
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 4 (2023), Article ID: JRPR-144
Special Issue: Physical Therapy: From Acute Care to Rehabilitation and Wellness
https://doi.org/10.33790/jrpr1100144Special Issue
Long-term Effects of Plantar Plate Therapy for Subtalar Joint Valgus Type for One Case Osteoarthritis of the Knee
Shingo Shimizu1*, Yukihisa Katoh2, Seiji Sabashi3, Kunio Ida4, & Hirokatu Hanamura5
1Assistant Professor, Department of Physical Therapy, Saitama Prefectural University, Faclity of Health Medical and Welfare 820, Sanomiya, Koshigaya-shi, Saitama-ken, 343-8540, Japan.
2Meijo University Faculty of Science and Technology, 501-1tyoume Shiogamaguchi, Tenpaku-ku, Nagoya-shi, Aichi-ken, 468-8502, Japan.
3Aichi Brace Co., Ltd. 18-13-Hishiike-cho, Moriyama-ku, Nagoya-shi, Aichi-ken, 463-0045, Japan.
4,5Sanzinkai Asahi Hospital 2090-Azamurahigashi, Shimohara-cho, Kasugai-shi, Aichi-ken, 486-0819, Japan.
Corresponding Author Details: Shingo Shimizu, Assistant Professor, Department of Physical Therapy, Saitama Prefectural University, Faclity of Health Medical and Welfare 820, Sanomiya, Koshigaya-shi, Saitama-ken, 343-8540, Japan.
Received date: 22nd February, 2023
Accepted date: 04th April, 2023
Published date: 07th April, 2023
Citation: Shimizu, S., Katoh, Y., Sabashi, S., Ida, K., & Hanamura, H., (2023). Long-term Effects of Plantar Plate Therapy for Subtalar Joint Valgus Type for One Case Osteoarthritis of the Knee. J Rehab Pract Res, 4(1):144.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
There are many research reports showing that the effect of plantar plate on medial knee OA is effective in the short term, but there are few reports that it is effective for a long period of 6 months or longer. Also although there are many studies on plantar plate in the varus type of the subtalar joint, there are few studies in the valgus type of the subtalar joint. In this study, we investigated the long-term effect of wearing a plantar plate that guides the subtalar joint to a neutral position in patients with the subtalar joint valgus type. The case is an elderly female diagnosed with bilateral knee osteoarthritis. The case is an elderly female diagnosed with bilateral knee osteoarthritis. X-ray evaluation was right III, left III in KL grade.
The plantar plate was evaluated by comparing the 10 m maximum effort walking time and pain evaluation VAS, the total consumption and the number of steps in one week without and immediately after wearing the plantar plate. In order to examine the long-term effects, functional evaluation was performed 3 months, 6 months, and 12 months after the installation of the plantar plate.
As a result, 10m walking time and walking pain improved, suggesting improvement in long-term walking ability after 3 months, 6 months, and 12 months. In addition, SF36.v2, a health-related QOL evaluation scale, total consumption, and number of steps improved, and a weight loss effect was obtained. Based on the above, it is suggested that the manufactured plantar plate is effective for a long period of time. I thought For cases in which the subtalar joint is valgus, a plantar plate that induces varus to the subtalar joint is more suitable than a lateral wedge-shaped plantar plate that induces valgus to the subtalar joint.
Key words: Knee osteoarthritis, Subtalar joint, Neutral, Plantar plate, Long term effect
Background and purpose
There are few reports on the long-term effects of lateral wedge- shaped plantar plate that induce valgus of the subtalar joint [1-6]. There is a previous study showing that plantar plate do not have long term effects on knee osteoarthritis(OA) [7]. According to Shimizu et al, the reported found that setting the valgus induction for the subtalar joint varus type and conversely setting the varus induction for the subtalar joint valgus type was short-term but effective [8].
Long-term effects of lateral wedge-shaped plantar plate that induce valgus of the subtalar joint have been observed, but there are currently no reports of long-term effects of plantar plate that induce varus of the subtalar joint. Therefore, we investigated the long-term effect of subtalar joint varus induction for subtalar joint valgus type in one case and report it.
Case introduction
The case is a 78-year-old woman who complained of pain in both knees three years ago, visited a hospital, and was diagnosed with bilateral knee OA medial type. Her physique had a height of 156 cm, a weight of 65 kg, and a Body Mass Index (BMI) of 26.3 kg/ m2. X-ray evaluation showed that the Kellgren-Lawrence (KL) grade was III on the right and III on the left, and narrowing of the joint space was observed. In addition, the femoro-tibial angle (FTA) showed marked varus deformation of 188° to the right and 187° to the left (Fig. 1).
Case Foot Evaluation
The first lateral angle was 30 degrees to the right and 26 degrees to the left, and both hallux valgus deformities were observed [9].
The broad rate was 47.9% on the right and 46.8% on the left, and both transverse arches were lowered. The broad ratio (%) was obtained by dividing the foot width (cm) by the actual foot length (cm) of the line connecting the heel and the second toe. According to Shimizu et al, the broad rate (%) of the broad foot is 40.9% or more as a standard [10] (Fig.2).
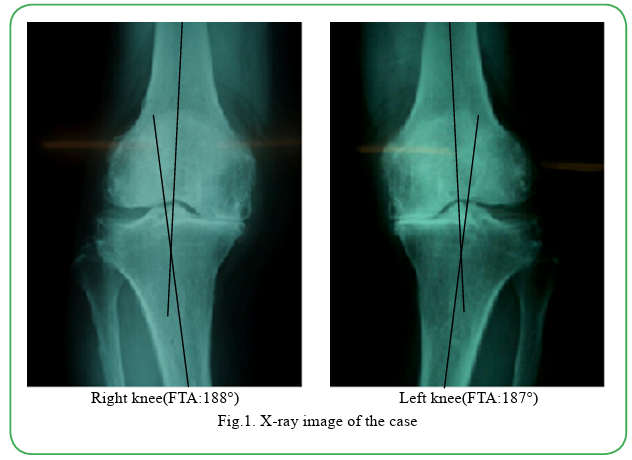
Fig.1. X-ray image of the case

Fig.2. footprint evaluation
The medial longitudinal arch height rate was 11.3% on the right and 10.4% on the left, confirming low left and right arches. The height of the longitudinal arch (%) was calculated by dividing the height of the navicular bone (cm) from the floor by the actual foot length (cm) and multiplying the value by 100. According to Shimizu et al, defined flat foot as having a longitudinal arch efficiency value of 16.4% or less for men and 14.6% or less for women [11].
The calcaneal varus/valgus evaluation was 8 degrees valgus right and 10 degrees valgus left [12,13] (Fig.3). Result left and right foot was confirmed valgus flatfoot and hallux valgus.
How to production the planter plate
The plantar plate was manufactured using a DSIS pad (manufactured by Sanshin Kosan Co., Ltd.) and an EMSOLD pad (manufactured by EMSOLD Co., Ltd.).
DSIS Biaxial Arch Pad®, DSIS LTW Pad®, and DSIS Heel Wedge Pad® were attached so as to cover the talus on the posterior calcaneus of the medial arch, and were manufactured to guide the subtalar joint to varus [14,15]. Using DSISLTW Pad®, DSIS Plainsheet®, and EMSOLD Metatarsal Pad®, while stacking the pads so that the calcaneus is within 2 degrees of 8 degrees of right pronation and 2 degrees of 10 degrees of left pronation. Fine adjustments were made (Fig.4, Fig.5).
In addition, the counter is equipped with a soft material, EMSOLD Pad®, to hold the lateral longitudinal arch, and a DSIS forefoot wedge pad® is attached to the anterolateral side to guide kicking to the big toe [15](Fig.6). The final finish was completed by pasting No Stack Aim glue (thickness about 0.1 mm) on the surface as a finishing material made by Nintoku Trading Company.
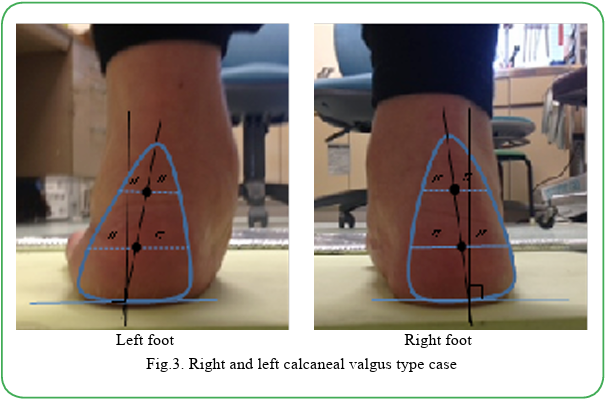
Fig.3. Right and left calcaneal valgus type case
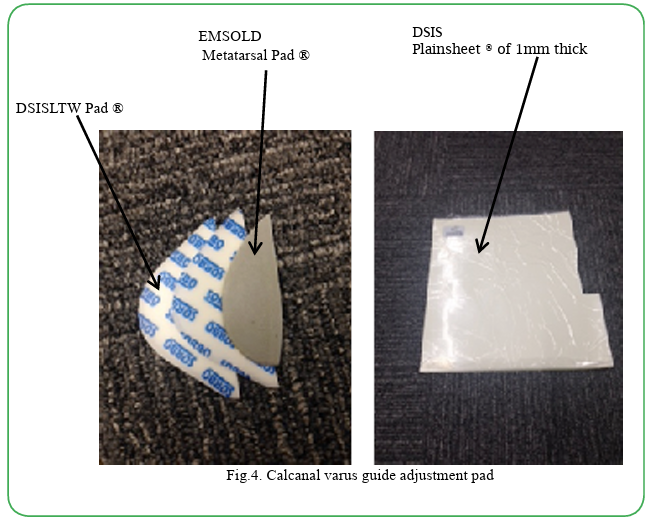
Fig.4. Calcanal varus guide adjustment pad
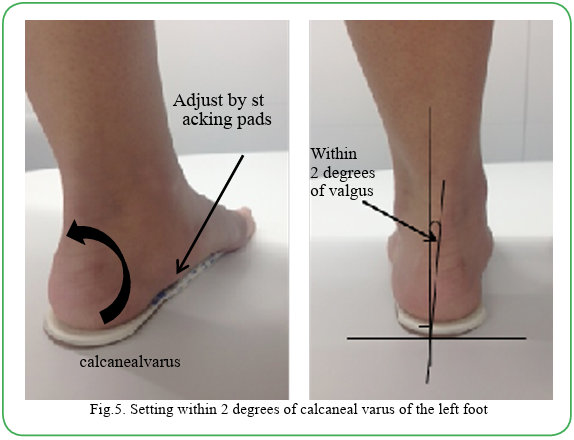
Fig.5. Setting within 2 degrees of calcaneal varus of the left foot
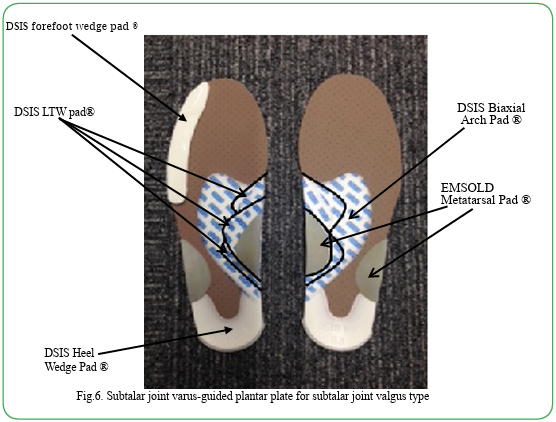
Fig.6. Subtalar joint varus-guided plantar plate for subtalar joint valgus type
How to judge the effect
The plantar plate were evaluated by comparing the 10m maximum effort walking time and pain evaluation Visual Analog Scale (VAS), the total consumption and the number of steps in one week without wearing the plantar plate and immediately after wearing the plantar plate.In order to see the long-term effect, functional evaluation was performed 3 months, 6 months, and 12 months after wearing the plantar plate. Evaluation items are 10m walking time, VAS after 10m walking, hallux valgus angle (first toe side angle), number of steps with a lifestyle recorder (lifestyle recorder Lifecorder GS manufactured by Suzuken), and total consumption. Evaluation of 10m walking was performed 3 times for each measurement and compared from the average value.
For the hallux valgus angle, the lateral angle of the first toe in the footprint was measured using the method of Uchida et al. For quality of life(QOL) evaluation, the health-related QOL rating scale (SF36. v2) was used to confirm the long-term effects of plantar plate. He standards to measure health-related QOL (HRQOL: Health Related Quality of Life) are classified in a comprehensive standard and a disease-specific standard roughly, but SF-36® is placed as the former. The shoes used in this study had to have unworn plantar plate and fit in size and width.
Result
Immediate effects and long -term effects were obtained after wearing the plantar plate. The effect of QOL was obtained after wearing the plantar plate.
Immediate effect of the plantar plate
The average of 3 evaluations of 10m walking was 9.9 seconds for 10m walking without plantar plate, and the VAS score was 72 points for the right knee and 70 points for the left knee.
After wearing the plantar plate the 10m walking time was 8.5 seconds, and the VAS improved to 50 points for the right knee and 40 points for the left knee (Table.1).
An increase in the total amount consumed and the number of steps taken during one week of wearing the plantar plate was observed (Table.1).
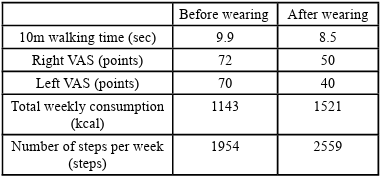
Table.1. Immediate effect of wearing a sole plate set within 2° of calcaneal valgus
Long -term effect of the plantar plate
After 3 months, 6 months, and 12 months after wearing the plantar plate, the VAS improved to 0 points in both knees and the 10m walking time improved to 6.7 seconds. The lateral angle of the first toe was 30 degrees to the right and 26 degrees to the left, but improved to 20 degrees to the right and 21 degrees to the left after 12 months (Table. 2). The Lifecorder GS measurement results showed an average of 1954 steps and a total consumption of 1143 kcal during the first week without wearing plantar plate.
After 12 months of wearing plantar plate, the average number of steps was 3730 steps and the total consumption was 2012 kcal, indicating an increase in energy consumption (Table. 2). Without plantar plate weight was 64 kg, BMI was 26.3 kg/m2, waist (W) was 109.5 cm, hip (H) was 100 cm, and body fat percentage was 34.8%. Twelve months after wearing the plantar plate, the weight decreased to 60 kg, BMI to 24.7 kg/m2, W to 93.0 cm, H to 95.0 cm, and body fat percentage to 31.2% (Table. 2).
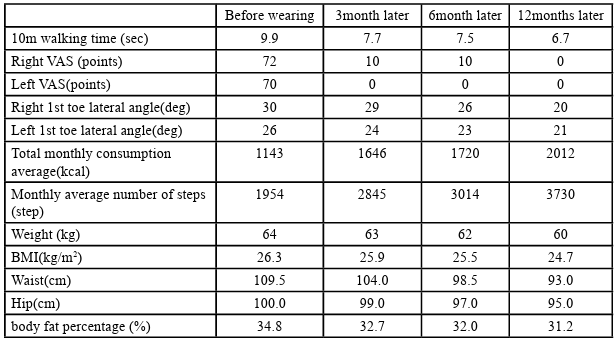
Table.2. Progress of functional evaluation by wearing plantar plate
QOL effect of the plantar plate
SF36.v2 score without plantar plate was 15 points for physical functioning (PF), 0 points for physical role (RP), 32 points for body pain (BP), general well-being, 47 points for general health (GH), 31.3 points for vitality (VT), 25 points for social functioning (SF), 33.3 points for role emotional (RE), 40 points mental health (MH). After 12 months of wearing plantar plate, QOL improved with 65 points for PF, 87.5 points for RP, 74 points for BP, 67 points for GH, 68.8 points for VT, 75 points for SF, 83.3 points for RE, and 85 points for MH (Table.3).
Discussion
The manufactured plantar plate has been suggested to be effective in the long term, and the inversion guidance of the calcaneus valgus to within 2 degrees by the plantar plate reduces pain during walking. The thought it was possible resulting in comfortable walking. For cases in which the subtalar joint is valgus, the varus guide that guides the calcaneus to within 2 degrees of valgus is used instead of the lateral wedge-type plantar plate that induces valgus of the subtalar joint [1-5]. The results supported the effectiveness of the varus guide plantar plate.
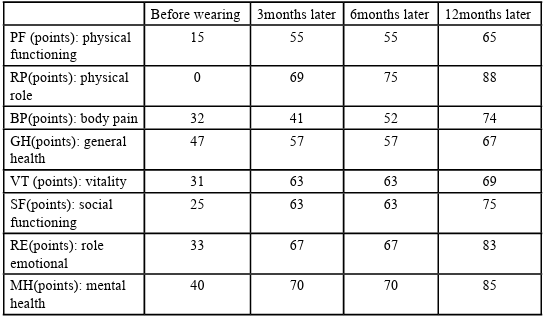
Table.3. Progress of QOL evaluation by wearing a plantar plate
We believe that the use of plantar plate reduced pain during walking and temporarily corrected knee movements, resulting in short-term effects. It is inferred that the longer the wearing period plantar plate, the more the knee movement was improved, and the longer the effect was obtained. The improvement of hallux valgus deformity was considered to be the effect of wearing a plantar plate, and it was thought that the improvement of hallux valgus deformity was related to the improvement of posture during walking, and that walking ability [16], QOL.
Relief of pain during walking by wearing a plantar plate makes going out and walking more enjoyable, and is expected to have the effect of extending healthy life expectancy.
Conclusion
We investigated the long-term effect of wearing a plantar plate on an elderly female diagnosed with bilateral knee osteoarthritis. The case had bilateral flatfoot, bilateral hallux valgus, and bilateral subtalar joint valgus. The plantar plate of the subtalar joint valgus type was manufactured to guide the subtalar joint to neutral (subtalar joint varus guidance). As a result of wearing this plantar plate pain was reduced as an immediate effect, and walking ability was improved. Walking ability, hallux valgus angle, energy consumption, and QOL were evaluated 3 months, 6 months, and 12 months after plantar plate. As a result, improvements were obtained in all items compared to before wearing the plantar plate. A plantar plate that guides the subtalar joint to neutral has a long-term effect on bilateral knee osteoarthritis.
Competing interests:
The authors declare that they have no competing interests.
References
Joaquin, A Barrios, Jaremy R Crenshaw, Todd D Royer, lrene S Davis, (2009). Walking shoes and laterally wedged orthoses in the clinical management of medial tibiofemoral osteoarthritis: a one-year prospective controlled trial, The Knee 16(2), 136-142.View
Marks, R., and Penton, L., (2004). Are foot orthotics efficacious for treating painful medial compartment knee osteoarthritis? A review of the literature, International journal of clinical practice, 58(1), 49-57.View
Yasuda, K., and Sasaki, T., (1987). The mechanics of treatment of the osteoarthritic knee with a wedged insole, Clinical orthopaedics and related research, 215, 162-171.View
Zhang, W., Moskowitz, R., Nuki, G., Abramson, S., Altman, R., & Arden, N., et al, (2008). MOARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines, Osteoarthritis and cartilage, 16(2), 137-162.View
Rana, S Hinman, Kelly Ann Bowles, Kim L Bennell, (2009). Laterally wedged insoles in knee osteoarthritis: do biomechanical effects decline after one month of wear? BMC musculoskeletal disorders 10, 146,1-8.View
Reinoud W Brouwer, Tom M van Raaij, Arianne P Verhagen, Jan A N Verhaar,, Sita M A Bierma-Zeinstra, et al. (2015). Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database of Systematic Reviews,1-29.View
K A Reilly, K L Barker, D Shamley, (2006). A systematic review of lateral wedge orthotics—how useful are they in the management of medial compartment osteoarthritis? The Knee, 13(3), 177-183.View
Shingo, S., Hirokatu, H., & Takehiro, M., Japan(2013). Plantar plate therapy for hindfoot overpronation type and oversupination type of medial type knee osteoarthritis, Journal of Japanese Society of Clinical Orthopedic Surgery, vol.38, no.1, 84-88.
Shingo, S., Takehiro, M., Yukihisa, K., Katunori, S., & Toshihiko, U., Japan (2010). Footprint and assessment of hallux valgus angle and digitus minimus varus angle. Journal of Japanese Society of Foot Surgery 31(2), 35-39.
Shingo, s., Tikara, N., Eiichi, G., & Gorou, O., Japan (2013). nvestigation of the reliability of the spread rate and spread angle, the diagnostic reference value of the spread foot, and the prevention of injury. Sports Industry Research, 23(1), 11-17.View
Shimizu, S., and Yukihisa, K., Japan (2009). Reliability of footprint and arch ratio values for flat foot, clinical biomechanics, 30, 243-248.
Mamoru, O., Japan(1995). Lower Limb Alignment and Biomechanics, Foot heel varus and valgus disorder, joint surgery, 14(7), 857-865.
Shingo, S., Hirokatu, H., Seiji, S., & Yukihisa, K., Japan (2010): Relationship between hindfoot pronation and medial space in medial type knee osteoarthritis, Correlation between pronation heel angle and medial space ratio, shoe medicine, 23(2), 77-80.
Makoto, I., Foot-Ankle, Tsutomu, Y., Japan (2001). Theory and techniques of orthopedic physical therapy, Medical View, 62-83.
Katunori Sasaki Japan (1998). Plantar plate therapy for ankle ligament injuries-dynamic shoe insole system, Orthopedic Disaster Surgery, 41, 1225-1236.
Shingo, S., Hirokatu, H., Seiji, S., & Yukihisa, K., Japan (2009). Relationship between hindfoot pronation and supination in medial knee osteoarthritis and hallux valgus deformity. Shoe Medicine, 22(2), 7-10.