
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 6 (2025), Article ID: JRPR-180
https://doi.org/10.33790/jrpr1100180Review Article
Comparative Effectiveness of Medication-Assisted Treatment (Mat) for Opioid Use Disorder in Residential Settings: A Literature Review
Noel Casiano1*, and Nicholas Casiano2
1,2The Life Center of CT, Inc, 15-17 May Street, Hartford, CT 06105, United States.
Corresponding Author Details: Noel Casiano, The Life Center of CT, Inc, 15-17 May Street, Hartford, CT 06105, United States.
Received date: 17th June, 2025
Accepted date: 17th July, 2025
Published date: 19th July, 2025
Citation: Casiano, N., & Casiano, N., (2025). Comparative Effectiveness of Medication-Assisted Treatment (MAT) for Opioid Use Disorder in Residential Settings: A Literature Review. J Rehab Pract Res, 6(2):180.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Opioid Use Disorder (OUD) remains a public health crisis, with increasing rates of overdose and relapse. Medication-Assisted Treatment (MAT) is the gold standard for treating OUD, but outcomes vary based on the medication type, setting, and duration. This literature review synthesizes current research on MAT efficacy in residential treatment programs, focusing on long-term sobriety outcomes. Utilizing a systematic review of 31 empirical studies published between 2018 and 2024, the findings indicate that while all FDA-approved MAT options, methadone, buprenorphine, and extended-release naltrexone, improve treatment retention and reduce opioid use, buprenorphine and extended-release naltrexone show greater potential for long-term success when combined with residential care. Limitations and future research needs are discussed.
Keywords: Opioid use Disorder, Medication-Assisted Treatment, Residential Treatment, Buprenorphine, Methadone, Extended- Release Naltrexone, Long-Term Recovery, Substance use Disorder
Introduction
Opioid Use Disorder (OUD) continues to pose a major public health challenge. Deaths due to overdose from synthetic opioids, mainly fentanyl, have increased very significantly in the United States and reached record levels [1]. Medication-Assisted Treatment has thus evolved to become the best standard practice treatment for OUD. The treatment combines three pharmacological agents approved by the FDA – methadone, buprenorphine, and extended-release naltrexone (XR-NTX) – with psychosocial and behavioral therapies that would address the complex biopsychosocial dimensions of the problem of addiction [2].
MAT has consistently reduced opioid abuse, lower risks of overdose, and better retention in treatment [3] but varies by setting, patient characteristics, and the availability of post-discharge supports. Most research has focused on outpatient care. There is less evidence comparing outcomes for MAT in residential treatment programs where structured, medically supervised environments are provided that support stabilization and comprehensive therapeutic engagement [4].
This literature review weaves recent empirical evidence on the effectiveness of residential MAT around the core of long-term sobriety outcomes. It tries to answer the question of which MAT modality between methadone, buprenorphine, or XR-NTX best supports sustained recovery post-discharge. This review attempts to provide an answer while considering how integrated behavioral supports and patient-specific factors drive results.
Also very importantly, the concept of "success" in OUD treatment has shifted beyond abstinence alone to include a broader indicator conceptualization comprising functional recovery, social reintegration, and quality of life. Meanwhile health systems are progressively individualizing and integrating interventions by the type of MAT options that facilitate such extended version of recovery [5].
The central research question guiding this review is: What is the most effective MAT for individuals with OUD in residential treatment settings that promotes long-term sobriety? A systematic review of thirty-one empirical studies published between 2018 and 2024 will be used to try to inform clinical decision-making and policy development by identifying evidence-based best practices for delivering MAT in residential care.
Methodology
This review used a systematic literature search to find recent empirical studies about medication-assisted treatment (MAT) for opioid use disorder (OUD) inside residential treatment settings, and long-term sobriety outcomes. Major academic databases such as PubMed, PsycINFO, and Cochrane Library were thoroughly searched from January 2018 publications through April 2024 to make sure the most up-to-date evidence was included.
A combination of keywords and Medical Subject Headings (MeSH) terms guided the search strategy: “opioid use disorder,” “residential treatment,” “medication-assisted treatment,” “buprenorphine,” “methadone,” “naltrexone,” “long-term recovery,” and “treatment retention.” Boolean operators (“AND,” “OR”) were utilized to refine the search and capture relevant studies examining both pharmacological interventions and their integration with psychosocial supports.
Eligibility criteria mandated that studies:
• Focus on adult populations (≥18 years old) diagnosed with OUD;
• Include participants receiving residential or inpatient treatment services;
• Evaluate the use of FDA-approved MAT agents (methadone, buprenorphine, or extended-release naltrexone);
• Report on follow-up outcomes measuring retention in treatment, abstinence, relapse rates, or other indicators of long-term recovery, with a minimum follow-up period of six months post discharge;
• Be peer-reviewed empirical research published in English.
Studies that focus exclusively on outpatient settings without residential components and pediatric populations and those that do not provide adequate follow-up data were excluded.
After initial screening of titles and abstracts, 67 articles underwent full-text review. In the end, 31 studies qualified, 18 as original research articles that included randomized controlled trials (RCTs), prospective or retrospective cohort studies, and naturalistic longitudinal designs, while the remaining 13 were meta-analyses or systematic reviews that aggregated broader evidence on MAT effectiveness.
Study design, sample characteristics, type of MAT initiated during residential treatment, length and quality of psychosocial supports, outcome measures and follow-up duration were all emphasized in the data extraction. Quality appraisal of studies was conducted using established checklists appropriate to each design - for example, the Cochrane Risk of Bias Tool for RCTs.
This methodology ensured a synthesis of current evidence on the efficacy of MAT within residential treatment frameworks that could be robust and comprehensive, thereby allowing informed conclusions about what the best practice would be to support continued sobriety in populations with OUD.
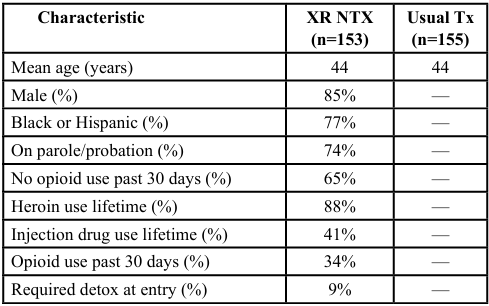
Table 1. Baseline Characteristics & Enrollment — Extended Release Naltrexone vs. Usual Treatment (Criminal Justice Pop.). [6]
The first table summarizes baseline characteristics and enrollment data from a randomized clinical trial evaluating extendedrelease naltrexone (XR-NTX) versus treatment-as-usual among individuals with opioid use disorder (OUD) involved in the criminal justice system [6]. Participants were predominantly male (85%), racially diverse (77% Black and Hispanic), and had significant histories of heroin and injection drug use. Notably, 79% were under legal supervision (probation or parole), and 65% reported no opioid use in the past 30 days, suggesting a relatively stable baseline at entry. Approximately 8.5% required detoxification before initiating XR-NTX. Retention was relatively high during the initial phases of the study, with 95% of XR-NTX participants receiving the first injection and 61% completing all six scheduled doses. These data highlight the feasibility of initiating XR-NTX in a structured setting with justice-involved individuals and suggest good short-term engagement with treatment.
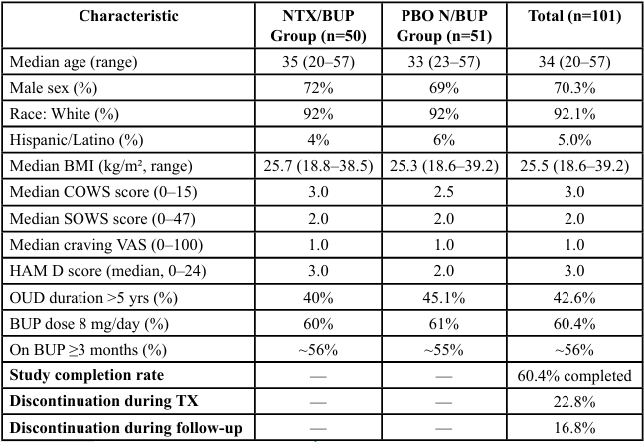
Table 2. Baseline Demographics — Transitioning from Buprenorphine to XR NTX. ([7] American Journal on Addictions, 2020) #6
The second table presents baseline demographics from a randomized controlled trial that examined the transition from buprenorphine to extended-release naltrexone [7]. This sample included 101 participants with similar demographic profiles across treatment arms, including a median age of 34, approximately 70% male, and over 92% identifying as White. The majority of participants had been on buprenorphine for at least three months, with daily dosages of 8 mg or higher. Baseline measures of withdrawal (Clinical Opiate Withdrawal Scale, COWS) and depression (Hamilton Depression Rating Scale, HAM-D) were low across both groups, indicating stability before transitioning medications. Despite these promising initial conditions, the study reported a 60.4% overall completion rate, with approximately 23% of participants discontinuing during treatment and another 17% lost during follow-up. These findings underscore the challenges of medication transitions in residential or medically supervised environments, even among relatively stable populations.
Together, these tables illustrate the methodological rigor of studies comparing MAT modalities within structured settings and highlight the importance of considering baseline patient characteristics and retention dynamics when evaluating long-term sobriety outcomes.
Participant Characteristics and Study Retention
Two studies have been referenced here in order to draw an outline of the methodological framework and MAT intervention participant characteristics inside residential or structured treatment settings.
The first study, conducted by Lee et al. [6], examined the efficacy of extended-release naltrexone (XR-NTX) versus treatment-as-usual among a justice-involved population diagnosed with opioid use disorder. A total of 308 participants were randomized (153 to XRNTX, 155 to usual care) following an initial screening of 437 individuals. The sample was demographically diverse, with 85% male and 77% identifying as Black or Hispanic. Most participants were under legal supervision (82%) and had significant histories of heroin use (88%) and injection drug use (42%). Notably, 65% reported abstinence from opioids in the 30 days prior to enrollment, and only 9% required detoxification prior to XR-NTX induction. Retention and adherence were strong in the early treatment phases, with 95% of participants receiving the initial injection and 61% completing all six monthly doses. These data suggest that XR-NTX is a feasible and potentially sustainable intervention in residential or correctional environments, particularly when supported by intensive clinical oversight.
The second study, conducted by Comer et al. [7], assessed the transition from buprenorphine to XR-NTX in a controlled clinical setting. Among 101 randomized participants, the demographic composition was relatively homogeneous, with a median age of 34 years and 70% identifying as male. Over 92% of participants were White, and more than half had been maintained on buprenorphine for three or more months at a dosage of 8 mg/day or higher. Baseline withdrawal symptoms, as measured by the Clinical Opiate Withdrawal Scale (COWS), and depressive symptoms, via the Hamilton Depression Rating Scale (HAM-D), were low across groups. Despite the clinical stability of the sample, the study reported a completion rate of 60.4%, with approximately 23% of participants discontinuing during the treatment phase and another 17% lost during follow-up. These findings highlight the inherent difficulty of transitioning between MAT regimens, even within a medically supervised setting, and underscore the need for individualized planning and support during such transitions.
Collectively, these investigations offer essential perspectives on the practicality, compliance trends, and situational obstacles of MAT administration within residential and organized settings. They emphasize the importance of considering both therapeutic and social variables in assessing the extended efficacy of MAT in fostering enduring rehabilitation from opioid usage issues.
Results
Methadone
Methadone continues to be the most extensively studied MAT with demonstrated efficacy in reducing illicit opioid use and improving treatment retention [8]. However, its daily dosing requirement and strict regulatory oversight pose challenges for patient’s postresidential care, often resulting in moderate relapse rates [9]. Numerous studies have confirmed methadone’s effectiveness in increasing treatment retention and reducing illicit opioid use during residential and outpatient care [8]. Its full opioid agonist properties provide substantial relief from withdrawal symptoms and drug cravings, which supports patient stability during the early phases of recovery. A large-scale meta-analysis conducted by Mattick, et al., [8] reported retention rates of 60% to 80% at 6 months in residential programs using methadone, which was significantly higher than placebo or non-MAT interventions.
In the long run, after residential care, methadone does not seem to be as effective. It is only available through extremely regulated OTPs, and because of possible diversion and overdose risks, making it less attainable and probably less sustainable post-discharge. Long-term studies have indicated moderate rates of relapse from 35% to 50% within a period of just 6 to 12 months after discharge. Particularly in the absence of structured outpatient support for individuals or when housing stability is an issue [9,10]. This places into perspective how much methadone can be effective under a residential stabilization setup but falls short in the absence of proper comprehensive continuums of care.
Buprenorphine
Buprenorphine is a partial agonist opioid with a good safety margin because of its ceiling effect on respiratory depression, and thus it has become an alternative widely accepted in use compared to methadone. It can be offered daily and long-acting monthly (for example in sublocade form) which will ensure adherence after discharge. In residential settings, buprenorphine has shown retention rates equal to that of methadone. The medication initiated in a residential program by patients, maintained abstinence at higher rates than that of methadone at about 68% compared with 52% at the 12-month follow-up-as reported by Degenhardt, et al., [11]. Such results are more pronounced in patients who got extended psychosocial support following discharge-considerably recovery coaching or housing support.
Buprenorphine shows identical retention rates with methadone in residential treatment and is preferred because it is safer to use, since there is a ceiling effect related to respiratory depression [12]. Better abstinence at 12 months was reported by Degenhardt, et al., [11] when buprenorphine was initiated in residential programs-consistent with findings from the large-scale randomized trial conducted by Lee, et al., [13].
Additionally, the lower potential for overdose associated with buprenorphine, easier administration, and growing availability of access through (OBOT) models make it a more flexible, scalable treatment option to use as treatment for continuing care following residential treatment. Studies have indicated that patients on buprenorphine have lower discontinuation rates and greater satisfaction with care when their provider offers this in the context of shared decisionmaking around their treatment plan [3].
Extended-Release Naltrexone (XR-NTX)
Extended-release naltrexone (XR-NTX) is a formulation that essentially represents a novel paradigm, being an opioid antagonist, blocking the action of opioids without precipitating withdrawal or euphoria. It is available as a monthly injection and requires complete detoxification before induction. This has also been the reason for its low uptake. However, residential settings do offer very optimal contexts for medically supervised withdrawal periods, which are required for XR-NTX induction. Full detoxification is needed before administration of XR-NTX but it has quite good evidence in long-term relapse prevention. Krupitsky et al., [14] found that the combination of XR-NTX and cognitive-behavioral therapy reduced relapse rates at both 12 months and 18 months distinctly compared to control groups. Similar conclusions were drawn by Lee et al., [6] in which this medication was indicated to be much more efficient among criminal justice populations starting treatment in controlled environments.
Krupitsky, et al., [14] noted significantly lower relapse rates at 12 and 18 months for individuals initiated on XR-NTX in residential treatment compared to those initiated on buprenorphine. When structured cognitive-behavioral therapy (CBT) and case management were added to the plan, abstinence rates that would otherwise not surpass 70% at one-year post-treatment are realized. Lee, et al., [13] in a randomized trial also found that XR-NTX is not inferior to buprenorphine in the prevention of relapse among patients who have successfully initiated medication post-detox.
However, there are barriers to the use of XR-NTX. The same detox requirement which lowers the rate of induction onto treatment as compared to agonist therapies applies here, and in general, there is an increased risk of dropout if a patient begins treatment with cravings or has low motivation toward treatment. This does suggest that targeting highly motivated patients or targeting areas where community support can be mobilized post-discharge would make this medication more effective.
Combination with Psychosocial Support
Medication-assisted treatment, combined with behavioral therapies and peer support yield better retention and long-term outcomes [15,16]. Residential programs that implement comprehensive patientcentered psychosocial care provide greater sustained recovery rates, emphasized by [4]. Medication-assisted treatment combined with behavioral treatments such as Cognitive Behavioral Treatment, Motivational Interviewing, and trauma-informed approaches increases adherence to medication and decreases relapse highlighted by [15]. Studies have also emphasized the necessity of a strong linkage for patients to peer recovery support and housing assistance and employment services in comprehensive discharge planning [5].
In particular, retention in post-residential care programs was markedly higher when MAT was paired with 12-step facilitation, recovery coaching, and consistent follow-up through case management services [10]. These interventions were associated with improved self-efficacy, better coping strategies, and stronger recovery capital, all of which are protective factors against relapse. Thus, regardless of the specific MAT medication used, long-term sobriety is most likely when pharmacological and psychosocial supports are delivered in an integrated, continuous care framework.
Discussion
This literature review underscores crucial differences between the three main medication-assisted treatment (MAT) options; methadone, buprenorphine, and extended-release naltrexone (XRNTX) in residential treatment for opioid use disorder (OUD). The other two medications besides methadone available for treatment, buprenorphine, and XR-NTX show better long-term results in residential settings when there is an option to include structured behavioral health treatments such as cognitive-behavioral therapy (CBT), motivational interviewing, and recovery coaching. Buprenorphine has long been credited with pharmacological effectiveness and safety that easily allows flexibility for treatment in trying to achieve long-term abstinence and retention post-discharge. As a partial agonist medication, it carries reduced overdose risk and can extend more freedom to patients when shifted into the monthly-injectable form or when applied within an Office-Based Opioid Treatment (OBOT) setting. It makes Buprenorphine not just appropriate for acute stabilization while in residential care but also supportable as a bridge into long-term outpatient recovery frameworks. Patients getting buprenorphine treatment who are relevant to therapy support were more likely to report better quality of life and reduced substance use at 12 months of follow-up [11].
Likewise, XR-NTX showed very good results in the maintenance of sobriety, particularly for individuals with a high motivation level to maintain total abstinence. It is administered once a month and since it blocks opioids from acting, it might interest patients looking for MAT that does not involve any sort of addiction. Should initiation be compared to other MATs, relapse rates at 12- and 18-month follow-ups are much reduced by XR-NTX. The major barrier is that induction requires completely opioid detoxified individuals; thus, its use is restricted immediately in most scenarios where treatment is carried out on an outpatient basis or in lower-acuity settings.
Residential treatment programs are conducted in a controlled environment with medical support available at all times. The findings support the recent trends in residential care protocols that prioritize the pathways of detox-to-induction for XR-NTX. This would be while making sure to integrate behavioral therapy as well as relapse prevention planning.
Methadone is highly effective in the acute phase of stabilization, but it poses great problems for post-residential continuity because it has to be administered daily and is not available outside federally regulated opioid treatment programs. Although residential care with methadone leads to good retention and symptom stabilization, its sustainability after discharge depends mostly on the availability of opioid treatment programs (OTPs) and patients’ compliance with an inflexible dosing schedule. Hence, relapse rates post-discharge are moderate to high particularly when an OTP infrastructure does not exist in underserved or rural communities. Therefore, while methadone does remain a foundational MAT option, this places the drug optimally for individuals who will subsequently move into structured outpatient OTPs where they have access to transport and adherence support.
This review underscores the very critical role of the residential treatment environment itself. Residential settings present an excellent opportunity for initiating MAT since one can take advantage of structure, clinical supervision, and peer support within these settings. These factors typically combine to form an optimal therapeutic milieu available in such settings wherein patients can both stabilize and detoxify while starting medications under close observation.
Also, residential care helps in making easy links to communitybased recovery networks when discharge planning is with coordinated referrals that include MAT continuation, housing support plus and behavioral health support. Studies reviewed found a consistent relationship between the integration of MAT with wraparound services including peer mentoring, vocational training, and family therapy and long-term outcomes.
Overall, buprenorphine and XR-NTX demonstrate superior longterm outcomes in residential settings, particularly when paired with comprehensive behavioral health support [13,14]. Methadone remains effective for acute stabilization but presents challenges related to daily dosing and continuity of care after residential discharge [9]. XR-NTX’s antagonist mechanism aligns well with patients motivated for abstinence, although detoxification requirements limit its initial accessibility [6]. Residential treatment offers an optimal milieu to initiate MAT by providing structure, medical supervision, and peer reinforcement, which facilitate better engagement and smoother transitions to outpatient care [3,4].
The evidence also underscores the critical role of tailored, patientcentered care plans that consider individual factors such as comorbid mental health disorders, social determinants, and patient preferences [12,16]. Without adequate integration of behavioral supports and discharge planning, the risk of relapse remains high despite pharmacological treatment [15].
In summary, while no single MAT has been demonstrably superior across populations, buprenorphine and XR-NTX have the best hopeful profiles for long-term sobriety that can be achieved in a residential setting. Success is most optimally achieved with behavioral health intervention support during treatment and robust continuity of care after discharge. Methadone certainly plays a role where there is high opioid tolerance and complex clinical presentations as an immediate stabilizer. However, its challenges underscore the need for enhanced discharge planning and better linkages to outpatient OTPs. The MAT outcome can be optimized if programmatic intervention is based on pharmacological efficacy and structural supports that are available to individuals across the recovery continuum.
Limitations of the Research
Valuable knowledge notwithstanding, current studies about medication-assisted treatment (MAT) for opioid use disorder (OUD) in residential settings have great limitations that reduce both generalizability and interpretability of the published results.
First, selection bias has always been a formidable challenge. Those who do well getting started on extended-release naltrexone (XR-NTX) typically share such factors as internal motivation, social support, or previous abstinence-applicable factors that make them predisposed to good outcomes in treatment. This is described as a self-selection effect and complicates comparisons with methadone or buprenorphine recipients who may be in treatment under more coercive or emergent conditions. Therefore, differences in relapse or retention rates between the medications might mostly be about baseline disparities rather than medication efficacy.
Second, variability in residential treatment quality, duration, and clinical staffing within the same study further limits the generalizability of findings across studies. Degrees of intensity regarding therapeutic intervention, peer support, access to clinical staff, and the quality of discharge planning components are assumed to vary and are known to influence outcomes. For example, results found from a study involving patients receiving XR-NTX in a highresource facility where comprehensive behavioral health support is provided cannot be generalized to other settings with less resource availability. Unless standardized treatment conditions are imposed across studies, it would be medication delivered and not the environment delivering it that could be isolated as having a specific effect.
Third, many existing studies suffer from short follow-up periods. Most studies that have been reviewed only track participants for 6 to 12 months post-treatment. Very few go beyond 18 months. This does not allow us to understand how durable the benefits of MAT are over time. Since sustained recovery typically requires cycles of relapse and re-engagement, long-term data are needed on whether initial treatment success is translated into sustained sobriety and improved life functioning. Without long-term outcomes, it is also difficult to assess the extent to which MAT contributes to the broader psychosocial recovery of an individual including such factors as stability in employment, reduced involvement with the criminal justice system, and family reunification.
Fourth, there is inconsistent attention to social determinants of health across the MAT literature. Stable housing, employment, and transportation, community stigma, and family support are recovery factors that are variably reported and unevenly measured in the existing literature. These external factors can and do moderate the effectiveness of MAT by influencing adherence to treatment as well as engagement in follow-up care and overall quality of life, however, they are rarely systematically assessed. Without their systematic assessment, results cannot be applied equitably across diverse populations and particularly the most marginalized or underserved groups.
Lastly, racial and ethnic disparities in MAT access and outcomes remain underexplored. While some studies report demographics of participants, even fewer disaggregate their results by race, gender, or socioeconomic status. Such oversight further limits the ability of this field to understand how structural inequities intersect with MAT engagement and success for the very population that is most disproportionately impacted both by opioid use and by systemic barriers to care.
Several limitations are noted within the current literature. Selection bias is common, as patients opting for XR-NTX may be inherently more motivated, skewing comparative results [13]. Variability in the quality, duration, and intensity of residential treatment programs complicates generalizations across studies [4]. Additionally, most research includes follow-up periods of less than 18 months, limiting insight into truly sustained recovery [14]. Finally, social determinants such as housing stability and family support, known to influence MAT success, are inconsistently accounted for, which hampers a holistic understanding of long-term outcomes [16].
Taken together, these limitations suggest the necessity of more stringent and longitudinal equity-focused studies to properly assess the long-term effectiveness of MAT modalities in residential treatment settings. Such future studies should be designed in a much more rigorous manner, having control for motivational as well as environmental variables including social determinants of health and ensuring diversity of demographic and geographic population representation.
Future Considerations
Building on the current evidence base, future studies about Medication-Assisted Treatment for OUD in residential treatment settings should address gaps in the evidence and further articulate factors that contribute to long-term recovery, with an extension beyond 24 months to better triangulate the durability of MAT-related outcomes about sustained abstinence and psychosocial functioning as well as quality of life. Longitudinal studies are sorely missing from the literature. Since relapse typically happens post one year of treatment, short-term follow-ups do not capture fully the dynamism and even the success that people have in maintaining sobriety over time.
Additionally, there is also a need for properly designed randomized controlled trials (RCTs) comparing the efficacy of different types of MAT-especially methadone, buprenorphine, and extended-release naltrexone-when initiated within standardized residential treatment programs with controlling intensity and type of psychosocial interventions being provided. Such trials should define the intensity and type of psychosocial support such as cognitive-behavioral therapy (CBT), motivational interviewing (MI), or 12-step facilitation that is often and variably described in studies to further 'standardize' these supports to help isolate the pharmacological effects of the medication from that of the treatment environment. This would allow comparison across MAT modalities.
Also, future studies should look at or test personalized or stratified ways of giving MAT by patient features such as severity of addiction, related mental health issues, history of trauma, number of past attempts at treatment, and level of motivation. The use of precision medicine rules by matching special ways to treat to related profiles may raise the likelihood of keeping and engaging in treatment and its success. This path would gain from the design and checking of tools for clinical decisions that help providers choose between many forms of MAT for different needs in patients.
Also, extremely important as an avenue for future study is the role of recovery housing and community-based support networks in sustaining outcomes on MAT after residential treatment discharge. Stable housing environments, inclusive of recovery residence or sober living programs, have generally been related to improved retention in care and reduced relapse; however, empirical studies intersecting the fields of MAT and recovery housing are limited. The research should also be oriented toward the impacts that wraparound services such as employment assistance, peer recovery coaching, and family support programs may have post-treatment in success. Specifically, when returning individuals to high-risk or underserved communities.
In the future, studies should purposely select and vary samples of different populations and settings across race, gender, socioeconomic status, and geography. Therefore, by social determinants of health and health equity in the study, the researcher stands a better chance of developing an intervention that works not only for the general population but also addresses specific unique barriers among marginalized groups to be more responsive who are facing the opioid crisis.
Future research should focus on long-term longitudinal studies exceeding 24 months to capture sustained recovery trajectories beyond the acute post-treatment phase Lee, et al., [13]. Randomized controlled trials comparing MAT modalities initiated in residential care with standardized psychosocial supports are needed to isolate the medication effect and optimize integrated treatment protocols [12,15]. Personalized MAT approaches that consider patient-specific factors such as psychiatric comorbidity, motivation, and prior treatment history, may improve retention and outcomes Doernberg, et al., [16]. Further exploration of recovery housing and communitybased supports post-discharge will clarify their role in enhancing MAT effectiveness Hadland, et al., [4]. Finally, research should prioritize diverse populations to address health disparities and ensure equitable access to evidence-based MAT services [2].
In summary, a future-oriented research agenda that places longterm, individual, and situational inquiries reflecting the complex realities of recovery at the forefront is promised to develop. This will not only fine-tune the clinical decision-making process but also policies and practices in sustaining recovery and bringing lives back to normal for people suffering from opioid use disorder.
Conclusion
This comprehensive literature review proves that there is no single medication-assisted treatment (MAT) which can be described as best for every individual with opioid use disorder (OUD) in residential treatment settings. At this stage of knowledge development, however, existing evidence consistently leads to the two MAT modalities, namely buprenorphine and extended-release naltrexone (XR-NTX), as those having the strongest support for long-term sobriety and retention if initiated during residential care. They offer pharmacological advantages from different perspectives. Buprenorphine with a partial agonist profile offers a safety margin, XR-NTX an antagonist product offering seemingly more consistent with patients seeking total abstinence.
The major determinant of the success of these MAT options lies in their integration with comprehensive, person-centered behavioral health support. Other critical components of treatment for OUD that must be integrated into pharmacotherapy are Cognitive-Behavioral Therapy (CBT), Motivational Enhancement Therapy (MET), and Peer Recovery Services. These psychosocial interventions have been more adherent to treatment, relapse rates reduced, and functioning better when combined with medication support than either intervention or medication alone. This speaks to the imperative need for integrated care addressing the biopsychosocial dimensions that create the multifaceted nature of OUD.
Given the heterogeneity of patients presenting to residential treatment, differing in addiction severity, co-occurring mental health conditions, motivation, and social support systems. Programs should prioritize flexible and individualized MAT protocols. Flexible approaches allow medication choices and psychosocial interventions to be adjusted to the specific needs and preferences of the individual such that optimal engagement and outcomes are achieved.
Clinical and Policy Recommendations
1. Staffing Models: Residential programs should adopt interdisciplinary staffing models that include addiction medicine specialists, psychiatric providers, trained nursing staff, peer recovery coaches, and licensed behavioral health clinicians. This team-based approach ensures the coordinated delivery of MAT alongside evidence-based psychotherapy and wraparound services.
2. Medication Induction Protocols: Programs should develop clear and flexible medication induction protocols that allow for the timely initiation of buprenorphine or XR-NTX based on a thorough clinical assessment. Incorporating shared decisionmaking and motivational interviewing during induction can improve patient engagement and adherence.
3. Discharge Planning: Effective discharge planning must begin at admission and include warm handoffs to outpatient MAT providers, linkage to recovery housing, continued access to peer support networks, and enrollment in intensive outpatient or community-based services. Establishing formal partnerships with outpatient clinics can reduce treatment gaps and prevent relapse.
4. Program Design Implications: Residential facilities should consider integrating longer-stay options or step-down levels of care for individuals needing extended stabilization. Programs should also invest in ongoing training for staff on best practices in MAT delivery, trauma-informed care, and stigma reduction.
5. Policy Advocacy: At the systems level, providers should advocate for insurance reimbursement models that support bundled care (e.g., combining MAT with psychosocial services) and regulatory frameworks that allow residential programs to initiate and maintain MAT without barriers. Emphasizing the need for parity between mental health, substance use, and medical services is critical for sustainable delivery.
In conclusion, residential treatment centers play a very important as the starting point of effective MAT strategies that significantly improve long-term recovery trajectories. As such, programs can reposition and operationalize supportive staffing structures, induction protocols, and discharge processes to embrace an evidence-based patient model of care by integrating pharmacological and behavioral treatments. More specifically, future research and policy development should focus on improving these approaches to maximize access and equity in long-term success across the diverse populations who have been variably impacted by the opioid epidemic.
Competing Interests:
The authors declare that they have no competing interests.
References
Centers for Disease Control and Prevention (CDC). (2024). Overdose Deaths Remain High in the U.S. Retrieved from View
Volkow, N. D., & Collins, F. S. (2017). The role of science in addressing the opioid crisis. New England Journal of Medicine, 377(4), 391–394. View
Hadland, S.E, Wharam, J.F., Schuster, M.A. (2017). Trends in Receipt of Buprenorphine and Naltrexone for Opioid Use Disorder Among Adolescents and Young Adults, 2001-2014. JAMA Pediatrics. 171 (8). 747-755. View
Laudet, A. B. (2007). What does recovery mean to you? Lessons from the recovery experience for research and practice. Journal of Substance Abuse Treatment, 33, 243-256. View
Lee, J. D., Friedmann, P. D., Kinlock, T. W., Nunes, E. V., Boney, T. Y., Hoskinson, R. A., Jr., ... & O’Brien, C. P. (2016). Extended-release naltrexone to prevent opioid relapse in criminal justice offenders. New England Journal of Medicine, 374(13), 1232–1242. View
Comer, Sandra D, Mannelli, Paolo, Alam, Danesh, Douaihy, Antoine, Nangia, Narinder, Akerman, Sarah C., Zavod, Abigail, Silverman, Bernard L., Sullivan, Maria A. (2020). Transition of Patients with Opioid Use Disorder from Buprenorphine to Extended-Release Naltrexone: A Randonmized Clinical Trial Assessing Two Transition Regimen. The American Journal on Addictions, 29: 313-322. View
Mattick, R.P., Breen, C., Kimber, J., & Davoli, M., Breen, R. (2009). Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence (Review). Cochrane Database of Systematic Reviews, (3), CD002209. View
Sordo, L., Barrio, G., Bravo, M. J., Indave, B. I., Degenhardt, L., Wiessing, L., ... & Pastor-Barriuso, R. (2017). Mortality risk during and after opioid substitution treatment: Systematic review and meta-analysis of cohort studies. BMJ, 357, j1550. View
Alrwaily, M., Timko, M., Schneider, M., Stevans, J., Bise, C., Hariharan, K, Delitto, A. (2016). Treatment-Based Classification System for Low Back Pain: Revision and Update. Phys Ther. 96(7):1057-1066. View
Degenhardt, L., Clark, B., Macpherson, G., Leppan, O., Nielsen, S., Zahra, E., Larance, B., Kimber, J., Martino-Burke, D., Hickman, M., Farrell, M. (2023). Buprenorphine versus methadone for the treatment of opioid dependence: A systemic review and meta-analysis of randomized and observational studies. Lancet Psychiatry. 10 (6): 386-402. View
Weiss, R. D., Potter, J. S., Fiellin, D. A., Byrne, M., Connery, H. S., Dickinson, W., ... & Ling, W. (2019). Adjunctive counseling during brief and extended buprenorphine-naloxone treatment for prescription opioid dependence: A randomized clinical trial. JAMA Internal Medicine, 179(1), 13–22. View
Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., ... & Rotrosen, J. (2018). Comparative effectiveness of extended-release naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): A multicenter, open-label, randomized controlled trial. The Lancet, 391(10118), 309–318. View
Volkow, N.D., Jones, E.B., Einstein, E.B. and Wargo, E.M. (2019). Prevention and Treatment of Opioid Misuse and Addiction: A Review. JAMA Psychiatry, 76, 208-216. View
Krupitsky, Evgeny, Zvartau, E., Blokhina, E., Verbitskaya, E., Wahlgren, V., Tsoy-Podosenin, M., Bushara, N., Burakov, A., Masalov, D., Romanova, T., Tyurina, A., Palatkin, V., Slavina, T., Pecoraro, A., Woody, G.E. (2012). Randomized Trial of Long-Acting Sustained-Release Naltrexone Implant vs Oral Naltrexone or Placebo for Preventing Relapse to Opioid Dependence. Arch Gen Psychiatry. 69 (9). 973-981. View
Nunes, E. V., Levin, F. R., Reilly, M. P., & El-Bassel, N. (2021). Medication treatment for opioid use disorder in the age of COVID-19: Can new regulations modify the opioid cascade? Journal of Substance Abuse Treatment, (122). View
Doernberg, M., Krawczyk, N., Agus, D., Fingerhood, M. (2019). Demystifying buprenorphine misuse: Has fear of diversion gotten in the way of addressing the opioid crisis? Substance Abuse; 40 (2). View