an eight-camera motion capture system (Vicon, Oxford, UK). A whole body marker configuration as per the Plug-In gait model was used (Vicon Oxford, UK). Analysis of segment kinematics focused on rotations about the yaw axis (vertical axis) to define reorientation into the turn. Data reduction was performed as per previously published methods [16]. Onset of rotation for the head, trunk, and pelvis segments in milliseconds were dependent variables. In addition, turn time was calculated from one-step prior to one-step following the turn.
Statistical Analysis
Mixed model repeated measures MANOVAs determined the effects of the independent variables TASK and AGE on the rotation onsets of the head, trunk and pelvis segments and on turn time. Within-subjects variable TASK (two levels: single motor task (A) and dual task (B)) and between-subjects variable AGE (two levels: young adults (YA) and older adults (OA)). Post-hoc analysis was conducted using Bonferroni pairwise test.
Results
Effects of age and task condition on turning time
A significant interaction effect of TASK and AGE on turning time was found (F (1, 42) = 6.419, p = 0.015, η2= 0.127). This result indicates that the dual task condition affected the turn time differently in the young and older adult groups. Further post-hoc one-way ANOVA examined the effects of AGE for each TASK independently. For the single motor task condition (A), no significant difference in turn time due to AGE was found (F (1, 42) = 0.116, p = 0.734) (Fig. 1). For the dual task condition (B), a statistically significant difference due to AGE was observed (F (1, 42) = 4.816, p = 0.034). The younger adults took a greater amount of time to turn when compared to the older adults in the dual task condition (Fig. 1).
Effects of age and task condition on turn onsets of the head, trunk, and pelvis
No significant interaction of TASK and AGE on the turn onset of the head, trunk and pelvis segments was found (F (4, 39) = 2.397, p = 0.067). However, a significant main effect of AGE on the turn onsets of the segments was observed (F (4. 39) = 3.293, p = 0.020, η2 = 0.252). Based on this main effect, we examined the effects of AGE on segment onset for the single motor task (A) and dual task (B) independently.
Effects of task condition on the turn onsets in healthy young adults
No significant effect of TASK was observed for turn onsets of eyes, head, trunk and pelvis in healthy young adults. (F (4, 21) = 0.774, p = 0.555). Thus, the dual task condition did not affect the turn onset of the head, trunk and pelvis in young adults (Fig. 2).
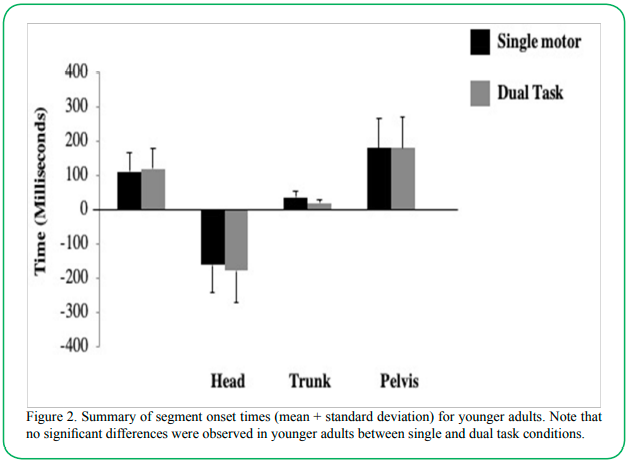
Figure 2. Summary of segment onset times (mean + standard deviation) for younger adults. Note that no significant differences were observed in younger adults between single and dual task conditions.
Effects of task condition on the turn onsets in healthy older adults
A significant main effect of TASK was observed for turn onset of the head, trunk and pelvis in healthy older adults (F(4,15) = 5.077, p = 0.008, η2=0.559). Bonferroni corrected pair-wise comparisons revealed significant differences in the turn onsets of head, trunk, and pelvis (Fig. 3). Thus, the dual task condition affected the turn onsets of various body segments in the older adult group.
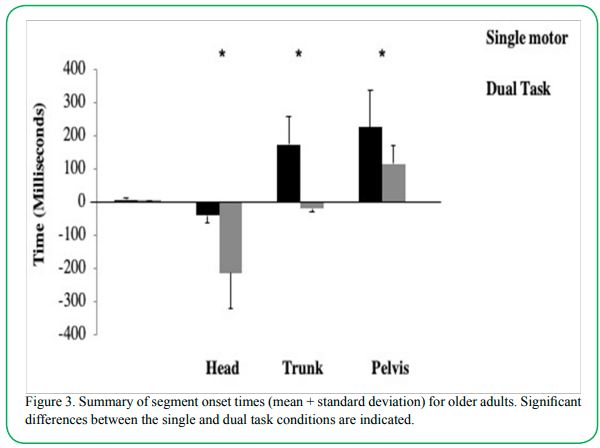
Figure 3. Summary of segment onset times (mean + standard deviation) for older adults. Significant differences between the single and dual task conditions are indicated.
Discussion
The purpose of this study was to determine whether dual tasking influences body segment coordination during walking turns (a.k.a. steering) in healthy younger and older adults. Overall, the results of the study did not support our hypotheses that dual tasking delays segment reorientation. In contrast, while turn time increased during dual tasking (Fig. 1), segment coordination was unaltered by the dual task condition (Fig. 2). In addition, older adults did not display interruption to segment control under dual task conditions suggesting that cognitive decline associated with healthy aging does not influence the ability to coordinate the body’s segments during turning activities (Fig. 3). The most notable difference between the two age groups was that older adults completed the turn more quickly overall than younger adults.
Effects of age on steering under single motor task conditions
Under single motor task performance, there were few differences between steering behavior in young and older adults. Turn time was not significantly different between the young and older adult groups (Fig. 1). While turn onset times of the head, trunk and pelvis in older adults occurred later when compared to younger adults, only the trunk onset time was statistically significant. Delayed segment reorientation suggests older adults tend to take more time to plan segment coordination when available, however; it is unlikely this is critical to their steering control, as increased delays were not observed under dual task conditions.
Effects of dual tasking on steering in healthy young adults
Under dual task conditions, healthy young adults took significantly longer to complete the turn, however; there were no differences in the timing of when the body segments began reorientation to the new direction of travel (Figs. 2). Findings of increased time to complete a task are consistent with previous literature on the effects of dual tasking on gait in young adults. Specifically, reduced velocity may be a strategy to account for increased processing time of sensory information under increased cognitive load [27-31]. The most significant finding of this study is that while younger adults increased turn time while dual tasking, the initiation of body segments remained unaltered. These results suggest that the sequence of segment movement occurs independently of cognitive influence. These conclusions support the hypotheses that body segment coordination is a synergy type system belonging to phylogenetically old neural mechanisms and is a basic component of the human locomotor repertoire [2,17,21].
Effects of dual tasking on steering in healthy older adults
Turn onset for the head, trunk and pelvis segments occurred earlier in the dual task condition for older adults (Fig. 3). The time taken to turn was also significantly increased when dual tasking, however not to the extent that was observed in younger adults (Fig. 1). In fact, when comparing segment initiation between older and younger adults, it was during the dual task condition that the older adults’ onset of body segment rotation closely resembled those observed in young adults (Fig. 2 & 3). This finding was counter to what we hypothesized.
It was hypothesized that older adults might display greater disruption to steering control compared to younger adults in the dual task condition. A number of studies have reported a decline in motor task performance in healthy older adults due to dual tasking [32-35]. However, this was not the case in the current study. In fact, the older adults’ steering control became more reflective of the younger adults’ control while dual tasking. A potential reason for this result could be that dual tasking forced older adults to pay more attention to their steering task. Older adults have been found to prioritize stability of gait when walking and performing a cognitive task using a “posture first” strategy to avoid hazards and prevent falls while walking [28,30,36]. It might be that the older adults in the current study, although they were not asked to, prioritized the steering task over the serial 7 subtractions task. A ‘posture first’ strategy could also help to explain the faster turn times, when compared to YA turn times, of OA in the dual task condition. This observation may indicate a tendency to rush the movement in order to perform both tasks.
Overall, this is the first study to examine the role of attention in the top-down control of body segment coordination of steering in a healthy young and older adult group. The results of this study provide evidence that initiation of body segment coordination during steering is not influenced by cognitive load but that cognitive load may have influence during the planning of movement time. Increased time to turn is a strategy adopted to account for the increase in sensory information processing and motor planning as a result of increased cognitive load [27-31]. This is a significant finding and provides a substantial addition to the current literature on steering control. In addition, the current study suggests that the healthy aging process does not significantly alter the amount of cognitive involvement in steering control. However, this finding should be interpreted with due caution, as these results do not suggest that cognitive impairment does not affect steering control. In particular, the older adults involved in this study represented a group that were recreationally active and did not have any mobility difficulties. As such, further study of the effects of dual taking on steering control in older adult groups with mobility difficulties and/or measured cognitive impairments would be valuable. In conclusion, the results of the current study provide evidence that investigating steering control under dual task paradigms may provide greater insight into the neurological mechanisms that sub-serve steering control.
Declaration of Interest:
No potential conflict of interest.
Acknowledgements
The authors would like to thank Dr. Ashley Bangert and Dr. Deborah Diaz for their guidance with statistical analysis and dual tasks. We would also like to acknowledge Dr. Sandor Dorgo for his assistance with participant recruitment. We would also like to thank the participants for their contributions to the study. Support for this study was provided by the College of Health Sciences, University of Texas at El Paso (V.N.P. Ambati).
References
Vallis, L.A., & McFadyen, B.J. (2003). Locomotor adjustments for circumvention of an obstacle in the travel path. Experimental Brain Research, 152, 409-414.View
Grasso, R., Prevost, P., Ivanenko, Y P., & Berthoz, A. (1998). Eye-head coordination for the steering of locomotion in humans: an anticipatory synergy. Neuroscience Letters, 253, 115-118.View
Patla, A.E., Adkin, A., & Ballard, T. (1999). Online steering: coordination and control of body center of mass, head and body reorientation. Experimental Brain Research, 129, 629-634.View
Courtine, G., & Schieppati, M. (2003). Human walking along a curved path. I. Body trajectory, segment orientation and the effect of vision. European Journal of Neuroscience, 18, 170- 190.View
Reed-Jones, R., & Vallis, L. (2007). Proprioceptive deficits of the lower limb following anterior cruciate ligament deficiency affect whole body steering control. Experimental Brain Research, 182(2), 249-60.View
Hollands, M.A., Sorensen, K.L., & Patla, A.E. (2001). Effects of head immobilization on the coordination and control of head and body reorientation and translation during steering. Experimental Brain Research, 140, 223-233.View
Paquette, M., Fuller, J., Adkin, A., & Vallis, L. (2008). Age-related modifications in steering behavior: effects of base-of-support constraints at the turn point. Experimental Brain Research, 190, 1-9.View
Thigpen, M., Light, K., Creel, G., & Flynn, S. (2000). Turning difficulty characteristics of adults aged 65 years or older. Physical Therapy, 80(12), 1174-87.View
Wright, R.L., Peters, D.M., Robinson, P.D., Sitch, A.J., Watt, T.N., Hollands, M.A. (2012) Differences in axial segment reorientation during standing turns predict multiple falls in older adults. Gait & Posture 36(3):541–545.View
Lamontagne, A., Paquette, C., & Fung, J. (2007). Stroke affects the coordination of gaze and posture during preplanned turns while walking. Neurorehabilitation and Neural Repair, 21, 62- 67.View
Hollands, K., Hollands, M., Zietz, D., Wing, A., Wright, C., & Vliet, P. (2010). Kinematics of turning 180° during the timed up and go in stroke survivors with and without falls history. Neurorehabilitation and Neural Repair, 24(4), 358-367.View
Stack , E., & Ashburn, A. (1999). Fall events described by people with parkinson's disease: implications for clinical interviewing and the research agenda. Physiotherapy Research International, 4, 190-200.View
Hong, M., Perlmutter, J. S., & Earhart, G. M. (2009). A Kinematic and Electromyographic Analysis of Turning in People With Parkinson Disease. Neurorehabilitation and Neural Repair, 23(2), 166-176.View
Hollands, K., Agnihotri, D., Tyson, S.F. (2014) Effectsd of dual task on turning ability in stroke survivors and older adults. Gait & Posture 40, 564-69.View
Pashler, H. (1994). Dual-task interference in simple tasks: Data and theory. Psychological Bulletin, 116(2), 220-244.View
Ambati, V. N. P., Murray, N. G., Saucedo, F., Powell, D. W., & Reed-Jones, R. (2013). Constraining eye movement when redirecting walking trajectories alters turning control in healthy young adults. Experimental Brain Research 226, 549–556.View
Hollands, M.A., Ziavra, N.V., & Bronstein, A.M. (2004). A new paradigm to investigate the roles of head and eye movements in the coordination of whole-body movements. Experimental Brain Research, 154, 261-266.View
Fuller, J. R., Adkin, A. L., & Vallis, L. A. (2007). Strategies used by older adults to change travel direction. Gait & Posture, 25, 393-400. View
Akram, S. B., James, S. F., & Fraser, J. (2010). Effect of walking velocity on segment coordination during pre-planned turns in healthy older adults. Gait & Posture, 32(2), 211-214.View
Milham, M. P., Erickson, K. I., Banich, M. T., Kramer, A. F., Webb, A., & Wszalek, T. (2002). Attentional control in the aging: Insights from an fmri study of the stroop task. Brain and Cognition, 49, 277-296. View
Reed-Jones, R.J., Hollands, M.A., Reed-Jones, J.G., & Vallis, L.A. (2009). Visually evoked whole-body turning responses during stepping in place in a virtual environment. Gait Posture, 30, 317-321.View
Springer, S., Giladi, N., Peretz, C., Yogev, G., Simon, E. S., & Hausdroff, J. M. (2006). Dual-tasking effects on gait variability: The role of aging, falls, and executive function. Movement Disorder, 21(7), 950-7.View
Shkuratova, N., Morris, M., & Huxham, F. (2004). Effects of age on balance control during walking. Archives of Physical Medicine and Rehabilitation, 85, 582-588.View
Dubost, V., Kressig, R., & Gonthier, R. (2006). Relationships between dual task related changes in stride velocity and stride time variability in healthy older adults. Human Movement Science, 25, 372-382.View
Goldberg, D. P., & Williams, P. (1988). A user's guide to the General Health Questionnaire. Slough: NFER-Nelson.View
Stevens, J. (1992). Applied multivariate statistics for the social sciences. (2 ed., p. 458). Hillsdale, New Jersey: Lawrence erlbaum associates.View
Ebersbach, G., Dimitrijevic, M., & Poewe, W. (1995). Influence of concurrent tasks on gait: a dual task approach. Perceptual and Motor Skills, 81, 107-113.View
Lindenberger, U., Marsiske, M., & Baltes, P. (2000). Memorizing while walking: increase in dual task costs from young adulthood to old age. Psychology and Aging, 15, 417-436.View
Li, K., Lindenberger, U., Freund, A., & Baltes, P. (2001). Walking while memorizing: age related differences in compensatory behavior. Psychology and Aging, 12, 230-237.View
Bloem, B., Valkenburg, V., Slabbekoorn, M., & Willemsen, M. (2001). The multiple task test: development and normal strategies. Gait & Posture, 14, 191-202.View
Weerdesteyn, V., Schillings, A., Van Galen, G., & Duysens, J. (2003). Distractions affects the performance of obstacle avoidance during walking. Journal of Motor Behavior, 35, 53- 63. View
Faulkner, K., Redfern, M., & Rosano, C. (2006). Reciprocal influence of concurrent walking and cognitive testing on performance in older adults. Gait Posture, 24, 182-189.View
Coppin, A., Shumway-Cook, A., & Saczynski, J. (2006). Association of executive function and performance of dual-task physical tests among older adults: analyses from the inchianti study. Age Ageing, 35, 619-624.View
Hausdroff, J. M., Schweiger, A., Talia, H., Yogev-Seligmann, G., & Giladi, N. (2008). Dual-task decrements in giat: contributing factors among healthy older adults. Journal of Gerontology, 63A(12), 1335-1343.View
Verghese, J., Kuslansky, G., & Holtzer, R. (2007). Walking while talking: effect of task prioritization in the elderly. Archives of Physical Medicine and Rehabilitation, 88, 50-53.View
Gérin-Lajoie, M., Richards, C. L., & McFadyen, B. J. (2006). The circumvention of obstacles during walking in different environmental contexts: a comparison between older and younger adults. Gait & Posture, 24(3), 364-369.View