
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 4 (2023), Article ID: JRPR-141
Special Issue: Physical Therapy: From Acute Care to Rehabilitation and Wellness
https://doi.org/10.33790/jrpr1100141Special Issue
Efficacy of Kinematic Therapy on Mood Disorders, Functional Independence Recovery and Quality of Life of Stroke Survivors
Caleb Ademola Omuwa GBIRI PhD, FWSO, FWSFL1*, & Maryam Tolulope KAREEM BPT2
Department of Physiotherapy, College of Medicine, University of Lagos, Lagos, Nigeria.
Corresponding Author Details: Caleb Ademola Omuwa GBIRI PhD, FWSO, FWSFL, Stroke and Nervous System Disorders Research Team, Neurophysiotherapy Unit, Department of Physiotherapy, College of Medicine, University of Lagos, Nigeria.
Received date: 04th February, 2023
Accepted date: 09th March, 2023
Published date: 11th March, 2023
Citation: GBIRI, C.A.O, & KAREEM, M. T., (2023). Efficacy of Kinematic Therapy on Mood Disorders, Functional Independence Recovery and Quality of Life of Stroke Survivors. J Rehab Pract Res, 4(1):141.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background and Aims: Mood disorders impact negatively on rehabilitation process and outcomes in stroke survivors (SSv). This study determined efficacy of Kinematic Therapy (KT) on depression, anxiety, functional independence (FI) and QoL of SSv.
Methodology: Study involved 940 ambulant SSv recruited from eight health institutions in Lagos, Nigeria and were assessed for depression, anxiety, QoL and FI using Becks Depression Inventory, Becks Anxiety Inventory, Stroke-Specific-QoL questionnaire and FI Measure respectively. They were randomised into KT and Common Physiotherapy (CP) groups. The KT received 25minutes of kinematic therapy while the CP received usual physiotherapy, twice weekly for 6weeks.
Results: Six hundred and seventy-four (343males) of the 940 SSv were diagnosed of depression and/or anxiety and participated in this study; 341(50.59%) were in KT while 333 were in SP. More (81.23%) of KT had mild mood disturbance before intervention while 92.36% of them had normal mood after. More (83.18%) of SP had borderline mood disorder before intervention while 84.69% had normal mood after. There was significant (p<0.05) improvement in depression, anxiety, QoL and FI except in language, personality, family role, self care, social role, thinking and upper-limb function in SP. The KT had significantly better improvement all the outcomes than SP. There was negative significant relationship (p<0.05) between depression and anxiety, and FI and QoL. There was positive significant relationship (p<0.05) between FI and QoL except in vision domain.
Conclusion: Mood disorders is common in stroke survivors. Kinematic Therapy is more effective in managing depression and anxiety symptoms and improving functional independent recovery and quality of life than conventional physiotherapy in stroke survivors.
Key words: Kinematic Therapy, Anxiety Disorder, Depressive Disorder, Quality of life, Functional Independence.
Introduction
The burden of stroke is bore by both the stroke survivors, their informal caregivers, and the society at large. The disability associated with stroke is multi-dimensional ranging from physical, psychological, emotional to social disabilities [1]. Several psychosocial challenges including anxiety, depression and fatigue are frequently reported in stroke survivors resulting in long-time disability and failure to return to productive lifestyle [2-7]. Emotional and mood disorders such as depression, anxiety, anger, general psychological distress and social isolation are common within the first few months of stroke and may persist for years with negative impact on rehabilitation outcomes [2,3,8-11]. Stroke survivors with emotional disorders especially have problem following the course of therapy and it usually affect outcomes of their rehabilitation and recovery [9,12,13]. The mood disorders and psychosocial challenges sequel to stroke mostly result into long-term functional limitations and low quality of life in stroke survivors [9,12-14].
Many emerging approaches are being designed for effective outcomes in stroke especially in returning stroke survivors to community functioning and productivity. One of the innovative interventions for individuals with neurological conditions but not yet in stroke are music and dance [15-19]. Dance as an exercise is as a set of rhythmical body movements performed according to temporal, as well as spatial parameters in relation to a desired health benefit. However, Kinematic Therapy is a dance performed by more than one person doing the same things in response to the desired goals with involvement of both visual and auditory cues to guide the body movement in specific pattern. There is a distinct relationship between the psychological and physiological responses to moving to music, and this works to alter mood, leading to increased mental health and provides physical health benefits [20].
Dance presents multiple physical benefits including aerobic power, muscle endurance, strength, and body flexibility; static and dynamic balance/agility; and gait speed for older adults with or without neurological disorder and bridges the gap for enjoyable social activity [16,21-25]. Dance causes significant changes in plasma serotonin and dopamine concentrations and thereby decreasing the severity of depression [26]. Individuals who engage in synchronized activities have increased feelings of liking, interpersonal trust, willingness to help a partner and heightened sense of being similar in personality [23,25]. A possible mechanistic explanation for the social closeness that arises during these synchrony-based activities draws on the role of neurohormones, such as endogenous opioids which are associated social relationship and bonding [26-27]. However, it is unclear if Kinematic Therapy will improve mood disorders, functional independence performance, disability and other complications of stroke. Therefore, this research was designed to explore the effectiveness of Kinematic Therapy on post-stroke mood disorders and to determine the impacts on the quality of life and functional independence performance in ambulatory stroke survivors. The outcome of this study is expected to provide antidote to the management of mood disorders and functional dependency sequel to stroke. This may conversely provide solution to the disability associated with onset of mood disorders in stroke survivors.
Methodology
This study was approved by the Health Research and Ethics Committee of Lagos University Teaching Hospital (ADM/DCST/ HREC/APP/846) and the Health Service Commission (LSHSC/2222/ Vol. XIV/101) both in Lagos, Nigeria.This study screened 940 community-based ambulatory (with or without aids/support) stroke survivors and involved 798 of them with a score not less than 24 on the Mini Mental Scale assessment. Out of the 798, 116 declined their participation while 682 were screened for mood disorders out of whom 674 were diagnosed of having either depression or/and anxiety disorders. The participants were included if they had either depression and/or anxiety using diagnostic criteria of mood disorders in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5)[28], had no communication or hearing disorder and had no physical disability other than those that are attributable to stroke. Diagnoses of depression and/or anxiety were made by CAOG while other members of the research team and the participants were blinded to the diagnoses. The diagnoses were used to randomize them into Kinematic Therapy group (KTG) or standard physiotherapy group (SPG) by a blinded research assistant using simple random sampling technique. The KTG consist of 341 participants while the SPG had 333 participants. The flowchart for the recruitment and selection procedure is as presented in figure 1.
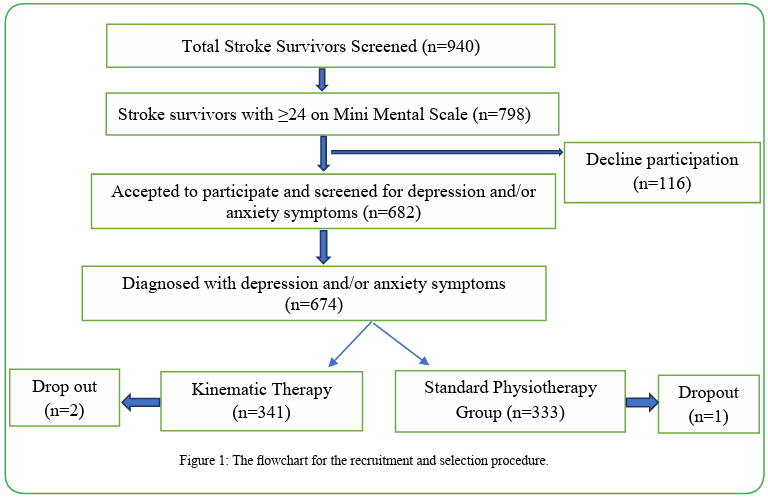
Figure 1. The flowchart for the recruitment and selection procedure.
Their socio-demographic data were obtained through interview. Clinical details were obtained from the hospital folder and from physical assessment. The Becks Depression Inventory [29], Becks Anxiety Inventory [30], Stroke-Specific QoL [31] and Functional Independence Measure [32] were administered on the participants. The assessments were made before the commencement of the interventions and at the end of the 6weeks of interventions. To avoid cyclical changes associated with emotional behaviour and weather, the assessments were carried out at the same time of the day, between 9am and 12noon. Participant’s blood pressure was checked at the beginning of every treatment session while they were instructed to stop if there is fatigued during a session.
The kinematic therapy was administered using specific music and dance system for aerobic dance in which the participants were grouped into eight participants per group. A music of low to mid-intensity beat tone with appropriate rhythm was used. A prerecorded audio-visual with dancers that exemplified the specific body movements required was used. The participants pre-watched the audio-visual for the first 30minutes to familiarize them with the content of the recording. Participants replicated the body movements in the video in their group. They were coordinated and supervised for compliance with the rhythm. The aerobic dance tailored towards functional performance while the SPG participated in individualized physiotherapy also tailored towards functional performance. In addition to the interventions for each of the groups, each participant received soft tissue massage with topical non-steroidal anti inflammatory at the end of each session. Each session lasted for an hour. The structure consisted of 5 components: warm-up exercises (5 minutes), movement therapy (5 minutes), aerobic dance (40 minutes) and relaxation in-between dance (5 minutes) and cool-down (5 minutes). The dance class was conducted for in a group-therapy, twice a week for 6weeks. The 40 minutes dance duration was stratified into two equal half of 20 minutes each with 5 minutes of rest in-between. Choreography was adopted for the aerobic dance (synchronized movements) with a video aid. During the dance, specific attention was paid to the segmental movements of the body parts: upper-limbs, Head, Trunk, and lower-limb for 5 minutes in each of the half of the dancing time. The dance was played to them through an audio-visual instrument with the monitor placed in front of them. They were to replicate all the activities in the audio visual display. The dance involved head and neck movement, upper limb movement, lower-limb movement, and trunk movement; each performed in specific and prescribed pattern according to the goal of the treatments. The dance intensity was set at 40-50% of maximum heart rate and was progressed to 60-70% maximum heart rate at the end of the 6weeks by changing the tempo of the music from medium energy to high energy. An electronic sphygmomanometer was worn by each participant during the dance programme to monitor their cardiovascular parameters. The parameters in the electronic sphygmomanometer were set for the individuals using their specific indices of age, sex, height, weight, and activity levels.
Participants in the standard physiotherapy group received physiotherapy designed for their functional performance executed individually. Their treatment protocol lasted for an hour consisting of passive mobilization of all joints of the affected limbs, assisted active exercises to muscle groups with sub-maximal performance, free active exercises for muscles with adequate muscle function, resisted active movement for overload of muscles, treadmill exercise, squatting exercise, bicycle ergometry, and reciprocal pulley exercises. No adverse event was recorded in any of the participants. The activities were played to them through a visual playback instrument with the monitor placed in front of them. They were to replicate the exercises pre-recorded in the audio-visual playback instrument during the treatments. The exercises involved head and neck movement, upper limb movement, lower-limb movement, and trunk movement as in the KTG; performed in specific and prescribed pattern according to the goal of the treatments. Each of the participants in the KTG and SPG was given the audio-visual for of their programme to aid their home programme. They were also provided with activity log to record their participations in the prescribed home programmes and a follow up call was placed to each participant every day as a reminder for their home programme.
Data Analysis: Data was analyzed with intention to treat analysis. McNemar’s test was used to compare the pre-treatment and post treatment outcomes in each group. Mann-Whitney U-test was used to compare treatment outcomes between the two groups post intervention while Spearman’s correlation statistics (r) was used to check relationship among outcomes.
Results
Six hundred and seventy-four (343males, 50.89%) ambulatory stroke survivors diagnosed of depression and/or anxiety made the final sample size for this study; 341(50.59%) were in KT while 333 were in SP. Three (2 males in KT and one female in SP did not complete the study due to relocation to a distance more than 100 kilometers from the research sites. The population was normally distributed with age between 35 years and 81 years (mean of 59.66±10.32 years, mode=59 years and median=59 years). Three hundred and one (44.66%) of them had a right hemispheric affectation while 55.34% had left hemispheric affectation. Majority (97.77%) of the participants were right-handed. Their period since onset of stroke range between 5 months and 180 months with a mean of 38.98±43. 52 months (median=37 months and mode=38 months). Almost all (93.47%) completed at least secondary school education with the rest completing post-secondary education. The most common co-morbid health condition in the participants was hypertension occurring in 72.70% of them with a few having diabetics (8.46%) asthma (2.08%), peptic ulcer (2.08%) in addition to hypertension.
The KT comprised of 173 males (50.73%) and 49.27% females. Most (75.07%) of them were married while 3.52% were widowed (Table 1). Other sociodemographic of the participants were as presented in table 1. The SP comprised of 170males (51.05%) and 48.95% females. Most (74.48%) of them were married while 4.81% had never been married (Table 1). Their other sociodemographic were as presented in table 1. The activities’ log showed that both the KT and the KT performed the home programmes as prescribed with 100% compliance.
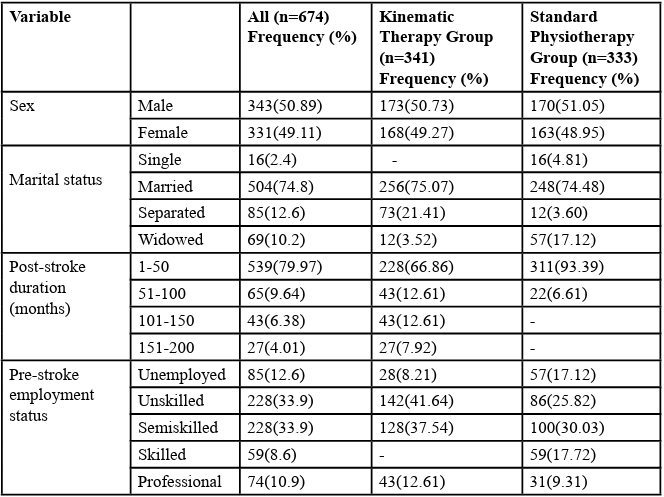
Table 1: Socio-demographic and Clinical Characteristics of the Participants
Participants in both groups were comparable at baseline in age, depression scores, anxiety rating, QoL and functional independent performances (p>0.05). More (81.23%) of the participants in the KT had mild mood disturbance before the intervention while after intervention 92.36% of them had normal mood at the end of the interventions (Figure 2). In the SP more (83.18%) had borderline mood disorder while after the intervention 84.69% had normal mood at the end of the interventions (Figure 2). There was statistically significant (p<0.05) improvement in depression, anxiety, quality of life and functional independent performance in both groups at the end of the interventions. There was statistically significant improvement (p<0.05) in the QoL and FI in both group except in language, personality, family role, self-care, social role, thinking and upper extremity function in the SPG. However, the KT had significantly better improvement in each of their depression, anxiety, functional independence, and quality of life scores than the SP (Table 2). There was negative significant relationship between each of depression and anxiety scores and functional independence and quality of life scores in the participants (Table 3). There was positive significant relationship (p<0.05) between functional independence and each of domain scores and total scores of the quality of life in the participants except in the domain of vision (Table 4).
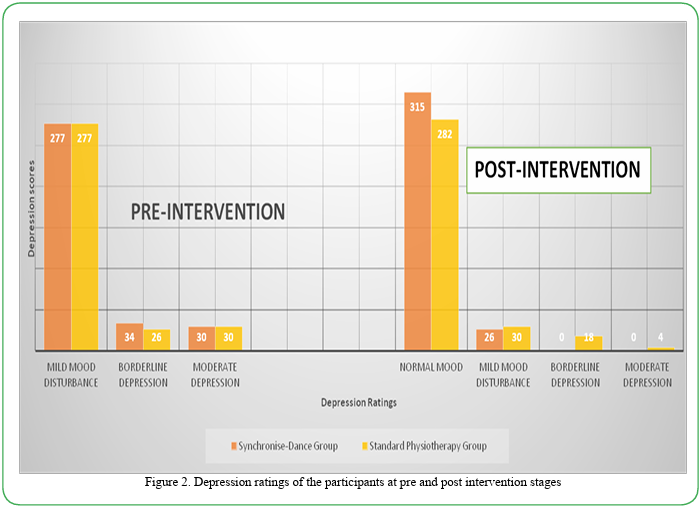
Figure 2. Depression ratings of the participants at pre and post intervention stages
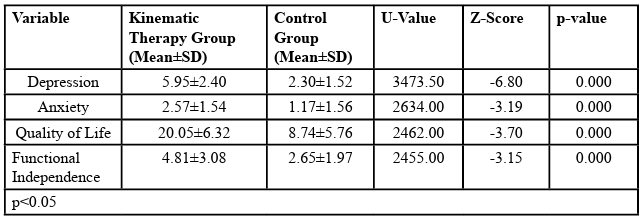
Table 2: Comparison of Depression, Anxiety, Quality of Life and Functional Independent Measure between the Kinematic Therapyd and Control Groups at the Post-Intervention stage
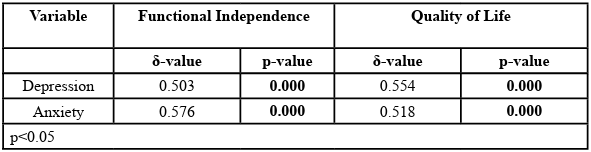
Table 3: Relationship between Depression and Anxiety and Each of Quality of Life and Functional Independence in the Participants
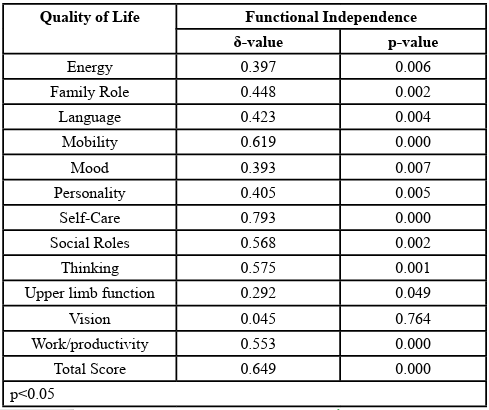
Table 4: Relationship between Functional Independence and Quality of Life of the Participants
Discussion
This study explored the efficacy of Kinematic Therapy on post stroke depressive and anxiety symptoms towards improving functional independence and quality of life in stroke survivors with mood disorders and to compare the outcome with that of standard interventional approach. The outcome of this study revealed that depression and anxiety are very common with stroke survivors and impact negatively on their functional independence performance and quality of life. Some previous studies among stroke survivors had documented high prevalence of depression and other emotional and their negative impacts on both the quality of life and rehabilitation outcomes in stroke survivors [8]. Although emotional disorders are rarely assessed in post-stroke individuals during evaluation for rehabilitation, the outcome of this study has shown how important it is to always include emotional assessment as part of routine assessment of stroke survivors to ensure comprehensive rehabilitation plan and entrenchment of holistic rehabilitation programme.
The fact that the participants for the Kinematic Therapy group found it easy to continue the dance at home and reported dance as a pleasurable activity that everyone can participate. It is therefore recommended that dance therapy should be incorporated as a therapy for stroke survivors. It should also be prescribed as home programme with a music of choice.
The improvement in functional performance and consequent improvement in their quality of life with the dance therapy could be attributed to the decrease in their depressive and anxiety symptoms. It can be said that, to improve functional independence and quality of life in stroke survivors, dance therapy could be an easy and readily available approach for use. The Kinematic Therapy is not just a therapy, but it also promotes social integration among the participants. Since social integration and participation is a concept in quality of life, it is not surprising that the quality of life of the participants improved with the dance therapy.
The results of this study show that Kinematic Therapy was more effective than conventional therapy in ameliorating mood disorders and improve functional independence and quality of life in stroke survivors. The significant improvements in the domains of family role, mobility, self-care, thinking, work/productivity, and mood also lay credence to the effectiveness of the Kinematic Therapy therapy. Earlier opined that aerobic exercises beneficial in improving anxiety, depression, and quality of life in individuals with neurological disorders [26]. Therefore, dance therapy, which is available, affordable, and accessible to everyone should be effectively utilized in the management of mood disorders, improve functional performance and quality of life in stroke survivors.
The inverse relationships that were observed between depression and each of functional independence and quality of life show that stroke negatively impact on quality of life of individuals after a stroke and it is complicated by onset of mood disorders especially depression. Therefore, clinicians should address depression in stroke survivors to improve their independence functioning and quality of life which are the main goals of rehabilitation. Conversely, the significant relationship that exists between anxiety score and each of domains of family role, energy and mood shows the negative impact of emotional disturbances on the quality of life and independent functioning in stroke survivors. apart from the need for early identification of mood disorders in stroke survivors, efforts should be directed at treating it using a good interventional programme such as synchronize-dance to reduce disability, improve functional performance and quality of life in stroke patients.
The fact that most people who were previously employed before stroke were without a job thereafter shows that stroke is cause of unemployment and loss of productive lifestyle. However, it had been shown that improve quality of life results in improve productivity after stroke [15,16]. Therefore every effort should therefore be directed at improving quality of life for improve productivity in individuals after a stroke.
Conclusion
Mood disorders are highly prevalent and are significantly related to functional dependency and reduced quality of life in stroke survivors. Kinematic Therapy is more effective than standard k known therapy in improving functional independence and quality of life in stroke survivors with mood disorders.
Competing Interests:
The authors declare that they have no competing interests.
References
Roger, V. L., Go, A. S., Llyod-Jones, D. M., Adams, R. J., Berry, J. D., & Brown, T. M., et al (2011). Heart disease and stroke statistics update: A report from the America Heart Association. Circulation 123(4):18-209.View
Teasell, R.W., McRae, M., & Finestone, H.M. (2000). Social issues in the rehabilitation of younger stroke patients.Archives of Physical Medicine and Rehabilitation 81(2):205-209.View
Daniel, K., Wolfe, C.D.A., Busch, M.A., & McKevitt, C., (2009). What Are the Social Consequences of Stroke for Working-Aged Adults? Stroke 40(6):431-440.View
Lerdal, A., Bakken, L.N., Kouwenhoven, S.E., Pedersen, G., Kirkevold, M., Finset, A., & Kim, H.S. (2009). Post-stroke Fatigue-A Review. Journal of Pain and Symptom. Management 38(6):928-949.View
Hofgren, C., Esbjornsson, E., & Sunnerhagen, K.S. (2010). Return to work after acquired brain injury: facilitators and hindrances observed in a sub-acute rehabilitation setting. Work 36(4):431-439.View
Wilz, G., & Soellner, R., (2009). Work loss following stroke. Disability & Rehabilitation 31(18):1487-1493.View
Visser-Meily, M.L., Rhebergen, G. J. E, Rinkel, G. J., Van Zandvoort, M. J., Post MW (2009). Relationship with psychological symptoms and personality characteristics long term health-related quality of life after aneurismal subarachnoid hemorrhage. Stroke 40:1526-1529.View
Knapp, P., Young, J., House, A., & Forster, A. (2000). Non-drug strategies to resolve psychosocial difficulties after stroke. Age and Ageing 29(1):23-30. View
Hackett, M. L., Duncan, J.R., Anderson, C. S., Broad, J. B., & Bonita, R. (2000). Health- Related Quality of Life Among Long-Term Survivors of Stroke: Results from the Auckland Stroke Study, 1991-1992. Stroke 31:440-447.View
Ferro, J. M., Caeiro, L., Santos, C (2009). Post-stroke emotional and behavior impairment: a narrative review. Cerebrovascular Disease 27(1):197-203View
Brown, C., Hasson, H., Thyselius, V., & Almborg, A.H . (2012). Post-stroke depression and functional independence: a conundrum. Acta Neurologica Scandinavica 126:45-51.View
Kijowski, S., (2014). Difficulties in post-stroke gait improvement caused by post-stroke depression. Chinese Medical Journal127: 2085-2090.View
Teoh, V., Sims, J., & Milgrom, J. (2009). Psychosocial predictors of quality of life in a sample of community-dwelling stroke survivors: a longitudinal study. Topics in Stroke Rehabilitation 16(2):157-166.View
Berrol, C. F. (1990). Dance/movement therapy in head injury rehabilitation. Brain Injury 4:257–265. View
Berrol, C. F., Ooi, W. L., & Katz, S. S. (1997). Dance/movement therapy with older adults who have sustained neurological insult: A demonstration project. American Journal of Dance Therapy19: 135–160.View
Hackney, M.E., Hall, C. D., Echt, K.V., & Wolf, S. L. (2012). Application of adapted tango as therapeutic intervention for patients with chronic stroke. Journal of Geriatric Physical Therapy 35: 206–217View
Orantin, M., Yelnik, A., Jousse, M., Guillemette, M., Bernard, A., Tlili, L., & Quintaine, V. (2018). Give music therapy a chance in post-stroke rehabilitation. Annals Physical and Rehabilitation Medicine. Feb 10. pii: S1877-0657(18)30009-5.View
Sarkamo, T., (2018). Music for the ageing brain: Cognitive, emotional, social, and neural benefits of musical leisure activities in stroke and dementia Dementia. 17, 6, p. 670-685View
Murrock, C., & HeifnerGraor, C. (2014). Effects of Dance on Depression, Physical Function, and Disability in Underserved Adults. Journal of Aging & Physical Activity 22(3):380-385View
Belardinelli, R.., Lacalaprice, F., Ventrella, C., Volpe, L., Faccenda, E., (2008). Waltz Dancing in patients with chronic heart failure new form of exercise training. Circulation Heart Failure 1:107–114.View
Keogh, J.W., Kilding, A., Pidgeon, P., Ashley, L., Gillis, D., (2009). Physical benefits of dancing for healthy older adults: A review. Journal of Aging and Physical Activity 17: 479-500.View
Hove, M.J., & Risen, J. L. (2009). It’s all in the timing: interpersonal synchrony increases affiliation. Social Cognitive and Affective Neuroscience 27:949–961.View
Lees, R., Fearon, P., Harrison, J.K., Broomfield, N. M., Quinn , T. J. (2012). Cognitive and mood assessment in stroke research: focused review of contemporary studies. Stroke 43:1678–1680.View
Launay, J., Dean, R.T., & Bailes, F. (2013). Synchronization can influence trust following virtual interaction. Journal of Experimental Psychology 60: 53–63.View
Tarr, B., Launay, J., & Dunbar, R. I. M. (2014). Music and social bonding: ‘self–other’ merging and neurohormonal mechanisms. Frontiers in Psychology 5:1-10.View
Machin, A., Dunbar, R. I. M., (2011). The brain opioid theory of social attachment: a review of the evidence. Behaviour 148:985–1025.View
Chan, W., Immink, M. A., & Hillier, S. (2012). Yoga and exercise for symptoms of depression and anxiety in people with post stroke disability: A randomized controlled pilot study. Alternative therapies in health and medicine 18(3):34-43.View
Diagnostic and Statistical Manual of Mental Disorders, fifth edition (2013). American Psychiatric Association. 800 Maine Anenue, S.W., Suite 900, Washington, DC 20024View
Tombaugh, T. N., & McIntyre, N. J. (1992). The Mini-Mental State Examination: A comprehensive review. Journal of the American Geriatric Society 40:922-935.View
Chapman, L. K., Williams, S. R., Mast, B. T., Woodruff-Borden, J. A. (2009). Confirmatory factor analysis of the Beck Anxiety Inventory in African American and European American. young adults. Journal of Anxiety Disorders 23:387–392 View
Beck, A.T., Epstein, N., Brown, G., & Steer, R.A. (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56:893-897.View
Williams, L. S., Redmon, G., Saul, D. C., & Weinberger, M., (2000). Reliability and telephone validity of Stroke Specific Quality of Life (SS-QOL) scale. Stroke 32: 339. View