
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 7 (2026), Article ID: JRPR-200
https://doi.org/10.33790/jrpr1100200Expert Opinion
Wait Training: Reconditioning the Power of Impulse Control
Mike Studer, PT, DPT, MHS, NCS, CEEAA, CWT, CSST, CSRP, CBFP, FAPTA
Adjunct Professor, Touro University Las Vegas, Las Vegas, 4505 S. Maryland Pkwy, NV, 89154, United States.
Corresponding Author Details: Mike Studer, PT, DPT, MHS, NCS, CEEAA, CWT, CSST, CSRP, CBFP, FAPTA, Adjunct Professor, Touro University Las Vegas, Las Vegas, 4505 S. Maryland Pkwy, NV, 89154, United States.
Received date: 23rd February, 2026
Accepted date: 31st March, 2026
Published date: 02nd April, 2026
Citation: Studer, M., (2026). Wait Training: Reconditioning the Power of Impulse Control. J Rehab Pract Res, 7(1):200.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Most health care professionals and laypersons are familiar with the behavior known as “impulsive”. Clinically, the capacity or skill to inhibit actions that are inappropriate, or illegal is known as impulse control (IC). In social and clinical contexts, it can be rather easy to identify impulsive behaviors when we see them. Clinically, patients undergoing rehabilitation with acute to sub-acutely impaired IC are at higher fall risk, more likely to become agitated, and may be verbally or physically abusive to providers or caregivers. In addition, these patients can be more challenged to safely re-integrate for tasks such as driving and vocation. Science has helped us to understand the areas of the nervous system that play a role in IC. Psychiatric medicine and psychology have advanced in their identification and treatment of many of the primary behaviors emerging from impaired IC including various forms of addiction and compulsions. Rehabilitation of IC after neurologic injury is not nearly as advanced. The entire field of Physical Medicine and Rehabilitation would benefit from an improved understanding of these topics, to be covered in this paper: prodromal indications of poor impulse control; improving the accuracy of detailing and predicting care needs; the functional relationships between IC and other cognitive skills; testing IC; and finally, a novel framework and direction for rehabilitating IC.
Recent History and Present Understanding of Impulse Control
To begin, it is important to define impulse control and to identify the terms that are largely synonymous. Impulse control can be referred to by any of the following terms in the scientific literature: self-governance, self-control, self-restraint, self-regulation, or even sobriquet conscientiousness [1].
In their 2023 article entitled, “Impulse Control Disorders”, Fariba & Gokarakonda write, “Self-regulation arises from the existence of a conflict between two mutually exclusive inner psychic agencies, or more descriptively in Freudian terminology, between the impulsive id and the captious superego. One can either eat the cake, or not eat the cake, however, one cannot, both eat the cake and, at the same time, not eat the cake. Freud postulated that socialization was a process by which juveniles appreciated how best to suppress immediately satisfying urges, and instead consider what might be most beneficial for one's future self [2].”
Is impulse control a higher-order capacity, differentiating humans from all other lifeforms? This stance is both controversial and debatable, if not unanswerable, yet in the aforementioned article (2023), Fariba and Gokarakonda wrote, “Impulsivity is a trait ubiquitous with human nature. What separates humans from life forms of lower sentience is the evolution of neurocircuitry within the prefrontal cortex that allows one to practice self-governance [2].” Most certainly these would be some highly controversial claims that could be countered by those who have studied primates such as Jane Goodall, Robert Sapolsky and many others who write about actions consistent with impulse control and self-restraint that they have witnessed and documented in chimpanzees and baboons respectively.
Perhaps the best place to start when describing the evolution and our recent timeline for our understanding of impulse control should start on September 13th, 1848, when 25 year old Phineas Gage was accidentally impaled by his 3 foot 7” tamping iron. This bar, weighing 13# went through Gage’s left eye socket, through the frontal lobe of his brain, and landed some 30 feet away. Gage survived the trauma, remained awake throughout, walking nearly 1 mile for health care [3]. Accounts of Phineas Gage after the injury reflect a significant change in personality from businesslike and efficient to erratic and explosive. These changes helped to advance the localizationist movement of neuroscience. Specifically informing us that Gage’s “behavior center” was impaired by the accident.
Phineas Gage went on to recover some function, moved to Chile, and was even employed as a driver some 4 years after the accident [3]. Could we have helped him recover his social skills and reduce his loss of impulse control better today, nearly 200 years later?
In the late 1960s, Stanford psychologist Dr. Walter Mischel advanced our understanding of self-control under the presence of a temptation. Mischel’s work, often referred to as “the Marshmallow Test” was directed at self or impulse-control [4]. Mischel felt that the ability to control one’s impulses would be predictive of their success in later schooling and in life. The first of three studies, published in 1970, included 50 preschoolers that were evenly distributed across five conditions. Three of the groups were tempted to wait 15 minutes to eat their choice of a favorite snack, a marshmallow or pretzel. The methodology included various conditions of reward, a physical distraction (slinky), mental distraction (thinking of “something fun”), and two groups of “no instructions”.
Subsequent studies including different instructions and methodologies were conducted through 1974. In 1990, Mischel and two colleagues from Columbia University began to perform a longitudinal analysis. Suffice to say that between Mischel’s later work and that of others’ analyzing the data with the performance (SAT and other) of these now young adults found that those preschoolers who were better able to delay gratification had statistically higher SAT scores [4]. Also in 1990, those students that had been identified as having superior delayed gratification were now rated more highly by their parents on scales of self-worth, self-esteem, and the capacity to cope with stress during adulthood than the subjects who were less able to delay gratification earlier in life.
While these were not the only advances in impulse control, through them, what had we learned? That some of our behavior (self-control or impulse control) could be localized to the frontal lobe? Yes. That these skills appear to develop with normal maturation? Yes. That early mastery might have some correlation with later performance on tests of intellectual and emotional intelligence? Yes.
Where is impulse control “located”?
As with most cognitive functions, we now understand that it is entirely too reductionist to label one brain area as being wholly responsible for a function. The fear center, the reward nuclei, centers for attention, and anxiety, our attempts to oversimplify and “blame” an area is outdated, yet the list of “localized” centers, continues to be used. The functions listed above are not “located” in a place. They are reliant upon a network of activity that are likely never the same twice. Because impulse control must consider sensory processing, encoding, and consolidation of past experiences, then combine the perception of these lived experiences with current context (perception of the environment and situation) – every decision about impulse control is new, each time. We have recency bias that can be prioritized and influences our decision in the here and now. Information about the last time/repetition or exposure includes the temptation (reward), consequences (risk), as well as likelihood. Consider your driving behavior, videogaming, athletic endeavors, courtship decisions and social media tendencies. None of these are located in one place and all decisions include a degree of past with present. Actions that are permitted and those that must be inhibited are never static or fixed, meaning a large portion of the brain is being used. With this list alone we must utilize information from the hippocampus, corpus callosum, insula, prefrontal cortex (both dorsolateral and ventromedial), thalamus, anterior cingulate cortex, parieto-occipital lobes, nucleus accumbens and the amygdala.5 Generally speaking, persons with lesions in the prefrontal cortex are more likely to have impaired impulse control (IC).
Both the right and left hemispheres have roles in IC. The difference between injuries to the right or left hemisphere are most notable in the prefrontal cortices, anterior cingulate, and inferior frontal gyrus. The left dorsolateral prefrontal cortex (DLPFC) appears to have social behavior responsibilities (conversational appropriateness and related) while the right inferior frontal gyrus may be an efficient brake with motor behaviors required for sports, driving, and many of the fast-moving games that one might play with cards or spoons on a table.
In the field of rehabilitation, the acute loss of impulse control can be a presentation expected with some persons after stroke, brain injury, and those with Multiple Sclerosis or even Parkinson’s Disease. The post stroke syndrome known as Right Hemisphere Dysfunction (RHD) is defined by signs of neglect or hemi-inattention, impulsiveness and anosognosia [6]. RHD is most commonly associated with lesions of the frontoparietal network. Notably, RHD includes lesions in the frontal lobe projections that interconnect attention and behavioral networks. These same structures can be implicated in persons with MS or after brain injury with impaired impulse control.
In contrast, the pathophysiology of impaired impulse control in persons with Parkinson’s Disease (PwPD) is often altogether different. PwPD may have limitations as a function of the dynamics of low endogenous dopamine (DA), leading to more extreme thrill- seeking behaviors to produce or compensate for the paucity of DA production [7]. It is well-documented that some PwPD experience an iatrogenic complication of DA replacement therapy resulting in compulsive behaviors including binge eating, hypersexuality, pathological gambling, and uncharacteristic shopping [8-10].
Here ends one call to action regarding impulse control. To the scientists looking for an as yet untapped function to understand in mental health and rehabilitation – this is it. From this point, the article will remain largely focused on advancing our understanding of and rehabilitation for acquired neurologic insults leading to reduced impulse control. As such, it is beyond the scope of this article to perform either a comprehensive review of the anatomy of IC or even a cursory review of the iatrogenic (largely dopamine replacement therapy), congenital and developmental pathophysiologies leading to impaired IC.
Readers are again directed to the work of Probst & van Eimeren (2013) to explore anatomy and pathophysiology of congenital and developmental disorders of IC [5].
Fariba and Gokarakonda offered a particularly compelling description of two theories about the neurochemical nature of impulse control disorders in development, citing the reward deficiency hypothesis [11,12], as well as the sensitization theory [13].
Again, readers are directed to the aforementioned Probst (2013) article as a primary source for more explorations relevant to reduced impulse control in adolescents presenting with obsessive compulsive disorders, substance abuse disorders, and even some related hyperactivity disorders. While the commonalities of the inability to recognize or regulate their unacceptable behavior exist between these conditions and those sustained acutely after neurologic injury, the pathophysiology and rehabilitation are not the same.
Scope of Impulse Control Disorders for Neurological Rehabilitation
As noted, the remainder of this article will focus on acute and persistent impulse control disorders that are acquired through a neurologic injury or pathology. Acquired being the key word. We will not be addressing many of the common ICDs that are discussed in the psychiatric literature including obsessive compulsive disorders, addictive behaviors (gambling, video games, smart phone, eating), or thrill-seeking behaviors. Those interested in the disorders of impulse control that are not covered here, are directed to the seminal work of Limbrick-Oldfield et al., 2013; as well as Boes et al., 2009 [12,14].
Related, this article will not cover impulsive-compulsive disorders that emanate from dopamine therapy for persons with Parkinson’s Disease including gambling, hypersexuality, shopping, kleptomania, or compulsive eating. There are many exceptional references available to assist clinicians or scientists that are interested in this field, however [8-10].
The main conditions that will be addressed in the rehabilitation spectrum include stroke, traumatic brain injury, Multiple Sclerosis, and Parkinson’s Disease. Notably, frontotemporal dementia, Huntington’s Disease, and Chronic Traumatic Encephalopathy (CTE) have additionally been cited as conditions with an elevated incidence of behavioral changes and reduced impulse control. While some of the insights and future perspectives offered in this paper may help with the management of these (FTE, HD, CTE) progressive conditions, they are not the focus of this rehabilitation-themed paper.
Functional relevance
The functional relevance of reduced impulse control can be extensive, and dangerous. People that are not considering the environment/ situation, or only acting with consideration for themselves are at higher risk for falls, car accidents, aspiration pneumonia, addictions, criminal offenses, divorce, termination from work, and estrangement. All of these can lead to secondary problems of injury (trauma or substance related), poverty, loneliness and cognitive decline [15,16].
Clearly, a person with impaired IC is at risk for a compromised quality of life and potentially shortened lifespan as well. From a rehabilitative standpoint, a person can be functionally independent, yet less employable, unsafe in Instrumental Activities of Daily Living (IADLs), challenged to return safely to sports or school, and be less participative in their community when behavioral impairments lead to negative reinforcement within interpersonal communications. Literature on IC after concussion and traumatic brain injury details these quality of life changes well [17-21].
Prodromal indicators and care-need profiling
Research has provided insights into the anatomy and pathophysiology of impaired IC. This work combined with clinical presentation patterns/syndromes has helped us to improve rehabilitative care, education, and prognostication for persons with impaired IC. As suggested in the abstract and introduction for this article, there are remaining untapped opportunities.
Scientists and clinicians alike may consider increasing their utilization or investigation of any one of the multitude of tests currently available that examine impulse control. These tests are presently untapped and may be used better in the future to explore their power (specificity and sensitivity) indicating the early emergence of other conditions. This might include but not be limited to screening for Frontotemporal Dementia or Huntington's Disease within the degenerative diseases. Screening for impaired impulse control may also assist in the management of acutely impaired patients by providing clinicians with some insight as to further testing in the areas of attention, memory and problem solving.
The reader may recall that an accurate reflection of the amount of care that a patient may need is currently and may be increasingly used in the future for matters of reimbursement, factoring into acuity. For residents that are being admitted to a care facility, both the facility and family would benefit from a clearer picture of the care needs and costs associated. Clearly, in both the clinical and residential care needs scenarios, an accurate impression of fall risk would be helpful. Impulse control screening can serve as an essential part of that equation.
Related cognitive functions and steps to inhibit an impulse
It is apparent that an individual with acquired brain injury can continue a behavior that is either inappropriate, illegal, or unsafe for many reasons. Impulse control is just one of those reasons. However, the function of impulse control consists of several steps that would all have to happen correctly for a thought or action to be considered yet inhibited. The three steps below: recognition, decision making, and awareness are critical for a thought to be considered, leading to the final step of action or inaction. This section provides a framework and elaborates on each of these stages, so that we can have insight regarding the process of transferring a thought into action (or stopping it at thought) than we might think. Readers should note that each step, recognition through action/inaction will require episodic or declarative memory, likely both, with each event that requires inhibition. It is worth repeating here that without declarative memory, a person cannot be expected to fully rehabilitate impulse control. Persons with advanced Alzheimer's Dementia would be in this group. Even in 1848, the story of Phineas Gage includes some recovery of impulse control.
Step one: Recognition
Most decisions to walk away from a temptation will include visual or auditory recognition of the situation and the choices, or the need to make a choice. Whether a person come upon a lost item of clothing that they would like to have for themselves (visual) or a person hears about a dilemma that may cause one to act (auditory), an early step in most dilemmas could be described as problem recognition.
Step two: Decision making
Next, a dilemma requiring impulse control should include two or more possible actions, even if one of those is inaction, or walking away without engagement. Dilemmas that challenge our impulse control are common in daily existence. Everyday examples of impulse control include the above-referenced article of clothing left behind, an argument that makes a person feel certain they can “win”, and (arguably) even your dog on a walk deciding not to bark back at another dog that is charging out to the end of their fence. Engage or walk away are two very common options seen in dilemmas. Essentially a dilemma that requires impulse control requires a choice. There is a decision to be made. There are many instances in life when more than two choices are available, such as the case when ordering from a menu, choosing a restaurant, a movie, or the proverbial swipe left or right in a dating app. Step two is choice.
Step three: Awareness
Awareness could be listed as step three. Context matters. What is socially acceptable right now? What is best for me? What consequences do I face or risks am I willing to exercise? This considers time, place, and past actions (recent successes), severity of consequences and personal affinities as well as tendencies. There may be some pathway development or circuitry based on cue, routine and reward that we see in the recent work of Charles Duhigg or the ease, obvious, attractive and satisfying nature of an aberrant habit according to the work of James Clear [22,23]. Awareness not only requires our sense of the present, but also an appreciation for what we have learned (overtly state-able or (nearly) reflexively learned) from the past – combined with our perception of the present environment. We may be learning from recent trials (working memory), or more remote experiences (short- and long-term memory). Impulse control requiring awareness and memory can be seen in sports, “What pitch did he throw me last week when the count was 1 ball and 2 strikes?’; can be seen in political debates when a response from the last debate was highly criticized, and can be seen as we choose our nutrition, “I would love to have ice cream, but it is just too late in the night for me. I have bad dreams when I eat ice cream late in the evening.”. “Step three is awareness of context, which requires various lengths of recall.
Impulse control is a skill that requires several executive functions: problem recognition, decision making, awareness and memory. As one matures, their impulse control may develop as well. This would be socially expected and require learning. In development, learning about context (awareness) may be the most critical variable of the three steps listed above. This transitions us well as we now consider how to test impulse control and how to train, rehabilitate, or prevent decline. As you read further in subsequent sections, recall that impulse control is not an isolated function.
Action or Inaction?
Deciding to move, speak or gesture is often the final step in many dilemmas that require impulse control. Sometimes, the decision is action, at other times, impulse control requires inaction. Table 1 provides examples of common scenarios requiring IC across the rehabilitation continuum and distribution of functional activities.
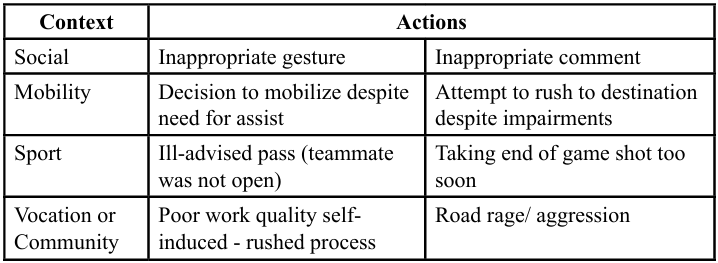
Table 1. Examples of Impaired Impulse Control
Unique Considerations with Impulse Control
Consider this scenario. Three patients were admitted to inpatient rehabilitation on the same day. Each of these people are 6 days removed from their respective injuries leading to hospitalization and ultimately admission to inpatient rehabilitation. Each patient commits an error that signals their impairment.
The first patient has endured a stroke and keeps falling to, if not pushing themselves over to the left side. This occurs in sitting and is even more pronounced in standing.
The second patient has endured their first exacerbation of what is now being thought of as Multiple Sclerosis (MS). This person presents with bladder incontinence, LE spasticity, and incomplete paraplegia.
The third patient has endured a traumatic brain injury. His face is bruised from a fall in the hospital and his movements are uncoordinated in the left arm and leg.
There can be a stigma associated with patients that are labeled inappropriate, aggressive, or unsafe. Healthcare providers may find it easier to both empathize and sympathize with the first two patients in this scenario. It may be more challenging to identify with and psychologically support the third patient who has reduced impulse control and has even been argumentative in his short stay thus far.
Clinical application: Watch out for your own biases and the tendencies to stigmatize. We may find ourselves gravitated toward patients without behavioral impairments that lead to self-injury, inappropriate actions, or potentially agitation. These are often the case for persons with reduced IC.
Screening, Examination and Objective Measures
Practitioners that are integrating the information from this article will quickly recognize that an impairment in memory, problem solving, attention, or awareness can indicate impulse control may be impaired in some or all contexts. Meaning, if impairments are identified in the aforementioned functions, it would be indicated to test impulse control specifically.
The reverse should be considered as well. Positive screening for impaired IC can give us broad insights for memory, attention, problem solving, awareness - indicating that further testing in one or all of these areas would be warranted.
Specific tests that will capture impaired IC would include the Stroop, Hayling Sentence Inhibition, and Flanker [24-27]. The Stroop and Flanker have several iterations and more being developed through emerging technologies (instrumented testing). Readers should not assume that all Stroop and Flanker tests that are being developed would hold fidelity with the original iterations that are validated and have psychometric statistics identified.
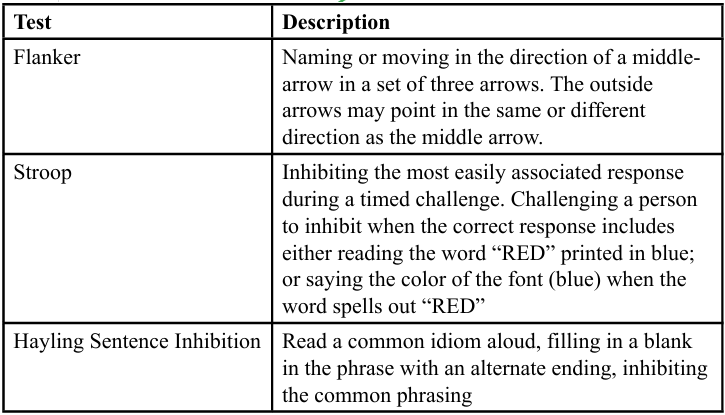
Table 2. Common Tests of Impulse Control
Wait Training: Rehabilitating IC with overtraining and neuroplasticity
Fall prevention is important. We spend over 50 billion dollars per year in the United States on fall related care and prevention. We devote research time and grant dollars to developing tests and screening tools focused on strength, power, walking speed, balance, fear, and environmental factors. While we know that reduced impulse control predicts fall frequency, we do not have adequate tools to measure and methods to rehabilitate impaired IC for persons with neurologic injury.
The concept introduced in this paper, “wait training” is more than a play on words. Learning of any kind requires a stimulus (demand on the brain) and a response (supply from the brain). Demand and supply are an oversimplified way to explain most learning arrangements in motor control, somatosensory reweighting, or even in cognition. While it may be easy for us to recall that all learning requires a stimulus sufficient to induce a response, this can feel awkward if not unsafe in the context of IC. Providers may feel inhibited in providing a task-specific stimulus when it comes to impulse control. A stimulus for the rehabilitation of IC can literally include tempting someone to be unsafe while following a primary directive “to do no harm”. Training and testing of IC each provide a person that has impaired IC the opportunity to accept a dangerous proposition. This can feel risky or be fraught with concerns of liability.
Examples and applications (5): Wait training
These four clinical scenarios are meant to be general examples of how to apply safety training in the face of impaired IC. The examples are intentionally described without a diagnosis both for simplicity and given the fact that most any person with impaired IC will have a history of a recent brain injury or stroke, the options are largely interchangeable.
1. Simon says (group training)
In this example, patients benefit from watching other group members and receiving direct feedback from their cohorts or fellow residents…but they are competing against one another. The functional context or dilemma is largely built around the common experiences of the patients. For example, in a group of people working on improving IC might all be residents of an inpatient rehab unit, so the tested tasks might include preparing a wheelchair to stand from, to transfer to/from, an urgent need to use the restroom, or related.
With Simon Says, the 3-5 members of a group might all be seated in unlocked wheelchairs across from one another (lined- up side by side). An instructor might give a request, “Okay, everybody stand up”. The pre-game instructions are clear. Patients (contestants) are not supposed to act on the command if it is not safe. If they inhibit the temptation and choose not to act on an unsafe command, they are awarded 10 points. If patients can make the task safe, then act, another 10 points. If patients perform these steps well, and catch someone else behaving unsafely, they are awarded an additional 10 points.
2. We will, we will watch you (group training)
In this example, patients benefit from watching other group members and receiving direct feedback from their cohorts or fellow residents. As with the example above, the residents may be competing against one another, or not. In this training, one person is being watched, while two to three other patients are standing or sitting, watching closely for errors.
When patients permit, this is also turned into a competitive game. Points are awarded for finding/pointing out errors in safety.
3. Challenge accepted
In a 1-1 treatment setting across the continuum of care, therapists could create a challenging scenario. “I made it unsafe. You move when it is safe.” Patients are encouraged to take time and advocate for their own safety by making the scenario safe or asking for help, rather than risking the challenge.
4. Tables-turned
In another 1-1 treatment setting, therapists role-play as a person with impaired impulse control. This can be thought of as, “You tell me what I am doing that is unsafe.“
5. Surprise attack
Finally, without the context of a game wherein a patient might alter their behaviors, therapists challenge patients with a surprise attack. In this scenario, a therapist might intentionally leave a brake off, invite a patient to stand up without an assistive device nearby, or tempt a patient to move faster than they are able. These are nuanced situations that can be both effective and well-received with the right relationship between patient and therapist. Certainly, these “attacks” would not be used in a manner that leaves a patient feeling that they are being spoken down to or that they cannot trust their provider.
Other options to screen a patient’s impulse control include opportunities for patients to predict their ability on an upcoming task, to give feedback after a task before the therapists’ assessment, or to provide a dyad option. With dyad training, patients are paired with another person with a similar diagnosis. Such training can be more well-received than feedback from a therapist that has not incurred a stroke or brain injury.
Clinical application: There are many strategies that patients’ IC can be both tested and trained. These scenarios follow the principles of neuroplasticity being task-specific, intense, challenging and may offer repetitions.
Opportunities for multidisciplinary collaboration
No matter your profession, you can benefit from multidisciplinary collaboration when treating a person with limited impulse control. Safety can be compromised by impulsive behavior in feeding, mobility, ADLs, and most certainly IADLs (shopping, meal preparation (stovetop), driving). None of us can cover all of these arenas. Allied health professionals (PT, OT, SLP), psychology, nursing, medical staff and all levels of assistants are needed to give a comprehensive opportunity to help patients regain safety through “wait training”.
References
Moffitt, T. E., Arseneault, L., Belsky, D., Dickson, N., Hancox, R. J., Harrington, H., Houts, R., Poulton, R., Roberts, B. W., Ross, S., Sears, M. R., Thomson, W. M., & Caspi, A. (2011). A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences of the United States of America, 108(7), 2693–2698. View
Fariba KA, Gokarakonda SB. Impulse Control Disorders. (2023). Aug 14. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32965950. View
Lessons of the brain: The Phineas gage story. (2019, March 8). Harvard Gazette. View
Probst, C. C., & van Eimeren, T. (2013). The functional anatomy of impulse control disorders. Curr Neurol Neurosci Rep. 13(10):386. doi: 10.1007/s11910-013-0386-8. PMID: 23963609; PMCID: PMC3779310 View
Falk, A., Kosse, F., Pinger, P. (2020). Re-Revisiting the Marshmallow Test: A Direct Comparison of Studies by Shoda, Mischel, and Peake (1990) and Watts, Duncan, and Quan (2018). Psychol Sci. 31(1):100-104. View
Stein, M. S., & Reynolds, F. A. (2022). How is carer strain related to the recovery of stroke survivors with right hemisphere dysfunction? Implications for practice. Disability and rehabilitation, 44(5), 693–701. View
Boes, A. D., Bechara, A., Tranel, D., Anderson, S. W., Richman, L., & Nopoulos, P. (2009). Right ventromedial prefrontal cortex: a neuroanatomical correlate of impulse control in boys. Soc Cogn Affect Neurosci. 4(1):1-9. View
Zhang, J. F., Wang, X. X., Feng, Y., Fekete, R., Jankovic, J., Wu, Y. C. (2021). Impulse Control Disorders in Parkinson's Disease: Epidemiology, Pathogenesis and Therapeutic Strategies. Front Psychiatry. 9;12:635494. View
Biundo, R., Weis, L., Abbruzzese, G., Calandra-Buonaura, G., Cortelli, P., Jori, M. C., Lopiano, L., Marconi, R., Matinella, A., Morgante, F., Nicoletti, A., Tamburini, T., Tinazzi, M., Zappia, M., Vorovenci, R. J., & Antonini, A. (2017). Impulse control disorders in advanced Parkinson's disease with dyskinesia: The ALTHEA study. Movement disorders: official journal of the Movement Disorder Society, 32(11), 1557–1565. View
Latella, D., Maggio, M. G., Maresca, G., Saporoso, A. F., Le Cause, M., Manuli, A., Milardi, D., Bramanti, P., De Luca, R., & Calabrò, R. S. (2019). Impulse control disorders in Parkinson's disease: A systematic review on risk factors and pathophysiology. Journal of the neurological sciences, 398, 101–106. View
Canesi, M., Lavolpe, S., Cereda, V., Ranghetti, A., Maestri, R., Pezzoli, G., & Rusconi, M. L. (2020). Hypomania, Depression, Euthymia: New Evidence in Parkinson's Disease. Behavioural neurology, 2020, 5139237. View
Blum, K., Gull, J. G., Braverman, E. R., & Comings, D. E. (1996). Reward deficiency syndrome. Am Sci. 84:132–45. View
Limbrick-Oldfield, E. H., van Holst, R. J., & Clark, L. (2013). Fronto-striatal dysregulation in drug addiction and pathological gambling: Consistent inconsistencies?. NeuroImage. Clinical, 2, 385–393. View
Robinson, T. E., & Berridge, K. C. (2008). Review. The incentive sensitization theory of addiction: some current issues. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 363(1507), 3137–3146. View
Boes, A. D., Bechara, A., Tranel, D., Anderson, S. W., Richman, L., & Nopoulos, P. (2009). Right ventromedial prefrontal cortex: a neuroanatomical correlate of impulse control in boys. Soc Cogn Affect Neurosci. 4(1):1-9. View
Cooper, C. L., Phillips, L. H., Johnston, M., Whyte, M., & MacLeod, M. J. (2015). The role of emotion regulation on social participation following stroke. The British journal of clinical psychology, 54(2), 181–199. View
Silva, S. M., Corrêa, J. C. F., Pereira, G. S., & Corrêa, F. I. (2019). Social participation following a stroke: an assessment in accordance with the international classification of functioning, disability and health. Disability and rehabilitation, 41(8), 879-886. View
Smith, N. I. J., Gilmour, S., Prescott-Mayling, L., Hogarth, L., Corrigan, J. D., & Williams, W. H. (2021). A pilot study of brain injury in police officers: A source of mental health problems?. Journal of psychiatric and mental health nursing, 28(1), 43–55. View
Taylor, K. M., Kioumourtzoglou, M. A., Clover, J., Coull, B. A., Dennerlein, J. T., Bellinger, D. C., & Weisskopf, M. G. (2018). Concussion History and Cognitive Function in a Large Cohort of Adolescent Athletes. The American journal of sports medicine, 46(13), 3262–3270. View
Hrabarchuk, E. I., Hannah, T., Kalagara, R., Li, A. Y., Schupper, A. J., McCarthy, L., Ali, M., Quinones, A., Gometz, A., Lovell, M., & Choudhri, T. F. (2024). Baseline ImPACT Composite Scores in Student-Athletes With Attention-Deficit/Hyperactivity Disorder. Archives of clinical neuropsychology: the official journal of the National Academy of Neuropsychologists, 39(3), 347–354. View
Hiraoka, T., & Yagi, M. (2023). The Pathogenesis of Disinhibition in Patients with Traumatic Brain Injury: A Two Patient Case Report. Brain sciences, 13(8), 1227. View
Tsushima, W. T., Ahn, H. J., Siu, A. M., Yoshinaga, K., Choi, S. Y., & Murata, N. M. (2019). Effects of repetitive subconcussive head trauma on the neuropsychological test performance of high school athletes: A comparison of high, moderate, and low contact sports. Applied neuropsychology. Child, 8(3), 223–230. View
Duhigg, C. (2012). The power of habit: Why we do what we do in life and business. Random House. View
Clear, J. (2018). Atomic habits: An easy & proven way to build good habits & break bad ones. Penguin. View
Soleimani Rad, H., Abolghasemi, A., Shakerinia, I., Mousavi, S. V. (2024). Self-control problems in Intermittent Explosive Disorder: Presentation of an explanatory approach. J Behav Ther Exp Psychiatry. 85:101973. View
Kamran, L., Golestaneh, S. M. (2025). Epidemiology and Cognitive Function in Adults with ADHD and Cognitive Disengagement Syndrome. Percept Mot Skills. 19:315125251370101. View
Motta, K., Lee, H., Falkmer, T. (2014). Post-stroke driving: examining the effect of executive dysfunction. J Safety Res. 49:33-8. View
Karr, J. E., Ingram, E. O., Pinheiro, C. N., Ali, S., Iverson, G. L. (2024). Test-Retest Reliability and Reliable Change on the NIH Toolbox Cognition Battery. Arch Clin Neuropsychol. 24;39(6):702-713. View