
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 6 (2025), Article ID: JRPR-171
https://doi.org/10.33790/jrpr1100171Research Article
Test-Retest Reliability and Concurrent Validity of the Isometric Mid-Thigh Pull as a Measure of Total Body Muscle Performance in Recreationally Active Adults
Richard A. Ferraro PT, PhD1*, Andrew D. Lynch PT, PhD1, Arjun K. Patel PT, DPT1, and James Scott Parrott PhD2
1Rutgers The State University of New Jersey, School of Health Professions, Doctor of Physical Therapy Program, Newark, NJ, United States.
2Rutgers The State University of New Jersey, School of Health Professions, Department of Interdisciplinary Studies, Newark, NJ, United States.
Corresponding Author Details: Richard A. Ferraro PT, PhD, Assistant Professor, Department Rehabilitation and Movement Sciences, Rutgers The State University of New Jersey, School of Health Professions, Doctor of Physical Therapy Program, 65 Bergen Street Newark, NJ 07103,United States.
Received date: 11st May, 2025
Accepted date: 07th June, 2025
Published date: 09th June, 2025
Citation: Ferraro, R. A., Lynch, A. D., Patel, A. K., and Parrott, J. S., (2025). Test-Retest Reliability and Concurrent Validity of the Isometric Mid-Thigh Pull as a Measure of Total Body Muscle Performance in Recreationally Active Adults. J Rehab Pract Res, 6(1):171.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Measuring muscle performance is a common objective for many clinicians. However, many available testing measures are imprecise, resource prohibitive and designed to measure single, isolated joints [1-4]. Therefore, it is difficult to accurately assess the effectiveness of interventions designed to improve strength and power as they relate to function. At best, clinicians use surrogate measures of total body muscle performance such as grip strength, sit-to-stand movements and broad jumps. Each targets a different aspect of performance – strength, endurance, or power – and none incorporates the entire kinetic chain.
The Isometric Mid-Thigh Pull (IMTP) is a simple and safe multi-joint test of strength and power used extensively in athletes [5-7]. Previous studies testing athletes suggest that greater isometric strength is associated with greater muscular power and force production against gravity [8]. The IMTP requires coordination of the lower extremity and core (deeper abdominal and back muscles, including transverse abdominis, internal and external obliques and multifidi) muscles to transmit force to the bar. The upper extremity links the legs and trunk to the bar and contributes to force development. Sit-to-stand tests and the broad jump require lower extremity coordination and trunk control but have little upper extremity involvement. Grip strength isolates upper extremity function. The IMTP incorporates grip strength, lower extremity power and endurance, and whole-body coordination. There appears to be an overlap among these tests, with the potential for efficient assessment of total body strength with the IMTP.
Multi-joint isometric tests like the IMTP correlate well with dynamic and functional activities [9]. Multi-joint testing closely replicates the neural and mechanical conditions required in athletic performance and daily functional activities [10]. The IMTP is quicker, simpler to administer and safer to perform than other standardized multi-joint tests like one-repetition maximum (1RM) squat or dead lift which require force generation in large ranges of motion and challenge overall coordination. Maximum effort isoinertial tests such as the 1RM are not practical in novice, elderly, or functionally limited populations [11]. The IMTP can measure clinically important aspects of overall function such as rate of force development (RFD) and peak force (PF).
Despite promising results of IMTP validity and reliability in studies using athletes, conclusions need to be tempered due to small samples [6,12-14]. There has been minimal investigation regarding clinimetric properties of the IMTP in people who are not competitive athletes. The purpose of this study is to establish test-retest reliability and concurrent validity of the IMTP in recreationally active adults. We compared IMTP performance to common clinical measures (grip dynamometry, sit-to-stand performance tests and broad jump) [6,15-17]. We hypothesized that (1) PF would be stable across a 7-21- day test-retest window, (2) IMTP PF would correlate strongly with standard clinical tests, and (3) the IMTP PF would be a good estimate of combined performance of grip strength, sit-to-stand tasks, and broad jump.
Methods
A convenience sample was recruited from two college communities via flyers and email correspondence. As this was a pilot investigation of the IMTP meant to understand the variability of performance in recreationally active adults, no a priori sample size calculation was performed. Participants were screened for eligibility and excluded based on the following criteria: musculoskeletal injuries in the past 6 months or any surgery in past 3 months that may limit participant’s ability to perform a maximum effort contraction or systemic illness or condition that could affect a participant’s ability to complete the procedures safely. Participants provided written consent after an Informed Consent discussion to explain the study and answer relevant questions. The rights of participants were protected. This study received approval from the Rutgers University Institutional Review Board (#XXXXXXXXXX).
All testing sessions were completed in a laboratory setting. Participants completed the International Physical Activity Questionnaire (IPAQ) which describes physical activity in the past 7 days. To ensure adequate functioning of muscle and minimize risk of injury, prior to testing, participants completed a standardized warm-up including a 5-minute walk, followed by a series of squatting, lunging, and hip hinge movements to increase blood flow and prepare the muscles for testing. Participants were given visual and verbal instruction for each assessment. For grip strength, broad jump, and IMTP, participants completed warm-up trials at 50%, 75%, and near 100% effort to become accustomed to the testing methods. For the 30-second chair rise test (CRT30) and five times sit-to-stand (5xSTS), participants completed 5 moderate-paced repetitions to warm up and receive feedback. Participants rested 60-seconds between trials and 2-minutes between activities or as required.
A Jamar grip strength dynamometer was used (JLW Instruments, Chicago, Illinois). Participants sat with their arm positioned at the side, elbow bent to 90° and wrist in neutral. Three maximum effort trials were completed on each arm with a 60 second rest between each trial. To standardize for hand and finger length, the dynamometer rung was aligned with the proximal interphalangeal joints. Peak force was recorded for each trial in kilograms and the best trial was used for analysis.
Participants completed CRT30 and 5xSTS simultaneously. The participants were asked to rise from an 18-inch hair as many times as possible during the 30-second test period. Participants were encouraged to keep their hands across their chest to minimize use of momentum. Participants completed two trials with a 60-second rest between each trial. Repetitions completed during each trial were recorded and the maximum number of repetitions was used for analysis. A stopwatch recorded the time to complete the first 5 repetitions of the CRT30. The trial with the fastest 5 repetitions was used for analysis.
Participants completed three maximum effort broad jumps with a 60-second rest between each trial. Participants stood with their toes at the 0-centimeter mark and jumped forward as far as possible with a controlled landing (i.e., no falling forward or excessive foot movement). Performance was measured from the contact point closest to the 0-centimeter mark (e.g., the heel). The longest recorded jump was used for analysis.
Participants completed three IMTP trials with a 60-second rest break in bwtween each trial. Data were captured at 100 Hz via LoadVUE (LV-1000HS-10K) software connected to an S-Beam Load cell (Loadstar Sensors, Fremont, CA). A similar system using a single axis load cell to measure PF during IMTP was shown to have acceptable reliability and validity when compared to force plates [18].
Participants stood with the load cell between their feet at the level of the metatarsal heads and at a width that aligned with their hips. The hips and knees were flexed between 20°-40° and 30°-50°, respectively [19,20]. Angles were confirmed with a goniometer. The IMTP was set to ensure a T-bar handle was mid-way between the knee and hip joints with the sternum positioned directly over the T-bar. Previous studies have used various methods for the participant to grasp the bar including unassisted grip, wrist straps, and taping the hands to the bar. We chose an unassisted pronated grip without wraps or straps to not minimize the effect of grip strength (See FIGURE 1). Hand width was measured with the lateral border of each hand one inch from the end of the bar.
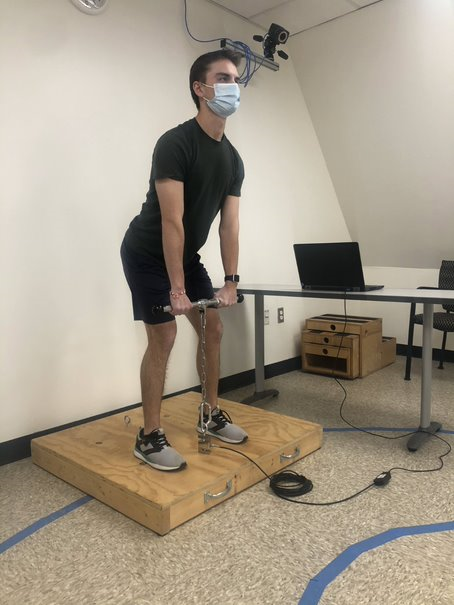
Figure 1: IMTP setup.
Following a standardized countdown, participants pulled as hard as possible while extending their legs into the platform and maintaining a straight spine for 5 seconds [21]. Participants were monitored for proper mechanics or excessive use of the lumbar spine and the trial was stopped if this was observed. The trial with the greatest PF was used for analysis.
A subset of participants returned for follow up IMTP testing 7-21 days after first collection to establish test-retest reliability. The methods did not change from the initial to follow-up dates including an identical T-bar height. Activity was not controlled between sessions, but participants were encouraged to come to both sessions well rested.
Data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Rutgers University [22,23]. Statistical analyses were performed with Stata 17.0 (StataCorp LLC, College Station, TX). IMTP data are reported multiple ways in the literature, from raw values in Newtons to normalized values in Newtons per kilogram of body weight (N/kg) [5]. To facilitate comparisons among participants and between tests, force and power data were normalized to anthropometric data. IMTP and grip strength were normalized and expressed as a ratio of force produced in N/kg of body weight to control for differences in participant size (IMTPN and GRIPN, respectively). Broad jump performance was normalized by dividing the distance jumped (cm) by body height (cm) (BROADN). Neither CRT30 nor 5xSTS was normalized as each participant was moving their own body weight. Physical performance tests were summarized with means and standard deviations.
To establish test-retest reliability, IMTPN from the first session was compared to IMTPN from the second session using a two-way random effects intraclass correlation coefficient model (ICC2,1). In addition, a minimal detectable change score (MDC95) was calculated from the standard error and ICC at a 95% confidence interval (CI) for IMTPN.
To establish the concurrent validity of the IMTP as a measure of total body strength, IMTPN was compared to GRIPN, BROADN, CRT30, and 5xSTS using simple correlations with 95% CI. Correlations greater than ± 0.8 are considered very strong, between ± 0.6 and ± 0.8 moderately strong, ± 0.3 to ± 0.6 fair, and between 0 and ± 0.3 are considered poor [24]. Because we expected differences between sexes, we also investigated sex-specific correlations for each measure.
Because GRIPN, BROADN, 5xSTS, and CRT30 each reflect one portion of the IMTP, we hypothesized that each would contribute to synergistic performance on the IMTP. Therefore, we attempted to predict IMTPN via multiple linear regression with age, GRIPN, BROADN, 5xSTS, and CRT30 as continuous covariates with gender as a categorical covariate. We evaluated the regression models thoroughly to determine the most parsimonious model and to determine the effects of influential cases [25-27].
Results
One hundred nineteen participants completed the full testing session with 34 returning for a second day to establish test-retest reliability. Participant demographics are described in TABLE 1 for each cohort. Non-normalized IMTP values in Newtons are presented for comparison to the existing literature. The IPAQ was added to the protocol after the first 10 participants. An additional 6 participants did not provide sufficient data to calculate metabolic equivalents. Therefore, only 105 participants sufficiently completed the IPAQ. Eighty-five percent of participants were classified as having a medium or high activity level.
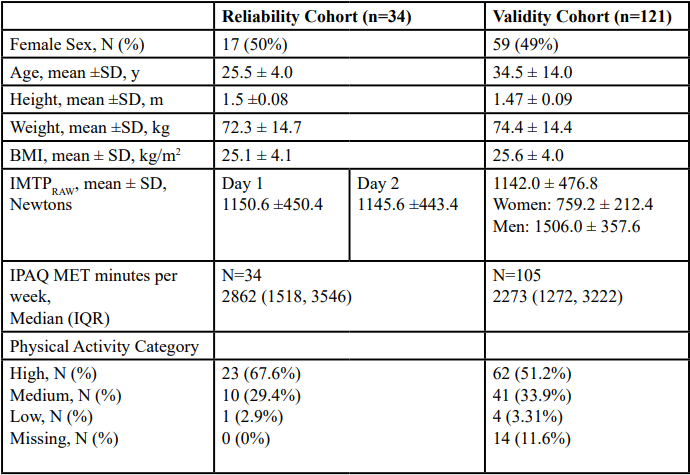
Table 1. Participant demographics and sample characteristics
IMTP results from sessions 1 and 2 are presented in TABLE 2. Session 2 was completed 11.8 ± 4.6 days (range 7-32 days) after Session 1. One participant who consented to complete Session 2 was unable as she experienced a shoulder strain 2 weeks after Session 1. One participant completed follow-up testing outside of the 21-day window. Day-to-day reliability was excellent overall (ICC2,1 > 0.98, 95% CI: 0.93 to 0.99) and for men and women individually.
Physical performance test results are summarized in TABLE 3. On average, participants produced 15.1 ± 5.2N/kg. Male participants produced more IMTPN force than female participants (t=-11, p<.001). GRIPN (r=0.80, 95% CI: 0.73, 0.87) and BROADN (r=0.76, 95% CI: 0.69, 0.83) had a moderately strong correlation with IMTPN. Sit-to-stand tests were fairly correlated with IMTPN (5xSTS r=-0.53, 95% CI: -0.64, -0.42; CRT30 r=0.52, 95% CI: 0.38, 0.65). Sex-specific correlations were poorer than overall correlations (maximum r=0.71, See FIGURES 2-5).
Regression results are presented in TABLE 4. The final model including age, sex, GRIPN, BROADN, and 5xSTS explained 73.3% of the variance in the IMTPN (F (5,110) = 64.01, p<0.001). Only one case was identified as potentially influential. Ultimately, we chose to report the model results with all cases included. 2 subjects were unable to complete the broad jump testing portion of the study and were removed from the BROADN regression analysis.
To determine if a specific predictor was driving the model, we examined squared semipartial correlations in the refined model and found that no individual predictor uniquely explained >7% of the total variance explained. This confirms that it is the shared (partial) variance among predictors that explains the majority of variance in IMTPN rather than any single measure. This confirms the clinical suspicion that IMTPN reflects the coordination of all joints in a strength measure.
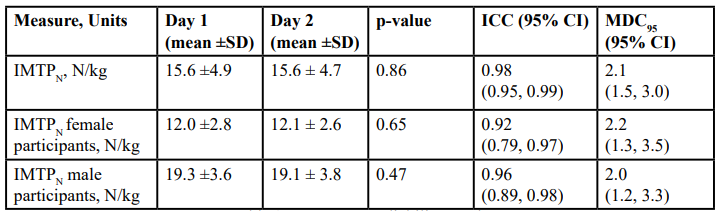
Table 2: Test-Retest reliability results
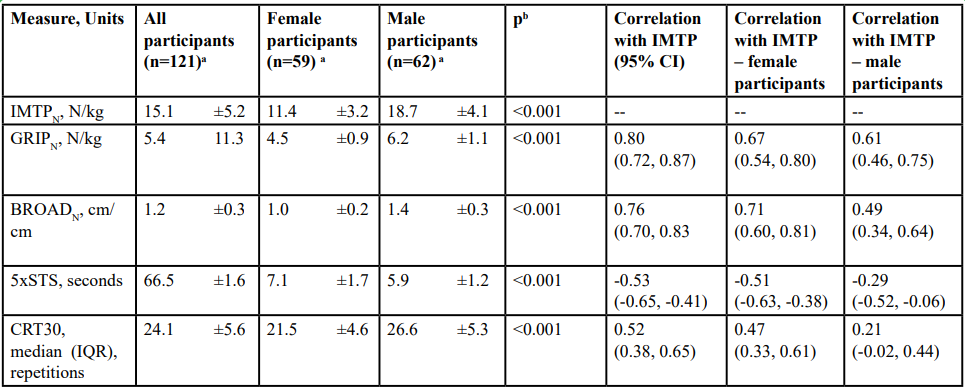
Table 3: Physical performance test results
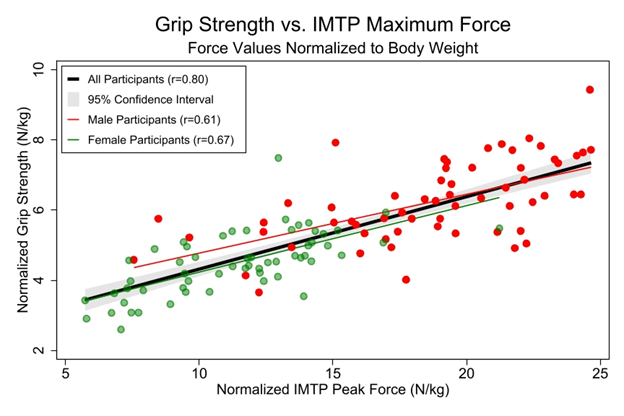
Figure 2. Grip strength vs. IMTP maximum force. This figure illustrates the strong correlation between grip strength and the IMTP for the whole sample, while the correlations within sex are weaker. Within sexes, there are fewer overall participants, so extreme values affect the correlation to a greater degree. This is best seen by the highly variable grip strength among males with IMTPN less than 15N/kg.
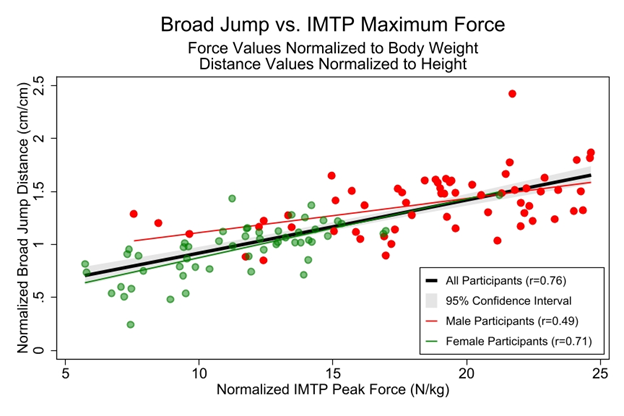
Figure 3. Broad Jump vs. IMTP Maximum Force
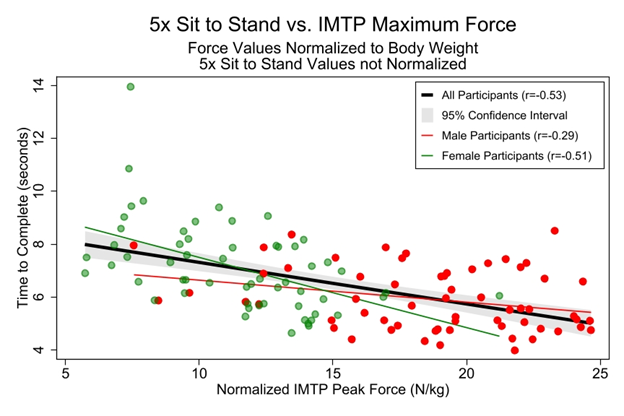
Figure 4. Time to Complete Five Times Sit-to-Stand vs Maximum IMTP Force
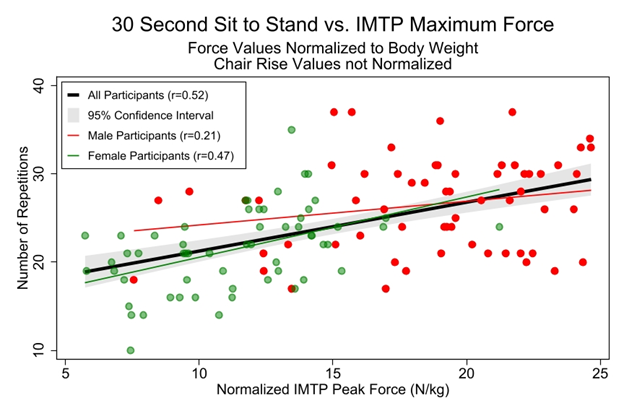
Figure 5. Repetitions Completed in 30-Second Sit-to-Stand vs. IMTP Maximum Force.
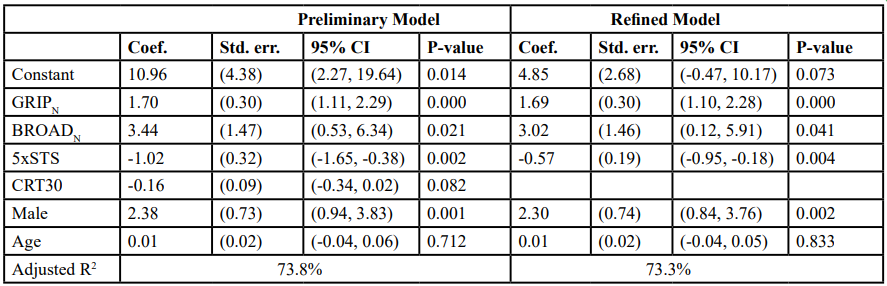
Table 4. Results of preliminary and refined linear regression models of IMTPN
Discussion
The purpose of this study was to establish test-retest reliability and concurrent validity for the IMTP in healthy, active individuals. The IMTP demonstrated excellent test-retest reliability for men and women and showed fair to strong correlations with common clinical tests of strength and power. Most importantly, the IMTP measures global physical performance as it accurately reflects a combination of standard tests, indicating it is likely a useful clinical measure of muscle performance. Specifically, it may be helpful to determine the effectiveness of strength and neuromotor interventions. To our knowledge, the present study is one of a few studies to investigate the IMTP as a measure of total body strength in recreationally active individuals [8,28,29].
Understanding test-retest variability and reliability is crucial for interpretation of clinical tests. We chose a retest period between 7 and 21 days as it is long enough to recover from a maximal effort test and unlikely long enough to make true strength gains from any outside training regimens. In addition to using ICC to assess agreement, we also calculated MDC95 scores. Despite the sex differences in IMTPN performance, there was not a substantial difference in sex-specific MDC95 values. To simplify interpretation, we recommend using the average MDC95 value of 2.1 N/kg. The average performance was about 17 N/kg, so a change of 2.1 N/kg equates to approximately 12.4%. To put this into familiar terms, this equates to a change of 0.22 pounds of force per pound of body weight or 0.21 kilograms of force per kilogram of body weight. The average participant in this study weighed 74.4 kilograms (163.7 pounds) and would need to improve IMTP performance by 15.6 kilograms (34.4 pounds). With these data, clinicians can trust the values produced from the IMTP and interpret follow-up data after intervention.
Clinicians often want to understand how a new measure compares to familiar measures before adopting it. The IMTP demonstrated fair to moderately strong correlations with common performance tests. The strongest correlations were between ITMPN and BROADN(r = 0.76) and GRIPN (r = 0.80). The broad jump and IMTP require similar coordinated force development patterns, including major contributions from lower extremity extensors. This is clinically meaningful because the broad jump may not be feasible in many patients due to neuromotor and balance demands. The correlation is consistent with the relationship between IMTP and vertical jump performance (r = 0.72) in athletes and supports isometric strength as a strong indicator of dynamic performance [20].
Grip strength is an acceptable indicator of overall strength in both healthy and compromised populations [30-32] and correlates similarly (r=0.73) with IMTP performance in athletes [20]. Previous studies have shown that isometric strength is a significant factor in determining dynamic strength outcomes explaining up to 71.9% and 55.7% of the variance in males and females respectively [11-13].
There was a poorer correlation between 5xSTS (r = -0.53) and CRT30 (r = 0.52), which is poorer than in previous studies using CRT30 (r = 0.67) [15,16]. It is unclear whether sit-to-stand tests reflect muscle strength or physical performance (functional capability) [33]. The biomechanical and neuromotor demands of sit-to-stand tests are similar to the IMTP. However, in sit-to-stand tests the cumulative effect of momentum and fatigue with sequential repetitions adds variability to the test and may explain the more modest correlations to the IMTP. Lastly, the IMTP is conducive for full intention and neural processing for a maximum effort which is different from the repetition goals of the chair tests.
Interestingly, sex-specific correlations were weaker for all the comparison tests. Within sex, there is less variability in all the measures (see smaller sex-specific standard deviations in TABLE 3) and influential cases affect the correlation more. When sexes were combined, the outlying cases for men and women did not have as much influence and the relationships became more linear. In each Figure 2-5, the performance of the weaker men and stronger women tended to overlap considerably, vastly improving the strength of the correlation. This is unlikely to be a biological aspect and more likely that the proportion of weaker men and stronger women were fairly low, so each case exerted a greater influence on the overall correlation. It is likely that the sex-specific correlations would improve if the sample size were to increase.
Despite the poor correlations within sex, the linear regression model that included sex as a predictor of IMTP was still very strong. We assessed the relationship between the IMTP and comparator tests with a linear regression as the IMTP incorporates aspects of all the comparators. To perform well on the IMTP, an individual needs well-developed leg strength and power, as well as a strong grip. Therefore, we hypothesized that individuals who performed well on many of the comparator tests would perform well on the IMTP. In general, this relationship held up. A combination of the predictors and sex explained 73% of the variance in IMTP performance, which was vastly superior to any single measure, supporting the multifaceted nature of the IMTP.
We investigated potentially influential cases to determine how individual variations impact the performance of the model. This is important if the IMTP is to be used successfully in clinical populations where one aspect of function may be more impacted than others. Only one case was deemed influential based on residual values. We reviewed the case, and data were determined to be physiologically plausible (i.e., no data recording errors). This case was the oldest person in the sample at 84 years old. As the sample data were more sparse with older individuals, it will be relevant to increase the sample size in those over 70 to have a more realistic estimate of normal performance.
There were limitations in this study. We chose a sample convenient to college campuses, which provided an active and younger population. Sixty-five (~55%) of the participants were aged 30 or younger. This may limit the study’s generalizability to clinical populations that tend to be older and less active but does provide a base of knowledge for comparison. The rate of force development (RFD), the speed at which peak force is realized, was not included in this study. Participants were instructed to produce as much force as possible, but not to do so quickly, and therefore, RFD could not be calculated. This might have provided valuable information for comparison in future studies in compromised clinical populations.
Conclusion
Based on this study's results, clinicians should feel confident in using the IMTP as an efficient measure of total body strength. The IMTP is reliable and has the potential to be implemented when dynamic tests like 1RM and jump tests are contraindicated. The IMTP is inexpensive, easy to administer, and portable. Physical space requirements are minimal, so even in smaller clinics the IMTP is feasible. The gold standard for collecting kinetic data such as this is using force plates which are much more expensive and often not an option for many clinics. The platform as constructed is lightweight and portable to make it simple to collect data in many locations. The only other requirements for the IMTP are a laptop computer and a strain gauge which can be purchased at a reasonable cost and requires minimal training to set up.
Future studies should investigate impaired populations with a focus on RFD as an additional quantitative aspect of function. The IMTP may also be used to quantify the effectiveness of interventions that target strength, endurance, and power, or as a predictor of disease progression or vitality in clinical populations. We have initiated such studies in persons living with HIV and those with cardiometabolic disease.
Study Details
Approval and Registration: This study was approved by the Rutgers University Institutional Review Board (#Pro2020000488). This study does not meet the NIH definition of a clinical trial and was therefore not registered at clinicaltrials.gov.
Public Involvement: No patients, athletes, or public partners were involved in the planning, design, or reporting of this study.
Author contributions: RAF and ADL conceived the purpose of the study. RAF, ADL, and JSP designed the study and participated in analysis. RAF, ADL, and AP participated in data acquisition. All authors contributed to the drafting and revision of the manuscript. All authors approved the final manuscript and agree to be accountable for all aspects of the work.
Data sharing: Data are available upon reasonable request to the corresponding author.
Acknowledgements:
The authors would like to acknowledge Vanessa Baggio, SPT, Christina Diamantis, DPT, Stephen Gibson, DPT, Mohamed Ibrahim, DPT, Eric Lippincott, DPT, Warren Yang, DPT for their contributions to data collection.
References
Toonstra, J., & Mattacola, C. G. (2013). Test-retest reliability and validity of isometric knee-flexion and -extension measurement using 3 methods of assessing muscle strength. J Sport Rehabil, 22(1). View
Knepler, C., & Bohannon, R. W. (1998). Subjectivity of forces associated with manual-muscle test grades of 3+, 4-, and 4. Percept Mot Skills, 87(3 Pt 2): 1123-1128. View
Invergo, J. J., Ball, T. E., & Looney, M. (1991). Relationship of push-ups and absolute muscular endurance to bench press strength. The Journal of Strength & Conditioning Research, 5(3): 121-125. View
Silva, M. G., Moreira, P. V. S., & Rocha, H. M. (2017). Development of a low cost force platform for biomechanical parameters analysis. Research on Biomedical Engineering, 33: 259-268. View
Dos'Santos, T., Thomas, C., Comfort, P., McMahon, J. J., & Jones, P. A. (2017). Relationships between Isometric Force Time Characteristics and Dynamic Performance. Sports (Basel), 5(3).View
Wang, R., Hoffman, J. R., Tanigawa, S., Miramonti, A. A., La Monica, M. B., Beyer, K. S., Church, D. D., Fukuda, D. H., & Stout, J. R. (2016). Isometric Mid-Thigh Pull Correlates With Strength, Sprint, and Agility Performance in Collegiate Rugby Union Players. J Strength Cond Res, 30(11): 3051-3056. View
Giles, G., Lutton, G., & Martin, J. (2022). Scoping Review of the Isometric Mid-Thigh Pull Performance Relationship to Dynamic Sport Performance Assessments. J Funct Morphol Kinesiol, 7(4). View
Suchomel, T. J., Nimphius, S., & Stone, M. H. (2016). The Importance of Muscular Strength in Athletic Performance. Sports Med, 46(10): 1419-1449. View
McGuigan, M. R., & Winchester, J. B. (2008). The relationship between isometric and dynamic strength in college football players. J Sports Sci Med, 7(1): 101-105. View
Tillin, N. A., Pain, M. T., & Folland, J. (2013). Explosive force production during isometric squats correlates with athletic performance in rugby union players. J Sports Sci, 31(1): 66-76. View
Jidovtseff, B., Croisier, J., Scimar, N., Demoulin, C., Maquet, D., & Crielaard, J. (2008). The ability of isoinertial assessment to monitor specific training effects. J Sports Med Phys Fitness, 48(1): 55-64. View
Spiteri, T., Nimphius, S., Hart, N. H., Specos, C., Sheppard, J. M., & Newton, R. U. (2014). Contribution of strength characteristics to change of direction and agility performance in female basketball athletes. J Strength Cond Res, 28(9): 2415- 2423. View
Thomas, C., Comfort, P., Chiang, C.-Y., & Jones, P. A. (2015). Relationship between isometric mid-thigh pull variables and sprint and change of direction performance in collegiate athletes. Journal of trainology, 4(1): 6-10. View
Grgic, J., Scapec, B., Mikulic, P., & Pedisic, Z. (2022). Test-retest reliability of isometric mid-thigh pull maximum strength assessment: a systematic review. Biol Sport, 39(2): 407-414. View
Alcazar, J., Kamper, R. S., Aagaard, P., Haddock, B., Prescott, E., Ara, I., & Suetta, C. (2020). Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: validation and translation to functional performance. Sci Rep, 10(1), 16337. View
McAllister, L. S., & Palombaro, K. M. (2020). Modified 30-Second Sit-to-Stand Test: Reliability and Validity in Older Adults Unable to Complete Traditional Sit-to-Stand Testing. J Geriatr Phys Ther, 43(3): 153-158. View
Tiwari, D., Talley, S. A., Alsalaheen, B., & Goldberg, A. (2019). Strength of association between the Five-Times-Sit-to-Stand Test and balance, knee extensor strength and lower limb power in community-dwelling older adults. International Journal of Therapy And Rehabilitation, 26(3): 1-10. View
James, L. P., Roberts, L. A., Haff, G. G., Kelly, V. G., & Beckman, E. M. (2017). Validity and Reliability of a Portable Isometric Mid-Thigh Clean Pull. J Strength Cond Res, 31(5): 1378-1386. View
Haff, G. G., Ruben, R. P., Lider, J., Twine, C., & Cormie, P. (2015). A comparison of methods for determining the rate of force development during isometric midthigh clean pulls. J Strength Cond Res, 29(2), 386-395. View
McGuigan, M. R., Newton, M. J., Winchester, J. B., & Nelson, A. G. (2010). Relationship between isometric and dynamic strength in recreationally trained men. J Strength Cond Res, 24(9): 2570- 2573. View
Brady, C. J., Harrison, A. J., & Comyns, T. M. (2020). A review of the reliability of biomechanical variables produced during the isometric mid-thigh pull and isometric squat and the reporting of normative data. Sports Biomech, 19(1): 1-25. View
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'Neal, L., McLeod, L., Delacqua, G., Delacqua, F., Kirby, J., Duda, S. N., & Consortium, R. E. (2019). The REDCap consortium: Building an international community of software platform partners. J Biomed Inform, 95, 103208. View
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)- -a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform, 42(2): 377-381. View
Chan, Y. H. (2003). Biostatistics 104: correlational analysis. Singapore Med J, 44(12): 614-619. View
Byham-Gray, L., Parrott, J. S., Ho, W. Y., Sundell, M. B., & Ikizler, T. A. (2014). Development of a predictive energy equation for maintenance hemodialysis patients: a pilot study. J Ren Nutr, 24(1): 32-41. View
Frey, B. B. (2021). The SAGE Encyclopedia of Research Design. SAGE Publications. View
Vittinghoff, E., Glidden, D. V., Shiboski, S. C., & McCulloch, C. E. (2006). Regression methods in biostatistics: linear, logistic, survival, and repeated measures models. View
Crewther, B. T., Carruthers, J., Kilduff, L. P., Sanctuary, C. E., & Cook, C. J. (2016). Temporal associations between individual changes in hormones, training motivation and physical performance in elite and non-elite trained men. Biol Sport, 33(3): 215-221. View
Orange, S. T., Marshall, P., Madden, L. A., & Vince, R. V. (2019). Can sit-to-stand muscle power explain the ability to perform functional tasks in adults with severe obesity? J Sports Sci, 37(11): 1227-1234. View
Bautista-Aguirre, F., Oliva-Pascual-Vaca, A., Heredia-Rizo, A. M., Bosca-Gandia, J. J., Ricard, F., & Rodriguez-Blanco, C. (2017). Effect of cervical vs. thoracic spinal manipulation on peripheral neural features and grip strength in subjects with chronic mechanical neck pain: a randomized controlled trial. Eur J Phys Rehabil Med, 53(3): 333-341. View
Bialas, A., Synder, M., Dyhdalewicz, A., & Walenczak, K. (2016). Analysis of Upper Limb Movement Range and Global Grip Strength After Surgical Treatment of AO Type C Distal Radius Fractures Using LCP Plates and K-wires. Ortop Traumatol Rehabil, 18(3): 223-229. View
Bohannon, R. W. (2008). Is it legitimate to characterize muscle strength using a limited number of measures? J Strength Cond Res, 22(1): 166-173. View
Yee, X. S., Ng, Y. S., Allen, J. C., Latib, A., Tay, E. L., Abu Bakar, H. M., Ho, C. Y. J., Koh, W. C. C., Kwek, H. H. T., & Tay, L. (2021). Performance on sit-to-stand tests in relation to measures of functional fitness and sarcopenia diagnosis in community-dwelling older adults. Eur Rev Aging Phys Act, 18(1): 1.View