
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 3 (2022), Article ID: JRPR-137
https://doi.org/10.33790/jrpr1100137Research Article
Effect of Education and Support on Stress and Wellbeing of Caregivers of Persons with a Stroke
Sanchala K. Sen, OTD, MS, OTR/L, BCPR,
Assisant Professor, Department Occupational Therapy, Winston-Salem State University, Winston-Salem, NC, USA.
Corresponding Author Details: Sanchala K. Sen, OTD, MS, OTR/L, BCPR, Assisant Professor, Department Occupational Therapy, Winston-Salem State University, Winston-Salem, NC, USA.
Received date: 17th August, 2022
Accepted date: 10th October, 2022
Published date: 12th October, 2022
Citation: Sen, S. K., (2022). Effect of Education and Support on Stress and Wellbeing of Caregivers of Persons with a Stroke. J Rehab Pract Res, 3(2):137.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The purpose of this study was to identify the level of burden and quality of life of family caregivers of persons affected by a stroke and further examine if an occupational therapy-led education would assist in alleviating stress and improving the overall perception of well-being. The project used a mixed quantitative and qualitative pretest-posttest design with a small convenience sample of seven family caregivers of persons with stroke. Caregivers were educated on strategies for caregiving and wellbeing for self in a group format. Caregivers who completed the 6-week educational modules indicated decreased stress and improved perceptions of wellbeing in themselves. The study outcomes support the use of education to assist caregivers in balancing their life by taking care of their health and well-being. This conclusion emphasizes the need for a structured educational program for caregivers in addition to the primary interventions to the care recipients.
Keywords: Caregiver Burden, Quality of Life, Group Support, Educational Modules, Life Balance
Introduction
Strokes occur suddenly and can be life-changing for both the patient and family. Informal caregivers such as family members provide most long-term care to survivors of stroke and play an important role in post stroke rehabilitation. Informal caregivers are typically defined as those persons who care for family members in their or their family member’s home without pay [1]. Often, they are unprepared and unequipped to deal with the consequences of stroke since it can be sudden and result in significant functional deficits [2]. This can lead to high levels of stress and feelings of inadequacy and place a burden on the well-being and health of the caregiver and their care recipient [3].
Patient and family education are essential, especially during the transition period from acute care or inpatient rehab to home. Studies such as Bartolo et al. [4] have highlighted that structured interventions targeting caregivers can decrease their level of stress, depression, and anxiety and increase their sense of well- being and ability to cope with the burden of caregiving. Healthcare practitioners must take this aspect of caregiver needs into consideration.
The patient and his family constitute the core members of the healthcare team. However, while the emphasis lies on the care and transition of the patient, the caregiver needs are often overlooked and more needs to be done to ensure the preparedness level of the caregiver [5]. In acute care, specific time is not spent on caregiver needs and readiness to meet the challenges of caring for the patient at home. Ideally, multiple sessions reviewing care of the patient and education to the caregiver regarding their health and well-being during the stressful task of caregiving should be included in the pre-discharge training [2]. Readiness and training for long term assistance may also have to be considered. This appears to be a neglected domain due to short lengths of stay, time constraints, and emphasis on the medical model in acute care settings [6].
Caregivers are as diverse as the United States as a whole: they come from every age, gender, socioeconomic, and racial/ethnic groups. Caregivers share many struggles but can face different challenges depending on their circumstances [7]. Spouses, partners, adult children, and extended family members now serve in the unpaid work force known as informal caretakers [8]. Family caregivers typically provide care for basic activities of daily living (BADLs) such as eating, grooming, bathing, and dressing, instrumental activities of daily living (IADLs) such as household chores, finances and medicine management and nursing/medical care if needed. Caregivers’ responsibilities often extend beyond the traditional direct care of BADLs and IADLs, to interacting with various providers, agencies, and professionals on their care recipient’s behalf [7].
According to the National Alliance of Caregivers [9], women make up the majority of informal caregivers (60%) and most of them are spouses. While the average age of an adult care provider is 49 years, the span of individuals between age 50 to 64 is growing. On average, the care recipient is 69.4 years old. Nearly half of all caregivers care for someone aged 75 years or older, and 39 percent care for someone age 50 to 74. Family caregivers spend an average of 24.4 hours per week providing care [7]. As the Baby Boomers age, there will be an increase in the age of older Americans and subsequently there will be increased need for services of informal caregivers [9].
The goal of this study was to assess the stress level and quality of life of caregivers providing care to persons affected by stroke. The study further examined if this burden was alleviated by the education and support provided through the occupational therapy-led program. The proposal included a six-part health education series with topics including stroke, caring for self, stress reduction techniques, communication, and wellness information. The literature supports the importance of supportive education in reducing the stress of caregivers and improving the quality of life of both the care recipient and the care provider. The study attempted to explore this concept.
Methods
This evidence-based study was a pretest and posttest mixed- method design. Participants were selected from a convenience sample of caregivers from the stroke support group and acute care patients of a comprehensive stroke center of a large hospital in the southeast United States. Participants were included in this study if they were informal caregivers of persons with stroke and provided physical or emotional support to the client, were 18 years or older, able to read and write English, and follow simple 2-step instructions. Those excluded from the study were persons who were not caregivers, were under 18 years of age, did not read or write English, were not able to follow simple 2-step instructions, and could not give written informed consent.
Measures
The project used two scales as quantitative measures- the Zarit Burden Interview (ZBI) [10] and the author created quality of life survey. The qualitative measures utilized were an author created exit questionnaire and a structured question that was audio-recorded. Burden of care was evaluated using the ZBI which contains 12 distinct questions measuring stress and burden faced by caregivers during their caregiving role. Higher scores indicate increased burden. The ZBI provides a comprehensive assessment of both objective and subjective burden, is a widely used burden measure, and has been validated in many culturally or ethnically different populations [11]. Permission to use the Zarit Burden Interview was obtained from the authors. The demographic questionnaire and the quality-of-life survey were both developed by this primary investigator. The Likert style quality of life survey was loosely based on the Short Form 12 Health Survey: SF-12 [12,13], and contained eight questions pertaining to physical and mental health, sleep, support available, and social functioning. The original SF-12 was not used since it did not capture all the areas this study aimed to report on. Validity of the quality-of-life measure included two rounds of peer review for construct validity by acute-care therapists and a pilot test with caregivers who were not part of the project. The primary investigator made changes based on feedback from peers and caregivers. These individuals had no part in the project, thus preventing contamination during the validity process. Reliability is limited as this was a new tool developed for the purposes of this project. Quantitative statistical analysis was completed pretest and posttest for both the scale questions to assess percentage of change using Microsoft Excel tools. The post-survey qualitative exit questionnaire and audio-recorded answer were analyzed using a grounded theory approach [14].
Procedures
Institutional Review Board (IRB) approval was received from the site facility for October 2018 to October 2019. Caregivers of patients with a stroke were identified by the stroke navigators and peer team members working in acute care of the study facility. Additionally, flyers announcing the study project were posted in prominent waiting areas of the hospital. The participants were contacted by the stroke navigators. Written consent was obtained from all participants prior to the start of the intervention. Participation in the study was voluntary and conducted on a day and time convenient to all the participants. To maintain confidentiality, those who participated in the study were asked to provide a four-digit code based on their mother’s birth month and year. A master code list was maintained by the primary investigator. All information collected was stored in a locked filing cabinet in the primary investigator’s office.
The intervention took place over a period of six weeks from October 2018 to December 2018. The primary investigator created educational binders for each participant with copies of all materials that were covered in the sessions. There were six educational modules that contained information on stroke, care of the patient, strategies for caregiver health and wellbeing, and community resources. The Zarit Burden Interview and the Quality of Life questionnaire were administered at week one. Thereafter, one educational module was presented each week in a lecture format via Microsoft PowerPoint® followed by a discussion for a duration of 60-90 minutes. Some modules had a practice component where the participants demonstrated what they had learned (e.g. safe transfers, breathing exercises). At the end of each session, the participants were encouraged to make a weekly goal for their well-being and ideas for activities were provided. The sessions occurred in a group format to allow for sharing of experiences. Using sound evidence from an established education program called “Powerful tools for caregivers’, other evidence-based articles, and this author’s over 30 years’ experience working with stroke patients, the structured sessions were created by the primary investigator. Articles were obtained from PubMed, Medline, OT Seeker, Research Gate, and the American Occupational Therapy Association (AOTA)[15] website. The weekly project schedule and topics discussed are shown in Table 1 (Six-week schedule for educational modules). At the end of the intervention, participants completed the same burden and quality of life surveys to compare the pre and posttest data. Participants also completed an exit questionnaire and an audio recorded answer. The exit questionnaire contained four questions regarding listing of two skills learned to reduce stress, two community resources, what they liked best about the program, and suggestions for improvement. The audio recorded question pertained to the caregivers’ perception of the education modules. A month after the study was concluded, the primary investigator made a phone call to each participant to answer any questions and encourage them to keep working on their wellness goal.
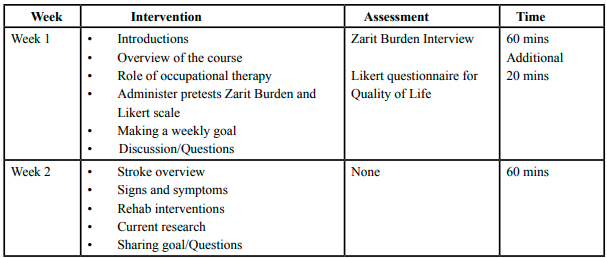
Table 1: Six-week schedule for educational modules
Data Analysis
Quantitative analysis of pretest and posttest surveys was completed using Microsoft Excel® version 2016 data analysis tools to compute the percentage of change in pretest and posttest results. Comparative analysis of pretest and posttest participants' surveys was completed. Demographic responses were analyzed using descriptive statistics. Qualitative analysis was completed using inductive content analysis and Microsoft Excel® version 2016 was used as the code book to highlight major concepts and ideas being conveyed. The resulting concepts were continually reviewed and grouped together to identify common themes related to the study question. Redundant or recurring information was eliminated. The audio-recorded answers were transcribed by the primary investigator by listening to the recording several times and noting pertinent themes. The primary investigator’s project guide and practice expert reviewed and confirmed the themes to support accuracy of the findings. Participants’ information was coded using a standard numbering method to identify respondents uniquely. Information collected from the pre- and posttest surveys were compared to determine if there were any significant changes in participants’ perceived care-burden and quality of life after completing the intervention modules. The qualitative survey was utilized to identify common themes, determine what participants found helpful, and areas for future improvement.
Results
Quantitative data were collected using 2 surveys: the ZBI and investigator created pretest and posttest survey using a 5-point Likert scale to measure caregivers’ self-ratings. The questions in the ZBI measured caregiver burden. The investigator created quality of life survey included questions about the caregivers’ perception of their overall well-being. An additional question assessed their satisfaction with the information they received to care for their relative.
Each of the caregivers reported their perceived burden and quality of life by circling the answer that best described their ability at week one and week six of the project using the ZBI and the quality-of-Life survey. Table 2 highlights the summary of pretest and posttest results of the Zarit Burden Interview. The ZBI scale included Never (0), Rarely (1), Sometimes (2), Quite Frequently (3), and Nearly Always (4). Table 3 provides a summary of pretest and posttest results of the quality-of-life survey. The quality of life scale included Very Dissatisfied (1), Dissatisfied (2), Neutral (3), Satisfied (4), Very Satisfied (5).
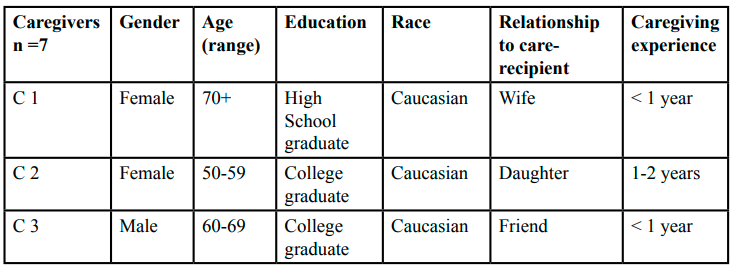
Table 2: Caregiver Demographics
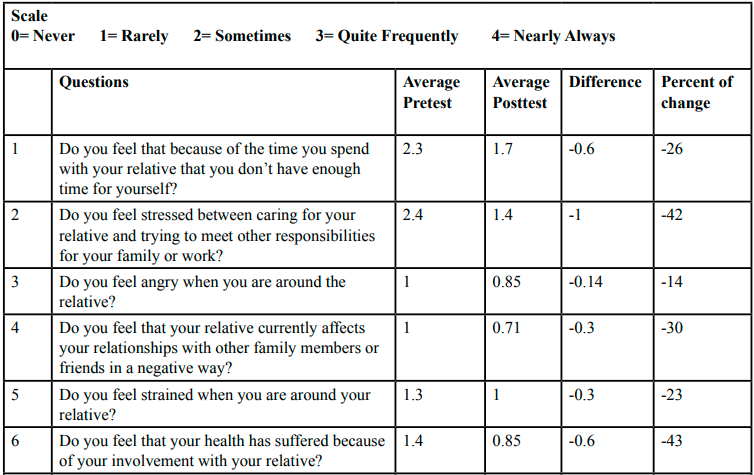
Table 3: Results of Zarit Burden Interview
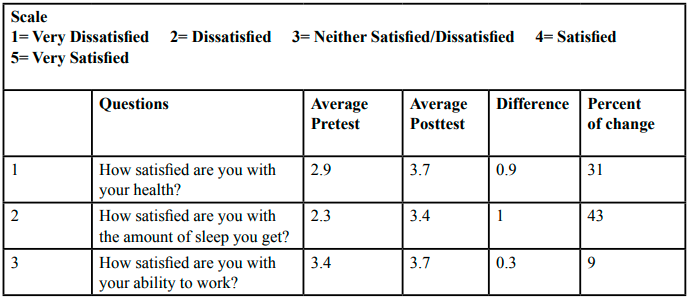
Table 4: Results of Quality of Life Questionnaire
After the intervention, data showed decreased burden and improved perception of wellbeing on all posttest questions. Statistical mean of caregivers’ responses on specific questions in the pretest and posttest surveys are visually displayed in Figure 1
Comparisons in the pre and posttest surveys of the ZBI were used to measure if the stress faced by the caregivers decreased due to the education and support provided during the interventions. When looking at the ZBI survey, results indicated that caregivers rated perceived burden lower in the posttest responses than in the pretest burden survey. Questions two and nine pertaining to stress due to caring for relative and loss of control of one’s life improved from “Sometimes” (a score of 2) and “Quite Frequently”(3) to “Sometimes” (2) and “Rarely” (1). Pretest question five which looked at strain faced by the participants when they were around the relative, improved from “Sometimes” (2) to “Rarely” (1) or “Never” (0). All responses demonstrated varying levels of improvement. Furthermore, the percentage of change was positive when calculated using mean pretest and posttest caregiver responses; this positive change is shown in Figure 2: Summary of Percentage of Change. Posttest questions positively changed an average of 32% with a range of 14% to 50%, indicating a positive response to the implementation of the project. Overall burden scores showed improvement from week one to week six indicating effectiveness of intervention.
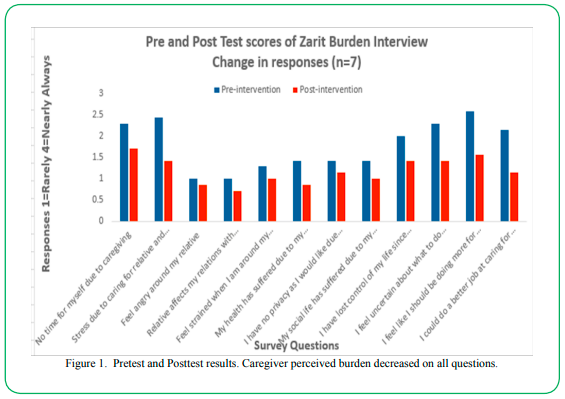
Figure 1. Pretest and Posttest results. Caregiver perceived burden decreased on all questions.
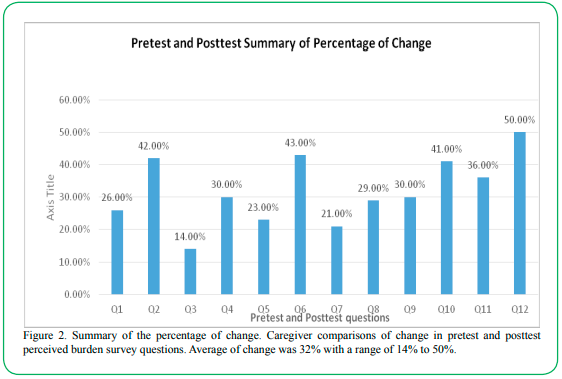
Figure 2. Summary of the percentage of change. Caregiver comparisons of change in pretest and posttest perceived burden survey questions. Average of change was 32% with a range of 14% to 50%.
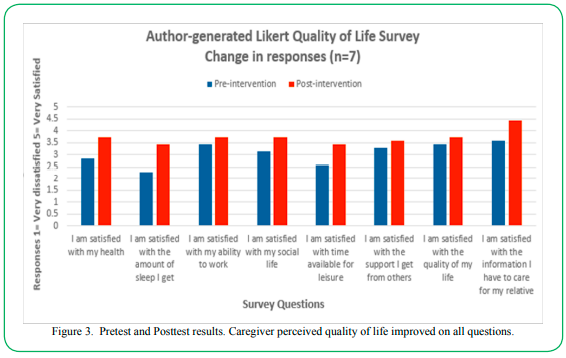
Figure 3. Pretest and Posttest results. Caregiver perceived quality of life improved on all questions.
The Likert Quality of Life questionnaire was utilized to compare the pre and posttest perceptions of caregivers about their own health and well-being. On pretest question one pertaining to satisfaction with health, two (28%) participants indicated satisfaction whereas post-intervention four (57%) expressed a perception of being satisfied with their health. At pretest, questions 2, 3, and 4 pertaining to amount of sleep, ability to work, and social life were scored between “Dissatisfied” (2) and “Neither Satisfied/Nor Dissatisfied” (3). Post intervention, these answers improved to a range between “Neither Satisfied/Nor Dissatisfied” (3) and “Satisfied” (4). Pretest question five about satisfaction with time available for leisure was scored by all seven (100%) participants as being dissatisfied or neither satisfied nor dissatisfied. Post-intervention, four (57%) participants reported being satisfied with time available for leisure. On pretest question eight, pertaining to satisfaction with the information participants had to care for their relatives, one (14%) participant reported being satisfied whereas post-intervention, all seven (100%) participants reported being satisfied with the information they had been provided by the investigator. Furthermore, the percentage of change was modestly positive when calculated using mean pretest and posttest caregiver responses; this positive change is shown in Figure 4: Summary of Percentage of Change. Posttest questions positively changed an average of 23% with a range of 9% to 43%, indicating a positive response to the implementation of the project. Overall scores showed an improvement in satisfaction from week one to week six indicating effectiveness of intervention.
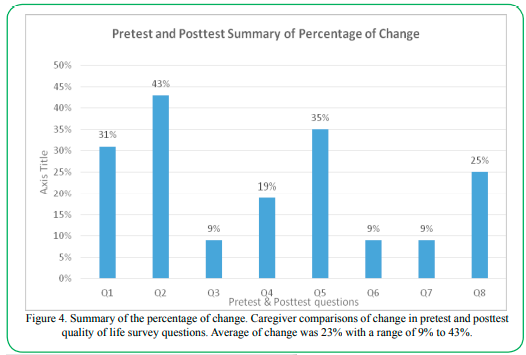
Figure 4. Summary of the percentage of change. Caregiver comparisons of change in pretest and posttest quality of life survey questions. Average of change was 23% with a range of 9% to 43%.
Qualitative Outcomes
Qualitative responses were obtained from the exit questionnaire created by the primary investigator and audio-recorded answer by each participant at the end of week six. The responses were organized and coded in Microsoft Excel by the primary investigator and reviewed by her project guide and her practice expert for accuracy and agreement on themes. The qualitative data analysis process included highlighting the major concepts and ideas being conveyed. The resulting concepts were continually reviewed and grouped together until saturation occurred to form themes related to the study question. Redundant or recurring information was eliminated. The audio-recorded answers were transcribed by the primary investigator by listening to the recording several times and making notes of pertinent themes. The responses yielded three prominent themes.
Theme one: Group support/sharing decreased stress.
Participants reported that sharing their experiences with people who were undergoing similar experiences helped them to believe that they were not alone in experiencing such feelings. Of the seven participants, six (86%) of them stated that sharing with other caregivers provided them with an outlet to speak with someone and relate to someone like them. It further helped them to see how everyone else coped and to learn from them. They emphasized that shared experiences with others in the group helped to decrease stress and that the support the group provided was very valuable. A sentiment shared by a caregiver was “I realized that I was not alone facing this situation. It helped to share experiences with others who were going through similar situations” (C5).
Theme two: Empowerment through knowledge.
Another prominent theme that emerged was the empowerment gained through improved knowledge of stroke. All seven participants (100%) acknowledged that they had gained new information on how to recognize a stroke and how to help their loved ones. Additionally, they had gained strategies on improving communication with their loved one and felt that they had valuable information on community resources for continued support. Participant C5 stated that the stroke information she received was the most imperative education for her. Another participant stated that “I learned a lot about community resources to help me and my husband” (C1).
Theme three: Learned strategies to care for self.
Participants expressed a new understanding of reasons to take care of themselves without feelings of guilt. Participant C4 stated “The classes taught me to prioritize my care of myself and not try to do everything in one day”. All seven participants (100%) felt that they had learned strategies for their own well-being through exercises, deep breathing, and relaxation techniques taught in the class. Another sentiment shared by participants C2 and C7 was that the exercises and breathing techniques taught for stress relief were new to them but very helpful. On the last day of the class, all the participants reported making time for themselves and engaging in some relaxing activity. Furthermore, they stated that they felt confident in taking care of themselves with the strategies learned in the classes.
Discussion and Conclusion
Quantitative data indicated that education and support decreased participants’ stress levels and increased their perception of wellbeing after the intervention. Additionally, the participants felt the education provided was beneficial for themselves and their care-recipients. Posttest surveys of the ZBI reflected lower levels of stress by all caregivers in varying degrees. Upon pre-evaluation, all the questions in the ZBI were scored between 1-2.57 whereas the post evaluation scores ranged from -.71 to -1.71 indicating a 32% average decrease in stress levels. The Likert style Quality of Life questionnaire similarly reflected improved quality of life post intervention. The pre-evaluation scores ranged from 2.28-3.57 and the post evaluation scores were between 3.42-4.42 indicating a 23% average improvement in overall feelings of wellbeing. The study results show that overall care burden decreased and quality of life improved due to the OT intervention provided. The results of this study correspond with a study by Perrin et al. [16], who identified a need for education to help caregivers cope mentally with the continued task of providing care. Interventions during rehabilitation services were helpful to caregivers which included direct care of the patient and strategies for stress reduction in themselves [2,16]. In a randomized controlled trial conducted by Whitebird et al. [17], the authors utilized mindfulness-based stress reduction techniques to counteract the negative effects of stress and improve health and well-being of caregivers.
Qualitative themes that emerged included feelings of empowerment due to the knowledge gained and decreased feelings of guilt in taking care of themselves due to the sharing of experiences and support provided by the group. Participants’ qualitative responses were positive and indicated the education modules were beneficial to the caregivers and the educational binders provided to them would serve as a resource for future use. The positive qualitative themes support this project’s focused question that education and support can help caregivers manage stress and better care for themselves and their care-recipients, especially considering that this can have an impact on patient outcomes. Both quantitative data and qualitative themes support the focused question in that education and support benefits caregivers.
Implications for occupational therapy practice
The results of this study demonstrated that engagement in caregiving activities leads to increased burden and lower quality of life. Caregiving without adequate support may have implications on health and well-being for caregivers. Interventions such as the ones utilized in this study that focus on the needs of the caregivers may help in reducing stress faced during their role of caregiving and contribute to perceptions of improved health and general well-being. Early identification of these caregiver needs is imperative. Occupational therapists must expand their practice to not only teach physical skills of caring for the patient but also include the understanding and skill of the caregiver in providing such care.
Informal caregivers need time and validation to practice what is taught for a safe transition to home. Strategies for problem-solving at home needs to be ongoing with continued face-to-face or telephonic support. This will help caregivers to experience greater well-being and reduce the perception of burden in the role of caregiving. A greater focus should be placed on caregiver education to students at all educational levels in OT. Additionally, OT practitioners need to be aware of the available resources they can direct the caregivers to and recognize the importance of including such resources as part of the OT intervention for both the client and their caregivers.
Limitations
Several limitations exist in this study. First was the small sample size (n=7) which decreases the ability to generalize the results to the wider population. Data saturation was not reached due to the limited number of participants. Convenience sampling was used so persons had some innate motivation when they started the classes. Second, there was not much diversity in race: 84% (n=6) were white and 14% (n=1) was black. Additionally, the snow conditions during the implementation month proved to be a deterrent due to hazardous driving conditions requiring rescheduling of one session due to safety reasons. The project was short, once a week for 6 weeks, and this must be considered a limitation as well. Finally, one of the outcome tools was developed by the primary investigator. While steps were taken to utilize the best available literature to create this survey, the tool was not standardized and had limited validity.
Summary
The purposes of this study were to identify the levels of burden and quality of life of informal caregivers of persons with a stroke. The study further investigated if this burden was alleviated, and quality of life improved by an OT-led education series and group support. The study revealed that structured education provided in a group format with topics covering care of the patient and strategies for the health of the caregiver were effective. It is recommended that family caregivers should be provided with strategies for problem-solving and long-term face-to- face or telephonic support. This will help caregivers to experience greater well-being and reduce the perception of burden in the role of caregiving. Additionally, there should be a greater focus on caregiver education to students at all educational levels in OT. Continued social networks and ongoing assist via support groups and technology-based strategies to provide practical solutions to problems are important. Monitoring caregiver needs and health once their loved one goes home may prove to be effective in preventing readmissions of patients. Policy changes related to healthcare coverage and reimbursement to allow the caregiver to stay home or being paid for caregiving may have to be considered to alleviate the physical and financial burden. These changes may promote health and wellbeing in both the caregiver and their care-recipient. OT practitioners are well-equipped to provide holistic care by focusing on both the client and caregiver and providing programs for the wellbeing of both [18].
Acknowledgements
I thank all the caregiver participants in this study for their time, support, and cooperation, without which this study would not have been possible. I also thank Dr. Heidi Baist (project guide) and Dr. Megan Edwards Collins (practice expert) for their guidance and support.
Declaration of interest
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper.
Additional information
Notes on contributor
Sanchala k. Sen, OTD, MS, OTR/L, BCPR. is an assistant professor in the department of occupational therapy at Winston-Salem State University, North Carolina, United States. She was a post-professional occupational therapy doctorate student at Chatham University, Pittsburgh at the time of this study. This study was completed as partial fulfilment of her degree under the guidance of Dr. Heidi Baist, OTD, OTR/L
References
Keglovits, M., Somerville, E., & Stark, S. (2015). In-Home occupational performance evaluation for providing assistance (I–HOPE Assist): An assessment for informal caregivers. American Journal of Occupational Therapy, 69(5). doi:10.5014/ ajot.2015.015248View
Rajan, B., Suman, G., Pruthvish, S., & Radhika, K. (2016). Assessment of stress among caregivers of the stroke survivors: Community based study. International Journal of Community Medicine and Public Health, 4(1), 211-215. doi:10.18203/23946040.ijcmph20164740View
Cameron, J. I., & Gignac, M. A. M. (2008). "Timing it right": A conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Education and Counseling, 70(3), 305–314. https://doi.org/10.1016/j.pec.2007.10.020View
Barth, J., Schneider, S., & Känel, R. V. (2010). Lack of social support in the etiology and the prognosis of coronary heart disease: A systematic review and meta-analysis. Psychosomatic Medicine, 72(3), 229-238. doi:10.1097/psy.0b013e3181d0161View
Rodgers, H., Francis, J. J., Brittain, K., & Robinson, A. L. (2007). Who cares? – Caring for the carers of stroke patients. Disability and Rehabilitation, 29(5), 425-427. doi:10.1080/09638280600834369View
Ekstam, L., Johansson, U., Guidetti, S., Eriksson, G., & Ytterberg, C. (2015). The combined perceptions of people with stroke and their carers regarding rehabilitation needs 1 year after stroke: A mixed methods study. BMJ Open, 5(2). doi:10.1136/ bmjopen-2014006784View
Caregiving in the U.S. (2015).HCBS Clearinghouse. http:// www.advancingstates.org/node/66488.View
Sakakibara, K., Kabayama, M., & Ito, M. (2015). Experiences of “endless” caregiving of impaired elderly at home by family caregivers: A qualitative study. BMC Research Notes, 8(1). doi:10.1186/s13104-015-1829-xView
National Alliance for Caregiving Public Policy Institutes (2015). Caregiving in the U.S.: 2015 report. Retrieved from http://www. caregiver.orgView
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist, 20(6), 649-655. doi:10.1093/geront/20.6.649View
Kheng, seng B. (2010). Validity and Reliability of the Zarit Burden Interview in Assessing Caregiving Burden. Annals Academy of Medicine, 39, 758–763.View
Akosile, C. O., Okoye, E. C., Nwankwo, M. J., Akosile, C. O., & Mbada, C. E. (2011). Quality of life and its correlates IN caregivers of stroke survivors from a Nigerian population. Quality of Life Research, 20(9), 1379–1384. https://doi. org/10.1007/s11136-011-9876-9 View
Salyers, M. P., Bosworth, H. B., Swanson, J. W., Lamb-Pagone, J., & Osher, F. C. (2000). Reliability and validity of the sf-12 Health survey among people with severe mental illness. Medical Care, 38(11), 1141–1150. https://doi.org/10.1097/00005650- 200011000-00008View
Hissong, A., Lape, J., & Bailey, D. (2015). Research for the health professional (3rd ed.). Philadelphia, PA: F.A. Davis Company
American Occupational Therapy Association [AOTA]. (2014). Occupational therapy practice framework: Domain and process (3rd ed.) American Journal of Occupational Therapy, 68(Suppl.1), S1-S48. doi.org/10.5014/ajot.2014.68200.1View
Perrin, P. B., Johnston, A., Vogel, B., Heesacker, M., Vega-Trujillo, M., Anderson, J., & Rittman, M. (2010). A culturally sensitive transition assistance program for stroke caregivers: Examining caregiver mental health and stroke rehabilitation. The Journal of Rehabilitation Research and Development, 47(7), 605. doi:10.1682/jrrd.2009.10.0170View
Whitebird, R. R., Kreitzer, M., Crain, A. L., Lewis, B. A., Hanson, L. R., & Enstad, C. J. (2012). Mindfulness-based stress reduction for family caregivers: A randomized controlled trial. The Gerontologist, 53(4), 676-686. doi:10.1093/geront/gns126View
Occupational therapy and sustainable development (2012). Swedish Association of Occupational Therapists- From a Swedish perspective. Retrieved from http://www. arbetsterapeuterna.se/Global/Om_forbundet/Other%20 languages/English/sustainable_ development_rev.pdf