
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 6 (2025), Article ID: JRPR-185
https://doi.org/10.33790/jrpr1100185Research Article
Development and Validation of the Dance-Specific Movement Competency Screen for Multi-Genre Dancers
Marie-Eve Pepin1*, PT, OMPT, MSPT, DPT, Hannah Andersen2, MFA, NCPT, FMT, Abigail Skallerud3, PT, DPT, CIMT, BFA-Dance, Veronica Prieur4, PT, DPT, SCS, CSCS, NCPT, and Kristen Robertson5, PT, DPT, CMTPT/DN, NCPT
1Associate Professor, Department of Physical Therapy, Wayne State University, Eugene Applebaum College of Pharmacy and Health Sciences, 259 Mack Avenue, Detroit, MI 48201, United States.
2Associate Professor of Teaching, Maggie Allesee Department of Theatre and Dance, College of Fine, Performing and Communication Arts, Wayne State University. 4841 Cass Ave, Suite 3226, Detroit, MI 48201
3Restorative Physical Medicine, 42350 Grand River Ave, Novi, MI, 48375
4Wayne State University, Eugene Applebaum College of Pharmacy and Health Sciences, 259 Mack Avenue, Detroit, MI 48201, United States.
5Staff Therapist Team Rehabilitation, Livonia East 20276 Middlebelt Road, Suite 8, Livonia, MI, 48152
Corresponding Author Details: Marie-Eve Pepin, PT, OMPT, MSPT, DPT, Associate Professor, Department of Physical Therapy, Wayne State University, Eugene Applebaum College of Pharmacy and Health Sciences, 259 Mack Avenue, Detroit, MI 48201, United States.
Received date: 25th August, 2025
Accepted date: 13th October, 2025
Published date: 15th October, 2025
Citation: Pepin, M. E., Andersen, H., Skallerud, A., Prieur, V., & Robertson, K., (2025). Development and Validation of the Dance-Specific Movement Competency Screen for Multi-Genre Dancers. J Rehab Pract Res, 6(2):185.
Copyright: ©2025, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Several screening tools are used to predict injury risk in dancers, but few are applicable to dancers practicing multiple genres. More valid, reliable, and sensitive screening tools are needed for improved assessment and injury prevention. The purpose of this study is to evaluate the reliability and validity of a new Dance-Specific Movement Competency Screen (DSMCS) for intermediate to advanced dancers training in multiple genres.
Methods: The DSMCS tool includes 22 dance-specific movement tasks, each graded on a three-point scale. Tasks include movements such as knee flexion (plié), leg lifts (extensions), quadruped crawling, dynamic weight shifts, and jumping. Content validity was assessed using a survey of 15 dance and rehabilitation experts while concurrent validity was determined by comparing 16 participants’ scores on the modified STAR excursion balance test (mSEBT) and the DSMCS. Interrater reliability was determined in 9 participants using the intraclass correlation coefficient (ICC (3, k)) across five raters.
Results: Nearly 100% of experts rated items as relevant, suggesting good content validity. There were statistically significant correlations between the DSMCS and mSEBT composite scores on the right and left side (r=0.512, p=0.031; r=0.578, p=0.015 respectively) suggesting good concurrent validity. Interrater reliability between raters was 0.917 (0.793-0.979) and considered excellent.
Conclusion: The DSMCS is novel in its ability to assess movements specific to dancers performing multiple genres. It assesses lower and upper body movements, spinal mobility and stability, incorporates movements at various speeds, and one movement includes a cognitive task. While results indicate the DSMCS may be valid and reliable, more testing using a larger sample size is necessary to confirm these findings. The preliminary data indicates the DSMCS has strong potential to appropriately screen for movement abnormalities in dancers and to identify movement patterns that may increase injury risk.
3 Key Points 1. A new Dance-Specific Movement Competency Screen assesses (DSMCS) movement competency in dancers who practice multiple dance genres.
2. This research found good interrater reliability of treliability of the DSMCS.
3. The content validity was good and strong correlations between the modified STAR excursion balance test (mSEBT) and the DSMCS were found indicating good concurrent validity.
Introduction
As an artistic gateway to culture, community, and performance, the study of dance as a recreational, competitive, or concert- based activity is increasingly common in the United States. In 2023, it was estimated there were 10942 dance studios, and 624 degree granting college programs in the United States [1-3]. Participation in training and performance requires tremendous athleticism and motor control, and dancing at an advanced level necessitates practicing movements repetitively and vigorously for prolonged durations leading to a high injury rate. Professional dance companies have reported a 67% to 95% injury rate on an annual basis while 81% of collegiate contemporary dancers reported such injuries [4]. A 2021 systematic review identified poor lower extremity alignment as the most important risk factor for lower extremity injuries in both recreational and elite ballet dancers [5]. Poor lumbopelvic movement control, inappropriate transversus abdominis contraction, decreased lower-extremity strength, and poor aerobic fitness were other risk factors identified in elite ballet dancers [5].
Many screening tools have been used to predict injury risks including, but not limited to, range of motion (ROM), strength, muscle endurance, Beighton Criteria, Star Excursion Balance Test (SEBT), Movement Competency Screen (MCS), Functional Movement Screen (FMS) and turnout measurements. In a 2018 meta-analysis, Armstrong [6] reviewed many of these screening tools in dancers of all genres and found that impairments such as ROM, posture, hypermobility, and strength were not consistently predictive of injuries in dancers. There was also a lack of evidence for movement screening tools like the MCS, FMS and SEBT [6]. The only helpful tool was the measurement of different types of turnout; however, this measure is very specific to ballet and turnout measurements may not be helpful for screening dancers who perform other genres [6]. A study by Coogan et al. [7] also found that the FMS did not predict injury rates in collegiate dance majors and reported that the tool “may not be sensitive enough to adequately capture dysfunctional movements predictive of injury in this particular (dance) population.” A very recent study by Watson et al. [29] established normative values and examined correlations for commonly used dance screening tests, including the FMS, Beighton Scale, Harvard Step Test, Y-Balance Test, Plank Tests, and Turnout Test. While this work provides valuable reference data and demonstrates replicability for future dance injury prevention programs, it did not evaluate the reliability or validity of the screening tests, nor did it examine their relationship to injury risk. Finally, a review by Callahan and Mangum (2024) [31] also concluded that the FMS was not predictive of injuries in ballet and modern dancers and that “while the MCS shows injury prediction potential, a dance-specific movement screening more accurately representing dance-related movement patterns may improve validity in this population.”
Strength and range of motion do not always translate to dance specific movements, and motor control may be more critical for proper technique execution [32]. Studies have shown that poor alignment and movement competency are key risk factors for injury [5,31], raising the question of why commonly used functional screens fail to identify dancers at risk. The authors, echoing Callahan and Mangum [31], speculate that the existing tools may not be specific enough to capture the unique movements that put the dancers most at risk or may not challenge the dancer sufficiently to reveal important deficits. Many dance movements are compound in nature and require multiple body regions to work in integration. In addition, most screening tools have been designed for the classical ballet dancer, which may not be specific enough to dancers who predominantly practice other dance genres. Many collegiate dance training programs now require dancers to study dance forms originating from the African diaspora including hip-hop, breaking, jazz, tap, afrobeat, and West African dance in addition to the contemporary modern and ballet curricula. Since dancers often study more than one discipline, especially at the collegiate level, valid, reliable, and sensitive dance-specific screening tools need to be developed for dancers of mixed genres. To the authors’ knowledge, no functional movement screen exists specific to the demands of contemporary modern, ballet, and African diasporic dance forms.
Pre-season screenings are valuable for the pre-professional dance community [8]. They can provide valuable information to the clinician or dance instructor to guide dance and rehabilitation prescription to the specific dancer’s needs, offer a baseline score for comparison and tracking, and have the potential to identify injury risk factors. Screening tools using dance movements have been created and published. Bronner and Bauer [8] developed a three-task movement screen (second position grande plié, developpé a la seconde, and jumps in first position) rating the spine and lower extremity joints as either problematic or within normal limits. Bowerman [9] suggests a two-task assessment (fondu and temps levé) to screen elite adolescent ballet dancers. The authors use video analysis to measure degrees of turnout, knee valgus angle and lateral pelvic tilt [9]. Steinberg (2012) [10] advocates a three-task movement screen (relevé, turnout, plié) at slow and usual speed, and rated the movements as either correct or incorrect. Schultz et al. (2024) [30] developed the Columbia Adolescent Dancer Screen (CADS), which administers health questionnaires and evaluates injury history, aerobic capacity, range of motion, strength, balance, orthopedic tests, and dance technique. Technical skills included: functional turnout, demi plié in first position, développé a la seconde, single leg sauté, and relevé in retiré. In three studies, movement quality, as assessed by the movement screens, was correlated with injury risks in the dancers [8-10]. However, the screens only used a few dance-specific tasks derived directly from ballet, thus, not capturing the multitude of skills needed by the dancer of multiple genres such as motor control with crawling and quadruped positions, jumping, use of the parallel position, weight shifting in all directions, and coordination of the spine while performing lower extremity tasks [8,9,10,30]. Only Steinberg [10] assesses movements at various speeds, and none add cognitive loads to the movement tasks. The screens from Bronner and Steinberg [8,10] use a dichotomized assessment of “correct/incorrect,” which could lower sensitivity and responsiveness. Bowerman [9] employed a video analysis assessment, which may be inaccessible to most health and dance professionals, and is specific to ballet dancers, whereas Bronner [8] assessed only college-level modern dancers. Clearly, there remains a critical need for a comprehensive, validated, dance specific screening tool that can assess movement competency across multiple genres and identify dancers at risk for injury. While existing tools have been used in dance populations, they often lack specificity to the unique movement patterns and demands of different dance styles. The DSMCS was developed to address this gap by providing a validated, dance-specific assessment that evaluates a wide range of movements across multiple genres, including ballet, modern, and contemporary. The purpose of this manuscript is to describe the development of the Dance-Specific Movement Competency Screen (DSMCS) and explore its reliability and validity. The authors hypothesized that:
1. Content validity: The screen would demonstrate good content validity by showing agreement between experts.
2. Concurrent validity: Scores on the DSMCS would have fair-to good correlation to the scores on the Y balance portion of the SEBT.
3. Reliability: The DSMCS would demonstrate good interrater reliability.
Methods
Study Design
This study used a mixed methods design.
Procedure
Institutional Review Board approval was granted prior to initiation of research activities. The data was collected over a three-year period at a Level 1 Research University. This study has several components: development and description of the screening tool, assessment of content and concurrent validity, and assessment of interrater reliability.
Development of the DSMCS
A team of five movement experts participated in the development of the screening tool (two dance educators, one physical therapist, and two physical therapists who were also dance educators). The developers followed the recommendations and steps described by Bennet et al [11] on how to create a high-quality movement assessment tool (Table 2). Using those guidelines, the authors performed a comprehensive literature review and triangulated their clinical experience and dance expertise to select the screening tool tasks. Selected movements met two criteria: 1) a potential to reveal imbalances or alignment issues that could increase injury risks in dancers and 2) had components commonly performed in contemporary modern, ballet, and/or African diasporic dance training. Table 1 lists the key scientific articles on movement competency and injury risk factors that were used to create this screen.
Description of the DSMCS
The DSMCS tool includes twenty-two movement tasks, each graded on a three-point scale. Tasks include basic dance movements such as knee flexion (pliés), spinal articulations, dynamic weight shifts, jumps, leg lifts (extensions), quadruped crawling, and calf raises (relevé). Some are performed in a variety of starting positions such as feet parallel, external rotation (turn out), and quadruped. To best reflect the demands of dance, some tasks use a set rhythm from a metronome, and one includes a simultaneous cognitive task. The DSMCS comes with specific implementation and grading instructions as well as a detailed verbal script for each task that can be read verbatim. Utilizing the rubrics provided, each task is rated on a three-point scale following objective and well described criteria.
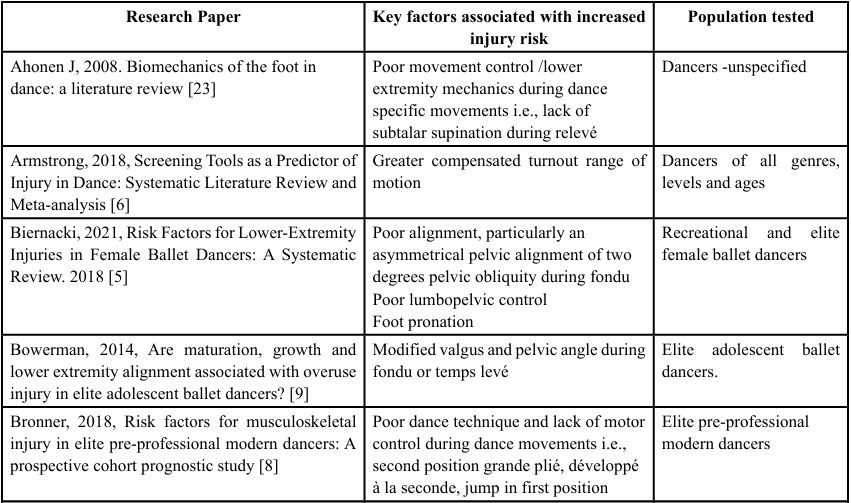
Table 1. Key Literature Review Findings Relating to Movement Competency and Injury Risk In Dancers
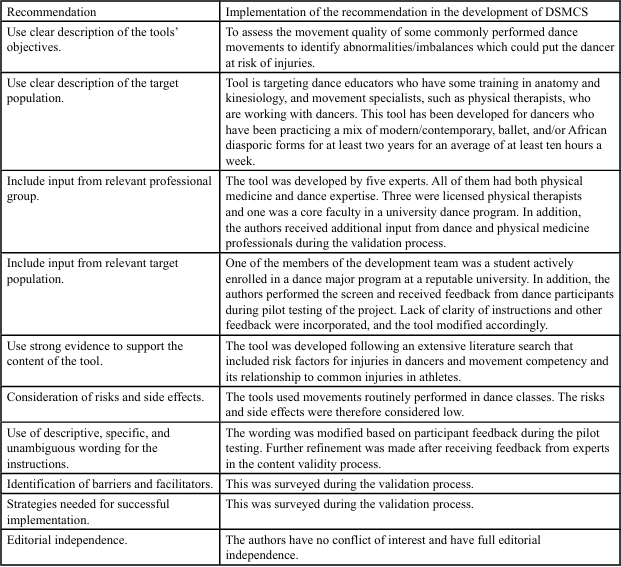
Table 2. Recommendations for Developing a High-Quality Movement Assessment Tool [11] and Their Implementation in the Development of the DSMCS
Assessment of Content Validity
Content validity refers to the degree to which an assessment instrument is relevant to, and representative of, the targeted construct it is designed to measure. The authors explored content validity by asking a convenience sample of 26 experts in physical therapy, movement science, and/or dance, to anonymously provide feedback on the DSMCS. Participants varied in their education, dance experience, professions, age, gender, and geographical location. Fifteen experts provided comprehensive responses to the questions listed in Table 3. The authors considered that the screen would have adequate content validity if questions one through three were answered with a “yes” at least 90% of the time. The rest of the questions were asked for future improvement of the tool’s efficacy, application, and relevance.

Table 3. Questions Used to Assess Content Validity
Assessment of Concurrent validity
Concurrent validity refers to the agreement between two measures taken at the same time or the comparison between a new assessment and one that has already been tested and proven to be valid. Concurrent validity of DSMCS was measured by comparing the outcome from the DSMCS to the Y Balance or Modified Star Excursion Balance Test (mSEBT). During the mSEBT, the subjects’ leg reach was measured in three directions representing a Y: anterior (ANT), posteromedial (PM) and posterolateral (PL), rather than the eight directions prescribed in the original Star Excursion Balance Test (SEBT). The mSEBT was suggested over the SEBT to save time and avoid redundancy [12]. The authors chose the mSEBT as the “gold standard” to measure concurrent validity because it evaluates skills deemed important for injury prevention such as balance, strength, neuromuscular control, and it has been used extensively as part of screening programs for both athletes and dancers. The mSEBT has excellent reliability [13], has the potential to predict injury occurrence in dancers [14] and is the only test shown to predict injuries in general athletes in two systematic reviews of clinician- friendly physical performance tests [15,16]. A fair-to-good correlation was expected between scores on the mSEBT and the scores on the DSMCS. Despite the mSEBT being one of the most accepted and useful functional screens for athletes, its reliability, usefulness, and predictive validity have not been thoroughly investigated in dancers of multiple genres. Also, the two tests do not assess the same constructs. The mSEBT does not include tasks in dance-specific positions such as jumping, movements in quadruped position, spinal articulations, and does not grade the quality of the movements. Nevertheless, higher scores indicate better balance, strength, and neuromuscular control, which are all important for better movement competency. Better movement competency should lead to better dance-specific movement competency and therefore higher scores on the DSMCS.
Prospective Participants were recruited via word of mouth and email. To be included, the dancers had to be at least 18 years of age, have participated in dance for a minimum of two years, been admitted to an undergraduate dance major at Wayne State University studying a mix of contemporary, modern, ballet, and dances of the African diaspora and dance a minimum of 12 hours per week as part of their program requirements. They could therefore be classified as advanced-level dancers. Exclusion criteria included dancers that had pain or injuries preventing them from participating fully in dance.
The DSMCS and mSEBT were administered as follows: one investigator not involved in the data collection instructed each task by reading the specific DSMCS and mSEBT task instructions verbatim (with occasional movement cues as needed) and two other investigators were each randomly assigned to an individual dancer to assess and score both the DSMCS and the mSEBT. To reduce risks of bias, evaluators utilized paper scoring sheets and were not able to see tabulated scores for either test during the evaluation period. After completion, scores were entered into a Microsoft Excel spreadsheet for calculations by a research team member not involved in the data collection.
The method used to perform the mSEBT is described by Stiffler [17]. Participants stood with the big toe of their test leg in the center of the “Y” and reached their test leg in the directions of the “Y” markings (anterior, posteromedial and posterolateral) for three trials. In the analysis, distance reached was normalized to the participant’s respective leg length. The composite score (average of the normalized reach scores for all three directions) was used for the analysis. Evaluators also scored movement quality of the ankle, knee, and spine on a three-point scale, zero being poor quality, one being fair, and two being good. All scores at each joint were added for a total score out of 36. Descriptive statistics were used for analysis of reach distances and Spearman correlation coefficients were used to calculate the correlation between the mSEBT and the DSMCS scores using SPSS statistical package version 29.0 (SPSS Inc, Chicago, IL, 2023). As per Portney and Watkins, correlations between 0.50 and 0.75 were considered moderate-to-good, and those above 0.75 were considered good-to-excellent [18]. The significance level was set as p<0.05.
Assessment of Interrater Reliability
Using the same recruitment tactics, qualifications, and exclusion criteria as the concurrent validity study, nine students participated in the assessment of reliability. In this study, only the DSMCS was performed. While performing the DSMCS, five evaluators independently scored each of the nine participants using the DSMCS rubrics. Evaluators included three physical therapists and two dance instructors. Each of the 22 DSMCS tasks was scored on a three-point scale (0–2) based on predefined criteria in the rubric, with borderline performances being scored according to the closest matching descriptor. Two of the evaluators had no prior knowledge of the DSMCS and received brief training, which included reviewing the scoring rubric and practicing with several live examples, followed by discussion to ensure consistent interpretation of the scoring criteria. An investigator blinded to the process entered all five evaluators’ scores into a Microsoft Excel spreadsheet. Reliability between raters was measured using intraclass correlation coefficient (ICC) estimates with a 95% confidence interval using SPSS statistical package version 29.0 (SPSS Inc, Chicago, IL, 2023). A two-way mixed-effects model based on mean ratings (ICC(3,k)) was used, as it is appropriate for a fixed set of raters and assesses the consistency of their ratings across different subjects.
Results
Content validity
Fifteen practicing professionals in physical therapy, movement science, and/or dance completed the content validity survey. Fifteen participants (100%) responded “yes” to questions one and two, agreeing that the movements selected were commonly performed in the practice of dance of multiple genres and were important to the overall screen. Fourteen out of 15 (93.3%) responded “yes” to question three agreeing that the items assessed movements that had the potential to increase injury risk (Table 4). This, along with the fact that the items were based on movement abnormalities identified in the literature, seems to indicate good content validity. Feedback received for questions 4-11 was analyzed and themed through qualitative analysis following methods described by Mainwaring [19]. Themes were divided into three domains for clarity and practical implementation for future versions of the DSMCS as indicated in
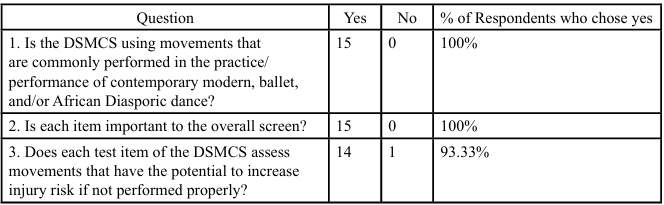
Table 4. Quantitative Results of Content Validity Survey
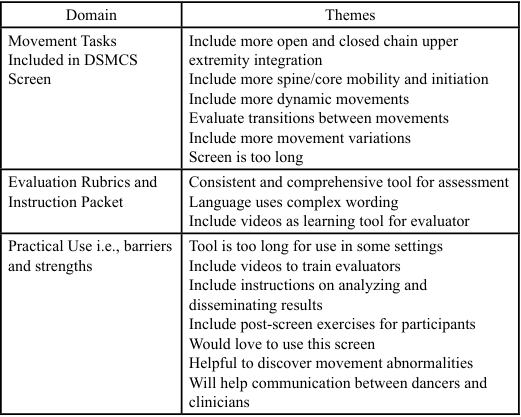
Table 5. Qualitative Results of Content Validity Survey
Concurrent validity study
Sixteen dance students pursuing either a Bachelor of Fine Arts or a Bachelor of Science in Dance participated in this study. Participants scored a mean of 92 on the DSMCS (range 59-113, SD 13.7) with a mean mSEBT composite score of 72.9 on the right (range 61.2-84.3, SD 7.6) and 73.2 on the left (range 61.2-84.5, SD 7.3). There was a statistically significant correlation of moderate strength between the DSMCS and mSEBT composite scores on the right and left side r=0.512 (p=0.031) and r=0.578 (p=0.015), respectively. The correlation between the DSMCS and the qualitative assessment on the mSEBT was r=0.753 (p<0.001).
Interrater Reliability
Nine collegiate dancers performed the screen and were each rated by five raters. The interrater reliability was 0.917 (confidence intervals (0.793 -0.979)) which is considered excellent.
Discussion
The first purpose of this manuscript was to describe the development of the DSMCS. The intention in creating the DSMCS was to add a dance-specific movement competency screen inclusive of multiple genres to already existing screening tools. The screen was developed by rehabilitation and dance experts using guidelines for the creation of high-quality movement assessment tools [11] and an extensive literature review.
DSMCS is unique and may offer several advantages over existing screen tools. Many existing tools focus on identifying impairments such as strength and mobility. While those elements are important, impairments do not always strongly correlate to function and/or injury risk [20]. Other tools such as mSEBT and the MCS provide a functional lens. While the mSEBT is a good predictor of lower extremity strength and movement competency, its usefulness in dance is uncertain. While being simple and quick to perform, mSEBT only gives a quantitative measure of lower body function while dance requires high quality compound movements involving multiple body regions. The MCS on the other hand is more functional and includes a variety of tasks such as squats, lunges, and push-ups; however, the movements are not dance-specific. While dance-specific screens have been used to predict injuries successfully, they often analyze only lower extremity movements that are derived from ballet [8-10].
The DSMCS is a multidimensional tool that examines key movements across multiple dance styles, such as knee flexion (plié) with spinal coordination, single-leg lifts (extensions), quadruped crawling, dynamic weight shifts, and jumping. It uses a variety of stances such as quadruped, parallel, turnout or wide second position, single or double leg stance, and assesses the influence of movement speed and cognitive load on movement execution. Specificity is important, and a systematic review of screening tools by Armstrong [6] shows that testing in dance-specific positions may have the greatest potential to predict injury risks. DSMCS uses movements that may expose neuromuscular deficiencies and compensatory techniques which have the potential to increase risks of injury: excessive knee valgus or midfoot pronation, compensated turnout, lack of lumbopelvic stability, and landing without sufficient knee flexion. (See Table 1). These motor control deficits, once identified, can be targeted through training and corrective strategies to reduce injury risk and enhance dance performance, making the DSMCS a practical tool for guiding individualized interventions [33].
Results from the pilot testing indicate the DSMCS may be valid and reliable for dancers training at least 10 hours a week for at least two years in multiple genres. Content validity was established using a synthesis of published evidence for movement-related injury risk factors in dancers and other athletes (Table 1). It was further investigated by surveying rehabilitation and dance experts who reported that the movements were specific and commonly performed by dancers of multiple genres, and relevant and important for screening for potential injury risk. An important and recurring tension point in the validity study and creation of the tool by the research team was the difference between screening for injury prevention and screening for aesthetic competency [21]. Sometimes sound and healthy movements may not align with traditional movement execution or educators’ and dancers’ perceptions about how a movement ‘should’ be accomplished. This theme emerged in the research team’s discussions and while reviewing the survey responses identified in Table 4.
The DSMCS demonstrated moderate-to-good concurrent validity with the mSEBT, and good-to-excellent validity when movement quality on the mSEBT was evaluated. Its interrater reliability was excellent, with consistent ratings across raters in both health and dance contexts, supporting its potential application in both fields.
Dance screens are important for identifying movement deficits that may increase injury risk, monitoring improvements, and evaluating readiness to return to dance following a pause or injury. The DSMCS offers practical applications across clinical, educational, and performance settings. Clinicians can use it to guide targeted rehabilitation and injury prevention programs, monitor recovery, and inform individualized exercise prescriptions. Dance educators may incorporate DSMCS results to tailor technique instruction, address faulty movement patterns, and track progress over a semester, year, or program. Performance coaches can use the tool to identify movement inefficiencies that may limit performance or increase injury risk, enabling early interventions to optimize technique and performance outcomes. By integrating the DSMCS with other screening tools and assessments, professionals gain a more comprehensive understanding of a dancer’s strengths, deficits, and risk factors. While the authors believe a movement competency screen might be most helpful, it does not eliminate the need for other robust screening tools, comprehensive assessments, and questionnaires which capture impairments and factors not tested in the DSMCS. A comprehensive screen may include history of previous injuries, menstrual irregularities, nutritional habits, body mass index, psychosocial factors, VO2max, strength, mobility (ROM), hypermobility scores, and more. While the DSMCS might be helpful to identify faulty movements, it is one tool in the toolbox of screens already available to the dance educators and health professionals.
Limitations and direction for future studies
As an exploratory study aimed at establishing preliminary normative data, reliability, and validity for the DSMCS, an a priori power analysis was not conducted. The sample sizes used are comparable to those reported in prior dance-specific screening tool studies, providing sufficient data to support initial evaluation of the tool’s psychometric properties. More testing on larger numbers is needed to establish stronger validity and reliability. No real gold standard for movement screen exists in dance medicine, making the measurement of concurrent validity difficult to assess. In addition, although blinded to previous scores, the same rater assessed both the DSMCS and mSEBT for an individual participant, which could have introduced some rater bias. Importantly, the population tested was a convenient sample of collegiate dancers and application to other dance populations is not known. In addition, the responsiveness of the tool needs to be established. A recent study published by Benoit Piau et al. [22] found that using a 5-level scoring system for the MCS showed greater internal consistency and concurrent validity in a dance population compared to the 3-level scoring system. It is not known if a 5-level scoring system for the DSMCS would be superior to the existing 3-level scoring system and how this may affect interrater reliability and clinical applicability.
At the time of the tool’s creation, limited evidence required researchers to work with experts and use data from other athletic/ dance populations to surmise injury risks for dance forms other than ballet and contemporary modern dance. A revised version might be required to better represent emerging data and trends. In addition, if a future revised version of the DSMCS is indeed needed, consideration will be given to the feedback received from the validity study (including more integration of the upper extremity, evaluating transitions between movements, and more dynamic movements) and will be weighed against the existing evidence and practical consideration (such as time and ease of administration). Future research could expand upon the current study by conducting longitudinal investigations to evaluate predictive validity over time, adapting the DSMCS for younger or less experienced dancers, and integrating the tool into dance curricula or injury prevention programs.
Conclusion and practical implications
With good-to-excellent validity and reliability, preliminary data indicate that the DSMCS shows strong potential for screening movement abnormalities in dancers and identifying patterns associated with increased injury risk. Importantly, it can be used by trained health professionals and dance educators to assess dancers across multiple genres, reflecting the diverse training typical of youth and collegiate programs. To the authors’ knowledge, the DSMCS is the only screening tool designed specifically for multi-genre dancers that incorporates speed-contingent tasks and tasks performed under added cognitive load. By providing objective, dance-specific movement assessments, the DSMCS has the potential to directly inform injury prevention strategies, optimize performance, and guide individualized training interventions, representing a meaningful advancement in dancer health and education.
Acknowledgements
We extend our thanks to Lisa McCabe, SPT, BS, and Riley Tiarks, BFA, BS and the Maggie Allesee Department of Theatre and Dance students for their participation.
Competing Interests:
The authors declare that they have no competing interests.
References
IBISWorld. Dance Schools Industry in the US - Market Research Report. Secondary Dance Schools Industry in the US - Market Research Report 12-19-2022 2022. View
IBISWorld. Dance Studios Industry in the US - Market Research Report. Secondary Dance Studios Industry in the US - Market Research Report 2023. View
Organization NDE. Colleges / Universities. Secondary Colleges /Universities 2023. View
van Winden, D., Van Rijn, R. M., Richardson, A., Savelsbergh, G. J. P., Oudejans, R. R. D., Stubbe, J. H., (2019). Detailed injury epidemiology in contemporary dance: a 1-year prospective study of 134 students. BMJ Open Sport Exerc Med; 5(1):e000453 View
Biernacki, J. L., Stracciolini, A., Fraser, J., Michel, L. J., Sugimoto, D., (2021). Risk Factors for Lower-Extremity Injuries in Female Ballet Dancers: A Systematic Review. Clin J Sport Med; 31(2):e64-e79 View
Armstrong, R., Relph, N. (2018). Screening Tools as a Predictor of Injury in Dance: Systematic Literature Review and Meta analysis. Sports Med Open; 4(1):33 View
Coogan, S. M., Schock, C. S., Hansen-Honeycutt, J., Caswell, S., Cortes, N., Ambegaonkar, J. P., (2020). Functional Movement Screen (Fms) Scores Do Not Predict Overall or Lower Extremity Injury Risk in Collegiate Dancers. Int J Sports Phys Ther;15(6):1029-35 View
Bronner, S., Bauer, N. G., (2018). Risk factors for musculoskeletal injury in elite pre-professional modern dancers: A prospective cohort prognostic study. Phys Ther Sport; 31:42 51 View
Bowerman, E., Whatman, C., Harris, N., Bradshaw, E., Karin, J., (2014). Are maturation, growth and lower extremity alignment associated with overuse injury in elite adolescent ballet dancers? Phys Ther Sport;15(4):234-41 View
Steinberg, N., Siev-Ner, I., Peleg, S., et al. (2012). Extrinsic and intrinsic risk factors associated with injuries in young dancers aged 8-16 years. J Sports Sci; 30(5):485-95 View
Bennett, H., Davison, K., Arnold, J., Slattery, F., Martin, M., Norton, K., (2017). Multicomponent Musculoskeletal Movement Assessment Tools: A Systematic Review and Critical Appraisal of Their Development and Applicability to Professional Practice. J Strength Cond Res; 31(10):2903-19 View
Picot, B., Terrier, R., Forestier, N., Fourchet, F., McKeon, P., (2021). The Star Excursion Balance Test: An Update Review and Practical Guidelines. International Journal of Athletic Therapy & Training; 26. View
Powden, C. J., Dodds, T. K., Gabriel, E. H., (2019). The Reliability of the Star Excursion Balance Test and Lower Quarter Y-Balance Test in Healthy Adults: A Systematic Review. Int J Sports Phys Ther; 14(5):683-94 View
Sekulic, D., Prus, D., Zevrnja, A., Peric, M., Zaletel, P., (2020). Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children (Basel); 7(12) View
Hegedus, E. J., McDonough, S. M., Bleakley, C., Baxter, D., Cook, C. E., (2015). Clinician-friendly lower extremity physical performance tests in athletes: a systematic review of measurement properties and correlation with injury. Part 2- the tests for the hip, thigh, foot and ankle including the star excursion balance test. Br J Sports Med; 49(10):649-56 View
Vogler, J. H., Csiernik, A. J., Yorgey, M. K., Harrison, J. J., Games, K. E., (2017). Clinician-Friendly Physical Performance Tests for the Hip, Ankle, and Foot. J Athl Train; 52(9):861-62 View
Stiffler, M. R., Sanfilippo, J. L., Brooks, M. A., Heiderscheit, B. C., (2015). Star Excursion Balance Test Performance Varies by Sport in Healthy Division I Collegiate Athletes. J Orthop Sports Phys Ther; 45(10):772-80 View
Portney, L. G., (2015). WM. Foundations of CLinical Research. Applications to practice. Philadelphia, PA: McGraw Hill. View
Welsh, T., Ambegaonkar, J. P., Mainwaring, L., (2023). Research methods in the dance sciences. Gainesville: University Press of Florida. View
Skallerud, A., Brumbaugh, A., Fudalla, S., Parker, T., Robertson, K., Pepin, M. E., (2022). Comparing Lumbar Lordosis in Functional Dance Positions in Collegiate Dancers With and Without Low Back Pain. J Dance Med Sci; 26(3):191-201 View
Angioi, M., Metsios, G. S., Twitchett, E., Koutedakis, Y., Wyon, M., (2009). Association between Selected Physical Fitness Parameters and Aesthetic Competence in Contemporary Dancers. Journal of Dance Medicine & Science;13(4):115-23 View
Benoit-Piau, J., Morin, M., Guptill, C., Fortin, S., Gaudreault, N., (2022). Movement Competency Screen: Rethinking the Rating. Int J Sports Phys Ther;17(7):1282-89 View
Ahonen, J., (2008). Biomechanics of the foot in dance: a literature review. J Dance Med Sci;12(3):99-108 View
Campbell, R. S., Lehr, M. E., Livingston, A., McCurdy, M., Ware, J. K., (2019). Intrinsic modifiable risk factors in ballet dancers: Applying evidence based practice principles to enhance clinical applications. Phys Ther Sport; 38:106-14 View
De Bleecker, C., Vermeulen, S., De Blaiser, C., Willems, T., De Ridder, R., Roosen, P., (2020). Relationship Between Jump Landing Kinematics and Lower Extremity Overuse Injuries in Physically Active Populations: A Systematic Review and Meta Analysis. Sports Med; 50(8):1515-32 View
Kaufmann, J. E., Nelissen, R., Exner-Grave, E., Gademan, M. G. J., (2021). Does forced or compensated turnout lead to musculoskeletal injuries in dancers? A systematic review on the complexity of causes. J Biomech;114:110084 View
Kenny, S. J., Whittaker, J. L., Emery, C. A., (2016). Risk factors for musculoskeletal injury in preprofessional dancers: a systematic review. Br J Sports Med; 50(16):997-1003 View
Roussel, N. A., Nijs, J., Mottram, S., Van Moorsel, A., Truijen, S., Stassijns, G., (2009). Altered lumbopelvic movement control but not generalized joint hypermobility is associated with increased injury in dancers. A prospective study. Man Ther; 14(6):630-5 View
Watson, M. D., Lasner, A. N., Hada, N., (2025). A Review of Musculoskeletal Dance Screening Tests in Collegiate Dancers: A Ten-Year Retrospective Study. J Dance Med Sci. Aug 13:1089313X251358325. View
Schultz, K., Sun Worrall, K., Tawa, Z., Binney, J., Boyle, J., Abbruzzese, L. D., (2024). Development and Feasibility of an Adolescent Dancer Screen. Int J Sports Phys Ther. Mar 2;19(3):301-315. View
Callahan, E., Mangum, L. C., (2024). The Movement Competency Screen Shows Improved Injury Predictive Ability Compared With the Functional Movement Screen in Ballet and Contemporary Dance Populations: A Critically Appraised Topic. J Sport Rehabil. Dec 10;34(4):456-462. View
Pepin, M. E., Prieur, V., Skallerud, A., (2025). Investigating the Complex Relationship Between Movement Competency Scores, Hip Mobility, Strength, and Turnout Measures in Collegiate Dancers. J Dance Med Sci. Aug 9:1089313X251357651. View
Zhang, M., Ma, H., Liu, Z., Smith, D. M., Wang, X., (2021). The Effects of a 10-Week Neuromuscular Training on Postural Control in Elite Youth Competitive Ballroom Dancers: A Randomized Controlled Trial. Front Physiol. Mar 25;12:636209. View