
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 5 (2024), Article ID: JRPR-147
https://doi.org/10.33790/jrpr1100147Research Article
Anatomic Characteristics of Ultrasound Imaging of the Temporomandibular Joint at Rest and in Various Jaw Positions in Healthy Individuals: A Descriptive Study
David J. Dominguese, PHD
Associate Professor, Department of Physical Therapy & Health Science, Bradley University, United States.
Corresponding Author Details: David J. Dominguese, PHD, Associate Professor, Department of Physical Therapy & Health Science, Bradley University, United States.
Received date: 08th December, 2023
Accepted date: 08th January, 2024
Published date: 10th January, 2024
Citation: Dominguese, D. J., (2024). Anatomic Characteristics of Ultrasound Imaging of the Temporomandibular Joint at Rest and in Various Jaw Positions in a Healthy Individual: A Descriptive Study. J Rehab Pract Res, 5(1):147.
Copyright:©2024, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This study examined the temporomandibular joint (TMJ) anatomy and biomechanics using Ultrasound (US) imaging to examine the TMJ anatomy at rest and in various positions of normal jaw movement in healthy individuals. A secondary aim was to describe US imaging parameters used to visually observed the TMJ. The study included 11 participants (8 M and 3 F; 22.9 ± 3.4 yrs) University with no history of TMJ problems. All 11 participants had some atypical anatomy (flat mandibular head, altered articular disc shape, displacement or deformation of the disc during movement) while using US imagining. No participants had current pain or dysfunction and none met the Diagnostic Criteria for Temporomandibular Dysfunction (DC-TMD) classifications for the condition. Most participants denied symptoms during testing, although one participant did have pain with retrusion and another had popping without pain. This study in part has added to the growing interest of using US imaging as modality to investigate the anatomy and biomechanics of the TMJ and the relationship to TMD. Future studies are warranted to examine TMJ anatomy and biomechanics via US imaging in order to provide further recommendations on the techniques and settings for the modality for the end-user.
Keywords: Musculoskeletal, Anatomy, Biomechanics, Diagnostic imaging, TMD, Physical Therapy
Introduction
Temporomandibular disorder (TMD) refers to heterogenous pathologies or dysfunctions impacting the temporomandibular joint (TMJ), masticatory muscles, and associated musculoskeletal and neurovascular structures [1]. Dentists, physical therapists, chiropractors, and medical doctors evaluate and treat individuals with TMD. As part of the examination, the Diagnostic Criteria for TMD (DC-TMD) classification system [2] is used to lead clinicians to broad diagnostic categories of myalgia, arthralgia, disc displacement with reduction, disc displacement without reduction, and subluxation. While the diagnosis of TMD is made primarily via clinical presentation (pain in the jaw, head, and neck regions, headache, periauricular pain, tinnitus, limited jaw opening, and loss of function) [1,3], anatomy and biomechanical function and dysfunction are relevant to both examination and treatment.
The TMJ is a true synovial joint. An avascular fibrocartilaginous disc divides the joint into two functional sections. The disc is firmly attached to the mandibular condyle on all sides by ligaments, capsule, and retrodiscal tissue. Opening of the mouth begins with rotation of the lower compartment of the joint followed by anterior translation [1,3]. Under normal conditions, the disc moves with the mandibular condyle during translation, maintaining a functional relationship in which the center of the disc is in contact with the superior surface of the mandibular condyle [1]. Normal function of the jaw in movement requires simultaneous motion of both the right and left joints. Dysfunction can occur when the disc no longer maintains the functional relationship with the condyle or when one joint is more or less mobile than the other.
The use of radiological imaging in TMD is considered a routine part of examination by dental practitioners [2]. Magnetic resonance imaging (MRI) is considered the gold standard in examining the disc and observing inflammation. Computerized tomography (CT) has been used to observe bone/joint pathology [4]. Ultrasound (US) imaging can also be used to examine the TMJ and assist in diagnosis of disc displacement [4-6] joint effusion [4], condylar change, and condylar mobility [7]. While US imaging is not the most common imaging modality for the TMJ, Friedman et al found 100% specificity and 79% sensitivity with few false negative results examining disc displacement and other relevant anatomy [8].
Musculoskeletal (MS) US imaging is becoming more prevalent with medical providers due to lower cost and improved accessibility [4]. The application of US imaging is taught in some fashion in Doctor of Physical Therapy (DPT) education programs and is becoming more common in physical therapy clinical practice for both examination and treatment purposes [9]. While administration of US and interpretation of results can be limited based on studies on adopted standards and experience of the end-user; the real-time evaluation of anatomy at rest and with movement is an important benefit [4,9]. The use of US imaging can help clinicians visualize the biomechanical relationship between the disc and mandibular condyle at rest and during movement. The modality has been used to examine joint space relative to mobility and range of motion (ROM) of the jaw [10,11]. Understanding anatomy, biomechanics, and how jaw movement might relate to anatomy can assist clinicians with examination and treatment options for individuals with TMD. This study examined the TMJ anatomy and biomechanics via US imaging. The primary aim was to examine the TMJ anatomy at rest and in various positions of normal jaw movement in healthy individuals. A secondary aim was to describe US imaging parameters used to visually observe the TMJ anatomy to provide clarity for replication in the clinic.
Methods
The study was approved in the fall of 2022 by the University Internal Review Board for research with human subjects (IRB #: 22 018 Participants were recruited through recruitment flyers, emails, and word of mouth. Recruitment was delayed due to the Covid-19 pandemic. Data collection took place in a controlled laboratory setting at a mid-size university in Illinois in 2022 and early 2023. All participants provided informed consent.
Healthy university students aged 18-30 were included if they agreed to follow Center for Disease Control and Prevention (CDC) and University Guidelines related to the Covid-19 pandemic. Individuals were excluded from the study if they had current pain in the face or jaw, recent dental procedure, a history of TMD or injury to the face, jaw, or neck in the last six months or if they had Covid-19 or any other respiratory illness signs or symptoms of a virus including Covid-19 within the last four weeks to start of the experiment. Participants who were pregnant or could not sit in a chair for 20 minutes comfortably were also excluded. Participants were screened and evaluated for this inclusion criteria via questionnaire. Participants were provided and instructed to wear a surgical face mask, gloves, and a surgeon's cap to cover their hair during the experiment. The research team also wore a mask and gloves during data collection.
In this cross-sectional descriptive analysis, participants came one time only to a controlled laboratory setting. As part of the consent process, participants were informed of the possibility that the US imaging scans could reveal a previously unknown health condition of the face, jaw, and neck. Participants were informed that this may exclude them from the study and that a referral to a physician would be made if indicated.
Procedure and Ultrasound Imaging
There is no standard methodology for attaining and viewing US images of the TMJ in clinical settings. This study provides a general description of methodology for US imaging of the TMJ that can be used in the clinic.
A Terason™ uSmart 3200t (Burlington, MA) US imaging device with a linear, flat 2.54 cm probe was used. The transducer was cleaned and disinfected before and after each participant. Ultrasound/ transmission gel (Parker Aquasonic 100, Fairfield, NJ) was applied to the transducer. Parameters for the ultrasound included a depth of 5cm, frequency of 15 Hz, Omni Beam, dynamic range of 63, Map C, TV Level 3, focal zone and range were set at 2, and the image format was set at rectangle. The standards and settings used in this study were established in a pilot performed by the research team to allow the best image quality of relevant TMJ anatomy. The investigator is trained in musculoskeletal US imaging and confirmed the placement of the transducer and the validity of each image scan during data collection and analysis.
Participants were examined in a seated position and received education regarding the movements they would be asked to do and the expectations for data collection. Participants were instructed to assume a jaw resting position (lips together, teeth apart, tongue in the roof of the mouth) and to give a thumbs up when they have assumed the proper position. The ultrasound transducer was placed parallel to the zygomatic arch to examine the TMJ of one side at a time in each of the jaw position conditions (Figure 1). A TheraBite® (Tanawana, NY) Jaw ROM Scale (paper disposable tool) was used to quantify the various jaw positions for imaging (Figure 2).
Participants moved from the resting position into 10 mm opening, 20 mm opening, contralateral deviation, protrusion, and retrusion for the right side and again for the left side (right and left side were recorded separately).
Data from images was summarized in a descriptive fashion. Documentation of results for each movement included a dichotomous yes/normal (score of 1) or no/abnormal (score of 2). The lead investigator examined all images to make these determinations related to the following criteria: appearance of the head of the mandibular condylar at rest (crown or not crown), appearance (deformation) of the articular disc of the TMJ (normal or abnormal), displacement of the articular disc (movement and tilt beyond the posterior angle of the condyle present (yes) or absent (no), articular disc deformation (flattens; yes/no), and articular disc displacement and deformation. Additional documentation was noted if participants reported pain, clicking, grinding, or locking with any testing.
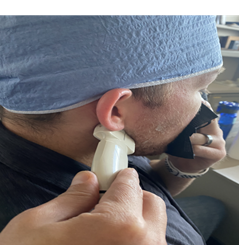
Figure 1: US Transducer Placement

Figure 2: The TheraBite® ROM Scale

Figure 3: Image scan of the TMJ
Results
The study included 11 participants: eight male and three female University students. Descriptive means are as follows: age 22.9 (±3.4), height 69.8 inches (± 3.2), weight 176.4 pounds (± 18.6). No participants were excluded as all interested individuals met inclusion criteria without a reason to exclude.
In this cross-sectional examination, all participants had some atypical anatomy (flat mandibular head, altered articular disc shape, displacement or deformation of the disc during movement) in US imagining, at least one position (at rest or during jaw movements). However, no participants had current pain/dysfunction and none met the DC-TMD classifications for the condition. Most participants denied symptoms during testing, although one participant did have pain with retrusion and another had popping without pain.
Results of individual images in each position of testing were recorded as yes/no for normal, typical)/abnormal (atypical) or condition present/absent as noted in methods. See Table 1 and Table 2 for summaries right and left (respectively) TMJ US images. At rest, 45-64% of participants had a typical appearance (shape) of the mandibular condyle and 45-55% had a typical appearance (shape) of the articular disc. No participants had movement of the disc beyond the angle of the condyle at rest, however 27% had deformation or flattening of the disc at rest.
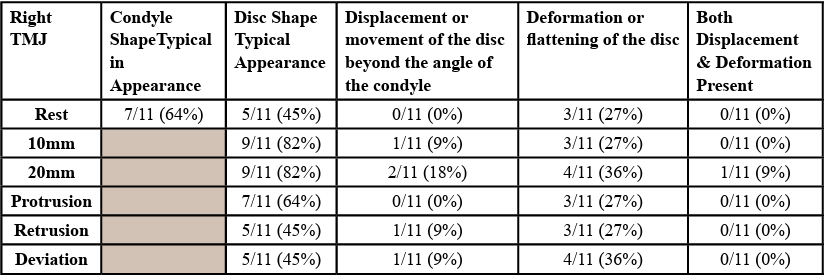
Table 1: Right TMJ Results
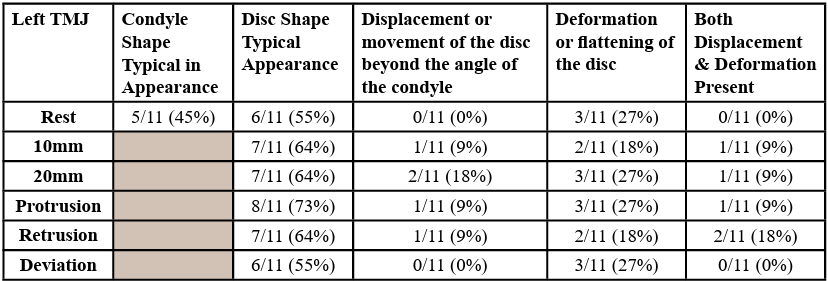
Table 2: Left TMJ Results
During the opening motion of the jaw, we expect to see rotation followed by anterior translation. The disc should remain in contact with the mandibular condyle. While no participants had movement of the disc beyond the angle of the condyle at rest, 1/11 had displacement of the disc at 10 mm of opening and 2/11 had displacement at 20 mm of opening. During movements of protrusion, retrusion or deviation away, 0-9% (0-1 participants) had disc displacement. Deformation or flattening of the disc was noted in 18-36% (2-4 participants) with the various movements.
One participant had jaw pain with retrusion despite no resting pain or history of TMD in the last 6 months. However, the participant did have a history of headaches in the last 4 weeks and a history of TMD > 6 months ago. Pain stopped when testing stopped. Another participant had clicking in the jaw with deviation during opening. This participant had no pain and no history of pain or TMD. Of note, there were no individuals with abnormal findings on exam or in US imaging that required referral.
Discussion
Anatomical changes may be noted in imaging of healthy individuals as well as those with a diagnosis of TMD. As with other chronic pain conditions, radiographic or image findings demonstrating abnormal positioning of the TMJ disc or other anatomical abnormalities are poorly correlated with pain, tenderness, and/or dysfunction [1,12]. In a cross-sectional study looking at imaging findings and pain, function, and disability associated with TMD, researchers concluded there was no relationship found between joint status and pain or dysfunction. While imaging is common, Stern et al [13] suggested imaging may not be necessary in all TMD patients. Imaging can help visualize anatomy, however, treatment often remains unchanged [14] despite results of imaging. The individuals in this study did not have symptoms of TMD, yet anatomical changes were noted.
While authors understand and appreciate the nuanced relationships between anatomy/biomechanics and pain/function, understanding anatomy and biomechanical relationships is still important. Implementing US imaging in the clinical setting can allow clinicians to see anatomy and biomechanics in real-time and overtime with their treatment for individuals with TMD. Ultrasound imaging at rest and during normal motion or exercises can help providers understand what may and may not be ‘typical’ anatomical or biomechanical change during motion. A case report by Ho et al [15] describes the space between the articular capsule and the mandibular condyle in a patient with TMJ ankylosis before and after joint mobilization and exercise focused on joint mobility. A change in space correlated with a change in mouth opening. Some interventions described for individuals with TMD attempt to focus on the typical biomechanical relationships described with typical movement. These include exercises like controlled opening (opening with the tongue in the roof of the mouth) [16] or retrusion before opening as well as manual therapy interventions like those described as ‘recapturing’ the disc [17]. Future research and examination of TMJ US imaging during rest and active movements of the jaw can improve understanding of biomechanics that may change in various positions of active movement or exercise targeted at improving biomechanical relationships. The specificity of these exercises could be better analyzed to determine accuracy and relative importance to change in function or pain.
Limitations in this investigation include a small sample size, difficulty keeping one US imaging setting to achieve good views of anatomy in each position tested, and lack of standardized measurements of anatomy seen via US imaging for the TMJ. Generalizability is quite limited due to the nature of the research design and noted limitations. An additional limitation and in general for US imaging studies, is the movement of the transducer while a body part is moving and trying to capture an image. This can lead to difficulty in the quality of the images and this study was no exception in that challenge.
Conclusion
The TMJ anatomy was visualized with US imaging revealing variations of typical anatomy in 11 healthy participants. Different positions of opening or ROM of the jaw revealed changes in this anatomy as compared to resting positions. The nuanced relationships between anatomy/biomechanics and pain/function make it difficult to draw specific conclusions. However, when someone does seek treatment for pain or dysfunction, the anatomy and biomechanics may have relevance in examination or treatment. This study and other related studies can help to provide to the growing interest of using US imaging as modality to investigate the anatomy and biomechanics of the TMJ and the relationship to TMD. Future studies are needed to examine TMJ anatomy and biomechanics via US imaging to add to the findings and to provide further recommendations on the techniques and settings for the modality.
Conflict of interest:
Contributing author has no conflicts or competing of interest to report.
Acknowledgements
The authors would like to sincerely thank Bre Reynolds PhD, DPT and Kyle Cottone DPT, PT for their work on piloting the study, collecting data, and providing feedback on the study methods, data collection and acquisition. In addition, I would like to thank Kelly Hernandez SPT and Melissa Adrian SPT for their efforts on all facets of this study from the inception of the study and to its conclusion. Most importantly for the honor to mentor and work with both students.
References
Shaffer, S. M., Brismee, J. M., Sizer, P. S., & Courtney, C. A. (2014). Temporomandibular disorders. Part 1: anatomy and examination/diagnosis. J Man Manip Ther, 22(1), 2-12. doi:10. 1179/2042618613Y.0000000060View
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J.-P., . . . Jensen, R. (2014). Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. Journal of Oral & Facial Pain & Headache, 28(1), 6-27. doi:10.11607/jop.1151View
Harrison, A. L., Thorp, J. N., & Ritzline, P. D. (2014). A Proposed Diagnostic Classification of Patients with Temporomandibular Disorders: Implications for Physical Therapists. J Orthop Sports Phys Ther, 44(3), 182-197. doi:10.2519/jospt.2014.4847View
Almeida, F. T., Pacheco-Pereira, C., Flores-Mir, C., Le, L. H., Jaremko, J. L., & Major, P. W. (2019). Diagnostic ultrasound assessment of temporomandibular joints: a systematic review and meta-analysis. Dentomaxillofac Radiol, 48(2), 20180144. doi:10.1259/dmfr.20180144View
Dong, X. Y., He, S., Zhu, L., Dong, T. Y., Pan, S. S., Tang, L. J., & Zhu, Z. F. (2015). The diagnostic value of high-resolution ultrasonography for the detection of anterior disc displacement of the temporomandibular joint: a meta-analysis employing the HSROC statistical model. Int J Oral Maxillofac Surg, 44(7), 852-858. doi:10.1016/j.ijom.2015.01.012
Su, N., van Wijk, A. J., Visscher, C. M., Lobbezoo, F., & van der Heijden, G. (2018). Diagnostic value of ultrasonography for the detection of disc displacements in the temporomandibular joint: a systematic review and meta-analysis. Clinical Oral Investigations, 22(7), 2599-2614. doi:10.1007/s00784-018 2359-4View
Chen, H. Y., Wu, S. K., Lu, C. C., You, J. Y., & Lai, C. L. (2014). Assessing the Mobility of the Mandibular Condyle by Sonography. Patient Prefer Adherence, 8, 1419-1425. doi:10.2147/PPA.S72532View
Friedman, S. N., Grushka, M., Beituni, H. K., Rehman, M., Bressler, H. B., & Friedman, L. (2020). Advanced Ultrasound Screening for Temporomandibular Joint (TMJ) Internal Derangement. Radiol Res Pract, 2020, 1809690. doi:10.1155/2020/1809690View
Whittaker, J. L., Ellis, R., Hodges, P. W., C, O. S., Hides, J., Fernandez-Carnero, S., Stokes, M. J. (2019). Imaging with ultrasound in physical therapy: What is the PT's scope of practice? A competency-based educational model and training recommendations. British Journal of Sports Medicine, 53(23), 1447-1453. doi:10.1136/bjsports-2018-100193View
Elias, F. M., Birman, E. G., Matsuda, C. K., Oliveira, I. R., & Jorge, W. A. (2006). Ultrasonographic findings in normal temporomandibular joints. Brazilian Oral Research, 20(1), 25 32. doi:10.1590/s1806-83242006000100006View
Ho, K. Y., Ho, S., & Colletti, P. M. (2016). Use of Ultrasonography for Assessing Treatment Efficacy in a Case With Ankylosis of the Temporomandibular Joint. J Orthop Sports Phys Ther, 46(3), 225. doi:10.2519/jospt.2016.0404View
Chantaracherd, P., John, M. T., Hodges, J. S., & Schiffman, E. L. (2015). Temporomandibular Joint Disorders' Impact on Pain, Function, and Disability. J Dent Res, 94(3 Suppl), 79S-86S. doi:10.1177/0022034514565793View
Stern, I., & Greenberg, M. S. (2013). Clinical Assessment of Patients with Orofacial Pain and Temporomandibular Disorders. Dental Clinics of North America, 57(3), 393-404. doi:10.1016/j. cden.2013.04.002View
Ghurye, S., & McMillan, R. (2015). Pain-Related Temporomandibular Disorder - Current Perspectives and Evidence-Based Management. Dental Update, 42(6), 533-533. Retrieved from http://search.ebscohost.com/login.aspx?direct=t rue&db=ccm&AN=109003705&site=ehost-liveView
Ho, K.-Y., Ho, S., & Colletti, P. M. (2016). Use of Ultrasonography for Assessing Treatment Efficacy in a Case With Ankylosis of the Temporomandibular Joint. Journal of Orthopaedic & Sports Physical Therapy, 46(3), 225-225. doi:10.2519/jospt.2016.0404View
Mulla N, B. V., Kumar S, Rizvi S. (2015). Effectiveness of Rocabado's Technique for Subjects with Temporomandibular Joint Dysfunction- A Single Blind Study. Int J Physiother, 21(1), 365-375. View
Lindfors, E., Arima, T., Baad-Hansen, L., Bakke, M., De Laat, A., Giannakopoulos, N. N., . . . Ernberg, M. (2019). Jaw Exercises in the Treatment of Temporomandibular Disorders An International Modified Delphi Study. J Oral Facial Pain Headache, 33(4), 389–398. doi:10.11607/ofph.2359View