
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 6 (2025), Article ID: JRPR-176
https://doi.org/10.33790/jrpr1100176Research Article
Reference Patterns for Sinusoidal Harmonic Acceleration Responses in Healthy Young Adults: Clinical Implications for Vestibular Assessment
Cara Makuta Tolan
Assistant Professor, Department of Rehabilitation Sciences, Commonwealth University of Pennsylvania - Bloomsburg, Bloomsburg, Pennsylvania, 236 Centennial Hall, 400 East Second St. Bloomsburg, PA 17815-1301,United States.
Corresponding Author Details: Cara Makuta Tolan, Assistant Professor, Department of Rehabilitation Sciences, Commonwealth University of Pennsylvania - Bloomsburg, Bloomsburg, Pennsylvania, 236 Centennial Hall, 400 East Second St. Bloomsburg, PA 17815-1301, United States.
Received date: 15th May, 2025
Accepted date: 23th June, 2025
Published date: 25th June, 2025
Citation: Tolan, C. M., (2025). Reference Patterns for Sinusoidal Harmonic Acceleration Responses in Healthy Young Adults: Clinical Implications for Vestibular Assessment. J Rehab Pract Res, 6(1):176.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Sinusoidal Harmonic Acceleration (SHA), a subtest within rotational chair assessments, evaluates vestibulo-ocular reflex (VOR) function across a range of physiologic frequencies. This study explored VOR performance using SHA testing conducted with the NeuroKinetics (NOTC) rotational chair, focusing on normative findings in a healthy young adult population.
Thirty-four participants aged 18 to 28 with normal vestibular function were assessed at seven frequencies (0.01, 0.02, 0.04, 0.08, 0.16, 0.32, and 0.64 Hz) using a peak chair velocity of 60°/sec. VOR metrics—gain, phase, and asymmetry—were analyzed using twoway repeated measures ANOVA to evaluate the effects of frequency and sex. Results revealed no statistically significant differences in gain, phase, or asymmetry across frequencies or between sexes. These findings suggest that VOR function remains stable within this age range regardless of stimulus parameters or participant sex, establishing a consistent normative baseline.
For rehabilitation professionals, including audiologists and physical therapists, these normative values provide essential benchmarks for identifying deviations that suggest vestibular dysfunction. They support accurate diagnosis, targeted treatment, and effective rehabilitation monitoring. Device-specific datasets enhance the diagnostic precision and clinical utility of vestibular assessments.
Key words (3-5): Vestibular Rehabilitation, Sinusoidal Harmonic Acceleration (SHA), Vestibulo-Ocular Reflex (VOR), Rotational chair Testing, Normative Data
Introduction
Dizziness and balance disorders are among the most frequently reported complaints in clinical settings, with approximately 69 million Americans experiencing some form of dizziness each year [1]. A healthy vestibular system is critical in maintaining balance, stabilizing gaze, and supporting spatial orientation. Symptoms such as dizziness, imbalance, or vertigo often indicate dysfunction within this system. Accurate diagnosis of vestibular pathology is essential for guiding effective treatment planning and reducing fall risks, one of the leading causes of injury and mortality in older adults [2].
Vestibular function is supported by a complex interplay of peripheral and central structures. The peripheral vestibular apparatus, situated in the inner ear, comprises the semicircular canals and otolith organs, which detect rotational and linear acceleration of the head, respectively [3]. The peripheral structures communicate with central vestibular pathways to produce coordinated reflexes, such as the vestibulo-ocular reflex (VOR) and the vestibulospinal reflex (VSR). The VOR, in particular, plays a key role in gaze stabilization by producing eye movements opposite to head motion, allowing visual fixation to be maintained during movement [3].
To evaluate vestibular system integrity, clinicians employ a battery of diagnostic vestibular tests. Among these, rotational chair testing is widely accepted as a physiologically accurate and reliable assessment that simulates natural head movements across various frequencies. A commonly used subtest within this modality is the Sinusoidal Harmonic Acceleration (SHA) test, which quantifies VOR performance by measuring gain (the ratio of the eye-to-head velocity), phase (the timing relationship between eye and head movements), and asymmetry (the difference in responses to leftward versus rightward rotations).
Research suggests that factors such as sex, age, and stimulus frequency may influence SHA outcomes [4]. Clinicians must depend on well-controlled normative studies to interpret individual results accurately. The rotational chair is a clinically accepted vestibular test measure. However, limited research exists regarding normative SHA values obtained using this specific equipment [1]. This lack of normative data hinders clinicians’ ability to interpret test results confidently and reliably distinguish normal from pathological vestibular function [5].
This study aimed to evaluate SHA performance in a sample of healthy young adults using the NeuroKinetics rotational chair. Specifically, the objectives were to (1) establish normative data for SHA parameters: gain, phase, and asymmetry across seven test frequencies ranging from 0.01 Hz to 0.64 Hz, and (2) assess whether these measures varied by sex or stimulus frequency. Addressing these goals will contribute valuable normative data and improve the clinical utility of rotational chair testing for both diagnostic and rehabilitative applications.
Materials and Methods
The purpose of this study was to establish normative data for healthy young adults, aged 18–28, using standardized protocols for the Sinusoidal Harmonic Acceleration (SHA) subtest of the NeuroKinetics I-Portal NOTC rotational chair. A quantitative research design was employed to examine the relationships between the independent variables, sex and stimulus frequencies (0.01, 0.02, 0.04, 0.08, 0.16, 0.32, and 0.64 Hz), and the dependent variables, SHA measures of gain, phase, and asymmetry. A repeated measure analysis of variance (ANOVA) was selected to evaluate differences both within and between subjects, accounting for variability across conditions and reducing error variance [6].
Participants included 34 healthy individuals (4 males and 30 females). All participants completed the Dizziness Handicap Inventory (DHI), a validated tool assessing the self-perceived impact of dizziness. Scores below 15 were required for inclusion, indicating minimal or no perceived vestibular impairment [7]. Exclusion criteria included any history of vestibular or otologic disorders, hearing loss, visual impairments (other than corrected vision), neurological conditions, or abnormal vestibular or audiologic test results. Screening included assessments of spontaneous and gaze-evoked nystagmus, saccades, and smooth pursuit, all of which were within normal age-appropriate limits.
Participants were instructed to refrain from caffeine and vestibular suppressant medications for 24 hours prior to testing. To avoid interference with video-oculography, participants were also asked not to wear facial or eye makeup. Testing was conducted using the NeuroKinetics I-Portal NOTC rotary chair system, which delivers earth-vertical axis rotation and is capable of measuring VOR responses from 0.001 to 1.28 Hz at velocities up to 300°/s. The system operates using VEST 7.5 software in a light-tight room. Eye movements were recorded with video-nystagmography (VNG) goggles and processed via I-Portal 3.2 software. Participants were seated securely in the chair with proper head coupling to ensure horizontal canal alignment within the plane of rotation. Each participant was engaged in alerting tasks to maintain attention. Calibration was performed prior to each trial, and eye movements were recorded using 4D binocular video-oculography. The SHA subtest was administered at seven frequencies (0.01–0.64 Hz) with a constant peak velocity of 60°/s. Testing lasted approximately 20 minutes.
Analyses were conducted using JASP software [8]. Repeated measures ANOVA was used to evaluate the effects of sex and frequency on gain, phase, and asymmetry, accounting for withinsubject and between-group variance. Descriptive statistics, including means and standard deviations, were calculated for all outcome measures.
Results
Due to the interval data and the study's within- and between-subjects design, two repeated measures ANOVAs were conducted to compare the effects of stimulus frequency and participant sex on gain, phase, and asymmetry. Mauchly's sphericity test indicated a sphericity violation (p < .05) for all three ANOVAs. It is worth noting that Mauchly's test can overestimate the effects in small sample sizes, potentially inflating Type I error rates (Laerd Statistics, n.d.). Interpretation of effect sizes followed Cohen's (1988) guidelines: small effect (ηp² = .01), medium effect (ηp² = .06), and large effect (ηp² = .14).
Results revealed a significant main effect of frequency on gain (F(6, 192) = 8.659, p < .001). Post-hoc analysis (Table 5) showed significant differences in gain between 0.01 Hz and 0.04, 0.08, 0.16, and 0.64 Hz, as well as between 0.02 Hz and 0.04, 0.16, and 0.64 Hz. No significant main effects of sex or sex × frequency interactions were found. Table 1 presents the average vestibulo-ocular reflex (VOR) gain, standard deviations, and minimum and maximum values across all tested frequencies.
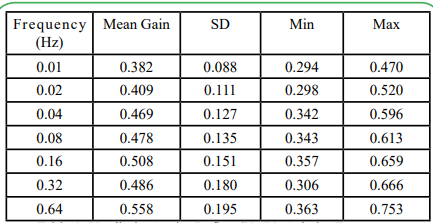
Table 1: Vestibulo-Ocular Reflex (VOR) Gain by Frequency
A repeated measures ANOVA also showed a significant effect of frequency on phase (F(6, 192) = 66.811, p < .001). Post-hoc analysis (Table 6) indicated significant differences in phase between 0.01 and 0.02 Hz, 0.01 and 0.04 Hz, 0.02 and 0.04 Hz, 0.04 and 0.08 Hz, and 0.08 and 0.16 Hz. No significant main effect of sex or interaction between sex and frequency was found. Table 2 presents each tested frequency's average VOR phase, standard deviations, and minimum and maximum values.
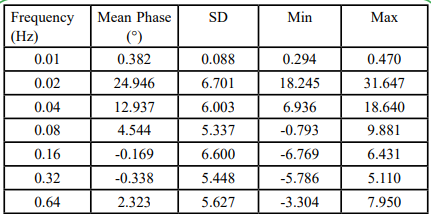
Table 2: Vestibulo-Ocular Reflex (VOR) Phase by Frequency
Finally, a repeated measures ANOVA revealed a significant main effect of frequency on asymmetry (F(6, 192) = 4.735, p < .001). Posthoc analysis (Table 7) indicated substantial differences in asymmetry between 0.01 and 0.02 Hz and between 0.02 and 0.64 Hz. Again, no significant main effect of sex or interaction between sex and frequency was observed. Table 3 presents all frequencies' average VOR asymmetry values, standard deviations, and minimum and maximum values.
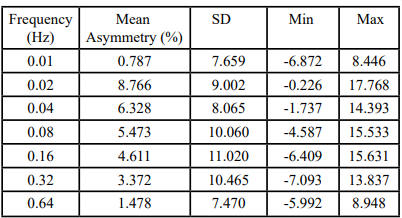
Table 3: Vestibulo-Ocular Reflex (V/OR) Asymmetry by Frequency
The data collected in this study provided the Commonwealth University-Bloomsburg clinicians with normative values for gain, phase, and asymmetry derived from sinusoidal harmonic acceleration (SHA) testing in young adults. Reference ranges were calculated using each parameter's mean and standard deviation to define minimum and maximum values and represented as descriptive statistics (Table 4). Post hoc analyses (Tables 5, 6, & 7) revealed significant main effects of stimulus frequency on all three vestibulo-ocular reflex (VOR) measures of gain, phase, and asymmetry, with the most pronounced differences occurring at lowerfrequency stimuli (≤0.16 Hz). These findings suggest that stimulus frequency significantly influences VOR performance, with less variability observed at lower frequencies. No significant effects or interactions were found for sex, indicating that VOR function does not differ meaningfully between male and female participants.
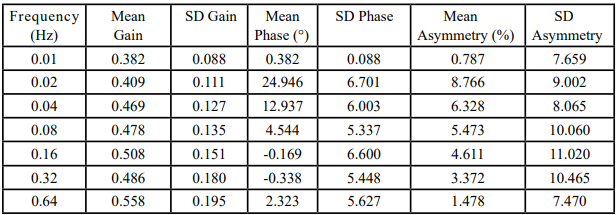
Table 4: Summary Descriptive Statistics
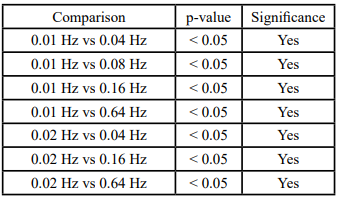
Table 5: Post Hoc Comparisons of Gain Between Frequencies
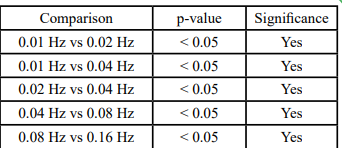
Table 6: Post Hoc Comparisons of Phase Between Frequencies
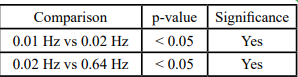
Table 7: Post Hoc Comparisons of Asymmetry Between Frequencies
The highest average VOR phase (24.946 ± 6.701 degrees) was observed at 0.02 Hz, aligning with the findings of Li et al. [9], who reported a similar increase in phase lag at this frequency compared to higher frequencies. Asymmetry data, while included, were interpreted cautiously due to their inherent variability and the limited normative data in young adults [1].
Discussion
When a patient's dizziness is suspected to originate from a vestibular source, rotational chair (RC) testing offers unique diagnostic advantages. RC testing evaluates bilateral vestibular function, approximates natural physiologic conditions, and enables monitoring of central compensation, an important consideration in therapeutic planning [1]. While device manufacturers supply most normative data for RC testing, the methodologies used to collect these data are often proprietary. Few peer-reviewed studies offer transparent, age-stratified normative data that can be confidently applied across diverse patient populations. This study contributes to the literature by providing such data for young adults, enhancing clinical interpretability in this demographic.
A key advantage of SHA testing is its precise, computer-controlled delivery of acceleration, velocity, oscillation duration, and amplitude, which supports accurate, reproducible VOR measurements [9]. Despite its clinical utility, the current literature on SHA is still evolving. This study addresses a critical gap by establishing normative reference values for a narrowly defined yet clinically relevant age group.
This study investigated the effects of stimulus frequency and sex on SHA-derived VOR gain, phase, and asymmetry measures. Frequencyand sex-specific averages are presented with the data. No significant differences were found between male and female participants across the VOR measures. However, stimulus frequency significantly affected outcomes. Specifically, responses became less variable at lower frequencies (≤0.16 Hz), underscoring the diagnostic value of including low-frequency stimuli in SHA protocols. These findings are consistent with prior research by Li et al. [9], who reported increased phase lag at frequencies <0.04 Hz, which normalized at higher frequencies (0.08–0.64 Hz). This suggests that higher-frequency SHA testing alone may fail to detect abnormalities identifiable at lower frequencies.
The normative data established in this study provide clinically useful reference values for SHA testing using the NOTC rotary chair in young adults. However, interpretation of these findings should consider the study's limitations, particularly the narrow age range (18–28 years) and the unbalanced sex distribution (30 females, four males). While existing evidence suggests sex does not significantly impact vestibular function, future studies with more balanced cohorts are warranted.
The findings of this study hold important implications for vestibular rehabilitation professionals, including audiologists, physical therapists, and occupational therapists involved in evaluating and managing dizziness and balance disorders. Access to normative VOR gain, phase, and asymmetry values enables clinicians to more accurately identify vestibular dysfunction's presence, severity, and laterality. Notably, the reduced variability observed at lower frequencies reinforces the importance of including these frequencies in SHA protocols—especially when assessing patients with mild, compensated, or bilateral vestibular deficits.
These findings can directly inform the design and progression of vestibular rehabilitation interventions. Frequency-specific VOR deficits identified through SHA testing may guide the selection of targeted gaze stabilization exercises and adaptive protocols that address the impaired frequency range. Furthermore, accessing normative data for young adults supports clinicians in distinguishing pathological findings from normal age-related variability, enhancing diagnostic precision.
Rehabilitation professionals can also use these data to tailor interventions based on individual functional profiles and recovery trajectories, contributing to more efficient and personalized care. Integrating these insights into vestibular therapy practice may improve patient outcomes by facilitating early identification and focused treatment of subtle or early-stage vestibular impairments.
Future research should adopt longitudinal designs to investigate the progression of VOR function and compensation across the lifespan. Broader and more balanced samples, particularly in age and sex, are needed to enhance the generalizability of findings. Moreover, developing normative datasets for other commonly used rotary chair subtests such as step velocity, subjective visual vertical (SVV), subjective visual horizontal (SVH), and dynamic unilateral centrifugation would support evidence-based clinical decisionmaking. Lastly, given the time-intensive nature of SHA testing, future studies should assess whether each tested octave frequency provides unique, clinically actionable information that justifies its inclusion in routine assessment protocols.
Competing Interests
The authors declare that they have no competing interests.
List of Abbreviations
A Repeated Measure Analysis of Variance (ANOVA) Dizziness Handicap Inventory (DHI) NeuroKinetics I-Portal Rotary Chair (NOTC) Subjective Visual Horizontal (SVH) Subjective Visual Vertical (SVV) Vestibular-Ocular Reflex (VOR) Optokinetic Nystagmus (OKN) Vestibular-Ocular Reflex (VOR) Videonystagmography (VNG)
Acknowledgments
The researchers would like to thank the Commonwealth University of Pennsylvania – Bloomsburg, as this was the site of this study’s completion. The researchers would also like to acknowledge Dr. Devon Suiter and Dr. Michael McKenna, who assisted with data collection and supported the researchers throughout the project.
References
Chan, Y., Galatioto, S., Amato, M., & Kin, N. (2016). Evaluation of sinusoidal harmonic acceleration responses in a healthy population. *Journal of Vestibular Research, 26*(5–6), 409–416.
Agrawal, Y., Carey, J. P., Della Santina, C. C., Schubert, M. C., & Minor, L. B. (2009). Disorders of balance and vestibular function in US adults: Data from the National Health and Nutrition Examination Survey, 2001-2004. *Archives of Internal Medicine, 169*(10), 938–944. View
Jacobson, G. P., & Shepard, N. T. (2016). *Balance Function Assessment and Management* (2nd ed.). Plural Publishing.
Maes, L., Dhooge, I., D’haenens, W., Bockstael, A., Keppler, H., Philips, B., ... & Vinck, B. (2010). Measuring the vestibuloocular reflex in children. *International Journal of Pediatric Otorhinolaryngology, 74*(10), 1135–1141.
Ahmed, R. M., Goebel, J. A., & Sinks, B. C. (2009). The clinical application of rotational chair testing. *Otolaryngologic Clinics of North America, 42*(1), 111–120.
Creswell, J. W. (2014). *Research design: Qualitative, quantitative, and mixed methods approaches* (4th ed.). SAGE Publications. View
Jacobson, G. P., & Newman, C. W. (1990). The development of the Dizziness Handicap Inventory. *Archives of Otolaryngology– Head & Neck Surgery, 116*(4), 424–427. View
JASP Team. (2019). *JASP (Version 0.11.1) [Computer software]*. https://jasp-stats.org Laerd Statistics. (n.d.). *Sphericity in repeated-measures ANOVA*. View
Li, C., Layne, C., Neely, G., & Collins, S. (1991). Frequency specific characteristics of the vestibulo-ocular reflex in normal subjects. *Annals of Otology, Rhinology & Laryngology, 100*(9), 765–769.