
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 2 (2020), Article ID: JMHSB-119
https://doi.org/10.33790/jmhsb1100119Mini Review
The Role of Social Work in Integrating Mental Health Students in Traditional School Settings: Community Care Approach
Terrance Ruth*, Ph.D., Kelsey O’Connor
Department of Social Work, North Carolina State University, United States.
Corresponding Author Details: Terrance Ruth, Ph.D., Professor in the Department of Social Work at North Carolina State University, United States. E-mail: trruth@ncsu.edu
Received date: 09th May, 2020
Accepted date: 17th June, 2020
Published date:26th June, 2020
Citation: Ruth, T., & O’Connor, K. (2020). The role of Social Work in Integrating Mental Health Students in Traditional School Settings: Community Care Approach. J Ment Health Soc Behav 2(1):119.
Copyright: ©2020, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This article introduces critical reflection, embedded in critical social work tradition, as a tool to equip social workers with the skills to integrate mental health K-12 students into mainstream school environments. Using the context of community of care model debate, this article examines the seclusion of students impacted by mental health. It is argued that the isolation of mental health students is a form of oppression and injustice that harms a student’s sense of belonging. Therefore, it is recommenced that Social Workers use critical reflection coupled with an intersectional approach as a tool to focus on the interplay and complexity of oppression, inequalities and injustices. The perceived stigma of mental health in school settings require a critical reflection tool, due to the extended isolation of students. This article applies critical reflection and intersectionality to understanding the ideal process of integration for mental health students in a school environment while examining: (1) Student Belonging, (2) Difference and (3) Community Care approach.
Keywords:
Community Care, Mental Health, Belonging, Social Work
Introduction
In public schools (K-12 grades), students provided with a mental health diagnosis are often served in settings outside of the mainstream student population. Attention provided to students with mental health services occur outside of communion with student-peers. As a result, the social ignorance surrounding mental health and the stigma of difference are amplified by physical isolation. Social workers are important in bridging the understanding and interventions, involving mental health, to education professionals and traditional students. Historically, Social workers held a similar knowledge awareness role in the mental health movement transfer to community care approaches. There are several overlapping similarities in integrating students with mental health services into the mainstream school environments and the 20th century shift to community-based mental health services. The three overlapping concepts are (1) Student Belonging, (2) Difference and (3) Community Care approach.
Mental Health Problems in Adolescence
In the United States, 20% of adolescents may experience a mental health problem in any given year [1][2]. Researchers estimate that 10% of children and young people (aged 5-6) have a clinically diagnosable mental problem [3]. Mental health functioning of children and youth varies according to gender, presence of disability and household socioeconomic standing (SES).
Research indicates, that adolescence girls have a higher prevalence of depression and eating disorders and engage more in suicidal thoughts and suicide attempts than boys, who are more likely to participate in high-risk behaviors and commit suicide more often [4,5]. K-12 students with an intellectual disability display behavior which may be symptomatic of mental health or psychological impairment four times more often than their peers; with psychiatric disorders in students with a disability often undiagnosed and untreated [6]. Students’ SES (social-economic-status) influences mental health across the lifespan, with socially and economically disadvantaged children and adults found to be most at-risk for both physical and mental health problems [7,10]. It is important to account for within group variability in mental health functioning of students.
There is alarming evidence that support the stability of mental health concerns in students and its longitudinal impact on mental health disorders, crime, delinquency, unemployment, homelessness and suicidal behavior in adulthood [11,14]. Mental health problems in students could be antecedents of chronic, complex, disabling and expensive complications in adult life. For these reasons, early detection and treatment of mental health issues is significant. Research indicate that mental health disorders that are likely to persist into adult life emerge between ages 12 and 25 [15,16]. Early intervention is preferred due to economical and cost-effectiveness [17]. There is a need for additional understanding of mental health K-12 students [18,20].
School belongingness refer to students’ beliefs of being ‘‘personally accepted, respected, included, and supported by others in the school social environment’’ [21], has emerged as an important factor associated with positive health outcomes [22]. A growing body of evidence with typically developing youth supports the interrelationship between school belongingness and positive mental health outcomes. School belongingness and mental health functioning, is the exclusion of students with disabilities in the study samples, despite their presence in the traditional school system. Findings show school belongingness to be negatively associated with emotional stress, suicide attempts, and violence amongst students with learning disabilities [23].
Schools are an ideal setting for efficiently detecting and treating children and adolescents with identified mental health diagnosis because they offer the opportunity to reach large numbers of students [18,20]. The proposed treatment is the inclusion of mental health services and mental health students into the mainstream school environment. Traditionally, mental health services are placed in discrete areas of the school environment which often result in the isolation of students receiving mental health supports. Social Workers advocating for mental health service integration can lead to a sense of belonging for students receiving the mental health supports.
Understanding group difference
Integration describes the process of shifting access to community, between two groups, with the understanding that healthy relationships contribute positive social determinants. Often, the two groups involved are engaged in a relationship divided by social differences and an imbalance of power. Allport describes social differences as the barrier to healthy relationships or successful integration. Differences are interpreted through social categories, prejudices and stereotypes. Cognitive processes associated with social categorization facilitate the harm done by prejudices [24]. Prejudice is the fundamental problem of intergroup relations [24]. Allport argued that categories and their attendant stereotypes operate in the service of prejudice, noting that the purpose of stereotypes “is to justify (rationalize) our conduct in relation to that category” [24]. He primarily centered his understanding in racism and ethnic relations. For the social differences between mental health students and traditional students, it is assumed that the functions of prejudice, stereotype and categorization functions the same for disability stigma.
According to Allport, differences come from the existence of a core actual people-group difference which become magnified by prejudices so that the resulting stereotypic beliefs about out-groups are more extreme, negative, and overgeneralized than warranted [24]. Each group started with an observed difference rooted in reality, but these perceptions became negative caricatures of what the groups were actually like. The prejudiced person then comes to invoke group differences as a justification for his/her prejudiced attitude [25]. Although beliefs can be internally challenged, typically “they have the slippery propensity of accommodating themselves somehow to the negative attitude which is much harder to change” (p.13). Krech and Crutchfield [26] argued that the “Grouping of people in perception does not, in itself make for (negative) prejudice – it merely makes such beliefs and attitudes possible” (p. 506, emphasis in original). Social grouping can just as easily lead to favorable attitudes toward a group and it is the “nature of the cue that supports the grouping” that is critical to whether or not negative prejudice follows [26]. It is not the cue of “mental health” that leads to prejudice, but rather, Krech and Crutchfield argued, the supporting or correlated cues of poverty, special education, and stigma of mental weakness. What is important is to eliminate these correlated cues as a barrier to integrating the mental health student population with the mainstream population. Social Workers are ideally trained and positioned to manage the school culture surrounding perceptions of students with disabilities. Social Workers are also prepared to understand the unique experience of each student both in a diverse school community setting and in a homogenous classroom setting. Schools, staffed with social workers, can benefit from the community care approach by providing an environment that increases students’ sense of belonging.
Lessons to Learn from Community Care
The school building contains both the informal and formal community for students. Although the community care approach adopts a macro view of community, there are lessons to learn from the history of this perspective. The community of care approach references the larger community, to include: neighborhoods, religious institutions, local markets and businesses, medical and non-medical settings, etc. The origins of community care were to improve the care of people impacted by mental health effects, in society. The reasons for the shift toward community-based mental health services is complicated [27]. Historically, the challenges to social workers, in implementing this approach, included factors such as the discovery of new medications and treatments, changing social attitudes, and wider government policies. However, economic policies of governments created new funding avenues to promote the implementation of community care.
The varying approaches of institutionalization and communitybased care are all responses to mental illness [28]. The era of implementing asylums was interpreted as a departure from the abandonment of groups of the poor mentally ill and private provision for the wealthy. Then the community care approach was seen as a variant of a continuum of enhancements to mental illness services. The impulse behind community care was to improve the standards of mental health provision. Social workers should see the integration of students, impacted by a mental health illness, as part of the continuum of enhancements to mental health services. The student community, in a school setting, relegate mental health students to the peripheral of school activities and engagement. For example, the location of special education classrooms, support service personnel offices, and recreational areas for students, provided with mental health services, are often isolated from traditional-student learning spaces. The location of classrooms for students, impacted by mental health illnesses, are customarily in areas of the school that are visited less-frequently. The physical and social isolation of students with mental illness may have negative implications.
One of the most important arguments put forward in support of community care is that prolonged periods of isolated care are, in and of themselves, damaging. The same argument stands for students isolated from peers during extended times in the school environment. Furthermore, it is argued that services need to exist to intervene at an earlier stage to provide support to those suffering from any form of mental distress. Additionally, exposing students impacted by mental distress, at an early age, to students in traditional school environments may have a positive long-term affect. A community of care model make provisions that ideally develops tiers that serve the individual and community need. Historically, the asylum system resulted in a complete social imbalance. Services were almost always operated in isolation from communal engagement. The focus of modern mental health services is similarly unbalanced. The insurance-risk dominated model of service delivery focuses on a smaller population group. The concern is that this means that the social determinants (http://www. who.int/social_determinants/en/) of and the impact of mental illness become obscured or marginalized. This focus on audit, compliance, and regulation has been termed bureau-medicalization [29].
The justification for the development of community-based mental health services is based on clinical and moral arguments. It is a consolidation of pragmatic and idealistic approaches. The idealism was embedded in human rights which suggested that Communitybased services would be, by definition, more humane. Lamb and Bachrach [30] argue that this was based on a moral argument with minimal supportive evidence. The supporters of community based mental health services did not argue that asylums should be replaced by increased seclusion alternatives, like jail. Deinstitutionalization, a progressive policy aimed at reducing the civic and social isolation of the mentally ill, failed to accomplish their goals [31]. Moon [32] and Knowles [33] shows the ways that asylums have been replaced by a fragmented network of bedsits, housing projects, day centers, or increasingly, prisons, and the criminal justice system. This process was labeled “trans-institutionalization”, which incorporates the ideas that individuals live in a community setting but have little engagement with others and major social interactions are with professionals paid to visit or monitor them. Kelly [34] suggest that social seclusion is a form of structural violence, which highlights the impact of a range of factors including health, mental health status, and poverty. These trends are likely to increase as the direction of services withdraws from decentralized provisions [35]. Although the case was made for the benefits of this model, it is important to understand the limitations.
Problems in the community care movement
The problems in the community care movement can be summed up as idealistic assumptions of community care and normalization.

Table 1Community Care Assumptions
Researchers critically assessed the underlying assumptions of the community care movement. These are as follows:
Critics suggested that all these assumptions of community care were actually false rather than the reality of caring for mental health students in the community [36]. Others have shared similar concerns challenging whether the community could fulfil the ideology and functions of community care. Both Hawks and Bachrach assumed that good community care was not a realistic idea. Outcome studies found that many mental patients were left uncared for within the community. Similarly, the principles of normalization have been challenged. In principle, it is good to pay due respect to the rights and equal opportunities of the disabled. In practice, its advocates appear to have left many disabled persons in the community without sufficient care and protection. In the de-institutionalization and community care movements, the advocates have tended to utilize the ideology of community and normalization to close ‘expensive’ centralized supports but provide cheap and insufficient community services for the individuals impacted by mental health [37,39].
The types of community care
Centuries ago, scholars identified two types of community care [40]. The two care models were described as ‘care in’ and ‘care by’ the community. ‘Care in’ the community means care provided in the community and refers to formal care in service units. In school settings, this would resemble mental health service providers deliberately distributed throughout the building with rather than in isolation. For example, the office of key support professionals, such as social workers and psychologist, will be located near classrooms in proximity to the direct learning spaces. This proximity will normalize the coexistence of students receiving mental health services with traditional peers. ‘Care by’ the community implies the care provided by informal or natural networks [40],[41]. In school settings, this would resemble service embedded in traditional classrooms alongside peers in the same physical location. For example, school systems invest in additional support staff so that social workers are integrated into the classroom student ratio.
In Bulmer’s view, the failure of the community care movement is mainly due to the under-development of informal community care [41]. Community care should not only be interpreted as transferring institutional care into formal community care or decentralizing medically oriented hospital care into small units of mental healthrelated services. It should also mean the development for students, impacted by mental health, of natural support systems such as peers, family and friends. It is encouraged to challenge assumptions that every community has the capacity to fulfil all the requirements of providing adequate community care. Furthermore, it is discouraged to maintain a pessimistic view that all communities are harmful to the care and rehabilitation of students with mental health services. Rather,one should put more effort into estimating and developing the caring potentials of the learning community by smoothing the coordination of formal services, educating the general public to accept students with mental health services, and supporting the teachers and administrators to care for the students in a more decentralized environment.
Community care (de-centralized) and institutional (or centralized) care for students, impacted by mental health, should not be interpreted as mutually exclusive to each other. In application, the protective functions of small-sized mental health services can never be under-estimated [39]. They can never be replaced by community care services, especially in dealing with psychiatric and medical emergencies. Early thinkers pointed out that severe and chronic mental patients require good and humane institutional care [36]. The failures of the community care movement are partly due to the assumption of the total elimination of the centralized care and partly due to the neglect of the protective and custodial function of good and humane medium-sized or small mental health services. For schools, it is important to value the existing mental health supports that occur in the isolated spaces and see the extension of services as the movement towards integration of classrooms. In other words, it is critical to promote shifting to the de-centralization and integration of mental health services towards a proximal distance of direct instruction. Also, it is important to understand the impact on social workers as the profession that is key to understanding the limitations of the community care approach.
Implications for social work practice
Historically, social workers have been involved in all aspects of mental health services, especially at the community level. Clinical social workers were sometimes the only mental health providers in a geographic area. The contribution of social workers in the development of the community care movement can never be overstated. The deinstitutionalization movement generated an opportunity for social workers to develop aftercare and community support for individuals impacted by mental health [42]. The problems of the community care movement have strong implications for social work practice. If they can be handled properly, they represent good challenges and opportunities for social workers. Schools already depend on social workers to exist as a bridge between the external neighborhood community and the school environment. Social workers will maintain that community function for the integration of students impacted by mental health into mainstream school environment. However, the environment under consideration is on a micro scale that only includes the school-based environment.
Enriching the concept of community care by normalization and social integration
The concept of community care should have been enriched by the debate of normalization and social integration in caring for mental patients [43],[46]. One of the reasons for the idealistic assumptions of community care is the concept that the mental patients can be integrated into the community immediately without any burdens and problems. Nevertheless, theories of social integration and normalization stress that the rehabilitation and community care of students with mental health concerns should be a gradual process that requires acceptance by peers, the services, the school-community, the professionals, and their families. In the absence of a rigorous rearticulation of the concept of normalization, community care will be a question of pushing back a disabled individual into an ignorance traditional school-community, both of which reject and are mutually exclusive of one another. Without the concept of social integration, community care will remain a sudden transfer of an isolated student from the specialized treatments to a strange and unfamiliar schoolcommunity where s/he cannot adapt. The ideology of normalization and social integration is closer to the values of social work, such as respecting the individuality, dignity, self-determination and integrity of every mental patient in his or her process of rehabilitation.
Developing an inclusive community for students
In the community care of mental health students, a social worker should spearhead the implementation of an inclusive community. Social work intervention in psychiatric rehabilitation and community care services should not be confined to passive individual-oriented skills training, casework or counselling approaches. Community development in the form of community education, locality development, and even social planning Rothman [47] has to be included in social work intervention with students impacted by mental health. Social workers in community care services must identify themselves as community workers. Recommended roles are as follows:
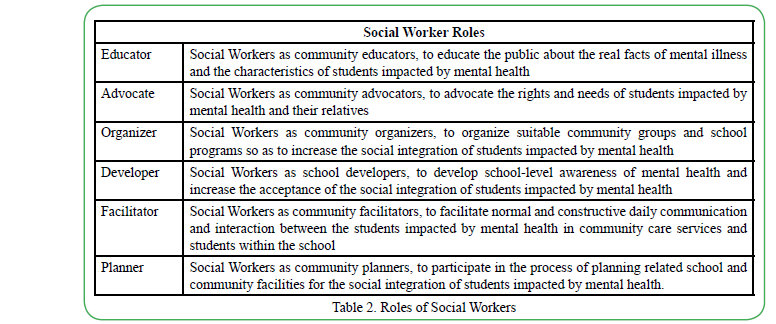
Table 2Roles of Social Workers
Through exercising all these roles, social workers can gradually develop the community to become caring and supporting in the social integration of students impacted by mental health.
Social Workers should also have sensitivity to the differences between formal and informal community care structures. Formal and informal community care are not mutually exclusive. They are complementary of each other. First, formal community care service agencies can designate professional resources for developing informal support networks, such as support team members, peers, teachers and volunteers, so that individuals impacted by mental health can be treated in an integrated, normalized environment. Second, informal community care networks, once established, can reduce the load of formal community care for individuals impacted by mental health. The leading thought is that the prevention of mental relapse is increasing likely within stable networks that lead to a sense of belonging. These natural support networks, if properly developed, create more effective and long-lasting resources for formal community care. Third, formal community care in terms of good and humane small mental hospitals, residential hostels and community mental health centers no doubt can provide good support, shelter and treatment for those mental patients and out-patients with poor and rejecting relatives, friends, neighbors and colleagues. However, these services should not be targeted as the final end of mental patients. Rather, their aim should be to prepare patients to rebuild better social supports for their return to the community. Finally, good informal community care in forms of mutual aid groups and teachers and student groups can provide a role in advocating the rights of students impacted by mental health. These groups should work hand in hand with the professional formal community care services. Social workers should be ideally the more suitable for strengthening the linkage of formal and informal community care.
Conclusion
This article reviewed the relationship between the processes of moving individuals impacted by mental health for macro communities and micro school communities. The similarities highlight the key elements that provides implications for social work practice. To implement the suggestions, schools should be willing to put enough resources into developing appropriate community care strategies and developing the school into an inclusive community. Education leaders should not regard community care as a cheaper way of replacing existing care. Secondly, within a multi-disciplinary team setting in mental health services, social workers’ unique contribution in intervention, school and community development should be recognized and supported by decision makers. Finally, the care and dependency elements in community care should be replaced by an ideology of mutual support among administrators, teachers and students within the school. Students, impacted by mental health, should be regarded as members of the school community too. Only in these ways can the potential and strengths of students, impacted by mental health, be developed during their sense of belonging and health.
Conflicts of Interest (COI) Statement
The author has declared no conflict of interest.
References
1. WHO (2003). Caring for children and adolescents with mental disorders: Setting WHO directions. [online] Geneva: World Health Organization.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., Merikangas, K.R., & Walters, E.E. (2005). Lifetime Prevalence and Ageof- Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62 (6) pp. 593-602. doi:10.1001/archpsyc.62.6.593.View
Green, H., Mcginnity, A., Meltzer, Ford, T., & Goodman, R. (2005). Mental Health of Children and Young People in Great Britain: 2004. Office for National Statistics.
Hawton, K., Rodham, K., Evans, E., & Weatherall, R. (2002). Deliberate self-harm in adolescents: self-report survey in schools in England. BMJ 23: 1207–1211.View
Parker, G., & Roy, K. (2001). Adolescent depression: A review. Aust N Z J Psychiatry 35: 572–580.View
Sturgeon, L. (2007). Mental health and intellectual disability in children and adolescents: working with this challenging population, (PPT).
Berkman, L.F., & Kawachi, I. (2000). Social Epidemiology. New York: Oxford University Press.
Wickrama, K.A.S., Conger, R.D., Lorenz, F.O., & Jung, T. (2008). Family Antecedents and Consequences of Trajectories of Depressive Symptoms from Adolescence to Young Adulthood: A Life Course Investigation. Journal of Health and Social Behavior 49: 468–483.View
Herd, P., Goesling, B., & House, J.S. (2007). Socioeconomic Position and Health: The Differential Effects of Education versus Income on the Onset versus Progression of Health Problems. Journal of Health and Social Behavior 48: 223–238.View
Barbadoro, P., Ponzio, E., Pertosa, M.E., Aliotta, F., D’Errico, M.M., Prospero, E., & Minelli, A. (2011). The effects of educational intervention on nutritional behavior in alcoholdepedent patients. Alcohol & Alcoholism, 46(1), 77-79.View
Petticrew, M., Cummins, S., Ferrell C., Findlay, A., Higgins, C., Hoy, C., Kearns, A., Sparks, L. (2005). Natural Experiments: An Underused Tool for Public Health? 119(9):751-7. doi: 10.1016/j. puhe.2004.11.008.View
Geller, D.A., Biederman, J., Faraone, S., Agranat, A., Cradock, K., Hagermoser, L., Kim, G., Frazier, J., & Coffey, B.J. (2001). Developmental Aspects of Obsessive Compulsive Disorder: Findings in Children, Adolescents, and Adults. J Nerv Ment Dis, 189(7):471-7. doi: 10.1097/00005053-200107000-00009.View
Cicchetti, D., & Rogosch, F. A. (1999). Psychopathology as risk for adolescent substance use disorders: A developmental psychopathology perspective. Journal of Clinical Child Psychology, 28(3), 355–365. https://doi.org/10.1207/ S15374424jccp280308 View
Fordwood, S.R., Joan, Asarnow., Diana, P.H, & Steven, P.R. (2007). Suicide Attempts Among Depressed Adolescents in Primary Care. Journal of Clinical Child & Adolescent Psychology 36(3):392-404. DOI: 10.1080/15374410701444355 View
Patel, M., Farzana, L., Robertson, L.K., Hutchinson, J., Grubbs, N., Shepherd, M.N., & Mahaffey, J.W. (2007). The appendage role of insect disco genes and possible implications on the evolution of the maggot larval form. Dev. Biol. 309(1): 56--69.View
R. S. C. Lee, M. A. Redoblado-Hodge, S. L. Naismith, D. F. Hermens, M. A. Porter, and I. B. Hickie (2004). Cognitive remediation improves memory and psychosocial functioning in first-episode psychiatric out-patients. Psychol Med. 2013 Jun; 43(6): 1161–1173. doi: 10.1017/S0033291712002127 View
Viswanath, V., & Fred D. Davis. (2000). A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. 46(2):186-204. DOI: 10.1287/mnsc.46.2.186.11926.View
M G Sawyer, F M Arney, P A Baghurst, J J Clark, B W Graetz, R J Kosky, B Nurcombe, G C Patton, M R Prior, B Raphael, J M Rey, L C Whaites, S R Zubrick. (2001). The Mental Health of Young People in Australia: Key Findings From the Child and Adolescent Component of the National Survey of Mental Health and Well-Being. Aus N Z J Psychiatry, 35(6):806-14. doi: 10.1046/j.1440-1614.2001.00964.x.View
Verhulst, F. C., & Koot, H. M. (Eds.). (1995). The epidemiology of child and adolescent psychopathology. Oxford University Press.View
VHall, S., Matthew, J. K., Ryan, M., Nielson, J.S. Horne (2009). Identifying and prioritizing ungulate migration routes for landscape-level conservation. https://doi.org/10.1890/08- 2034.1 View
Carol Goodenow (1993). Classroom Belonging among Early Adolescent Students. The Journal of Early Adolescence 13(1):21-43. DOI: 10.1177/0272431693013001002 View
R.W. Blum (2005). A case for school connectedness. Educational leadership: journal of the Department of Supervision and Curriculum Development, N.E.A 62(7):16-20 •
Maria Veronica Svetaz, Marjorie Ireland, Robert Blum (2000). Adolescents With Learning Disabilities: Risk and Protective Factors Associated With Emotional Well-Being: Findings From the National Longitudinal Study of Adolescent Health. Journal of Adolescent Health 27(5):340-8. DOI: 10.1016/S1054- 139X(00)00170-1View
Allport, G. W. (1954/1979). The nature of prejudice. Cambridge, MA: Perseus Books.View
Jost, J. T., & Hamilton, D. L. (2005). Stereotypes in Our Culture. In J. F. Dovidio, P. Glick, & L. A. Rudman (Eds.), On the nature of prejudice: Fifty years after Allport (p. 208–224). Blackwell Publishing. https://doi.org/10.1002/9780470773963.ch13 View
Krech, David/Crutchfield, Richard S. (1948): Theory and Problems of Social Psychology. New York: McGraw Hill View
Pilgrim, D., Rogers, A. (2013) Sociology of mental health and illness, Buckingham, England: Open University Press.
Scull, A. (1989) Social order/mental disorder: Anglo-American psychiatry in historical perspective, Berkeley, CA: University of California Press.View
Nathan, J., Webber, M. (2010) Mental health social work and the bureau-medicalization of mental health care: Identity in a changing world. Journal of Social Work Practice 24(1): 15–28.View
Lamb, R., & Bachrach, L. (2001) Some perspectives on deinstitutionalization. Psychiatric Services 52(8): 1039–1045.View
Wolff, N. (2005) Community reintegration of prisoners with mental illness: A social investment perspective. International Journal of Law and Psychiatry 28: 43–58.View
Moon (2000) Risk and protection: The discourse of confinement in contemporary mental health policy. Health & Place 6(3): 239–325.View
Knowles, C. (2000) Bedlam on the streets, London, England: Routledge.View
Kelly, B. (2005) Structural violence and schizophrenia. Social Science and Medicine 61: 721–730.View
Wacquant, L. (2009) Punishing the poor: The neoliberal government of social insecurity, Durham, NC.View
Hawks, D. (1975) ‘Community Care: An Analysis of Assumption’, British Journal of Psychiatry 127: 276–83.
Hafner, H. and W. Heidner (1989) ‘The Evaluation of Mental Health Care Systems’, British Journal of Psychiatry 155: 12–17.View
Lamb, H.R. and R. Shaner (1993) ‘When There Are Almost No State Hospital Beds Left’, Hospital and Community Psychiatry 44: 973–6.View
Thornicroft, G. and P. Bebbington (1989) ‘De-institutionalization from Hospital Closure to Service Development’, British Journal of Psychiatry 155: 739–53.View
Bayley, M. (1973) Mental Handicap and Community Care. London: Routledge & Kegan Paul.View
Bulmer, M. (1987) The Social Basis of Community Care. London: Allen & Unwin.View
Rose, S.M. (1987) ‘Deinstitutionalization: A Structurally Generated Opportunity for Social Work’, International Social Work 30: 251–7.
Wolfensberger, W. (1972) Normalization: The Principle of Normalization in Human Services. Toronto: National Institute for Medical Research.View
Tyne, A. (1992) ‘Normalization: from Theory to Practice’, in H. Brown and L. Ward (eds) Normalization: A Reader for the Nineties, pp. 35–46. London: Routledge.
Ramon, S. (1989) ‘The Value and Knowledge Bases of the Normalization Approach: Implications for Social Work’, International Social Work 32: 11–23.View
Cotterill, L. (1994) The Social Integration of People with Schizophrenia. London: Avebury.View
Robert A. Rothman (1979). Occupational Roles: Power and Negotiation in the Division of Labor* Volume20, Issue4 September 1979 Pages 495-515. https://doi. org/10.1111/j.1533-8525.1979.tb01231.x View