
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 7 (2026), Article ID: JRPR-196
https://doi.org/10.33790/jrpr1100196Case Report
Body Awareness as a Missing Link in Fall Prevention: An Occupational Therapy Case Study
Brigitte Belanger*, DSc, OTR/L, C-AAIS, Paul Arthur, PhD, OTR/L, and Ahmed Elokda, PT, PhD, FAACVPR
Department of Occupational Therapy Program, Florida Gulf Coast University, 10501 FGCU Blvd, Fort Myers, FL 33965, United States.
Corresponding Author Details: Brigitte Belanger, DSc, OTR/L, C-AAIS, Associate Professor, Department of Occupational Therapy Program, Florida Gulf Coast University, 10501 FGCU Blvd, Fort Myers, FL 33965, United States.
Received date: 11th November, 2025
Accepted date: 29th January, 2026
Published date: 31st January, 2026
Citation: Belanger, B., Arthur, P., & Elokda, A., (2026). Body Awareness as a Missing Link in Fall Prevention: An Occupational Therapy Case Study. J Rehab Pract Res, 7(1):196.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Falls represent a major risk for older adults, often resulting in injury, decreased independence, and increased healthcare utilization. Traditional fall-prevention programs primarily focus on environmental modification and strengthening, with limited attention to body awareness and the role of proprioception. This single-case study explored whether a six-week occupational therapy intervention emphasizing body awareness could improve balance, confidence, and functional performance in an older adult with fear of falling. The intervention protocol included body brushing followed by repetitive body-awareness and balance exercises incorporating visual and tactile feedback to strengthen sensory–motor integration [1]. Evidence suggests proprioceptive and body-awareness–based interventions enhance neuromuscular activation and balance performance [2,3], while specific repetitive neurokinetic exercise has been shown to improve core endurance, pelvic alignment, and flexibility supporting retraining of neuromuscular control and proprioceptive efficiency [4]. Preliminary findings from this project indicate that integrating body-awareness strategies into OT fall-prevention improved performance across all fall-related assessments and increased client self-perceived performance and confidence, suggesting potential to improve movement confidence and balance-related performance.
Keywords: Body Awareness; Proprioception; Fall Prevention; Occupational Therapy; Older Adults; Balance; Sensorimotor Training
Introduction
Falls among older adults commonly result in fractures, traumatic brain injury, hospitalization, and substantial declines in quality of life. They also create a major financial burden, with national costs projected to exceed $101 billion annually by 2030 [5-7]. Falls are also a significant public health issue and remain a leading cause of injury-related morbidity and mortality worldwide. The World Health Organization [8] identifies falls as the second leading cause of unintentional injury death globally, with an estimated 684,000 fatal falls annually, and reports that 37.3 million falls each year are severe enough to require medical attention [8]. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that over 14 million adults aged 65 years and older (approximately 1 in 4) experience a fall each year, underscoring the urgency of effective and scalable prevention strategies [9].
Globally, fall prevention strategies emphasize multifactorial approaches that address physical function, environmental hazards, and individualized risk factors through community and health-system level interventions [8,10]. Conventional fall-prevention approaches similarly prioritize environmental modifications, strengthening, and balance training; however, comparatively little attention has been directed toward body awareness and postural regulation in aging as a modifiable factor influencing fall risk [11,12].
Body awareness including proprioception, kinesthesia, and perceptual integration is foundational to postural control and occupational performance. As Suetterlin and Sayer [13] note, “The awareness of body segments in space is crucial for the organism to communicate effectively with the environment.” Age-related reductions in proprioceptive acuity and balance further contribute to fall risk [14]. Despite this relevance, commonly used fall-risk assessments such as the Berg Balance Scale [15] and the Functional Reach Test [16] do not adequately capture proprioceptive or body-awareness components. Current balance tests may not isolate proprioceptive processing or sensory components underlying balance control [17,18]. This assessment gap may limit the identification and targeted rehabilitation of sensory-motor contributors to instability and fear of falling.
Emerging rehabilitation approaches that emphasize the brain–body connection may offer a promising direction for fall prevention by combining sensory feedback with precise, intentional movement to retrain neuromuscular activation and enhance proprioceptive processing. Although Neurokinetic Therapy (NKT) has limited evidence as a distinct branded intervention, its underlying principles align with broader evidence-supported rehabilitation approaches, including sensorimotor training, neuromuscular re-education, proprioceptive training, motor control retraining, and body awareness–based interventions. Therefore, the present intervention is described as drawing from principles consistent with NKT while being grounded in the larger body of literature supporting proprioceptive and sensorimotor exercise for balance improvement. Notably, a recent systematic review and meta-analysis by Sluga and Kozinc [19] demonstrated that sensorimotor/proprioceptive exercise can improve balance outcomes in older adults, supporting the theoretical foundation of this approach.
This single-case study investigated the effects of a neurokinetic, body-awareness–focused occupational therapy protocol on balance, confidence, and functional performance in an older adult with fear of falling.
Study Design and Recruitment
This single-case design was approved by the institutional review board (2022-101). Single-case and case study designs are appropriate for early-stage evaluation of novel clinical protocols, particularly when outcomes are individualized and context-sensitive [20,21]. Reporting follows recommended guidance for single-case experimental design description and transparency, including clear participant characteristics, repeated measurement at defined timepoints, and detailed intervention procedures to support replication.
Reporting was informed by recommended guidance for transparency in single-case experimental design methods, including clear participant description, defined timepoints, and detailed intervention procedures to support replication [22].
One 74 year old male who met inclusion criteria (fear of falling, ability to participate in six sessions, English proficiency, and functional mobility adequate for exercises) was referred by a local occupational therapy provider. The participant signed the consent document and completed a baseline evaluation which was followed by six weekly, one-hour sessions and a discharge re-evaluation.
Interventions
Each session began with a 6 minute sensory brushing protocol (Appendix A) to increase tactile awareness of targeted body regions. Brushing provides afferent tactile input via cutaneous mechanoreceptors through peripheral nerves to the central nervous system and may influence somatosensory processing and autonomic arousal. For this participant, brushing was used as a preparatory strategy to support attention and movement readiness through modulation of arousal and enhanced sensory awareness [23]. This preparatory sensory strategy was not intended as a fall-prevention intervention in isolation but rather as a means of enhancing somatosensory attention and readiness for movement-based training.
Following brushing, the participant completed body-awareness and balance activities using mirror-based visual feedback to support postural self-monitoring. Exercises were delivered in a structured format using repetitive movement sequences designed to promote functional movement patterns and neuromuscular co-activation. Intervention activities emphasized slow, deliberate, and controlled movement with guided feedback to support improved awareness of body position and movement execution.
Specific exercises included toe activation tasks, controlled heel raises, and sit-to-stand practice to target foundational lower-extremity activation and transitional movement control. Static and dynamic balance activities were incorporated to address postural sway and to progressively challenge postural stability [24]. Progression was based on observed performance and tolerance, with exercises advanced by increasing postural demands, balance challenge, and dual-system engagement (e.g., combining controlled movement with simultaneous perceptual feedback).
As performance improved, simulated activities of daily living (ADLs) were integrated to facilitate transfer of skills into functional contexts. These occupation-based tasks incorporated intentional movement sequencing, postural transitions, and controlled weight shifting. Tasks included reaching into a cabinet while maintaining tripod foot pressure, carrying a laundry basket while weight shifting, hair brushing in standing to promote symmetrical weight bearing and trunk rotation, and lower-body dressing (donning shoes and socks) in seated preparation for standing transitions. Throughout all sessions, the participant was closely monitored to ensure safe body mechanics, postural control, and appropriate use of feedback (see Appendix B for intervention details).
Tool selection rationale:
The Canadian Occupational Performance Measure (COPM) was selected to capture client-identified occupational performance problems impacted by fall risk and to quantify perceived changes in performance and satisfaction following intervention. Because fall risk often leads to activity restriction and reduced confidence, the COPM provides a client-centered measure of functional change and self-perceived ability in real-life daily activities beyond standardized balance testing. The COPM is also sensitive to clinically meaningful change over time, supporting evaluation of intervention effectiveness in outcomes that are directly relevant to participants.
The Berg Balance Scale (BBS) was used as a standardized measure of functional balance across common mobility tasks (e.g., transfers, reaching, turning). It is widely used in older adult and fall-prevention research and provides an objective indicator of static and dynamic balance performance, helping quantify change following intervention [15].
The Functional Reach Test (FRT) was selected to assess limits of stability and anticipatory postural control during forward reaching. This test captures the ability to maintain balance while performing a functional task that commonly contributes to falls (e.g., reaching for objects), making it a clinically relevant measure of fall risk and intervention responsiveness [16,25].
The 4-Stage Balance Test was included as a brief, practical screen of static balance control across progressively challenging foot positions. It helps identify balance impairment related to fall risk with minimal equipment and time, supporting efficient baseline screening and post-intervention comparison [26].
The Thumb Localization Test was used to evaluate proprioception/ body awareness, specifically the ability to perceive limb position without visual input. Because the intervention targets sensory–motor integration and body-awareness strategies, this measure provides an objective indicator of changes in proprioceptive processing, which is strongly linked to postural control and balance regulation [27].
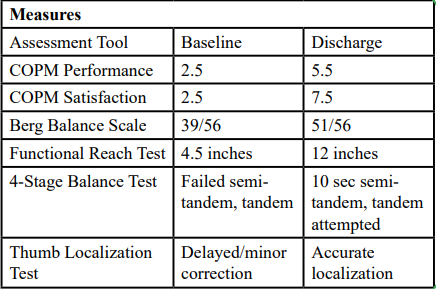
Table 1
Results
The participant demonstrated measurable improvements in balance, body awareness, and perceived performance. BBS scores improved by 12 points, exceeding the minimal detectable change threshold of 6.5 points [28]. Functional Reach increased by 7.5 inches, indicating significant fall risk reduction. COPM scores showed substantial gains in both performance and satisfaction. Observational measures revealed improved weight shifting, toe engagement, and decreased compensatory postures.
In addition to standardized outcomes, clinical observation during task-based sessions reflected visible movement-quality changes, including improved symmetry and control during functional transitions, more consistent weight shifting onto the affected/less dominant side, and increased ability to initiate and sustain heel-to-toe engagement without external cueing. The participant demonstrated enhanced postural alignment with fewer compensatory strategies (e.g., reduced trunk rigidity, less lateral trunk lean, and decreased reliance on hip hiking or upper-extremity bracing). During balance challenges and functional reaching tasks, the participant displayed more efficient anticipatory postural adjustments, improved righting reactions, and reduced fear-based guarding behaviors. The participant also appeared increasingly able to self-correct posture and movement patterns, indicating improved proprioceptive awareness and internal feedback processing.
Importantly, the participant reported no falls during the six-week treatment period, further supporting functional carryover and potential real-world safety benefit.
Discussion
The participant’s performance improvements over time, observed during repeated and mindful movement practice, support the premise that experience-dependent neuroplasticity may enhance sensory processing efficiency and facilitate more coordinated motor responses [29].
Similarly, repetitive motor learning strengthens the integration between sensory input and motor output, contributing to improved movement efficiency and postural control [1]. Consistent with these mechanisms, emerging evidence suggests that proprioception and body awareness–based interventions are associated with improved neuromuscular activation and balance performance [2,3].
The participant’s improvements are consistent with occupational therapy frameworks such as the Person–Environment–Occupation (PEO) model and the Occupational Therapy Practice Framework (OTPF), which emphasize the dynamic interaction of physical, psychological, and contextual factors influencing occupational performance. Although direct evidence evaluating body awareness outcomes within NeuroKinetic Therapy (NKT) remains limited, emerging studies indicate that neurokinetic approaches can enhance neuromuscular function and movement quality. Moreover, the broader literature on proprioceptive and body awareness–focused interventions supports improvements in sensorimotor performance, providing rationale for integrating neurokinetic principles to strengthen body awareness and potentially reduce fall risk [1-4]. Taken together, this case study provides preliminary support for a neurokinetic, body-awareness–based occupational therapy approach that pairs targeted sensorimotor exercises with occupation-based functional tasks as a feasible fall-prevention strategy.
Limitations
While the findings support incorporating body-awareness– focused intervention strategies with neurokinetic principles into occupational therapy, several limitations should be acknowledged. The intervention protocol is not standardized, which may lead to variability in how interventions are delivered; thus, future research should establish consistent procedures to improve reproducibility. The single-case design further limits internal validity and prevents causal inference, as there was no control or comparison condition. It is also possible that the Hawthorne Effect was in place with frequent client-therapist interaction. As fall history data were anecdotal, this reduces the ability to contextualize baseline functional risk. Findings should be interpreted with caution and cannot be generalized without replication in large, more diverse samples.
Conclusion
Preliminary findings suggest that a holistic body awareness approach to fall prevention may enhance confidence and reduce fall risk in older adults. This perspective may broaden occupational therapy practice by targeting proprioceptive and perceptual dimensions that are often underemphasized in conventional programs.
Future Direction
Although early in nature, these findings support continued investigation of age-related changes in proprioceptive processing and postural control to inform the development of sensitive measurement tools and individualized, responsive interventions.
Competing Interests:
The authors declare that they have no competing interests.
Acknowledgment:
The authors would like to express sincere appreciation to Carly Rimes, OTR/L, for her passion, dedication, and continued efforts to provide clinical training and mentorship in body awareness and sensorimotor rehabilitation. And to Olivia Weeks, OTR/L whose contributions and support were valuable throughout this project and whose continued professional development alongside Carly exemplifies the mentorship and clinical excellence we strive to cultivate in occupational therapy. As an educator, few experiences are more meaningful than witnessing a former student not only excel in practice, but forge her own path advancing the profession through innovation, leadership, and service.
References
Cardile, D., Lo Buono, V., Corallo, F., Quartarone, A., & Calabrò, R. S. (2025). A scoping review on the body awareness rehabilitation after stroke: Are we aware of what we are unaware? Frontiers in Neurology, 15, Article 1497052. View
Prajan, P. S., Abathsagayam, K., & Vishnuram, S. (2024). Effectiveness of neurokinetic therapy on pain and plantar fascia thickness among patients with plantar fasciitis. Journal of the Foot & Ankle, 18(2), 222-226. View
Winter, L., Huang, Q., Sertic, J. V. L., & Konczak, J. (2022). The Effectiveness of Proprioceptive training for improving motor performance and motor dysfunction: A systematic review. Frontiers in Rehabilitation Sciences, 3. View
Sulaiman, M. L., Mohanan, K., Kandaswami, K., & Nagaraj, D. (2024). Exploring Neurokinetic Therapy on core muscle endurance, lateral pelvic tilt, and quadratus lumborum flexibility for subjects with chronic non-specific low back pain. Muscles, Ligaments and Tendons Journal, 14(4), 614–622. View
Elliott, S., & Leland, N. E. (2018). Occupational therapy fall prevention interventions for community-dwelling older adults: A systematic review. American Journal of Occupational Therapy, 72(4), 1–11. View
Haddad, Y. K., Bergen, G., & Florence, C. S. (2019). Estimating the economic burden related to older adult falls by state. Journal of Public Health Management and Practice, 25(2), E17–E24. View
National Council on Aging. (2023, March 13). Get the facts on falls prevention. View
World Health Organization. (2021). Step safely: Strategies for preventing and managing falls across the life-course. World Health Organization. View
Centers for Disease Control and Prevention. (2024, May 9). Facts about falls. View
Montero-Odasso, M., van der Velde, N., Martin, F. C., Petrovic, M., Tan, M. P., Ryg, J., Aguilar-Navarro, S., Alexander, N. B., Becker, C., Blain, H., Bourke, R., Cameron, I. D., Camicioli, R., Clemson, L., Close, J., Delbaere, K., Duan, L., Duque, G., Dyer, S. M., Freiberger, E., … Task Force on Global Guidelines for Falls in Older Adults (2022). World guidelines for falls prevention and management for older adults: a global initiative. Age and ageing, 51(9), afac205. View
Ahn, S. N. (2018). Differences in body awareness and its effects on balance function and independence in activities of daily living for stroke. Journal of Physical Therapy Science, 30(11), 1386–1389. View
Sarican, Y., Erdoğanoğlu, Y., & Pepe, M. (2023). The effect of body awareness on trunk control, affected upper extremity function, balance, fear of falling, functional level, and level of independence in patients with stroke. Topics in Stroke Rehabilitation, 30(3), 1–10. View
Suetterlin, K.J., & Sayer, A.A. (2014). Proprioception: where are we now? A commentary on clinical assessment, changes across the life course, functional implications and future interventions. Age Ageing, 43(3):313-318. View
Ferlinc, A. Fabiani, E, Velnar, T. (2019). The importance and role of proprioception in the elderly: A short review. Materia Socio-Medica, 31(3), 2019-221. View
Berg, K. O., Wood-Dauphinee, S. L., Williams, J. I., & Maki, B. (1992). Measuring balance in the elderly: Validation of an instrument. Canadian Journal of Public Health, 83(Suppl 2), S7–S11. View
Duncan, P. W., Weiner, D. K., Chandler, J., & Studenski, S. (1990). Functional reach: A new clinical measure of balance. Journal of Gerontology, 45(6), M192–M197. View
Koelewijn, A. D., Selverian, S., Testa, M., & van der Kooij, H. (2020). Exploring the contribution of proprioceptive reflexes to balance control in perturbed standing. Frontiers in Bioengineering and Biotechnology, 8, 866. View
Labanca, L., Rocchi, J. E., Arcangeli, V., & Santilli, V. (2021). Balance and proprioception impairment, assessment tools, and rehabilitation training after total hip arthroplasty: A comprehensive review. International Journal of Environmental Research and Public Health, 18(9), 4786. View
Pšeničnik Sluga, S., & Kozinc, Ž. (2024). Sensorimotor and proprioceptive exercise programs to improve balance in older adults: A systematic review with meta-analysis. European Journal of Translational Myology, 34(1), 12010. View
Yin, R. K. (2018). Case study research and applications: Design and methods (6th ed.). SAGE Publications. View
Kazdin, A.E. (2011). Single-case research designs: Methods for clinical and applied settings (2nd ed.). Oxford University Press. View
Tate, R. L., Perdices, M., Rosenkoetter, U., Wakim, D., Godbee, K., Togher, L., McDonald, S., & Vohra, S. (2016). The Single-Case Reporting guideline In Behavioural interventions (SCRIBE) 2016 statement. Archives of Scientific Psychology, 4(1), 1–9. View
Owens, D. M., Lumpkin, E. A., & Patapoutian, A. (2014). Diversification and specialization of touch receptors in skin. Nature Reviews Neuroscience, 15(3), 175–186. View
Munoz-Martel, M. A., Espinosa, C. A., Romero-Franco, N., & Cardona, G. A. (2022). Impact of age on the postural stability measured by a virtual reality tracker-based posturography and a pressure platform system. BMC Geriatrics, 22, 506.
Duncan PW, Studenski S, Chandler J, Prescott B. (1992). Functional reach: Predictive validity in a sample of elderly male veterans. Journal of Gerontology, 47(3):M93-8. View
Centers for Disease Control and Prevention & National Center for Injury Prevention and Control. (2017). 4-Stage Balance Test. View
Otaka E, Otaka Y, Kasuga S, Nishimoto A, Yamazaki K, Kawakami M, Ushiba J, Liu M. (2020). Reliability of the thumb localizing test and its validity against quantitative measures with a robotic device in patients with hemiparetic stroke. PLoS One, 15(7):e0236437. View
Downs, S. (2015). The Berg Balance Scale. Journal of Physiotherapy, 61(1), 46. View
Marzola, P., Melzer, T., Pavesi, E., Gil-Mohapel, J., & Brocardo, P. S. (2023). Exploring the role of neuroplasticity in development, aging, and neurodegeneration. Brain Sciences, 13(12), Article 1610. View