
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 6 (2025), Article ID: JRPR-155
https://doi.org/10.33790/jrpr1100155Research Article
Blood Flow Restriction on Lower Extremity Increased Neuromuscular Timing on Proximal Musculature While Performing a Resisted Sled Push in Healthy Subjects
Luciano Garcia III, PT, ScD, OCS, COMT, Adam Bender, SPT, Aubrey Dillon, SPT, Rae Edwards, SPT, Brianna Ramirez, SPT, and Martin Rosario*, PT, PhD, CSFI, ATRIC
1 Texas Woman’s University, Physical Therapy Program, Dallas Campus; Texas, United States.
Corresponding Author Details: Martin Rosario, PT, PhD, CSFI, ATRIC, Assistant Professor, Texas Woman’s University, Physical Therapy Program, Dallas Campus, 5500 Southwestern Medical Ave. Dallas, TX 75235-7299. United States.
Received date: 12th September, 2024
Accepted date: 20th January, 2025
Published date: 22nd January, 2025
Citation: Garcia, L., Bender, A., Dillon, A., Edwards, R., Ramirez, B., & Rosario, M., (2025). Blood Flow Restriction on Lower Extremity Increased Neuromuscular timing on Proximal Musculature While Performing a Resisted Sled Push in Healthy Subjects. J Rehab Pract Res, 6(1):154.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Blood flow restriction (BFR) is beneficial in various settings; however, the neuromuscular activation during low-speed tasks is poorly understood.
Objective: This study investigated the effect of BFR on the electromyography (EMG) timing of six lower extremities (LE) musculature during a resisted sled pushing activity at two different walking speeds, 80 bpm and 140 bpm at the beginning (acceleration) of the walking tasks.
Methods: This study recruited 32 healthy individuals, an average of 23.8 years old (±1.42 SD). The study utilized surface electromyography on the dominant lower extremity (LE) of subjects, focusing on the tibialis anterior (TA), gastrocnemius (GA), vastus medialis (VM), biceps femoris (BF), gluteus maximus (GMax), and gluteus medius (GMed). Participants pushed a resistive sled for 40 feet across three trials at 80 and 140 beats per minute. Researchers repeated all trials after applying BFR at 80% limb occlusion pressure. The analysis focused on the time to peak, decay, and interpeak of the first three muscle activations in each trial.
Statistical Analysis: A 2x6 (BFR group and muscle) repeated measures multivariate analysis of variance (MANOVA) tested for significant interactions and main effects during each speed and BFR condition. The time to peak, decay, and interpeak EMG values are presented for each muscle pairing.
Results: Statistical analysis of the MANOVA revealed significant decay at 80 bpm with GMax regarding BFR (p=.018). Also, the nter peak of the at140 bpm (p=.013) for the biceps femoris.
Conclusion: At 80 bpm, BFR affected the GMax regarding EMG decay. At 140 bpm, BFR significantly affected the biceps femoris, with increased interpeak values due to BFR. Rehabilitation specialists can use these findings to accurately target GMax and biceps femoris activation patterns with BFR use, most notably using shorter training intervals to reduce fatigue.
Keywords: Electromyography, Blood Flow Restriction, Sled Pushing, Timing
Liteature Review/ Background
Physical activity and exercise are essential components of a healthy lifestyle. As the United States population ages, activity participation becomes more important. Increased exercise participation can help combat the recent increase in heart disease and diabetes-related illness [1]. Physical activity has improved cardiovascular fitness, muscle tone, and emotional outlook as more jobs become sedentary and remote.
Exercise training can be divided into lower-level and higher-level impacts. Low-level types of exercise can include aerobic and low level circuit training, and (https://aptageriatrics.org)—higher-level types of exercise include HIIT, plyometrics, and CrossFit. In some populations, such as people with mobility dysfunction, the ability to perform higher-level exercises can be restricted; thus, a lower-level training option is warranted. An alternative to heavy-load exercises is to add low load with blood flow restriction (BFR). For instance, Fatela et al. [2] incorporate light resistance training in 20% of the subjects, with a maximum of one repetition of unilateral knee extension. Researchers f ound that although training was at a lower load, subjects could increase their muscle activity through BFR training.
Electromyography (EMG) has been studied during resistive exercises, such as pushing components as illustrated by Rosario and Mathis., [3]. With EMG, surface sensors capture minute electrical activity produced during voluntary muscle contraction. For our study, EMG will be used to analyze the timing of muscle contractions during a functional activity. Since multiple muscle contractions of the same muscle are necessary during repeated activity, such as walking, the timing aspect of each contraction and the intensity of subsequent contractions will be studied. Rosario et al. [4] found that while walking while pushing a sled, more proximal LE muscle activation was evident, and more trunk muscle activation when the activity was elevated to running and pushing the sled. Similarly, Rosario et al. [5] demonstrated that using a resistance sled at different speeds increases the distal lower extremity (LE) recruitment as the task speed increases.
Regarding gait, the timing of muscle activation depends on the speed of the activity; for distal musculatures such as the gastrocnemius, the force-length and force-velocity of the muscle decrease as speed increases, favoring a cumulative activation throughout the lower extremity [6]. Similar to the above study, Alcaraz et al. [7] in their systematic review, found improved sprint performance through a resistive sled, most notably during the acceleration phase.
In recent years, BFR training has gained considerable popularity as a treatment method. Blood flow resistance training uses a pneumatic tourniquet system applied to the upper thigh to block the femoral artery and restrict blood supply to the lower leg. The muscle adapts to the lack of oxygen by changing skeletal muscle activation from slow oxidative fibers to fast oxidative–glycolytic fibers, similar to the effects seen in high-intensity exercise [8]. One advantage of BFR training is its ability to boost muscle strength and activation in a shorter period through neuromuscular changes, while longer-range training programs can increase muscle strength through hypertrophy and cross-sectional area increases.
The XPO trainer, produced by Armored Fitness Equipment, LLC in Plano, TX, is a weight sled designed for push-pull exercises that offers steady resistance during walking or running. The sled trainer offers a dependable resistance that adjusts to various movement speeds. Rosario et al. [5] examined the effects of pushing the sled at speeds chosen by the participants and found altered lower extremity muscle activation, mainly in the gastrocnemius. Mathis et al. [9] compared the muscle amplitude of the LE while comparing walking to running while pushing the XPO Trainer. The study revealed that pushing the sled resulted in more significant activation of the quadriceps than the hamstring, gastrocnemius, and tibialis anterior. Garcia et al. [10], researchers discovered that participants showed greater activation of the gastrocnemius and vastus medialis muscles when they walked at a faster pace and pushed the sled.
The acceleration aspect of the EMG activity will be the focus of this study regarding the timing of muscle activation during functional activity. In order to accurately capture adaptations in muscle activation related to acceleration, parameters we will explore include the time to the first peak, decay of the signal, and interpeak pulse. Rosario et al. [4] examined the timing aspects of thoracolumbar and LE activation levels at two different speeds of sled pushing. The authors found that the proximal gluteal muscles were more active at the walking pushing speed, while the thoracic muscles were more active at the running speed.
As suggested by Rosario et al. and Garcia et al. (2025), it is imperative to identify how the timing of LE muscle activation responds to BFR while pushing a sled. These findings can help elucidate exercise principles in rehabilitation and exercise science. To maximize BFR's low-level intensity training benefits, patients unable to perform high-level exercises would benefit from learning to adjust training principles using BFR when performing a sled pushing walking activity.
Our study will attempt to analyze the timing pattern of six LE musculature EMG firing patterns during a resisted walking activity at two different prescribed speeds. Based on the work of Rosario et al. [5], we hypothesize that as the speed of walking increases, a faster peak recruitment of proximal to distal muscles pattern will occur in the acceleration portion of the walkway. Consequently, these proximal muscles will display a faster onset and time-to-peak characteristic. Therefore, we aim to highlight the effects of different walking speeds and BFR on this EMG timing pattern during the acceleration component in healthy young adults.
Methods
Thirty-two individuals participated in the study from the local Institute of Health Sciences. Participants had to be between 18 and 45 years old, capable of walking and pushing a sled, and able to follow commands and maintain the required tempo. The exclusion criteria encompassed standard contraindications for BFR, such as a history of vascular or clotting disorders, recent muscle injuries, skin problems, sickle cell disease, peripheral nerve damage, and any painful lower extremity conditions.
While the subject was unaware, researchers delivered a swift backward force to the subject's torso to ascertain which leg was dominant. The leg that was used for the stepping strategy was identified as the dominant leg [11]. To prepare for the trials, the researchers cleaned the area on the subject's skin with an alcohol wipe where they planned to attach electrodes, weighed them, measured their height, checked their blood pressure, and noted the circumference of their proximal thigh.
After placement of the appropriate EMG electrodes, Participants executed three repetitions of walking 40 feet while pushing the XP sled at 140 beats per minute (BPM), then continued with three repetitions at 80 BPM. A metronome helped the subject maintain the rhythm. Researchers randomized the order for alternating subjects to start with slow or fast repetitions. Following the first six repetitions, the participants took a 3-minute rest break during which they adjusted their BFR personal tourniquet pressure (PTP) using Delphi Systems USA while lying down. During the BFR trials, the subjects experienced an 80% occlusion pressure for their BFR pressure, as noted by Abbas [12]. After applying pressure, the subjects repeated the same six trials, now including BFR.
Data Analysis
All EMG data analyses were performed using Delsys EMGWorks Analysis v4.8.0 software (Delsys Inc., USA). In this study, we utilized the raw EMG files from previously gathered data at 1,000Hz for TA, GA, VM, BF, GMax, and GMed, as previously published by Rosario et al., 2022. Upon analysis, raw data was normalized to compare pre and post-BFR.
Researchers identified and analyzed each trial's first three peak activations to determine the acceleration of each subject's contraction with and without BFR. In the study, the variables analyzed were the time to onset (onset) of each of these contractions, as well as maximal peak activation (TP) of muscle activation, decay or end point of muscle activation. Since each trial was performed three times, an average was taken for each condition. Researchers used SPSS 28.0.1.0 (IBM SPSS Statistics) for the above calculations with a p-value of 0.05 using a MANOVA for all variables of interest.
Results
Subject demographics with standard deviations were as follows: the average age of the 32 subjects was 23.8 (±1.42 SD) years old, 17 female and 15 male, 155 pounds (±29.89 SD), and 66 inches (±3.61 SD) in height.
Statistical analysis of the MANOVA revealed that decay at 80 bpm for the GMax and inter peak for BFR was at 140 bpm (p=.013) for the biceps femoris was also significant at 80 bpm (p=.045).
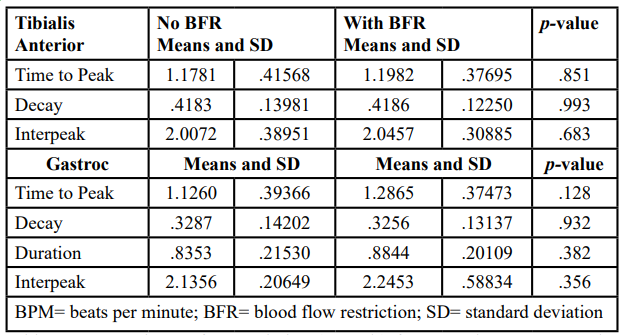
Table 1a: Comparisons of EMG timing (seconds) for TA and GA among tasks. Results of a MANOVA were performed comparing 80 bpm resisted walking without BFR to with BFR with significance level was set at p=0.05.
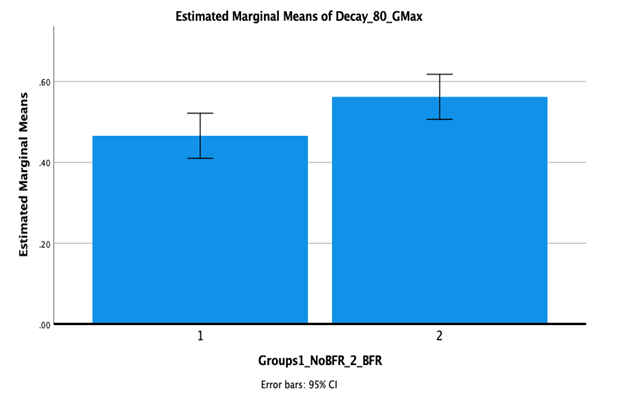
Figure 1
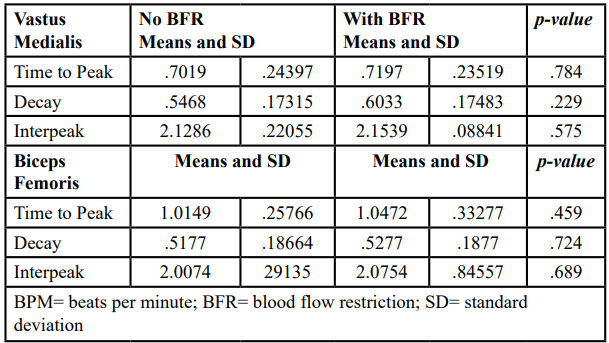
Table 1b: Comparisons of EMG timing (seconds) for VM and BF among tasks. Results of a MANOVA were performed comparing 80 bpm resisted walking with and without BFR with significance level was set at p=0.05.
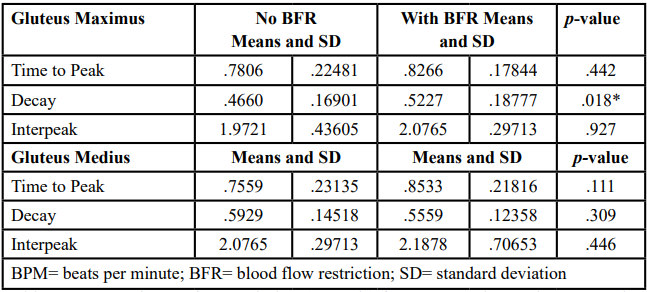
Table 1c: Comparisons of EMG timing (seconds) for GMax and GMed among tasks. Results of a MANOVA were performed comparing 80 bpm resisted walking without and with BFR with significance level was set at p=0.05.
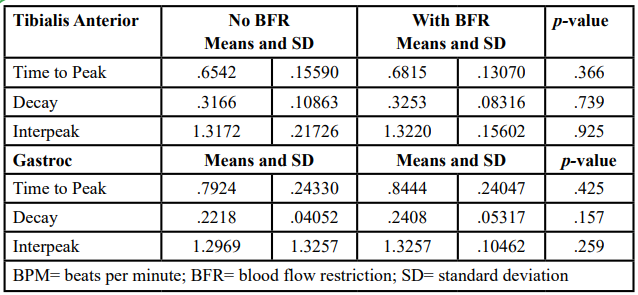
Table 2a: Comparisons of EMG timing (seconds) for TA and GA among tasks. Results of a MANOVA were performed comparing 140 bpm resisted walking without BFR to with BFR with significance level was set at p=0.05.
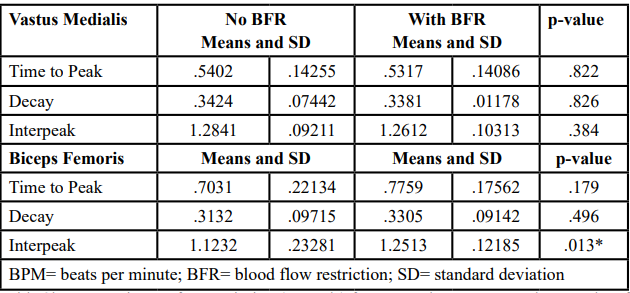
Table 2b: Comparisons of EMG timing (seconds) for VM and BF among tasks. Results of a MANOVA were performed comparing 140 bpm resisted walking with and without BFR with significance level was set at p=0.05.
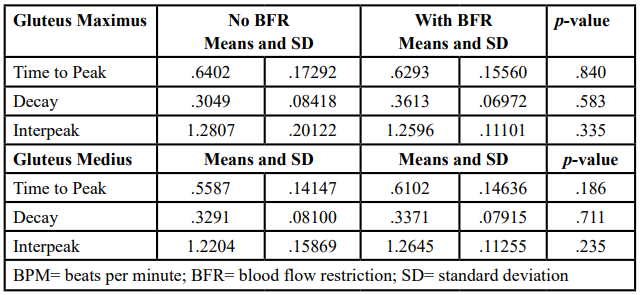
Table 2c: Comparisons of EMG timing (seconds) for GMax and GMed among tasks. Results of a MANOVA were performed comparing 140 bpm resisted walking without and with BFR with significance level was set at p=0.05.
Discussion
As noted earlier, our objective for this work was to determine the effect BFR had on resisted walking at two different speeds during acceleration. The effects of BFR were most noted with GMax and BF musculature, not with the distal lower leg musculature, thus partially supporting our study hypothesis.
This research showed that out of the four data points of acceleration studied, only decay and interpeak were significant for any condition, leading to a proposed lack of oxygen consequence from the BFR. Our BFR findings correlate with the shorter decay aspect of fatigue with fast cycling [13] and wheelchair basketball played by subjects with spinal cord injury [14]. On the other hand, the biceps femoris interpeak activation was discovered to be significant at the 140 bpm condition in favor of BFR. These findings suggest that with BFR, the biceps femoris had a significantly larger interpeak distance than the non-BFR trials, predominantly at a faster speed. An explanation for this could be a decrease in hamstring recruitment needed at a faster speed, possibly for the resisted late swing phases of walking. The above results correlate with the findings of Lee et al. [15] when analyzing subjects with knee osteoarthritis walking at faster than self-selected speeds.
Our findings also suggest that at the slower speed of 80 bpm, the gluteus maximus could recruit with greater activation when using BFR. Hora et al. [16] found that a crouch posture gait activated more gluteal and thigh musculature over more distal LE musculature. Since the XPO Trainer Sled resistance is speed dependent, subjects may have adapted a more flexed posture position at the slower speed of 80 bpm, engaging further the gluteal muscles and therefore needing more time to do so at the 140 bpm condition. The above finding is supported by the work of Sturdy et al. 2024 who found increased gluteus maximus activation when walking flexed uphill or with a weighted backpack.
Rosario et al. (2024) stated that with BFR analysis, lower limb musculature has different activation patterns. Muscles proximal to the cuff may respond differently than distal ones. Lambert et al. [17] found that with the upper extremity, rotator cuff muscles can increase strength, lean mass, and muscular endurance with BFR, even though the BFR cuff is distal to the target musculature. This "upstream" influence may differ from those distal to the cuff. Our outcomes highlight that one upstream, gluteus maximus, and one downstream muscle, biceps femoris, responded to the application of BFR. Similar to our discovery, Sun and Yang [18] also found that BFR to the LE influenced gluteus maximus activation, translating into increased vertical jumping height in female footballers.
Another discovery of the recent study showed that proximal and distal muscle activation responds to a preemptive trunk contraction. Since the GMax is located proximally on the trunk, trunk co-contractions may influence its activation. Since the lumbar musculature contracts in a feedforward manner prior to extremity movements [19], the GMax may benefit from this increased trunk activation. As noted earlier, Rosario et al. [20] found increased GMed and GMax while pushing the XPO sled at a walking speed, then increased thoracic muscle activation at the running speed. McCormick et al. [21] found increased lumbar and proximal LE muscle activation when performing squat variations with preemptive abdominal contraction. These findings may help clinicians understand proximal muscles' role in trunk stability.
Regarding the distal pairing of muscles, no significance was found between the TA and GA. Since muscle timing was the primary variable studied, the effects of BFR might have needed more time to reach these distal muscles, regardless of the activity speed. Valencia et al. [22] studied lower limb timing during rearfoot and forefoot running, finding differences in GA and TA timing delays at these faster running speeds. Similarly, Labanca et al. 2021 found increased TA timing activation when the activity was unplanned when studying subjects with chronic ankle instability. These results suggest that distal timing activations may need a faster or unplanned activity to create proper activations.
Interestingly, the gluteus medius did not exhibit any BFR timing effects. As the role of a lateral stabilizer, the GMed should increase activation during all stance phases of gait. However, Bolgla et al. [23] demonstrated that subjects with patellofemoral pain exhibited delayed GMed timing activation during the loading response and single limb stance of stair descending, but at a higher amplitude than the vast musculature. Similarly, Hart et al. [24] found delayed GMed activation when examining subjects with knee osteoarthritis using a brace after anterior cruciate ligament surgery, as well as Semciw et al. [25] when examining running with subjects with patellofemoral pain.
BFR conditions stem from various physiological mechanisms and adaptations linked to blood flow restriction. As an illustration, lessened oxygen levels and delayed muscle contraction recovery result in a hypoxic setting. Hypoxia can delay the recovery of muscle fibers after contractions as metabolites accumulate, which changes the adaptation strategy needed to reach peak muscle activation again in repetitive pushing tasks [26]. A different mechanism pertains to modified neuromuscular recruitment patterns resulting from blood flow restriction. In BFR, the body can modify its strategies for engaging motor units due to reduced blood circulation. This approach might involve activating more slow-twitch fibers, adjusting the timing of muscle activation to maintain effort, and modifying time variables as the neuromuscular system adapts to limited conditions [27].
Conclusions
The current study's contribution was to identify the neuromuscular adaptation during BFR, especially during the acceleration part of the sled-pushing walkway. Our study found increased gluteus maximus activation and decay at the slower walking speed while increasing bicep femoris interpeak distance with the addition of BFR. This knowledge can be applied to the clinical setting with BFR training regimes for increased gluteus maximus maximus strengthening for patients with patellofemoral or lower back pain at a lower speed focusing on the starting point of gait. Nevertheless, the current study looked at one-time acute neuromuscular interaction with BFR and muscle activation. Although BFR changes the muscle activity of said muscle, the long-term effect needs to be examined to determine a clear mechanism and activation pattern.
Future studies should investigate the inter-peak time to comprehensively illustrate the impact of BFR on muscle activity during walking and pushing. Additionally, future examinations could focus on BFR on the non-dominant LE. Findings could further clarify unilateral dominant LE sports such as soccer or kickball. Similarly, pushing the sled upwards or downwards an incline using our similar protocol could gleam light into longer-term training effects, such as using VO2 max as a dependent variable. Another scenario worth mentioning is incorporating the protocol into a pulling task. Similar to walking backward, a pulling study could determine if BFR affects LE muscle activation patterns in an antagonist recruitment pattern and different concentric and eccentric LE activation patterns. Since walking backward is a more novel activity, speed could affect muscle activation patterns differently than a forward gait. Finally, continuing the current research model into subjects with pathology is warranted. Since this study protocol requires using all musculature from shoulder level inferiorly, examining the effects of shoulder pain or upper thoracic pain with the BFR to the UE or lower back, hip, knee, and foot dysfunction with the BFR to the LE, these findings could help clarify how subjects respond with altered muscle activations secondary to these disorders.
Conflict of interest:
The authors declare no conflict of interest.
References
Palazzuoli, A., Iacoviello, M. (2023). Diabetes leading to heart failure and heart failure leading to diabetes: epidemiological and clinical evidence. Heart Fail Rev 28, 585–596. View
Fatela, P., et al. (2019). Blood Flow Restriction Alters Motor Unit Behavior During Resistance Exercise. Int J Sports Med. 40(9):555-562. doi: 10.1055/a-0888-8816. Epub 2019 Jul 10. View
Rosario, M, Mathis, M., (2020). Lower limb muscle activation and kinematics modifications of young, healthy adults while pushing a variable resistance sled, Journal of Human Sport and Exercise, 16(4) (2020a). View
Rosario, K., et al. (2022). Freshwater macrophytes harbor viruses representing all five major phyla of the RNA viral kingdom Orthornavirae. PeerJ. 16 (10). View
Rosario, M., et al. (2020). Neuromuscular timing modification in responses to increased speed and proportional resistance while pushing a sled in young adults, European Journal of Human Movement, 44 (2020). View
Monte, A., Tecchio, P., Nardello, F., Bachero-Mena, B., Ardigò L, Zamparo, P., (2022). The interplay between gastrocnemius medialis force–length and force–velocity potentials, cumulative EMG activity and energy cost at speeds above and below the walk to run transition speed. Experimental Physiology. Nov 17, 2022. Pages: 90–102. View
Alcaraz, F., et al. (2018). Thalamocortical and corticothalamic pathways differentially contribute to goal-directed behaviors in the rat. Elife. 6(7). View
Karabulut, M., and Perez, G., (2013). Neuromuscular response to varying pressures created by tightness of restriction cuff. Journal of Electromyography and Kinesiology. Volume 23, Issue 6, December 2013, Pages 1494-1498 View
Mathis, M.W., and Mathis, A. (2020). Deep learning tools for the measurement of animal behavior in neuroscience. Curr. Opin. Neurobiol. 60, 1–11. View
Garcia, L., Brewer, W., Skevington, M., Smith, L., Waters, H., & Rosario, M. (2024). The Effects of Blood Flow Restriction on Lower Extremity EMG Amplitude While Performing a Resisted Sled Push in Healthy Subjects. J Adv Sport Phys Edu, 7(3), 35–46.
Bowman, C., & Rosario, M. G., (2021). Does Balance Fluctuates Depending on Leg Dominance? A Cross-sectional Study. Journal of Rehabilitation Practices and Research. View
Abbas Muhammad, B.S., Malik E. Dancy, M.D., Erick M. Marigi, M.D., Lafi S. Khalil, MD, Toufic R. Jildeh, M.D., Patrick J. Buckley, B.S., Javair Gillett, MS, William Burgos, Ph.D., & Kelechi R. Okoroha, M.D. (2022). An Automated Technique for the Measurement of Limb Occlusion Pressure During Blood Flow Restriction Therapy Is Equivalent to Previous Gold Standard. Arthroscopy, Sports Medicine, and Rehabilitation. Vol4 no3 (June) p1127-1132. View
Chen, S-W., Liaw, J-W., Chan, H-L., Chang, Y-J., Ku, C-H., (2014). A Real-Time Fatigue Monitoring and Analysis System for Lower Extremity Muscles with Cycling Movement. Sensors. 14(7):12410–12424. View
Uzun, S., Pourmoghaddam, A., Hieronymus, M., Thrasher, T., (2012). Evaluation of muscle fatigue of wheelchair basketball players with spinal cord injury using recurrence quantification analysis of surface EMG. European Journal of Applied Physiology. 112, 3847–3857. View
Lee, S., Neogi, T., Costello, K. E., Senderling, B., Stefanik, J. J., Frey-Law, L., Kumar, D., (2023). Association of mechanical temporal summation of pain with muscle co-contraction during walking in people with knee osteoarthritis. Clin Biomech (Bristol, Avon). 110:106105. doi: 10.1016/j.clinbiomech.2023.106105. Epub 2023 Sep 22. PMID: 37778085; PMCID: PMC10841902. View
Hora, M., Struška, M., Matějovská, Z., Kubový, P., Sládek, V., (2024). Muscle activity during crouched walking. Am J Biol Anthropol. Jan;183(1):79–91. doi: 10.1002/ajpa.24834. Epub 2023 Aug 22. PMID: 37606347. View
Lambert, B., Hedt, C., Daum, J., Taft, C., Chaliki, K., Epner, E., McCulloch, P., (2021). Blood Flow Restriction Training for the Shoulder: A Case for Proximal Benefit. Am J Sports Med. 49(10):2716–2728. doi: 10.1177/03635465211017524. Epub 2021 Jun 10. PMID: 34110960. View
Sun, D., Yang, T., (2023). Semi-Squat Exercises with Varying Levels of Arterial Occlusion Pressure during Blood Flow Restriction Training Induce a Post-Activation Performance Enhancement and Improve Vertical Height Jump in Female Football Players. J Sports Sci Med. 1;22(2):212–225. doi: 10.52082/jssm.2023.212. PMID: 37293415; PMCID: PMC10244989. View
Silfies, S., Mehta, R., Smith, S., Karduna, A., (2009). Differences in feedforward trunk muscle activity in subgroups of patients with mechanical low back pain. Arch Phys Med Rehabil. 90(7):1159–69. View
Rosário, N., Luzzatto, L., (2022). Breakthrough Hemolysis in PNH with Proximal or Terminal Complement Inhibition. N Engl J Med. 14(387):160-166. View
McCormick, J. B., Drusch, A. S., Lynch, D. J., Seeber, G. H., Wilford, K. F., Hooper, T. L., Allen, B. S., O'Connell, D. G., Mena-Iturriaga, M. J., Cooper, K. J., Sizer, P. S., (2023). The Effect of Volitional Preemptive Abdominal Contraction on Biomechanical Measures During A Front Versus Back Loaded Barbell Squat. Int J Sports Phys Ther. 1;18(4):831– 844. View
Valencia, O., Weinstein, A., Salas, R., Guzmán-Venegas, R., Arvanitidis, M., Martinez-Valdes, E., (2023). Temporal differences in the myoelectric activity of lower limb muscles during rearfoot and forefoot running: A statistical parametric mapping approach. Eur J Sport Sci. 23(6):983–991. doi: 10.1080/17461391.2022.2081094. Epub 2022 Jun 24. PMID: 35593659. View
Bolgla, L. A., Malone, T. R., Umberger, B. R., Uhl, T. L., (2011). Comparison of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome. Int J Sports Phys Ther. Dec;6(4):285-96. PMID: 22163090; PMCID: PMC3230156. View
Hart, H. F., Holt, M., Semciw, A. I., Collins, N. J., Crossley, K. M., (2020). Influence of an unloader brace on lower limb electromyographic activity in individuals with predominant lateral osteoarthritis after anterior cruciate ligament reconstruction. Braz J Phys Ther. Jul-Aug; 24(4):342–348. doi 10.1016/j.bjpt.2019.05.004. Epub 2019 Jun 1. PMID: 31175006; PMCID: PMC7352036. View
Semciw, A., Neate, R., & Pizzari, T., (2016). Running related gluteus medius function in health and injury: A systematic review with meta-analysis. J Electromyogr Kinesiol. 30:98-110. doi: 10.1016/j. jelekin.2016.06.005. Epub 2016 Jun 17. PMID: 27367574. View
Scott, B. R., Loenneke, J. P., Slattery, K. M., & Dascombe, B. J. (2014). Exercise with blood flow restriction: an updated evidence-based approach for enhanced muscular development. Sports Medicine, 44(7), 1037–1040. This study reviews the effects of BFR on oxygen availability, muscle recovery, and metabolic accumulation. View
Yasuda, T., Fukumura, K., Fukuda, T., Uchida, Y., & Sato, Y. (2010). Muscle activation during low-intensity muscle contractions with restricted blood flow. Journal of Sports Sciences, 28(5), 463-471. This study discusses changes in muscle activation patterns, including increased reliance on slow-twitch fibers due to blood flow restriction. View